
Abstract
BACKGROUND:
Residential support workers (RSWs) provide 24-hour care to clients and many work overnight sleepover nightshifts. Although RSWs perform safety-critical tasks and are at high-risk of work stress and exhaustion, the health and safety of RSWs has not been investigated.
OBJECTIVE:
This explorative workplace case study explored the impact of support work on the eating and driving behaviours of RSWs.
METHODS:
Thirteen RSWs who had worked a dayshift (n = 6) or a sleepover nightshift (n = 7) completed questions on the timing of food intake during their shift, motivations for eating during the shift, subjective work performance, alertness and sleepiness post-shift, and driving performance post-shift.
RESULTS:
RSWs reported snacking during the night on a sleepover nightshift. Time available was the biggest determinant for when RSWs ate during a day and sleepover nightshift. Ratings of subjective alertness and sleepiness after eating were not different between shift types, however participants reported an increase in work performance after eating during a dayshift. Driving events were more frequently reported post-sleepover nightshift, compared to post-dayshift.
CONCLUSIONS:
Findings demonstrate an impact of shift type on eating and driving behaviours of RSWs and highlight the importance of further investigation of this under-researched group to identify appropriate strategies for improving health and safety.
Introduction
The demand for 24-hour services has led to an increasing need for people to work outside of regular daytime hours [1]. This is common in industries such as healthcare, transport, mining, military, and accommodation and food services. However, there are several negative consequences of shift work that impact safety critical tasks [2]. Shift work leads to reduced sleep quality and quantity [1] and is associated with increased fatigue and performance impairments [3–5], particularly during the night, when circadian and homeostatic processes promote sleep [6]. The consequences of shift work on the physical health of the workers include an increased risk of metabolic disorders, insulin resistance, type 2 diabetes, cardiovascular disease, mood disorders, obesity, and gastrointestinal disorders [7–14]. Additionally, shift work is linked to exhaustion, absenteeism, presenteeism, and increased social and family conflict [15–18]. Given these negative consequences, it is imperative for research to prioritise strategies to reduce the burden of shift work and prevent workplace injury and illness.
There are approximately 90,000 disability support workers in Australia [19], however despite the large number of workers in this growing industry, these workers are largely under-represented in the shift work literature. A sub-group of disability support workers, referred to as residential support workers (RSWs), work in group houses with clients of varying clinical profiles who require 24-hour care [20]. RSWs provide direct care to clients and perform tasks such as cooking, cleaning, social support, and administering medications [21–23]. RSWs are particularly vulnerable to burnout, work stress, exhaustion, work anxiety, and low morale [20, 24], in addition to physical and emotional caregiver strain [25]. This can have negative effects on the psychological and physical health of RSWs [26, 27], and can contribute to high rates of turnover, with recruitment challenges identified as a key issue within the carer industry [23, 28]. The quality of services provided to clients can also be negatively influenced by workers that may not be satisfied with their task demand [22, 29], and poor psychological health is linked to poor methods of providing care [30, 31]. Consequently, understanding the challenges for RSWs is a priority area.
It is particularly important to understand the impact of the unique shift schedule required in support work [28]. RSWs work ‘sleepover’ nightshifts, where the RSW is expected to sleep while the client is sleeping [32]. In some cases, this shift is followed by a day off or followed by a subsequent dayshift or evening shift. In an Australian context, sleepover nightshifts feature in the National Disability Insurance Scheme, a government healthcare scheme for people with a disability, with higher wages for employees to ensure quality care is provided to clients [33]. This is indicative of the importance of the workforce engaged in support work and the need for high quality workers. However, only one study has explored the sleep obtained by RSWs on these sleepover nightshifts [32]. It was found that that sleep quality and quantity on sleepover nightshifts can be influenced by several factors, including the assistance required by clients and environmental noise. RSWs reported significantly higher levels of sleep disturbance than normative scores, with large variability in the amount of sleep experienced. On sleepover shifts, despite an average of 7.5 h (SD = 1.2 h) time-in-bed, sleep duration was an average of 5.6 h (SD = 2 h), suggesting that some RSWs may be experiencing sleep restriction during these shifts [32]. Sleep restriction is associated with cognitive performance impairments [5, 35] and increased mood disturbance [36]. Therefore the sleep disturbance on sleepover nightshifts is of concern, as RSWs are performing tasks that require high cognitive function, such as administering medications, as well as interacting with clients [20, 32]. This highlights how the work responsibilities of RSWs can impact their sleep. It is unknown what the wider impact of support work is on the health and wellbeing of the RSWs.
When understanding the long-term health of workers, a key area to investigate are eating patterns at work [37]. Shift workers often have difficulty maintaining typical eating patterns due to their irregular working hours [38, 39], and may eat during the night, when the processes involved in digestion are slowed [40]. This can lead to increased risk of metabolic disorders, and diseases such as obesity, gastrointestinal disease and cardiovascular disease [41, 42]. RSWs prepare meals for clients as part of their on-shift duties [32, 43], however often the demands of the shift duties can lead to poor dietary practices, as reported by a sample of 55 home care workers for elderly clients in France [43]. During the day, this sample reported difficulty finding time to eat a midday meal, occasionally skipping lunch or eating in their car while driving between clients [43]. It is unknown how the demands of a sleepover shift may influence eating patterns. Exploring when RSWs are consuming food during their shifts is a first step in improving health related behaviours at work. It is also important to understand the factors that influence why workers eat on shift [44]. In healthcare workers, work demands and break availability [44–46], in addition to improving alertness [47] and reducing gastric upset [48], have a large influence on the decision to eat during a shift. Investigating whether these are similar for RSWs will be important for ensuring that any recommendations about eating during the shift appropriately consider the reasons that this behaviour is occurring. Further, eating during the nightshift also has implications for work performance on the shift, with increased driving impairment and reduced attention found after a large meal during the night [49, 50].
