
Abstract
BACKGROUND:
The majority of handicraft workers in India falls under the informal sector, which plays a prominent role in the employment generation. Artisans in handicraft sectors encounter various hazards and risks causing occupational diseases.
OBJECTIVE:
The key objective of the study is to identify the prevalence of musculoskeletal disorders and occupational risk factors among the artisans involved in making traditional lacquerware toys in Karnataka and Andhra Pradesh, South India.
METHODS:
The subjects considered in this study are 177 artisans who work in mechanized lathes at Channapatna of Karnataka and Etikoppaka of Andhra Pradesh, South India. The information regarding the reported work-related musculoskeletal disorders (WMSD) symptoms from 7 days to 12 months are collected through modified Standardized Nordic Questionnaire and by direct observations. Moreover, the intervention of WMSD in their day-to-day life and the overall comfort of their body are also determined. The questionnaire survey is conducted through face-to-face interviews and by direct field study.
RESULTS:
From the statistical analysis, it is found that about 76.83%of the study population (77.4%male and 74.28%female) has self-reported WMSDs. The prevalence of WMSD is most common in the age group of 30–40 years. Physical factors like workplace adaptability, stress at work, body postures, health status, body mass index, active and enough breaks during work and body condition at the end of work have a significant association with WMSD.
CONCLUSION:
In this study, many of the work-related and lifestyle/health-related factors show a significant association with WMSD in artisans. The sub-standard working environment and the nature of work expose artisans to many occupational risks in their day-to-day life. To mitigate the occupational risks and musculoskeletal disorders, the workspace needs to be redesigned ergonomically.
Keywords
Introduction
The uniqueness of a country or a region is reflected by its handicraft work. Handicraft-based industries belong to the secondary and informal/unorganized sector of a country’s economy. These informal/unorganized sectors consist of own account enterprises and operated by own account by hiring workers. In developing countries like India, handicraft is the major source of income for many communities in rural parts and it employs millions of artisans of various kinds [1]. These artisans in the handicraft industries of various sizes are subjected to many kinds of work-related musculoskeletal disorders (WMSD) [2]. WMSD is considered a costly occupational disorder often caused by overuse of joints, nerves, muscles, tendons and soft tissues of the body [3]. Rupture in tendons/muscles/ligaments, muscle strains, fracture of bones and other degenerative changes in the body causes MSDs [4]. WMSD mostly depends on the working environmental factors like man-machine interfaces, individual characteristics and total working system [5]. Physical demands at workplace are commonly assumed as a main cause of LBP and absenteeism among workers [6, 7]. Low back pain (LBP) is considered the main cause of disability adjusted life years (DALY) globally [8, 9]. Handicraft is a creative art and craft work which depends on the skill set of the artisans of specific geographical region. Artisans use many hand tools to manufacture various handcrafted products. The chances of getting hurt by the hand tools are common in routine works. Mishandling of hand tools, lapses of attention during work causes severe injuries to upper extremities [10, 11]. Several researchers worked on the handicraft sector have proved the relation between WMSDs and physical workplace exposure [12].
The art of making lacquerware wooden toys is over 200 years indigenous. It has been traditionally transferred to artisans from their ancestors through generations. Lacquerware toys are made of the wrightiatinctoria tree which is locally called ‘Ankudikarra’ in Andhra Pradesh and ‘Aalemara’ in Karnataka, South India. The natural dyes used for coloring the attractive toys are made from the resin secreted from the female lac bug on trees, vegetables, seeds, roots and barks. These toys are eco-friendly and non-hazardous. The state government of Andhra Pradesh and Karnataka has given the status of GI (Geographical Indication) for this traditional craft under WTO (World Trade Organization). Karnataka tableau, which depicts the famous Channapatna toys, has been awarded in the tableaux category by the Ministry of Defense, India for the competitive presentation in the 66th Republic day Parade-2015.
