
Abstract
BACKGROUND:
To address the quality of life of patients in Permanent Vegetative or Minimally Conscious States, the occupational health of those around them must also be taken into account.
OBJECTIVE:
By analyzing how the available scientific literature has addressed this issue, this study seeks to better understand how caring for these patients affects healthcare professionals’ psychological and health status.
METHODS:
We identified and selected 15 publications from both Anglophone and Francophone databases, i.e., Cairn, Francis, HAL, PsycINFO, PubMed, ResearchGate and ScienceDirect.
RESULTS:
The reviewed publications and studies highlight the difficulties healthcare professionals face with regard to the relationship with patients and their families. Two studies in particular suggest that the difficulties these professionals experience daily can lead to burnout. Other potential burnout factors include the healthcare profession category, the work environment, lack of training and the time spent working with this specific group of patients.
CONCLUSIONS:
Our literature review highlights the institutional and personal resources that may prevent these occupational risks. It also provides avenues for future research.
Introduction
Following cerebral anoxia, traumatic brain injury or an ischemic or hemorrhagic stroke, patients can come out of a coma but fail to recover their original capacities. There are two types of altered states of consciousness: the first is the Permanent Vegetative State (PVS) or unresponsive wakefulness syndrome, characterized by the awakening from a coma but re-maining unresponsive and showing only reflex movements. The second is the Minimally Conscious State (MCS), characterized by the presence of inconsistent but reproducible mediated behaviors [1]. These pati-ents suffer from severe motor (paralysis, spasticity), cognitive (difficult communication) and physiological (tracheotomy, gastrostomy) disabilities. They are extremely dependent and are perceived as patients “alive but who haven’t got a life to live” [2, p.417], “neither dead or dying, but living without manifestations of consciousness” [3, p.33], and have a completely disrupted family life. The day-to-day management of these patients is rather complicated and can lead to psychological distress or even burnout [5]. Moreover, their situation is particularly challenging because it necessitates very specific care which requires healthcare professionals to possess qualities such as “being attentive to others, humility in professional practice, empathy and solidarity” [6, p.76]. In that sense, their activity corresponds to the work of care, which is characterized by concern for others as well as by discreet knowledge and invisible work [7]. The issue of the recognition and working conditions of healthcare professionals who care for PVS/MCS patients therefore requires further attention.
This literature review seeks to identify and analyze the available literature (published between 2000 and 2018 excluded), in an attempt to better understand how working with PVS/MCS patients affects the occupational health of healthcare professionals. We will first focus on the difficulties encountered by these professionals with regard to the relationship with both patients and their families. Second, we will analyze the psychological and health impacts of working with patients in PVS/MCS. We will then highlight the factors of risk and protection and the resources which may help promote the quality of life of these professionals, and thus the quality of life of their patients and their families.
Method
Few studies have focused on the occupational risks of working with PVS/MCS patients. As part of a broader study on the quality of life of patients in a vegetative state, we employed a keyword search using the following Anglophone and Francophone data-bases: Cairn, Francis, HAL, PsycINFO, PubMed, ResearchGate 1 and ScienceDirect. We focused on the keywords “vegetative state” OR “minimally conscious state” AND “anxiety, burden, caregivers, com-munication, depression, emotion, pain, parents, sleep, stimulation, well-being”. We selected articles published between 2000 and 2018 (excluded) that evaluated the difficulties associated with caring for these patients, or the professional consequences on nurses, orderlies, doctors, and rehabilitation personnel. We also selected publications about healthcare professionals working in patients’ homes or in general health facilities or dedicated units. Although there appear to be more publications on family and unpaid caregivers in the literature, they have been excluded from the study. Indeed, we identified a total of 304 publications. As shown in Fig. 1, after excluding publications focusing primarily on the patients themselves or on families and healthcare professionals, we obtained 37 publications including a Master’s thesis describing a qualitative study from the caregivers’ perspective [4] and two conference presentations on the motivation of healthcare professionals presented by the head of a department [3, 8]. Some publications focused on the nature of the care provided (example: Puggina et al. [9]) or on the relationship between healthcare professionals and families (example: Verhaeghe et al. [10]). Owing to the fact that several publications were not directly related to the health and working conditions of healthcare professionals working with patients in PVS/MCS, we undertook a third selection.