Driving is an important aspect of support work, as clients may be driven to and from appointments and activities, and the RSWs may drive to and from work [24, 32]. Of particular concern when understanding the safety of RSWs is the commute home. Studies have shown that commuting home from a traditional nightshift, where the worker is awake and working throughout the night, is associated with an increased risk of crashes and inattentive driving [51–54]. In Australia, workers driving home from a nightshift are seven times more likely to be involved in an accident compared to other drivers at other times of the day [55]. This is likely due to the extended time awake following a nightshift [1]. The impact of a sleepover nightshift on the commute home is unknown. However, given that workers may be getting insufficient sleep during the sleepover nightshift [32], and sleep restriction has been shown to impair driving performance [56], we may expect the commute home from a sleepover nightshift to be associated with driving impairments. Exploring the risk on the commute home is therefore important for understanding the work-related safety of RSWs.
To date, no study has explored the wider impact of support work on the health and safety of RSWs, and, given their unique shift schedule and job demands, this is important to consider. The present study investigates the eating habits of RSWs and driving post-shift. A questionnaire was used to determine: (a) the typical timing of eating on shift; (b) the motivations for eating on shift; (c) subjective work performance, alertness and sleepiness after eating; (d) the frequency of driving events post-shift; and (e) the gastrointestinal health of RSWs.
Subjects and method
Participants
The study was advertised via a presentation to those employed as residential support workers at the participating organisation to explain the study and via flyers that were placed on noticeboards at the offices of the organisation. There were no exclusion criteria. The only inclusion criteria was current employment as an RSW at the participating organisation. Ethics approval was obtained from the University of South Australia Human Research Ethics Committee (HREC).
Study design
This study was a cross-sectional descriptive workplace case study conducted in an organisation with a mix of urban and semi-rural locations in Australia.
Measurements
Thirty-seven RSWs expressed interest in the study and were provided with information sheets and questionnaires. Thirteen completed questionnaires were returned. The questionnaire pack was paper and pen-based and given to RSWs in person or sent via mail for participants to complete at their convenience.
Participants (n = 13) completed a package of questionnaires that included demographic information, the Survey of Shiftwork [SOS; 57], the Psychosocial Safety Climate questionnaire [58], eating habits, driving events, and the Perceived Stress Scale [59]. A subset of questions from the SOS and the questions on eating habits and driving habits post-shift will be presented here, with other outcomes analysed elsewhere. In this paper, two shift types are referred to, a dayshift (typically worked between 6:00 am–5:00 pm) and a sleepover nightshift (typically worked between 10:00 pm–6:00 am).
The questions on eating habits were adapted from the food intake questionnaire developed by Waterhouse, Buckley [44]. These questions have been previously used to assess the eating patterns of flight attendants [60], and in the current study these questions are being piloted in an RSW sample.The questions referred to the most recent shift that the participant had completed. Participants were first asked to tick whether they consumed a snack (e.g. apple, chips, cake, and muesli bar) and/or a meal (lunch or dinner type meal) during the 24-hour period that contained the last full shift they completed. Participants completed this every hour and could indicate multiple snacks or meals or leave the hour blank. Participants were then asked whether this was their typical eating pattern during the last year of this shift type and responded using a 3-point Likert scale (1 = yes, 2 = I usually eat more, 3 = I usually eat less). Participants were asked to circle any of the following factors in response to what determined why, what and when they ate during their most recently worked shift: appetite, habit, social interaction, work/break schedule, time available, cost, food available, boredom, level of alertness, cravings, comfort, cultural factors, taste preferences, health considerations, don’t know and other. Participants were also asked to rate work performance, alertness and sleepiness after consuming a meal/snack compared to before, as better, worse, or not different.
To assess the frequency of driving events post-shift, participants were asked to complete a table of driving events that included crash, near-crash, falling asleep at the wheel, missing a turn, hitting the rumble strips, braking sharply, lack of awareness, swerving violently, shouting at another person, resting your eyes, being distracted and pulling over for a nap. Participants were asked to indicate how often they experienced each event, in the last year of driving home from their most recently completed shift, using a 5-point scale (never, once or twice, occasionally, frequently, very frequently). To date, no literature has measured the frequency of driving events in an RSW sample, however questions on these driving events were included in this questionnaire due to these events being frequently reported in nursing samples during the post-nightshift commute [51].
The SOS is a validated shortened version of the Standard Shiftwork Index [57] and is used to measure the impact of different shift systems on the health of the workers. Two subsets of the SOS were included in this research: sleep disturbance and gastrointestinal health. The sleep disturbance questions required participants to respond to statements relating to sleep habits (e.g., “How do you feel about the amount of sleep you normally get?”) by indicating the extent they applied to different shift types using a 5-point Likert scale (e.g., 1 = nowhere near enough, 2 = could do with a lot more, 3 = could do with a bit more, 4 = get the right amount, 5 = get plenty). The shift types were updated to reflect the shifts that RSWs within this organisation can work (morning shifts, dayshifts, evening shifts, sleepover nightshifts and stand-up shifts [an overnight shift where the RSW is required to be awake all night]). There were eight questions related to gastrointestinal upset (e.g. “how often do you have to watch what you eat to avoid stomach upsets?”). Participants responded using a 4-point Likert scale (1 = almost never, 2 = quite seldom, 3 = quite often, 4 = almost always).
Statistical analysis
Data were entered into SPSS version 22 for analysis. Means and standard deviations (M±SD) describing sample age, total work hours per week, and shift work experience were calculated. Proportions of the sample that reported that they were married and living with dependents were calculated. Total sleep disturbance (M±SD) was calculated for sleep periods between successive morning, evening, stand-up nightshifts and sleepover nightshifts. Scores were compared to normative values from a large sample of shift working nurses and midwives (n = 1532) [57]. Normative values were not available for sleepover nightshifts. Mean comparisons of sample participants compared to norms were conducted via Analysis of Variance (ANOVA).
Due to the small sample size, statistical analysis was not possible on the data from the eating and driving related questions. Descriptive statistics were analysed to identify patterns of behaviour and issues for future investigation within this sample.