The workforce in developed and developing countries are exposed to some form of occupation health and safety hazards [13]. The risk of having a work-related injury in developing countries is 10–20 times higher than that of developed countries [14]. Unsafe working conditions are one of the leading causes of death and disability among the working population [15]. This is because workers in unorganized units are unprotected by social security system [16]. ILO estimates that around 0.4 million people in India die every year due to work-related problems, that is, around 46 people die every hour [17]. Artisans working in the small and medium scale units are beyond the scope of labor regulations [18, 19]. Most of the toy-making units visited during the present research were having only 4–6 employees. Factories act-1948 of India does not cover the factories having less than 10 employees. But work-related injuries are common in these informal sectors leading to disability [20]. Occupational health problems in informal sectors are not reported anywhere or recorded in any form in state or national level surveys in India. Handicraft making units should be encouraged to ensure safety health and accident prevention practices at workplaces.
Artisans involved in making traditional lacquerware toys are settled down in rural and remote areas of South India, mainly in Karnataka and Andhra Pradesh. They are exposed to several risk factors in the workplace. Upper extremity disorders are the most common among artisans due to work nature [21]. Handicraft workers engaged in hand intensive jobs reported high prevalence of musculoskeletal symptoms in wrist and fingers [22]. In addition, handicraft workers experienced symptoms in their lower back, neck and knees [23]. Musculoskeletal disorders in upper extremities are due to repetitive manual works in the workplace [24]. The shoulder complex has a greatest mobility of all joints in the body. The forces and velocities applied by the shoulder have the great risk of injury especially in the setting of improper mechanics [25]. Several work-related risk factors such as awkward postures, high repetition rates and forceful exertions are some cause of increased prevalence of MSDs. Health and safety programs emphasizing primary prevention strategies have been proposed to reduce the prevalence of MSDs. Prevention of MSDs can lead to significant reductions in occupational disorders, decreased health care costs and improvements in production efficiency. The present study is aimed to identify the work-related musculoskeletal disorders (WMSD) and occupational physical risk factors among the artisans involved in making traditional lacquer-ware toys.
Subjects and methods
Sampling size selection
The sampling size is chosen based on a non-probabilistic method. Several thousands of artisan families are involved in traditional lacquerware toys making process, among which some artisans are making toys in hand lathes (Fig. 1a). Artisans working in hand lathes are majorly females and works for 2-3 hours daily during their leisure time. In this study, only artisans working on mechanized lathes are considered because these artisans are full-time workers and are working in the same units for more than 3 years. The sample size (n = 177) is considered for the present study. Ninety samples from Channapatna, Karnataka and 87 samples from Etikoppaka, Andhra Pradesh, South India are considered for the study. The places selected for this study were based on the concentration of toy making units and these places are well known globally for their traditional lacquer-ware toys.

Female artisan working with hand lathes.
The subjects selected in this study are the artisans who are involved full time in making traditional lacquerware toys for not less than three years continuously. Artisan’s workup to 10 hrs daily and sometimes duty stretches depends on the workload. Artisans get their wages on daily basis or sometimes weekly. For artisans, the wages are directly proportioned to production and there are no fixed wages. They have six working days with one day off. About 177 artisans belonging to the age group of 24–60 years are selected for this study based on availability and active participation in the questionnaire survey. Artisans who are physically challenged, suffering from traumatic injuries, affected by chronic diseases, met with accidents in past 12 months at workplace, part-time artisans, owners of toy-making units, pregnant women and those who have crossed the age of 60 years were excluded from this study. Data were collected for 480 artisans, considering the above-mentioned parameters 303 were excluded. The study covered a range of units from the household, small scale and several medium units. All the artisans who participated in the survey were made aware of the purpose of the study and written informed consent was obtained. The study was approved by the institutional human research ethics committee.
Pilot survey
Before the pilot survey, authors visited the toy-making units several times to understand the work process, working environment and interacted with artisans to identify the physical risk factors involved in making traditional lacquerware toys. More than 10%of the study samples participated in the pilot survey. Based on their feedback, necessary changes are made, and the modified Standard Nordic Musculoskeletal Disorder questionnaire is prepared for the study to be conducted.