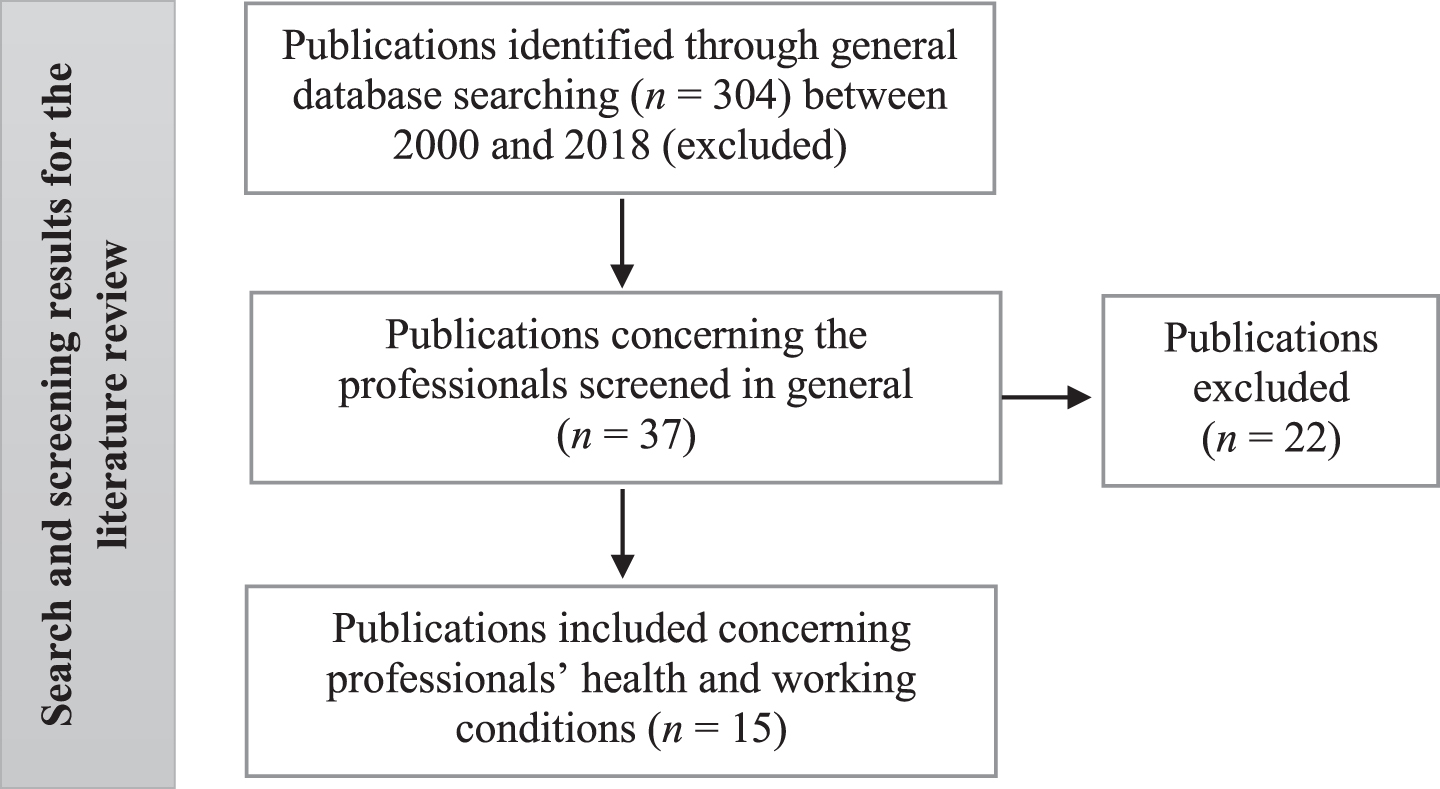
Diagram of search and screening results for the literature review on health and working conditions of healthcare professionals working with patients in PVS/MCS.
A total of 15 publications were selected (case studies, critical analyses, quantitative or qualitative studies). Owing to the few publications identified (Table 1), we also selected three scientific documents (a Master’s thesis and two conference presentations) despite the fact that they did not appear in the data-bases. The survey undertaken by Richer [3, 8] is a good example of the studies that may be difficult to locate and access because they belong to what is referred to as “grey literature”. It must be noted, however, that more than half of the publications were from France. This shows that this issue has attracted attention, including from the French scientific community.
List of the 15 publications concerning health and working conditions of health-care personnel working with patients in PVS/MCS, according to publication type, research method, country and date
Our method consists in analyzing the publications addressing healthcare professionals and classifying them in these five thematic categories. We must point out that these categories have been constructed as the different publications were analyzed. The method therefore involved (1) reading articles addressing healthcare professionals and identifying the topics covered, (2) grouping different themes together and categorizing the most significant themes and sub-themes, (3) five themes were thus selected. In the fo-llowing section, we will present these main themes, which will then be discussed and analyzed. Each of the three authors of this publication independently classified the publications according to the main themes and sub-themes addressed. They then compared the categories identified.