In order to describe temporal distributions of eating patterns, the timing of meals and snacks that participants provided in relation to their most recent shift was illustrated using radar plots. At the time of completing the questionnaire six RSWs had most recently completed a dayshift (morning or evening) and seven had most recently completed a sleepover nightshift. The radar plots have time (24-hour) around the circumference, and the spoke axis displays frequency (each ring denotes one, two or three meals or snacks). Typical timing of breakfast, lunch and dinner meals [61] have been superimposed on each radar plot.
Also derived from the eating habits questionnaire, to describe the factors that determined why, what and when RSWs chose to eat on shift, the frequency of each factor (appetite, habit, social interaction, work/break schedule, time available, cost, food available, boredom, level of alertness, cravings, comfort, cultural factors, taste preferences, and health considerations) being reported for each shift type, were calculated. Multiple factors could be endorsed for each question. Results were split by the most recently completed shift type (dayshift n = 6, sleepover nightshift n = 7). None of the sample responded ‘don’t know’ or ‘other’ for why, what or when. Results show stacked frequencies for each factor, listed by the most reported factor (combined total across why, what and when).
To assess the impact of eating on subjective work performance, alertness and sleepiness, the data was split into those who had most recently completed a dayshift (n = 6) or a sleepover nightshift (n = 7). The number of each shift type that reported an increase, decrease or no difference was calculated for work performance, alertness and sleepiness. This was illustrated using stacked frequencies.
To describe the frequency of driving events on the commute home, data were again separated by the most recently worked shift type (dayshift n = 6, sleepover nightshift n = 7). The number of participants who had reported each driving event as never, once or twice, occasionally, frequently or very frequently was described for each shift type. This was illustrated using stacked frequencies.
For gastrointestinal upset, the number of participants who had reported each symptom from the SOS questionnaire as occurring almost never, quite seldom, quite often or almost always was calculated. These questions refer to general health and not the most recently completed shift. Data were compared to normative values [57] using ANOVA. This was illustrated using stacked frequencies.
Results
Participant characteristics
Thirty-seven participants were provided with questionnaires, and 13 participants completed the study. There were seven females and six males, aged 27–59 years (M±SD:46.8±10.4 years). The majority of participants (62%) were married/living with a partner, and 46% lived with dependents. Participants had 0.3–27.3 years of experience working in shifts (12.1±7.8 years) and years in the current organisation ranged from 0.25 to six (1.7±1.6). Participants reported 45.6 hours of work per week (±17.7hours), this includes any paid work during the week and is not limited to the support work organisation (five of the 13 participants had a second paid job).
Total sleep disturbance between successive shift types were not significantly different to published normative values [57]. Participants reported total sleep disturbance between successive morning shifts as 18.5±4.4 (M±SD; normative values 18.0±4.1), between evening shifts as 16.6±3.7 (normative values 15.0±3.6), and between stand-up nightshifts as 16.8±2.1 (normative values 19.0±5.1). Total sleep disturbance between successive sleepover shifts was 18.5±3.8 (no normative values available).
Distribution of eating patterns
Figure 1 shows the distribution across a dayshift (n = 6) and a sleepover nightshift (n = 7). Eleven participants indicated that this was their usual eating pattern on shift, and two participants (one from the dayshift sample and one from the sleepover nightshift sample) indicated that they usually eat more. Overall, the sample of RSWs reported 20 snacks and 13 meals.
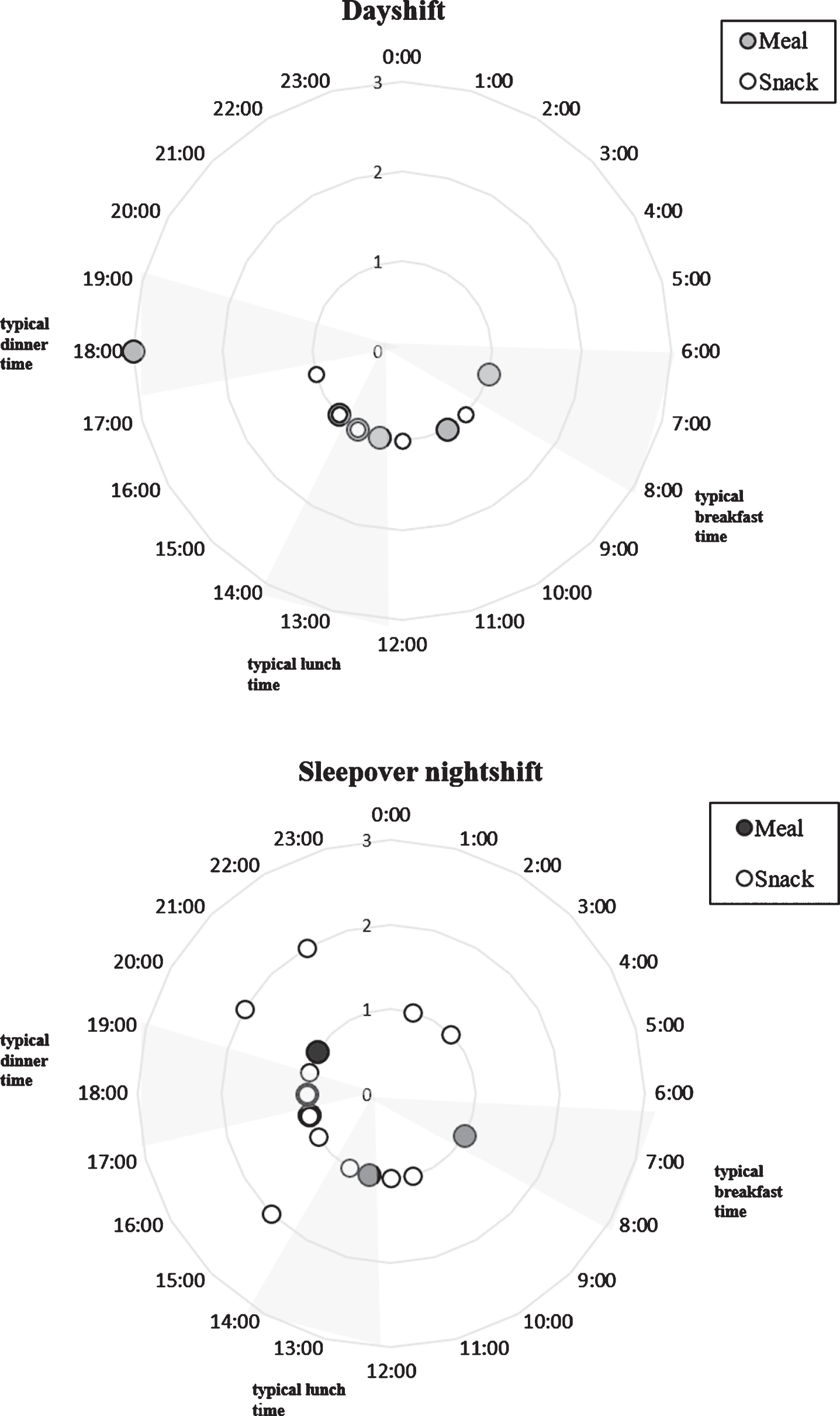
Radar plot showing domicile time (24-hour clock, circumference), by frequency (spoke axis, 1–3 (upper); 1–2 (bottom)) of meals (large filled in circles) and snacks (small unfilled circles). Top panel shows the results for dayshifts (light blue; n = 6) and the bottom panel shows results for a sleepover nightshift (dark blue; n = 7). The frequency represents the total number of RSWs that indicated meal, or a snack at that time. Super-imposed are typical breakfast, lunch and dinner timing [62].