Data collection
During the study, the data were collected from face-to-face interviews at toy making units with the help of questionnaires and by direct observation. Questions framed are based on the work nature, work environment, feedbacks from the pilot survey and Standard Nordic Musculoskeletal Question-naire (SNMQ) [26, 27]. Artisans’ opinion, experience and incidents happened earlier are taken into consideration while studying the associated risk factors. The questionnaire consists of three sections a) Socio-demographic information, b) Occupational/Behavior/Lifestyle Information, and c) Medical/Health (history) information. The first section includes information about gender, age, height, weight, marital status, work experience, shift timings. Weight (digital electronic weighing machine) and height (by height measuring anthropometer) are measured from the standard measuring instruments which were calibrated. From the WHO standards, for adults over 20 years of age BMI (Body Mass Index) (kg/meters2) is calculated as person’s weight divided by square of person’s height. BMI < 18.5 is underweight, BMI between 18.5–24.9 is normal weight and BMI > 25 is overweight. The second section covers the information on workplace adaptability, micro-breaks, body bending and repetitive tasks, stress at work, smoking/ tobacco consumption and drinking habits. The third section has information regarding the overall discomfort of the body, prevalence of MSDs from 7 days to 12 months and their inference in the day-to-day activities. The first section of the questionnaire has multiple choices to record the response of the participants. The second section has ‘yes’ or‘no’ type of responses and the third section has body charts to identify the regions and to record the response related to WMSDs. It also has a Likert scale method of following four choices: comfortable, very comfortable, uncomfortable and very uncomfortable to evaluate the overall discomfort of the body. Data collection and investigation of WMSDs are carried out for both male and female artisans (n = 177).
Data analysis
The response from a subject is entered in the questionnaire form and is coded suitably to analyze with suitable tools. The tool used for this study is SPSS version 20.0. Data analysis is performed using the chi-square test which is commonly used to assess the relationship between independent and dependent variables χ2 test is commonly used to assess the relationship between sociodemographic and workplace factors (independent variables) and reported musculoskeletal complaints (dependent variable) [6–8]. Independent variables considered in this study are socio-demographic, lifestyle/behaviors/occupational information, whereas reported musculoskeletal complaints are considered as a dependent variable. χ2 test results (with 95%confidence intervals) of p < 0.05 are considered statistically significant. Prevalence (%) of WMSDs during the last 12 months and the last seven days were recorded from the participants. The overall discomfort of the body and prevalence of WMSDs in different age groups and based on work experience are examined from various anatomical sites like the neck, shoulder, lower/upper back and in lower extremities.
Overview of typical workplace
Artisans work at traditional and mechanized small-scale units are shown in Fig. 1b. These units are generally characterized by the dusty environment, less floor area, congested workplace, poor ventilation and illumination, no sound/noise proof walls, less hygiene and cleanliness (Fig. 1c). Several thousands of traditional artisan families are engaged in the production of lacquerware toys in South India. Artisans work on the mechanized lathes that are driven by belt drives. The driving shaft is placed overhead which is connected to the small motor through a belt drive. To manipulate the surface, the toy artisans use many types of chisels and files of different sizes and shapes. Artisans sit over the wooden chairs which have no cushion, backrest, headrest, and armrest. Very few artisans in some units wear uniforms and self-protective equipment while performing the job.

Typical lacquerware toy-making unit.

Workspace of artisans.

Colored lac sticks used for coloring the wooden toys.

Tools used to modify the surface of wood.

Colored lac stick is pressed against a work piece to impart the color.
General information
The sample for the study consisted of 177 artisans. 10.2%belong to 24–28 age groups, 39.5%belong to the 29–39 age group and 50.3%belong to the > 40 age group. Mean height, weight and age of the participants are 1615.44 mm, 69.7 kg and 40 years (SD+7.5) respectively. 11.3%have completed elementary level, 27.1%have completed secondary level and 66.1%have no education. 85.31%of artisans in the sample study are married and 14.69%are unmarried. It is found that 42.94%of artisans have maintained good health with no WMSDs history while rest has average health status with a history of WMSDs. 60.45%of artisans are involved in tobacco consumption/smoking and drinking habits and none of them are involved in any gaming activities during their free time. Almost more than half of the study samples have reported that they feel muscle fatigue during working and lack of strength due to routine work. It is found that 67.80%of artisans are underweight, 16.38%are normal weight, and 15.82%are overweight. From the survey, it is found that 20.9%of artisans have undergone various surgeries and 47.9%have taken treatment for minor and major injuries.73.4%artisans have oral health problems, in which 37%of artisans belonging to age group > 40 years have 1–5 missing teeth.12%of artisans of age group 24–28 years have 1-2 missing teeth and 42%of artisans of age group 29–39 years have 1–4 missing teeth. Oral health problems among artisans are due to individual behavior like smoking/drinking and maintaining oral hygiene practices.