As Table 1 shows, a large majority of the studies selected in our corpus were conducted in Europe (Italy, Netherlands, England, Belgium, etc.). The publications listed are drawn from different sources: field studies, case studies, or critical analyses. In total, two of the fifteen publications are case studies, four are qualitative studies, and six involve quantitative studies. Moreover, the three critical analyses were published in French scientific journals. While some studies have focused on a more specific category of medical professionals such as neuropediatricians [11], the majority of studies have addressed healthcare professionals in daily contact with patients in PVS/MCS. Those interviewed and/or surveyed have thus been “healthcare professionals”, in the sense pro-posed by Mimouni, i.e., “anyone dealing with the patient, including the psychologist” [12, p.63]. This definition includes nurses (predominantly women), orderlies, physicians, physical therapists/speech therapists/occupational therapists, psychologists and social workers. These professionals make up a “team” sharing a base of common values [6] and collective responsibility for vulnerable patients and their families. In this team, nurses who are in contact daily with these patients play a central role [10], particularly in the transmission of information.
The characteristics addressed by the studies in-clude: age, gender (over-representation of women, with more than 75% being female healthcare professionals), profession, work environment (dedicated units, hospitals, rehabilitation centers, etc.), length of experience with special regard to caring for patients in a vegetative state (ex: <4 years, between 4 and 9 years, >9 years) and whether or not this is a first experience [1]. Nationality, marital status, the number of dependent children [13], education, interpersonal relationships with other members of the healthcare team [14], confidence in their ability to take care of these patients, where they trained (current or foreign countries) [14] or even the average number of hours worked weekly [13] are rarely analyzed in relation to occupational risks, despite the obvious interest.
Five main themes have been identified from the 15 selected publications: (1) the specific relationship and communication with patients in PVS/MCS, (2) difficult relationships with families, (3) burnout among healthcare teams working with patients in PVS/MCS, (4) occupational risk factors and (5) resources possessed by healthcare professionals. Table 2 categorizes each publication according to the main themes and sub-themes addressed.
List of the five themes and sub-themes identified from the literature, and primarily addressed in publications
List of the five themes and sub-themes identified from the literature, and primarily addressed in publications
A singular relationship
Healthcare professionals forge and maintain a singular (i.e. unique) relationship with each patient, whom they are expected to consider as a person in his/her own right [15]. However - and we found only one study that reported this - care can be perceived as “aggressive on the senses”, both with regard to odors (“the smell of death”), screams, the sounds of “difficult” secretions and the sight of patients perceived as being in a “state of the living dead”, “dirty”, “disgusting” or with a disturbing, “perverse” look [16] (following a qualitative study on the care of children in PVS by eight pediatric American registered nurses who had at least two years of service). As shocking as the terms may appear, they reflect the nurses’ malaise and their need for help.
A one-way communication model
Beyond the physical strain associated with the state of the patient [15] and with technical aspects, communication remains a major challenge. The difficult communication may be explained by the fact that patients express no desire to communicate with healthcare professionals [12]. A one-way communication model thus emerges. The professional may become a “purveyor of technique” [12, p.65] who does not speak to patients or addresses them in an absent-minded manner. The apparent absence of a subject with whom one can communicate is stress-provoking for healthcare professionals. According to Cohadon [17, p.241]:
It is still possible to establish a relationship with a patient, a relationship that inhabits his/her life, i.e., one that is meaningful for him/her (. . .); We know from experience that as difficult as it may be, one cannot predict the future of such a relationship, and this relationship may evolve into a more conventional form of communication, as limited as that may be.
Communication difficulties were mentioned by 74% of French healthcare professionals interviewed by Richer [8]. The relationship with the patient thus essentially comprises body language [4]. Touch and massages are a particularly important means of access to the patient’s needs and feelings. They are also sources of well-being, relaxation and shared privileged moments for patients. Richer [3] suggests that healthcare professionals should seize a set of non-conventional signs, give them meaning and use them to communicate: respiratory pauses, gazes, gestures, singular spontaneous or reactive motor activities. “Interpretation may help create an intersubjective universe” [12, p.65] and, even when wrong, it is this interpretation that helps the patient to live and allows him/her to be recognized as a “subject”. Richer [3] argues that this is a demanding process for professionals and requires unceasing attention across all levels of care, even though this is almost never rewarded or recognized. This new type of language is a form of knowledge acquired gradually after careful observation [4] and thus requires professionals to allow themselves the time needed.