When working a dayshift, all meal and snack consumption occurred during the daytime hours, with the last meal recorded at 6 pm and snack at 5 pm. Participants reported five snacks and eight meals. Five of the 13 instances of snack or meal consumption occurring outside of regular meal timing. A meal was consumed at 6 pm (typical dinner time) by three participants.
During the 24-hour with a sleepover nightshift, snack and meal consumption occurred across the 24-hour period, with snacks consumed during the night hours (8 pm–6 am). Participants reported 15 instances of a snack and five instances of a meal across the 24-hour period. Snacks were consumed during the night, with two snacks at 10 pm and one instance of a snack at 1 am and 2 am. During the daytime hours, nine of the 20 instances of meal or snack consumption occurred during regular meal timing.
Four of the 13 RSWs described what they ate on shift and this included juices and sandwiches (snacks) and pasta, red-meat, and salad (meals).
During a dayshift (n = 6), food available was the most endorsed factor for why participants ate on shift (four out of six participants; Fig. 2). Appetite and food available were the most endorsed factors for what participants ate on shift (four out of six participants). Time available was the most endorsed reason for when food was eaten during a dayshift (four out of six participants).
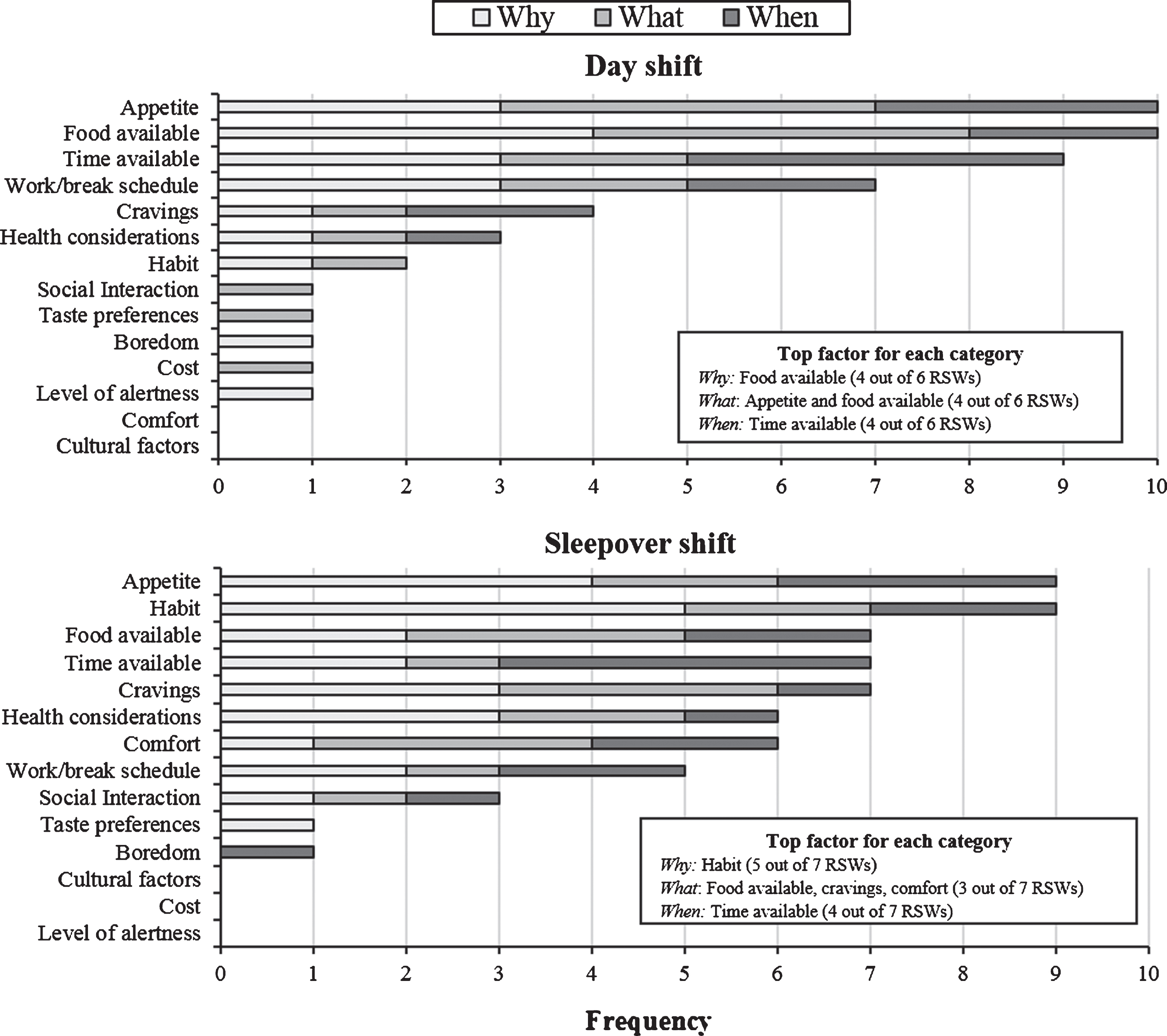
Stacked frequencies of the factors determining why, what and when workers reported eating during their most recent shift, ranked from most endorsed to least endorsed. Participants were asked “what determined [why/what/when] you ate during this shift?” and the factors included appetite, habit, food available, time available, cravings, health considerations, comfort, work/break schedule, social interaction, taste preferences, boredom, cultural factors, cost, and level of alertness. RSWs could endorse more than one factor for each category. The boxes in each panel show the most reported factor for why, what and when workers reported eating. Upper panel shows those that most recently worked a dayshift (n = 6), and the lower panel shows those that most recently worked a sleepover nightshift (n = 7). Factors are listed by most frequently reported to least frequently reported (combined total frequency of why, what and when) for each shift type.
