
Abstract
BACKGROUND:
Surgeon’s hands are exposed to a range of chemical and physical stressors that influence the integrity of gloves. Thus, glove perforation facilitates pathogen transmission through the holes. Numerous studies have shown that glove perforation is of great importance, but there is still no complete consensus.
OBJECTIVE:
This study aimed to investigate the safety conditions of surgical gloves based on the incidence of glove perforation among surgical teams.
METHODS:
A literature review was conducted by searching PubMed, Embase, Scopus, ISI, and ProQuest databases. The incidence of glove perforation was reviewed in eight categories. A total of 580 articles were found in the initial search.
RESULTS:
109 articles containing 130 datasets were analyzed. The overall incidence of glove perforation was 14.44 %. Surgeons had the highest incidence of glove perforation (23.09 %). An increase in the duration of surgery increased the odds of perforation. It was found that 68.58% of the glove perforations were not identified by practitioners.
CONCLUSION:
Despite major advances in the design of surgical gloves, the issue of safety and integrity of gloves has not improved. Due to the high incidence of surgical glove perforations, most of which had not been identified, it is imperative to consider strategies to minimize the incidence of perforation. The results of the present study can be used to integrate information related to the rate of perforation of surgical gloves in different surgeries.
Introduction
Operating rooms are high-risk environments and one of the most important hospital units where professionals are directly exposed to blood and body fluids. Exposure to blood or body fluids of infected patients can lead to dangerous diseases, such as hepatitis B and C or AIDS [1, 2]. According to Prus-Ustun et al., 16,000 cases of hepatitis C, 66,000 cases of hepatitis B, and 1,000 cases of AIDS might have occurred among healthcare workers around the world due to occupational exposure to blood and body fluids in 2000 [3]. One way to reduce the transmission of these microbes is to use medical gloves [4]. Gloves are considered to be a barrier that can prevent the transmission of microorganisms from operating room staff to patients and from patients to surgical team members and are of equal importance to the antisepsis of surgeons’ hands [5, 6]. However, tears and micro-perforations may occur, causing patients and members of the surgical team to be exposed to several complications [7, 8]. Breaking this barrier will certainly increase the risk of exposure to contagious diseases [9, 10]. In 2017, Dorcheh et al. reported that the risk of viral infections due to needle stick damage in surgical gloves was 0.3 %, 6–37%, and 1-2% for AIDS, hepatitis B, and hepatitis C, respectively [11].
Glove perforation exposes surgical team members to many diseases. In fact, by making holes in gloves, microbes find a passage through hands [12]. In 2018, Lee reported that approximately 14% of surgeons stated that the gloves were perforated and that perforating gloves significantly increased the number of microbes in surgeons’ hands [13]. Studies have also shown that glove perforation could reach 50% depending on the type of surgery [14].
Because of the high importance of the issue, numerous studies around the world have investigated the problems associated with surgical gloves perforation and the efficiency of using double gloves. Despite numerous reports about the high risks of surgical gloves perforation, most practitioners in operating rooms tend to underestimate the dangers of glove perforation and the important role of double gloves in minimizing contamination [7]. Surgical team members, especially surgeons, prefer not to use double gloves because it may reduce touch sensitivity. Surgeons prefer to do their work easily and skillfully even if they are not adequately protected [15, 16]. More importantly, surgical team members often do not notice that gloves are perforated and many perforations are not detected even after the gloves are removed [17–20]. This increases the likelihood of the risks that the surgical team is exposed to [21].
Numerous studies, as well as different glove configurations by surgeons and surgical team members, have shown that the issue of glove perforation is of great importance and there is still no complete consensus. Therefore, this systematic review and meta-analysis aimed to investigate the safety conditions of surgical gloves based on the incidence of glove perforation among the surgical team by integrating the results of the previous studies.
Methods
The present study was a systematic review and meta-analysis of the incidence of surgical gloves perforation in operating rooms. This study was designed in 2018. The method of reporting in this study was based on the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) checklist.