Ethical considerations
Beyond communication, the ethical challenge is related to the respect shown toward the PVS/MCS patient who families and professionals alike view as a “vulnerable, fragile, and present but inaccessible” person [18, p.31]. These are “patients who have an extremely precarious psychological condition [19] but also a precarious medical, intellectual, social, and emotional condition” [12, p.63]. They thus give healthcare professionals “excessive power” that they may not necessarily be conscious of, i.e., the power to destroy or build the relational process [12]. Respect thus appears as an obvious ethical factor in the relationship between professionals and patients. This is why it is essential to consider the patient as the subject one speaks to as well as the subject spoken about among healthcare professionals [20]. While the need for respect is rarely questioned, it remains nonetheless difficult to implement on a daily basis [18]. Mimouni refers to the “subjective precariousness” [12, p.64] of these patients and argues that there is a need for ethical conduct to prevent them from being considered “rejected subjects” or “objects”. The fatigue associated with patient care, the lack of communication, and even conflict with the family can drive professionals to a state of depersonalization, i.e., an inability to perceive the patient as a person. The professional thus acts like a robot, lacking any human consideration. This is one of the dimensions of burnout and it will be discussed further in section 3.3. Lastly, it is worth noting that there are additional difficulties associated with the doubts and questions of the healthcare personnel, notably regarding the benefit-risk assessment of the proposed treatments [9, 16]. These challenges may increase professionals’ moral distress [16].
Difficult relationships with patients’ families
Healthcare professionals are invaluable insofar as they provide strategies to cope for both at-home car-egivers and families. They may be perceived as “teachers” and they can provide support or even com-passion [21]. Given their lack of training, or the dif-ficult situations they encounter, these professionals tend to categorize certain families as complainers with “incessant” demands [10]. These self-preser-vation strategies simply reinforce the vicious cycle of unceasing and apparently unrealistic demands [22]. Moreover, families are forced to put their trust in the professionals, fueling their constant request for information [10].
Buxton et al. [23] identified a number of problems that may lead to strained relationships between the family and medical staff: language barriers, cultural and religious differences, the sudden emergence of the patient’s disease, parents’ perception of the suffering and pain of their child, misunderstanding of the treatment or diagnosis, an increase in the physiological stress of the family due to prolonged hospitalization and the deterioration of their personal lifestyle (lack of sleep, insufficient nutrition, inconsistent hygiene, etc.), an opaque etiology of the patient’s disease, a previous negative experience with medical staff, many people offering support but with poor communication between them, some family members with psychiatric illness, and financial or transport problems.
Rowe et al. [27] note, for example, that 68% of nurses from all departments of a teaching hospital have already been assaulted verbally by a member of a patient’s family. The cited study also found that in terms of frequency, families were the second group which insulted nurses most. Buxton et al. [23] explain in detail the case of a 12-year-old child in a permanent vegetative state and the conflicts between the family and the healthcare professionals. In this example, the family’s aggressive behavior was related to their difficulty in understanding the diagnosis. Indeed, the family sought to have the girl transferred to a different department after hearing the medical team use the term “permanent vegetative state” to describe their daughter’s state. They said that the nurses could not treat her if they thought she was “a vegetable”. They ultimately attributed their daughter’s stagnant progress, in a rather violent manner, to the nurses’ incompetence.
The tension in the family/healthcare professional relationship may also be considered from the perspective of the difficulties encountered by a disrupted family system facing uncertainty [24, 25]. This may help to explain the loss of confidence in and aggressiveness toward the medical staff. Indeed, the confusion caused by the event’s violence and by the feeling of helplessness may generate suspicion toward the medical staff [25]. The state of shock in which the family is thrust can prevent them from accepting any explanation. This shock is a real stumbling block for healthcare professionals seeking to build a relationship with the family.
Riveted to its hope of improvement, torn between the crushing emotional load of the situation and the desire to avoid cutting all ties, the family will transform its sense of guilt into aggressiveness toward the medical team. This aggression feeds on the suspicion and distrust of medical professionals that emerges right after the patient’s resuscitation. [. . .] The mismatch between the vision of the family of the patient and his/her care and the vision of the team can lead to a total communication breakdown between the two [25, p.237].
Gégout [26] argues that this may be due partly to the changing medical discourse that announces death on the one hand and the possible return to life on the other. This discourse can give way to irrationality and lead to endless hope among family and friends. Discrepancies between staff expectations and those of the family (for instance hoping for an awakening) can thus emerge and become reinforced. In this regard, Mimouni [12] speaks of “optimum fantasy”.
The available literature has addressed relationship problems with families from the perspective of verbal aggression or from that of the criticism levelled against healthcare professionals’ activities. When criticism is leveled against their daily actions, healthcare professionals can become destabilized and begin to question their ideal of “good caregivers”, which empowers them in their functions in dedicated units [28]. Families’ discourses about the practices and approaches of these professionals can notably take on a critical aspect which underscores that the patient remains a “social being”, a member of a network of friends and family relations [29].