On a sleepover nightshift (n = 7), habit was the most endorsed factor determining why participants ate on shift (five out of seven participants). Food available, cravings and comfort were the most endorsed reason for what participants ate on shift (three out of seven participants), and time available was the most endorsed reason for when workers (four out of seven participants).
Participants who worked the dayshift (n = 6) reported better work performance (four out of six participants) and increased alertness after eating (four out of six participants; Fig. 3). No change in sleepiness was reported after eating by the majority of participants who worked the dayshift (four out of six participants) with one participant indicating they had increased sleepiness after eating and one indicating that they had decreased sleepiness after eating.
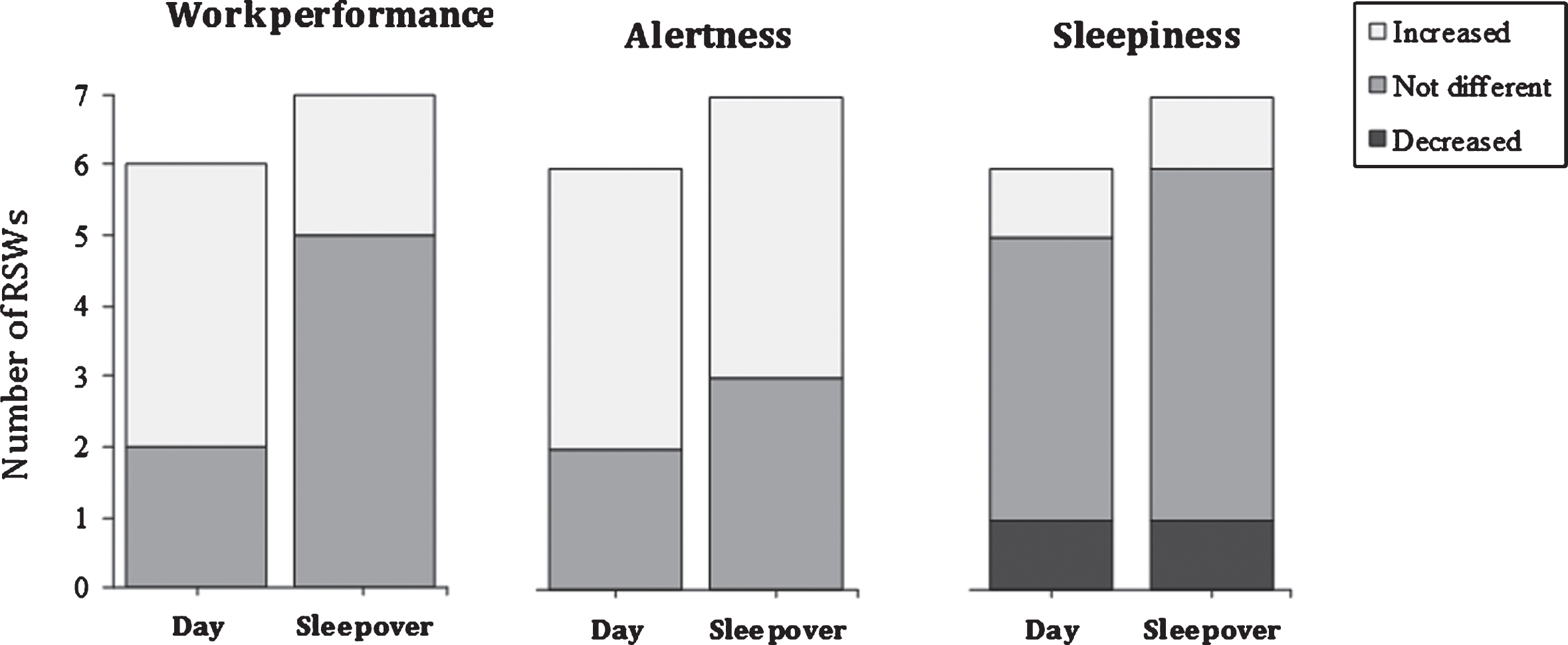
Stacked frequencies of the subjective reporting of work performance (left), alertness (middle) and sleepiness (right) after eating a meal/snack during the shift most recently worked by the RSW. Y-axis shows the number of RSWs for each shift type and the frequency of each response (dayshift [n = 6] or sleepover nightshift [n = 7]).