Prevalence of WMSDs for 12 months
The body part discomfort (BPD) scale has been used to record the self-reported objective rating of pain feeling [28, 29]. Artisans having symptoms with ratings from 3–5 (1-Not uncomfortable, 2-Barely uncomfortable, 3-Quite uncomfortable, 4-Very uncomfortable, 5-Extremely uncomfortable) are considered as suffering from MSDs. During 12 months, subjects have experienced symptoms in neck (55%), shoulder (60%), upper arm (54%), forearm (38%), hand/wrist (21%), finger (27%), upper back (62%), lower back (45%), hip /buttocks (33%), thighs (37%), knees (45%) and ankle/foot (14%). It is observed that the symptoms experienced by the subjects are more in upper extremities. Table 1 summarizes the overall results of the study which mainly focuses on the factors affecting the prevalence of WMSDs. No statistically significant difference has been found in independent variables such as marital status, height, education, posture training, work satisfaction and work interest. Table 2 gives the descriptive statistics on the prevalence of WMSDs from the last 12 months. Factors like age, seat adaptability, prolong sitting, body bending, repetitive task, stress at work, use of safety devices, Sound/noise proof walls, air ventilation, access to drinking water/restrooms at workplace, tobacco/alcohol consumption, active breaks, BMI, current health and oral health status are found statistically significant.
Association of socio-demographics, lifestyle/health and work-related factors and reported musculoskeletal disorders
Association of socio-demographics, lifestyle/health and work-related factors and reported musculoskeletal disorders
n = 177 n = number of samples; df = degrees of freedom; χ2= Chi-square value; pa = Significant values
Participants’ prevalence of WMSDs in the last 7 days
The highest prevalence of WMSD during the last 7 days is in the sites namely neck (39%), shoulder (55%), upper arm (21%), upper back (55%), lower back (37%) and knees (20%) are shown in the Table 3. It is found that there are fewer symptoms experienced by artisans in ankle/foot (1%), thighs (6%), Hip/buttock (5%), Fingers (5%) and no symptoms are recorded in the forearm (0%) and hand/wrist (0%).
Participants’ prevalence of WMSDs in the last 12 months
Participants’ prevalence of WMSDs in the last 12 months
Table 4 depicts the interference of WMSDs in daily activities. The response consists of 3 choices like Not at all, slightly interfered and substantially interfered with daily activities. Slightly interfered MSDs will cause acute and painful injuries, which can be overcome by involving in physical activities, maintaining a proper food diet and with little medical care. Substantially interfered MSDs will cause chronic and lingering injuries. This type needs intensive medical care. Highest discomfort/pain/fatigue interference is found in different anatomical sites like neck (23%), shoulder (32%), finger (26%), upper back (16%), lower back (27%) and knees (16%). From the study, it was found that there is very little intervention of pain in the forearm, hand/wrist, Hip/buttocks, thighs and ankle/foot in daily activities.
Descriptive statistics in terms of interference of discomfort in daily activities
Descriptive statistics in terms of interference of discomfort in daily activities
Figure 2 shows the prevalence of WMSDs based on the age group. It is determined that age contributes to MSDs in artisans [30, 31]. It can be concluded that WMSDs are predominant in the age group > 40 years when compared to other age groups. For the age group > 40 years, the highest prevalence is reported in shoulder (11%) and lower back (10%). For the age group, 29–39 years highest prevalence is observed in the lower back (14%), shoulder (5%) and neck (5%). For the age group 24–28 years, the highest prevalence is reported in lower back (3%), neck (2%), shoulder (3%) and hip/buttocks (2%).

Prevalence of WMSDs based on age group for 12 months.
Figure 3 shows the prevalence of WMSDs based on work experience. Previous studies show the association of musculoskeletal symptoms with increased duration of employment among artisans [32–34]. Highest prevalence of WMSD is reported in the shoulder, lower back and neck. The highest prevalence of WMSD is present among artisans with work experience 6–10 years followed by > 16 years, 3–4 years and 11–15 years of work experience.