Burnout among healthcare teams working with patients in PVS/MCS
Studies on healthcare professionals working in this field essentially focus on burnout. This may be explained by the fact that burnout is a well-known occupational hazard for these professionals, whose roles are based on aiding others [30]. Although some studies have analyzed nurses’ feelings of grief in the face of complex neurological patients, they have failed to provide in-depth information [14]. While depression, anxiety and other symptoms have been analyzed among family caregivers of patients with complex neurological disorders (including those in PVS/MCS), they have been completely overlooked among healthcare professionals. Richer [3, 8], focusing on the factors behind the loss of motivation of the healthcare team, noted reactions of “flight” and “anxiety” arising from feelings of working at the frontier between competence and incompetence. This singular emotional experience had an impact on both the physical and psychological well-being of the professionals and also led to feelings of helplessness and illegitimacy in 159 respondents (30% state nurses, 26% orderlies and 10% therapists). According to this French doctor, team members require motivation in order to draw on their value system and on the department’s project. Leonardi et al. [13, p.349] define burnout as a “chronic stress-induced occupational syndrome”. This professional risk may negatively influence the quality of life of healthcare professionals by generating symptoms of anxiety, irritability, moodiness, insomnia or a sense of failure [1]. It can also lead to a drop in productivity because of absenteeism, illness or physical or psychosomatic complaints and a lower quality of care.
The scientific literature has primarily employed the Maslach Burnout Inventory-Human Services Survey (MBI) [31, 32] to evaluate burnout [13]. Three components of burnout are evaluated: emotional exhaustion, depersonalization and a sense of a lack of personal accomplishment. The level of burnout is estimated as “low” if only one component is affected, “moderate” if two out of the three components are affected and “high” if the three components are pathological.
In the study conducted by Gosseries et al. [1], among the 523 healthcare professionals working with PVS or MCS patients, 18% reported symptoms of burnout (3% high, 15% moderate), 33% reported exhaustion, another 33% spoke of a lack of personal accomplishment and 36% of depersonalization. Another study [13] interviewed 1149 healthcare professionals and social workers working with PVS or MCS patients. The researchers found that 14.4% had a high score of exhaustion, 12.6% of depersonalization and 22% lacked a sense of personal accomplishment. In the latter study, a total of 41.7% of the professionals interviewed had a high score in at least one of the subscales of the MBI. No significant result was obtained in these studies in relation to the influence of gender [1, 13] and marital status [13] on burnout.
Factors of burnout among healthcare professionals of PVS or MCS patients
Some factors lead to a greater risk of burnout than others do. These include one’s healthcare profession, place of work, lack of training, lack of confidence in one’s professional capacities, work experience and weekly working hours.
Profession
Although it is important to pay attention to specific contexts [33], nurses and orderlies seem to be the categories most affected by the symptoms of burnout, given that they are in the front line with PVS or MCS patients and their families and often have intense and prolonged interactions with them. This, for instance, was true for 523 healthcare professionals surveyed by Gosseries et al. [1]. The study found symptoms of burnout in 24% of nurses and 23% of orderlies, compared with 10% of psychologists and social workers. Nurses reported significantly higher levels of depersonalization and lower levels of personal accomplishment than social workers [13]. These levels should be interpreted in relation to the number of patients under one’s care: for instance, Le Moal [28] recommends a ratio of one nurse per three patients and one orderly per two patients in post-acute rehabilitation services in France. However, there is no proof that this is applied universally, in France or elsewhere.
The work environment
There is no consensus on whether working with patients in functional rehabilitation centers or in more durable structures has an impact on burnout among healthcare professionals. While Gosseries et al. [1] suggest that there are greater levels of burnout in perennial structures (nursing homes) than in rehabili-tation centers, Leonardi et al. [13] found no significant differences between these structures. Whatever the case, managing fewer patients per department partly reduces the risk of burnout among these professionals [15].
Lack of pre-service and in-service training
A small number of studies have focused directly on the protagonists’ perception of their training. Baker [14] focused on the needs of English nurses and orderlies working among a broader public, i.e., working with patients suffering from acquired complex neurological conditions, including individuals in vegetative or minimally conscious states. They were 91% and 94%, respectively, to clearly recognize the need to develop a pre-service and in-service training program specific to the department dealing with severely neurologically disabled patients. Future training programs should include knowledge of a number of influences at work in this specific relationship: the influence of the values of healthcare professionals, their emotional processes, their behaviors, the information they possess about the patient; how a specific context influences behavior, their cultures and working practices, and the physical environment [14, 34]. Wade [35] argues that a multidisciplinary specialist team with adequate experience and expertise is required to care for these patients. Lack of training may also explain the loss of motivation among healthcare professionals [8].