Of the participants who worked the sleepover nightshift (n = 7), five out of seven indicated that their work performance was not different after eating during the shift, with the remaining two participants reporting better work performance (Fig. 3). Increased alertness was reported by four out of seven participants who had worked the sleepover nightshift, with the remaining three participants reporting no difference in alertness. Most participants reported no difference in sleepiness after eating (5 out of 7 participants), with one participant reporting increased sleepiness after eating and one participant reporting decreased sleepiness after eating.
All participants (n = 13) reported regularly driving home from their shift. On post-dayshift commutes (n = 6) 5 of the driving events were never experienced by participants (Fig. 4). The most reported event was shouting at another person, with four participants reporting an experience of this event occasionally and one participant reporting this once or twice. Being distracted was reported by half of the participants as occurring at least once or twice. Missing a turn, braking sharply, lack of awareness, swerving violently and resting your eyes were each reported by one participant as occurring once or twice.
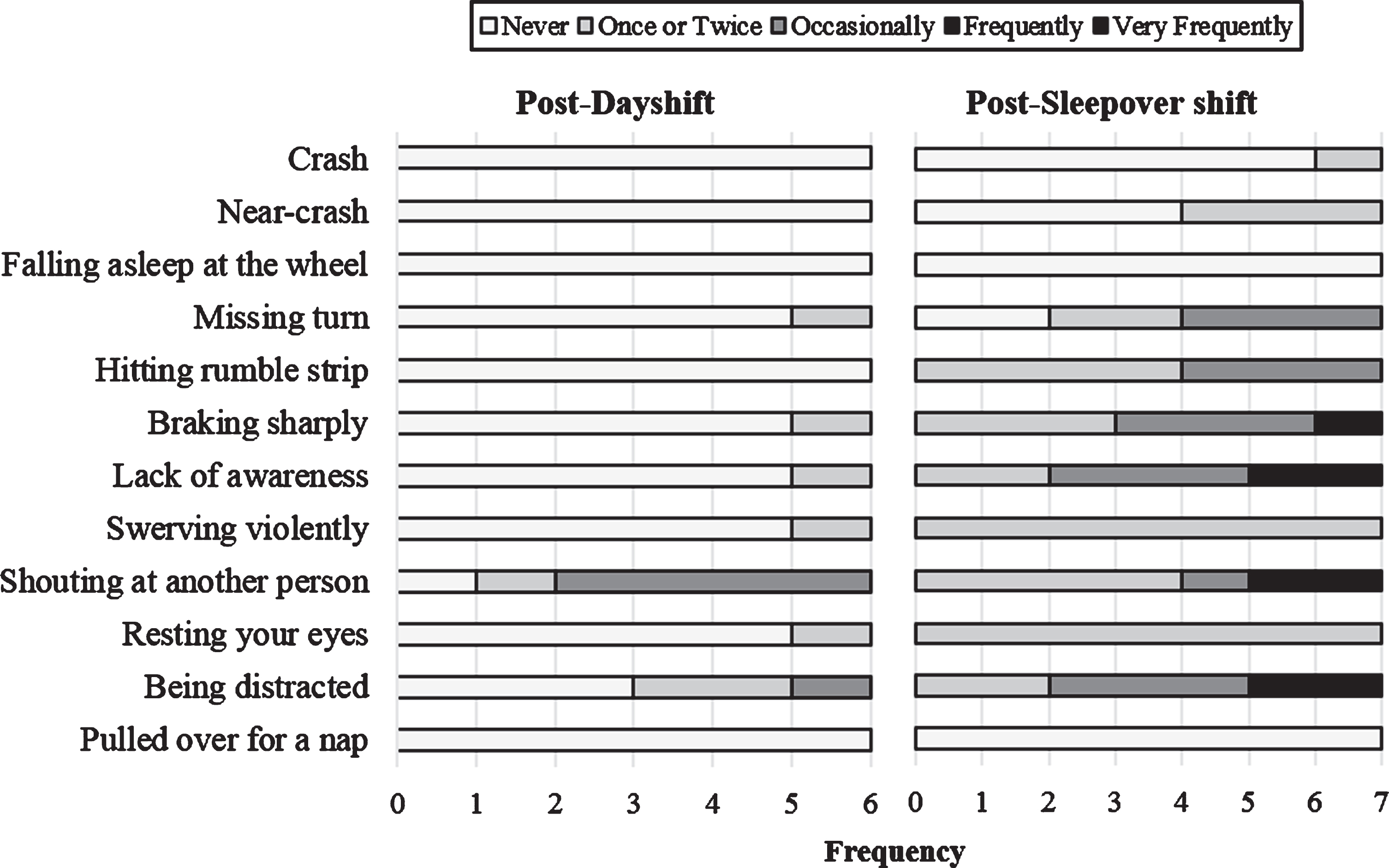
Stacked frequencies of driving events reported post shift for the previous year of this shift type. Left panel shows driving events post-dayshift (n = 6) and the right panel shows driving events post-sleepover nightshift (n = 7). The x-axis shows the 12 driving events and the y-axis shows the frequency shows the frequency of this event within the total sample for each shift type.
On post-nightshift commutes (n = 7) 10 of the driving events were reported as occurring at least once or twice by all seven participants (Fig. 4). Falling asleep at the wheel and pulling over for a nap were not reported by any of the participants. A crash was experienced by one participant once or twice, and a near crash was experienced by three participants once or twice. Hitting the rumble strip, braking sharply, lack of awareness, swerving violently, shouting at another person, resting your eyes, and being distracted were experienced by all participants at least once or twice. There were four events that were reported as occurring frequently by participants; braking sharply (one participant), lack of awareness (two participants), shouting at another person (two participants), and being distracted (two participants).
Within the sample (n = 13), the most frequently reported symptom of gastric upset was disturbed appetite, with only one participant experiencing this almost never and four experiencing this quite often (Fig. 5). Bloated stomach or flatulence was experienced quite often by six participants. Watching what you eat to avoid stomach upsets was reported by two participants as occurring quite often and two as occurring almost always. There was no difference between overall gastric upset in this sample and the normative sample.