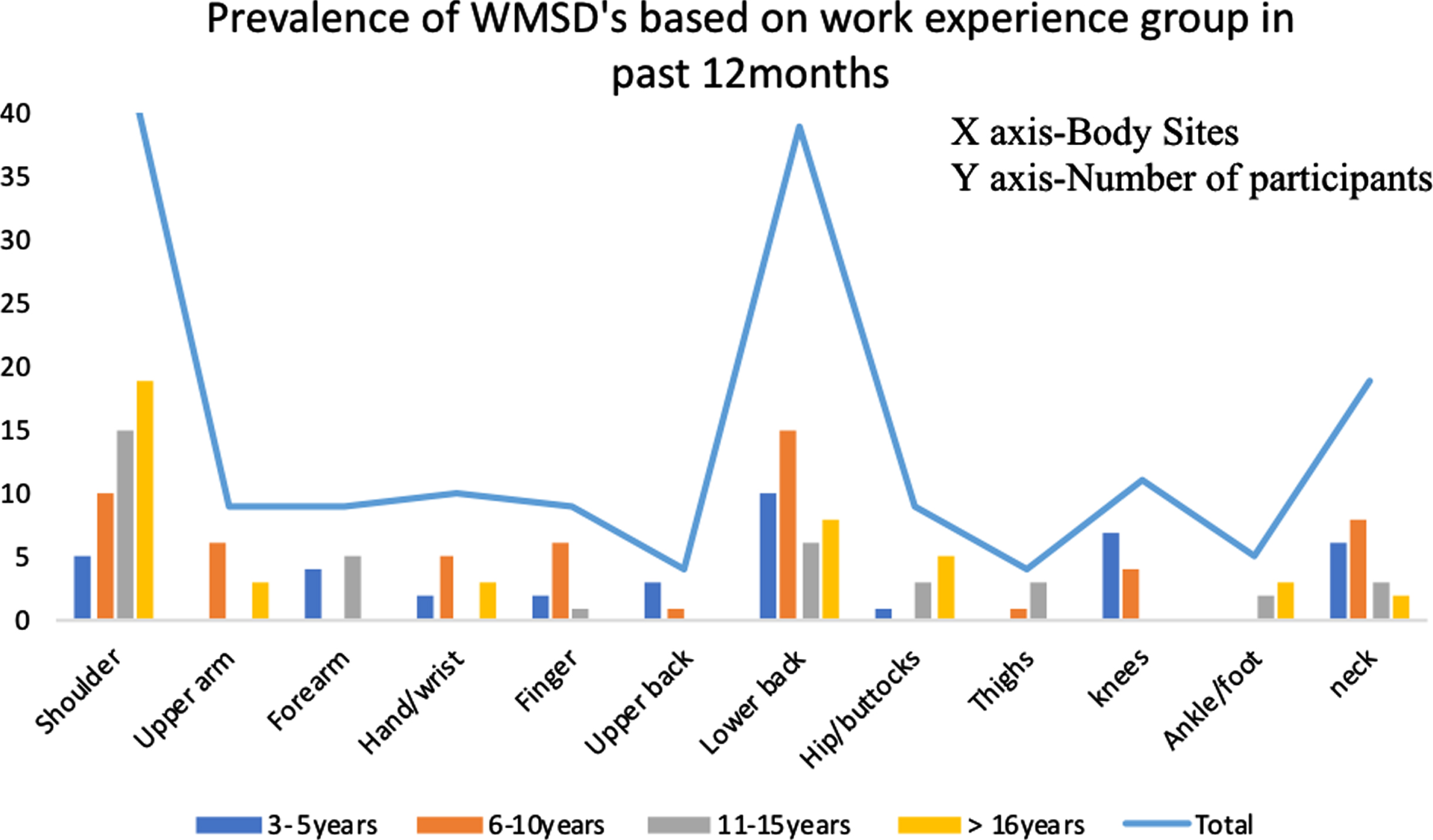
Prevalence of WMSDs based on work experience for 12 months.
Figure 4 depicts the response of the overall discomfort of the body. Responses are obtained based on the Likert scale which has four choices to select. Subjects are also asked to respond by showing the graphical representation of the body. Based on the response, it is seen that neck, shoulder, upper back, lower back, fingers, hand/wrist and upper arm lies in the extremely uncomfortable category whereas ankle/foot, thigh, knees, and forearm lie in the comfortable category.