Lack of confidence in one’s professional capacities
The lack of confidence in one’s professional skills is related to the little experience in this type of department and to lack of training. As Le Moal states, “the lack of technical training may push agents to draw on their maternal and paternal instincts to treat the sick with as much humanity as possible” [28, p.79], reinforcing the risk of burnout. While a number of studies have analyzed the impact of insufficient training, no direct relationship has been found between training and burnout in this population. However, Mimouni questions the existential or functional inabilities of healthcare professionals, which he defines as their inability to recognize the patient awakening from a coma as a “potential partner in the sharing of internal states” [12, p.65]. He argues that this can transform professionals into “purveyors of techniques” toward patients and lead to depersonalization. In a sample comprising 118 English nurses and orderlies caring for patients with complex neurological conditions surveyed by Baker [14], 80% declared that they had confidence in their skills and professional abilities. However, they said that this resulted primarily from the training they had received at the hospital.
Work experience
It is important for studies in occupational risk to differentiate between the years of service and the length of experience in this type of department. Experience and the number of hours worked per week are supposedly positively correlated to exhaustion and depersonalization [13]. Thus, length of experience not a protective factor and the turnover noted in these departments, which may highlight the wearing down of healthcare professionals, requires further analysis. In the study undertaken by Leonardi et al. [13], the length of experience in the unit was less than five years for more than half of the sample and was seven years on average (between six and ten years for 23.6%, and more than 11 years for 21.5%). While the years of service do not emerge as a risk factor, there have been inconsistent findings with regard to the age of the professionals. Indeed, some studies have found that younger professionals enjoy greater personal fulfillment than older ones, and this may have a protective effect [1]. Other studies suggest that being young and single can be an additional risk factor [13]. Complementary studies may help to reinforce these results in order to allow the implementation of processes to address the professional and personal aspirations of the healthcare staff with a view to prevention.
Time spent with patients in PVS/MCS
Gosseries et al. [1] suggest that among the professionals with symptoms of burnout, including high depersonalization, 68% spent a greater number of wo-rking hours with the patient (27 h +/–13 h) compared with those who had low (18 h +/–14 h) or moderate (19 h +/–13 h) depersonalization levels. A correlation between the weekly working hours and the lack of personal accomplishment and depersonalization was also established by Leonardi et al. [13]. In this study, 80% of the staff interviewed worked between 31 and 40 hours (with an average of approximately 35 and a half hours). That said, a few healthcare profess-ionals put things into perspective by comparing their working time with the commitment shown by patients’ parents, even though the specific context was not clearly defined (intervention in the institution? Home-based care?) [16]. It would be noteworthy to assess whether or not putting things into perspective can produce a protective effect.
The resources of healthcare professionals
Although many studies have focused on how families cope with patients in PVS or MCS, we found no studies addressing the coping strategies professionals caring for patients in this condition implement. The available studies, however, highlight several possible resources that may strengthen the psychological balance of healthcare professionals and thus improve their occupational health. They concern their training, their working conditions, and their external or more personal resources.
Training
Training is the first resource which helps professionals to cope with their daily functions [14]. These training programs are all the more important because new technologies have given rise to new medical requirements [1]. They must be regular [8] and must also take into account a number of elements. For instance, nurses must be trained in the following areas: the management of positive behaviors, handling/transfers, and working with families [13]. The benefits of the verbal communication of healthcare professionals when dealing with patients in a vegetative state and the potential damage of a parallel conversation, often undertaken in their presence with no consideration for them, should also be taught in training programs [9]. Indeed, professionals are rarely aware of the impact of their attitudes on patients’ behavioral reactions [14, 36]. For instance, Puggina et al. [9] point out that a negative conversation can demoralize patients and have adverse consequences on their physical abilities. Knowledge about the complexity of families’ feelings and difficulties is also important in order to interpret the behavior of the members of the family [10]. From this perspective, their need for information should be understood as a need to feed their hope and, as such, must be met with correct information that is comprehensive and as consistent as possible across different staff members [10].
Job resources
Other than the studies conducted by Le Moal [28], we found no studies on the analysis of professional practices. Moreover, although Le Moal mentions these practices briefly, this does not mean that they are not regular practices in these departments. Indeed, these exchanges often make it possible for healthcare professionals to discuss the problems encountered and to promote reflection on problematic situations. Their objective is to help everyone relieve their professional woes, irrespective of whether these stem from the relationship with the patient, the family or from problems with other professionals. Expressed in words, this provides the necessary and desired improvements to the department’s operations. It is worth noting that Saoût et al. [15] cite that among the wishs of the health executives of Maine-et-Loire in France are: an operational support group, pre-service and in-service training, meetings with healthcare professionals from other institutions, and moments allowing harmonization with family members. Also mentioned are discussions with external teams perceived as a source of motivation by the healthcare professionals interviewed by Richer [3, 8]. These different moments of discussion and training thus appear to be valuable for these professionals. According to Gosseries et al. [1], psychological support is essential, and more so to support older professionals in their personal accomplishment and improve their well-being and therefore the quality of their care and their productivity; 49% of the professionals interviewed by Richer [8] stated that this support was essential.