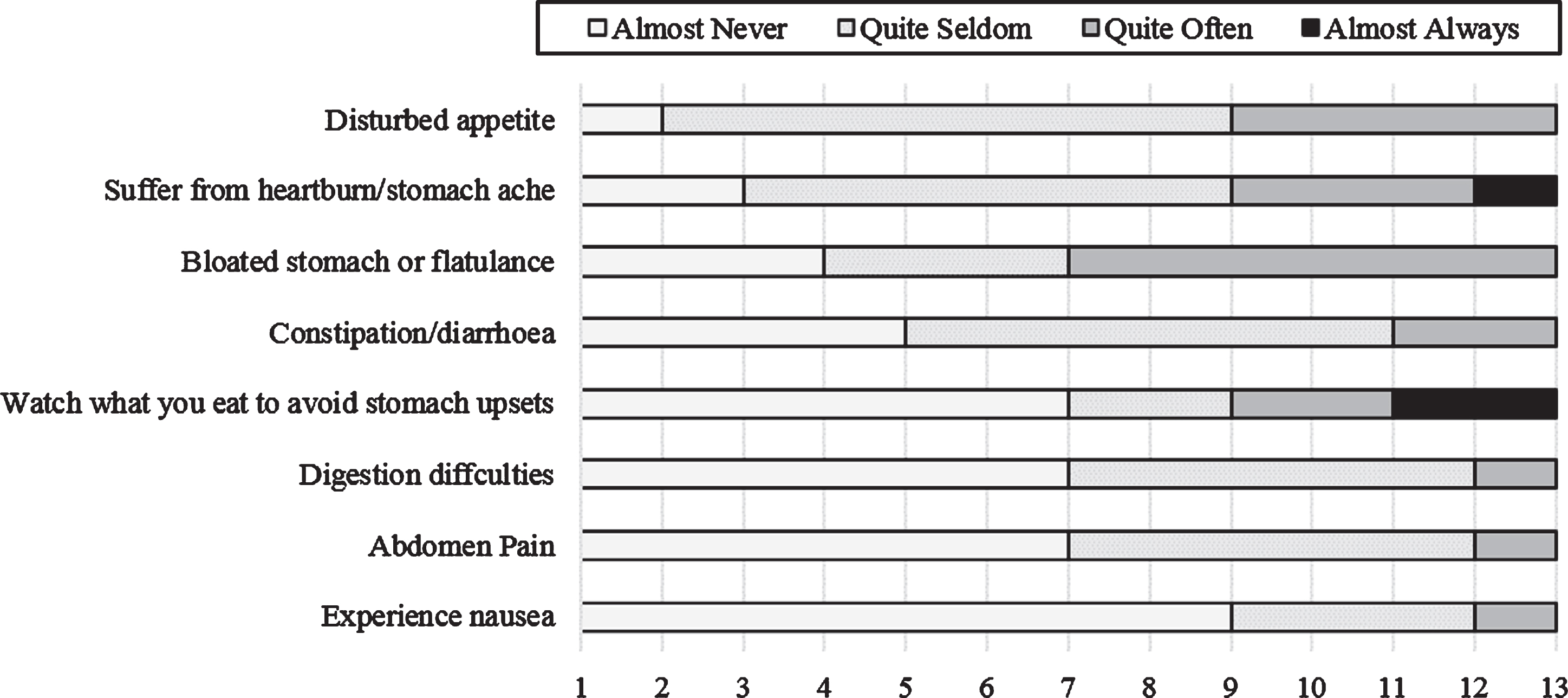
Stacked frequencies of the symptoms of gastrointestinal disturbance experienced by participants (n = 13), ranked from most often to least often experienced.
This study investigated the eating and driving behaviours of RSWs working either day or sleepover nightshifts with the aim to explore aspects of the health and safety in the workplace for this group of under-researched workers. We found that RSWs in our sample appear to be awake during a sleepover nightshift and habitually consuming food throughout the night. Time available influenced when RSWs ate during dayshifts and sleepover nightshifts, and the motivations for what and why food was eaten on shift, in addition to the subjective effects of eating on work performance and alertness, differed between a day and sleepover nightshift. In addition, our results suggest that the commute home from a sleepover nightshift may be associated with a greater risk of driving events than the commute home from a dayshift.
For dayshift workers, during a 24-hour period with a dayshift, food was only consumed during the daytime hours (6 am to 8 pm) and only occasionally corresponded with typical meal timing. RSWs have to fit in time to eat with the demands of clients [20, 43], and this may leave little time for the RSW to consume food. This is supported by the current findings, as dayshift RSWs reported time available as the biggest determinant for when they ate on shift. A previous study has demonstrated this effect of work demands on food consumption within the social care industry, with home carers for elderly clients reporting a lack of time to eat while working during the day leading to meal skipping behaviours [43]. Similarly, those in the health industry often report an inability to have adequate break time due to patient care responsibilities [63–66]. This is problematic, as disrupted eating patterns during the day can lead to poorer health outcomes [37] and has been linked to a greater risk of workplace accidents [67]. In a study by Nea, Pourshahidi [63] workers suggested a need for protected times to eat on shift. Such an intervention may be important to explore amongst a larger sample of RSWs to ensure they have time available to eat during the day and do not have to compromise their health-related behaviours at work.