Overall discomfort of the body in 12 months.
ILO (International Labor Organization) have concluded that the prevalence of WMSDs among workers are the highest number of work related diseases around the world [35]. In the present research work related physical risk factors like performing repetitive task (73.45%), workplace adaptability (71.19%), prolong sitting (73.45%), enough workspace (54.80%), use of protective equipment (55.93%), air ventilation system at work area (68.36%), body bending while performing task (82.49%) and accessibility to rest rooms and drinking water(57.63%) shows significant association with WMSD. Individual characteristics like BMI, age, smoking/drinking habits also show the significant association. Prevalence of WMSD among artisans in past 12 months is higher when compared to last seven days. 62%of participants have reported that they are suffering from LBP in past 12 months. LBP is most common WMSD which is the main reason for reduced work efficiency and absenteeism among workers (36,37). Highest prevalence of WMSD is recorded among artisans belong to age group > 40 years and with work experience of 6–10 years.
Monotonous jobs of artisans make them vulnerable to WMSDs. MSDs have a strong link with insufficient physical activity [38]. Work-related injuries are responsible for high mortality and morbidity in India [39]. The present research shows that none of the participants are involved in any physical activity during their leisure time. World health organization (WHO) recommends adults to involve in physical activity for at least 150 min/week of moderate-intensity exercises or 75 min/week of vigorous-intensity physical exercises [40]. Lack of physical activity in daily life leads to a higher risk of hypertension, diabetes cardiovascular diseases, etc. [41]. Involving in physical activity helps in the reduction of pain in body sites [42]. 70%of the countries globally have an operational physical activity policy, but their implementation is not effective or nil. Many countries have effectively implemented physical activity policy to encourage its people to utilize leisure time [43, 44]. India should also implement the existing physical activity policy effectively for its workers in all the sectors to mitigate the WMSDs.
Both male and female artisans are exposed to physical risk factors in the workplace and are vulnerable to injuries. Similar studies show that male workers are more vulnerable to injuries at the workplace due to aggressive working nature within them [45]. Few studies in developed countries indicated that the risk of occupational injury is higher in men than women [46]. The present study shows that gender has no significant statistical association with WMSDs. Majority artisans in lacquerware toy-making industries are untrained, uneducated and inexperienced with the tools that they are using.
Research in recent years on work-related MSDs has been conducted in different handicraft sectors using self-reported questionnaire and Modified Nordic musculoskeletal questionnaire in India and other countries. They focus mainly on industries dealing with wood carving, stone carving, pottery, metalcraft, jewelry making, Patti work, terracotta, glass painting, etc. Salve (2015) conducted a study on jewelry making artisans (n = 230) and reported that there are visual problems and musculoskeletal disorders among the participants [47]. Khan and Singh conducted a study on Patti workers (n = 100), and the study reported about the prevalence of MSDs in the body sites like lower back (96%), eyes (99%), neck (92%), shoulder (54%), palm (78%) and wrist (89%) [48]. Dianat and Karimi conducted a cross-sectional study on handicraft workers in the carpet, leather and textile industry and reported that more than half of the study samples are affected by MSDs [49]. Sahu et al. conducted a study on pottery and sculptor artisans (n = 130) and reported that the prevalence of MSDs namely low back pain (88%) and neck pain (86%) among the participants [50].