It is essential for these professionals to promote clear and coherent communication that incorporates the views of families in order to increase confidence and mutual understanding in this situation [23]. The family/healthcare professional communication must be regular to avoid the risk of conflicts [37]. It must also allow some form of recognition of family caregivers as experts in the care of their loved ones [16]. It is under such a condition that a relationship of trust may be established with all involved parties. Most conflicts can be resolved if protagonists make an effort to understand and respect each other [36, 38]. Psychologists, conscious of the “dynamics and power” of the reorganized family system, can act as a link between families and caregivers, but they need the commitment of the entire medical team [26]. Moreover, in an attempt to be reassuring, a healthcare professional may be designated as a referent for the family and employ a proactive approach to identify its issues of concern [23]. It is also the nursing management’s role to allow everyone - patients, friends and relatives, and healthcare professionals - to grow within a reassuring framework in which reference persons and procedures are as accommodating as they are motivating [28]. Staff rotation may also have a protective effect: 52.6% of the professionals interviewed in Leonardi et al.’s study [13] had been working in these units for less than five years.
External or personal resources
Lastly, on a more personal level, having a support network within and outside the department, participating in personal activities to recharge one’s batteries physically, morally and spiritually, and having spiritual practices and beliefs may help healthcare professionals find (or find once again) balance in the face of the difficulties of their duties [16]. Taking hindsight and putting things into perspective are also options that make it possible to perceive the positive aspects of one’s life and to find meaning in the patients’ state [16]. Drawing on in-depth interviews conducted with eight pediatric nurses working with children in a vegetative state, Montagnino et al. [16] show that because of the presence of children in these services, some nurses develop gratitude with regard to their own lives and this allows them to deal more easily with the injustice of the fate invested in these children.
Discussion
While the challenges encountered by healthcare professionals working with patients in a vegetative or minimally conscious state are unanimously recognized, few studies have sought to address them and find possible solutions. Difficult care (physical or unpleasant tasks) and increasingly technical tasks, problematic communication (often one-way), the respect one must have for these patients, and conflicts and the aggressiveness of families can cause psychological suffering which can lead to burnout.
This literature review underscores that while the challenges encountered by healthcare professionals working with patients in a vegetative or minimally conscious state are recognized, few studies have sought to address them and to find possible solutions. The review highlights two main issues which we discuss below: (1) The first concerns the recommendations that may help guide future research and thus complement this overview with regard to the challenges these professionals encounter and the potential solutions. (2) The second concerns practical guidelines that go beyond organizational and collective risk prevention measures. Lastly, we present the limitations of our literature review in order to contribute to future studies on this theme.
Future research avenues
The 15 publications selected provide avenues for future research. First, while two studies have ana-lyzed burnout [1, 13], other health-related conseq-uences have received little attention. These publications reveal several factors related primarily to the work context and likely to favor the onset of burnout. Moreover, further research is required to understand the interplay between the burden perceived by family caregivers and the experience of burnout among nurses [13]. Indeed, how may the suffering of family caregivers, which can be expressed via direct aggression, via feelings of persecution projected onto healthcare professionals, and/or via depression and the loss of a driving force, impact the experiences of these professionals and increase the risk of burn-out? Put differently, can the psychological impact of the former induce a downward spiral for the latter and thus for all parties involved? Moreover, we found no studies on the significance of the support healthcare professionals may provide for one another. This may be explained by poor relationships, a lack of shared values, or other possible reasons. However, there is no doubt that a negative atmosphere and issues such as rivalry within the department have an impact on the professionals’ quality of working life and therefore on patients’ and their families’ quality of life. A team must be strong and united to fulfill its duties to patients and their families, and it should also cultivate serenity in order to deal with these extreme situations [6]. Other potential avenues for research could also focus on the relationship between the existence of a common project within departments, and training or special education programs targeting professionals, and activities to boost team motivation for all education and healthcare teams.
Practical guidelines
Alongside personal resources specific to each professional, institutions may implement organizational measures to improve the working conditions of professionals working with patients in PVS/MCS. These may include: training, keys to understanding the communication with families, analysis of practices with an opportunity to express daily feelings and professionals’ anxiety, psychological support.