During a 24-hour period with a sleepover nightshift, participants consumed snacks during the night, and the largest determinant for why participants chose to eat was habit. This suggests that sleepover workers may not only be awake during parts of the night on a sleepover nightshift [32], but also habitually consuming food. Similarly, Waterhouse and Buckley [44] found an increased role of habit in motivating the decision to eat during a nightshift compared to a dayshift. In the current study, appetite was the second largest determinant for why food was eaten on shift. Appetite displays an endogenous circadian rhythm and is decreased during the night [68], however shortened sleep has been linked to increased hunger and appetite due to decreased leptin and increased ghrelin [69, 70]. Perhaps in our sample, RSWs working a sleepover nightshift are experiencing this increase in appetite due to their sleep potentially being shortened by environmental factors in the workplace, such as client awakenings [32]. Symptoms of gastrointestinal upset such as disturbed appetite, suffering from heart burn/stomach ache, bloating and flatulence were reported by participants. This may be due to the habitual intake of food during the nightshift, as eating at night can lead to an increase in gastric complaints [13]. There is also evidence that gastric upset during the night leads to workers altering their eating behaviours [48, 71]. This is consistent with the findings of the current study, as ‘watching what you eat to avoid stomach upsets’ was reported by participants. Given the participants were experiencing gastric upset, reducing eating behaviours at night may be a potential area to intervene when exploring ways to improve the health of RSWs.
Of further importance for the health of RSWs, participants who worked the sleepover nightshift also reported cravings and comfort as determining what they ate. If workers are awake during the night it is likely due to client demand and work stress [20, 32], and work stress is associated with increased food consumption [46, 73]. It is therefore not surprising that participants may be reporting craving and comfort as determining why they chose to eat during a sleepover nightshift. However, this does have implications for the health of the workers. Although data were not collected on what the participants ate, previous literature has demonstrated a link in the health care industry between work stress and eating unhealthier foods, such as chocolate [72, 75].
Overall our findings demonstrate a difference between the eating patterns of RSWs during a dayshift and a sleepover nightshift. Food consumption was restricted to the daytime hours during the 24-hour period with a dayshift, whereas during a 24-hour period with a sleepover nightshift, food was consumed across both the day and night time hours. Further, those working the sleepover nightshift reported greater overall instances of snack consumption. These results are consistent with those of previous studies that have reported that nightshift workers have increased instances of snacking compared to dayshift workers [44, 77]. It is important to note that the nightshift workers in these studies are awake and working at night, whereas participants in the current study are working sleepover nightshifts and are expected to be asleep during the night. Given that workers could be getting fragmented sleep during a sleepover shift [32] there is potentially more wake time on shift where food could be consumed. This may explain why the pattern of eating on a sleepover nightshift is similar to that of a nightshift.
Ratings of subjective work performance after eating also differed between day and sleepover nightshifts. During the sleepover nightshift, the majority of participants reported no difference in work performance after eating. However recent research has found that eating a large meal during the nightshift leads to performance impairments [49, 50]. This is concerning given that RSWs may be awake during the night to assist clients [32]. However, participants in the current study reported snacking during the night rather than meal consumption and it is unknown how snacking during the night can impact performance. The majority of participants reported an increase in alertness after eating. However only one participant indicated that their level of alertness influenced why they ate during a shift. Choosing to eat on shift to increase alertness has been frequently reported in the literature [47, 78], however although alertness is perceived as better after eating, this may not be influencing the eating behaviours of RSWs. Overall, participants reported no difference in sleepiness after eating during a day or sleepover nightshift. This finding could be explained by the findings of a study with shift working nurses, who reported eating on shift as a distraction from sleepiness [66]. It is possible that RSWs may be eating on shift to distract from sleepiness, rather than to alter their level of sleepiness.
Minimal driving events were reported post-dayshift. This what we would expect given that workers are driving home in the early evening, when the wake maintenance zone is promoting reduced sleep propensity [79]. This time of day is associated with improved neurobehavioral performance [80]. In comparison, driving events were more frequently reported by RSWs post-sleepover nightshift. This is consistent with research showing impaired driving performance after a night of restricted sleep [81]. The frequency of driving events post-sleepover nightshift is also consistent with driving events experienced after a nightshift where the workers are awake and working throughout the night [51, 82–84]. Typically, research on the commute home has focussed on post-nightshift drives, however this study has provided evidence that post-sleepover nightshift drives should also be considered when aiming to decrease road accidents.
The findings of this study are limited by the small sample size. This reduces the generalisability of results to a wider RSW population, particularly given that client demand differs between houses and organisations [32]. A larger sample size would allow for a greater exploration of the eating, and post-shift driving behaviour of RSWs, allowing for the differential impacts of house environment and client demand. It would also be useful to compare these results to the eating habits of RSWs during a day off, to see if patterns continue. Further, to reduce participant burden the questionnaire was limited in scope and detail, such as information on what foods the workers ate on shift. Another limitation of the questionnaire is the lack of detail on the length of the commute. Given that it is harder to sustain attention during long commutes and the RSWs may have experienced shortened sleep during their sleepover shift, thus contributing to fatigue and difficulty maintaining attention, the length of the post-sleepover nightshift commute is important to consider as a safety concern in this sample.
To overcome these limitations, future research should continue to explore the health and safety of RSWs. Collecting information on the types of food eaten on shift would be beneficial, in order to create targeted eating recommendations. Future research should aim to investigate the habits of RSWs by adopting methods such as interviews, to allow for the exploration of specific events that may influence eating on shift. Given the questionnaire was provided to participants to complete during their shift, the low return rate may be indicative of the high workload of RSWs on-shift and may represent a methodological constraint for this population group. Future research may benefit from collecting data from and RSW sample outside of shift times. With the aim of increasing safety on the commute post-sleepover nightshift, future research should continue to understand the accident risk post-sleepover nightshift and what countermeasures are used by workers.
Conclusion
RSWs are under-researched in the shift work literature, and this is the first study to explore eating habits and driving post-shift in this population. Overall, findings demonstrate a potential impact of support work on the eating habits and driving behaviours of the workers, and this has implications for the health and safety of this workforce. Given that RSWs are responsible for the safety-critical tasks involved in client care, further research into the health and safety of these workers is important.
Conflict of interest
None to report.
Funding
This project was supported by a University of South Australia Division Research Performance Fund.
Footnotes
Acknowledgments
The authors would like to thank the organisation for allowing this research to be conducted, and a huge thank you to the RSWs involved for their time and effort. Thank you to Darren Gray, Emma Ravet and Kylie Storey for their assistance with data collection and data entry.