Soongkhang and Laohasiriwong conducted a study on woodworkers (n = 511). The participants reported the prevalence of discomfort in their shoulders (88%) and neck (70%) [51]. Katara conducted a study on stone carving artisans (n = 150) and reported that stone carving is a tiring and long process leading to body pain [52]. Awkward postures in handicraft manufacturing expose artisans to much health risk [53]. Almost all the small-scale handicraft units are family-run businesses in India. To meet the demands, owners or higher authorities of small-scale units force the artisans to work for long hours as their compensation is directly proportionate to production. Long working hours, repetitive tasks and awkward posture of artisan cause fatigue leading to injuries [54]. In the present study, it is found that 60.45%of artisans have tobacco consumption/smoking and drinking habits. Smoking reduces the values of BMC (bone mineral content) in the femoral neck, tibia, lumbar spine and bones of the hand [55]. The lower value of BMC causes osteoporosis which increases the incidence of bone fractures. Tobacco increases the risk of developing vertebral fractures by 32%among men and 13%among women [56]. The present study revealed that oral hygiene practices are associated with MSDs. A greater number of teeth missing is found among artisans who smoke 4 times a day. Previous research has found a positive association between tooth loss and smoking. Dental caries followed by periodontal diseases is the leading cause of tooth loss among artisans. This agrees with the results from the earlier studies [57]. Education records of the artisans in the present study did not show any statistical association with the prevalence of WMSDs. This is because of higher physical risk factors at workplace. Individual factories/units/organizations should adopt reliable techniques to make the workplace safer for their employees/workers. Some studies show the significance association of education level and prevalence of MSDs [58]. Education defines the socioeconomic status (SES) of individual which intern determines the income. The relation between SES and MSDs are less clear but with the health status in general is well established. Toy makers in the present research are belongs to low income category and 61.1%have no education, they couldn’t afford the medical expenses for WMSDs. Education, income level, awareness on health and safety, use of proper tools and techniques can mitigate the WMSDs.
In this study, it is observed that 27%of artisans have a habit of alcohol addiction during the working hours in the daytime. Alcohol addiction shows a positive association with the prevalence of MSDs [59]. Li conducted a study on petrochemical workers and reported that stress at work and job dissatisfaction is associated with occupational injury [60]. In this present research, job stress and job dissatisfaction show a positive association with WMSDs. About 71.19%of artisans are facing problems in workplace adaptability. This issue is related to handling of strenuous hand tools, poorly designed worktable dimension, non-ergonomic chairs, dust accumulated floor area, poor illumination and congested workplace. Similar studies conducted earlier have proved that workplace issues cause WMSDs [61].
Limitations of the study
Most of the references mentioned related to WMSDs among handicraft workers are from the studies conducted in Asian countries. Limitations of the study are as follows: Toy making units selected for this study are family run business, home-based, small and medium scale units. WMSDs are recorded based on the subjective self-report of the participants. Chances of over or underestimation in reporting the WMSDs by the participants since artisans have no prior exposure/experience in similar kind of study. Sampling size selection bias may have led to under/over estimation of WMSDs.
Conclusion and preventive measures
The present study concludes that higher prevalence of WMSDs from past 7 days and last 12 months are found in body sites like neck, shoulder, upper back and lower back. Modified SNMQ, direct observations and statistical analysis provides correct and appropriate validation. 76.8%of the participants reported prevalence of WMSDs in the last 12 months. From the statistical analysis, it was found that most of the work related, lifestyle and individual characteristics considered in the study shows significant association with WMSDs. Further it is important to examine the identified physical risk factors with the tools and techniques to identify the potential interventions that cause WMSDs among artisans.
Toy making units visited during the survey were having sub-standard working environment. Bruises and gashes are commonly found on the artisan’s hands and legs due to mishandling of tools and due to absence of preventive safety measures taken while working over the mechanized lathes. In India, handicraft has hereditary links. In recent times, artisans are fleeing from this sector mainly because of health hazards and low earnings. Handicraft is considered as a nation’s heritage. An attempt is made to identify the physical risk factors among lacquerware toys makers of South India which is uncaptured group and unconsidered in occupation safety monitoring and protection.
WMSDs among artisans can be mitigated by following some of the below steps: Redesigning the artisan workplace ergonomically, which includes: Designing the workstation which is fully adjustable to maintain proper working position. Providing jigs and fixture to reduce muscle strain while handling the tools. Proper design of hand tools and careful maintenance saves muscular effort and has a positive impact on reducing MSDs. Conducting safety and health awareness programs like training, discussions, displaying videos and distributing handouts. Organizing regular health checkups and arranging insurance facilities for artisans. Providing and educating on safety devices like earplug, masks, caps, gloves, eyewear, shoes, uniforms and first aid kits. Providing proper access to restrooms and drinking water. By setting up of regulatory authorities to examine and verify the adoption of workplace safety and occupational health guidelines in the toy-making units of all sizes.
Footnotes
Acknowledgments
The authors gratefully acknowledge the support and co-operation of the staff members and owners of toy-making units in Channapatna, Karnataka and Etikoppaka, Andhra Pradesh, South India.
Conflict of interest
None to report.