Other than the organizational and collective risk prevention measures, other practical guidelines em-erge from the literature. Beyond the physical strain associated with the state of the patients in PVS/MCS [15] and with technical aspects, communication re-mains one of the major challenges for healthcare professionals. Respect is a second challenge. Mallet et al. [39] offer some practical pointers to help professionals effectively develop a healthcare and assistance process with tact, creativity, openness and mutual respect. In particular, this implies avoiding a professional/patient relationship that is heavily focused on legal information and law enforcement. Healthcare professionals should be able to privilege the joint construction of a scenario in which there is room for each actor.
Damaged by aggressive families, unconsciously used as a stage on which to project negative emotions, and possessing a legitimacy constantly challenged by the patient, the members of the healthcare team may also experience great psychological suffering reinforced by their sense of powerlessness in the face of medical decisions [16]. Buxton et al. [23, p.171] give advice to prevent divisions among team members following the bashing a professional may receive from the family: “to identify contributing factors, hold a team meeting to come to a shared understanding of the issues, consult appropriate services to assist in the experience of care, and find ways for staff to work with parents”. Finding the right distance is necessary but it may not always be easy [18]. Moreover, the incessant quest for information from nurses - notably with regard to prognosis and treatment, daily care, the department, the equipment and what the family members can do for the patient during the visit - generates anxiety and intense distress among family members. This may affect caregivers when they are unable to provide this information or when they underestimate its importance for the family [10]. Some institutions offer very factual brochures for families, which, in addition to considering the characteristics of these states, also advise on how to deal with the patient, the need for family members to have centers of interest other than the patient, and the problems other families in a similar situation have encountered. They focus on the experience of the healthcare staff and their confidence in this staff [40], providing a first source of reassurance for the family and thus preventing misunderstandings that are often sources of future conflicts.
Personal resources can also be developed within a therapeutic and/or institutional framework. Given the impact on their health and on the quality of their work, it is necessary to take into account healthcare professionals’ malaise, including anxiety-depressive disorders and stress, and to try to put preventive measures in place.
Moreover, for these healthcare professionals, it is also an issue of maintaining close ties with the family despite the suffering and uncertainty of the situation. As Puggina et al. argued, “Considering the hope of the members of the family and the associated need for information as a natural process enabling them to deal with the situation encountered is one way to show full respect for individual members” [9, p.268]. The medical staff’s objective must be to give the family a sense of continuity and control [10]. Anything that helps reassure a family eases family/healthcare professional relationships and protects all parties involved.
Limitations of the literature review
While our literature review has enabled us to review and synthesize the body of literature around professionals working with people in PVS/MCS, it is clear that few studies have addressed this subject. The paucity of studies undertaken outside Europe may reflect not only a lack of recognition but also general ignorance of the role of healthcare professionals caring for PVS/MCS patients. This explains why we have expanded our research and taken into account unpublished studies written in French because of their focus on healthcare professionals’ views [3, 8]. While this choice was enabled by our in-depth knowledge of the Francophone context (and the associated grey literature), it may present a risk of bias with regard to the selection of publications. This bias may explain in part why we were only able to identify critical reviews undertaken and published in France.
Conclusion
Our literature review focused on the difficulties encountered by healthcare professionals working with PVS/MCS patients. It highlighted the singular relationships established between those giving and receiving treatment. These relationships are marked by a lack of communication that may lead to tension with patients’ families, as well as to burnout and mal-aise among those working in these professions. Our synthesis also reveals a need for research on issues other than burnout, such as mixed anxiety-depressive disorders and stress. After discussing the risk factors that may induce it, we have summarized the resources proposed in the scientific literature. Despite the dearth of articles on the risks professionals working with patients in a vegetative state face, our review has established a list of resources and concrete measures to prevent these occupational risks. In this sense, this synthesis provides a global vision of potential and directly operational measures to improve the conditions of these healthcare professionals.
Conflict of interest
None to report.
Footnotes
Acknowledgments
We would like to express our thanks to the U.N.A.F.T.C. (Union Nationale des Associations de Familles de Traumatisés crâniens et de Cérébro-lésés - local family associations of head injury and brain damaged persons grouped in a national union) represented by Doctor Philippe Petit and Ms. Suzanne Aubert, the France Traumatisme Crânien association (association of health professionals working in trauma) represented by Doctor François Tasseau and Professor Eric Vérin, the CNSA (Caisse Nationale de Solidarité pour l’Autonomie - National Solidarity Fund for Autonomy), the FIRAH (Fondation Internationale de la Recherche Appliquée sur le Handicap - International Foundation for Applied Research on Disability), the Foundation of “Gueules Cassées”, the Foundation and the Great Research Networks of Upper Normandy for their financial assistance, which enabled us to undertake this study.
Social network where authors make their articles available.