Search strategy
In December 2018, five international databases, namely Medline/PubMed, Scopus, Embase, ProQuest, and Web of knowledge/ISI, were reviewed. The selected keywords included three categories; i.e., 1) perforation (perforation, integrity, glove perforation, bacterial passage, glove perforation rate, and barrier integrity), 2) surgical glove (surgical glove, double gloving, surgical gloves, medical glove, medical gloves, glove, single gloving, and protective gloves), and 3) safety (safety, infection, and patient safety). The search strategy is described in the supplementary data. The collected data were entered into the EndNote X7 software and duplicate articles were automatically deleted. It is noteworthy that the articles were reviewed by two researchers separately.
Inclusion and exclusion criteria
The studies specifically focused on surgical gloves and performed on surgical team members were included in the study. Studies performed in dental settings or focused on examination gloves were excluded. Review studies, non-English studies, and the articles that did not measure the incidence of perforation were excluded, as well.
Quality assessment
Joanna Briggs Institute Checklist was used to check the quality of the articles. The tool consisted of eight questions responded via ‘yes’, ‘no’, ‘uncertain’, and ‘no use’ options. The tool aimed to evaluate the methodological quality of the studies and ways to access and understand errors in the design, implementation, and data analysis.
Screening studies
Initial searches, screening of studies, extraction of results, and evaluation of the quality of the articles were conducted by two researchers. If there was a disagreement between the two researchers, the team leader would make a final comment on that article.
Statistical analysis
Heterogeneity among the studies was assessed by the Cochran test (significance level < 0.1) and its composition was evaluated using I2 statistic (significance level > 50%). In the case of heterogeneity, the random effects model was applied by the inverse variance method and in the absence of heterogeneity, the fixed effects model was used. Odds Ratio (OR) was used to compare the incidence of glove perforation based on the time of surgery. That way, the operation time of less than 30 minutes was set as a comparison (reference group) and glove perforation incidence at this time was compared to that in other times. The inclusion criteria for each study included reporting at least two times, one of which must have been less than 30 minutes. Meta-regression was used to investigate the relationship between quantitative variables and the incidence of perforation. To investigate the cause of heterogeneity in the studies, subgroups were evaluated based on job type and Human Development Index (HDI, a composite measure of success in each country based on three basic criteria of human development, including ‘long and healthy life’, ‘access to knowledge’, and ‘a standard of living’). In this index, countries are compared regarding educational, health, economic, social, environmental, political, etc. indicators). All analyses were performed using the STATA software, version 12.
Results
Description of literature search
After searching the international databases, 580 articles were found. After filtration, 109 articles were included in the final analysis. It is worth noting that some studies reported the incidence of perforation in several types of surgery or different types of gloves separately. As shown in Table S.1. of the supplementary data, some studies have been reviewed separately due to the presence of several sets of results that were independent of each other. There were 109 articles in this study, but 130 datasets were extracted from them. The flowchart of the studies has been shown in Fig. 1.

Flowchart of the included studies in the systematic review.
The characteristics of the studies have been listed in Table S.1 in the supplementary data. Of the 109 articles included in the present study, the USA and UK had 23 and 22 studies, respectively. There were eight studies from Brazil and six from Germany. Finland and Italy each had five studies. Besides and India each had four studies. Additionally, Australia, China, South Korea, Nigeria, Thailand, and Turkey each had three studies. Saudi Arabia, France, and Japan each had two studies. Finally, Denmark, Tunisia, Scotland, South Africa, Norway, Oman, Iran, and Spain each had one study. In the studies included, standard methods (EN-4551, FDA or ASTM Water leak test of medical gloves) were used to identify holes and perforations in gloves. The methods of all studies were almost the same. Various surgeries were present in these studies. One study had examined animal-related surgeries [22].
The results related to the evaluation of the quality of the articles
In the questionnaire used for evaluating the quality of the articles, the number of positive responses was counted and the articles were classified into three categories as follows: low quality (scores 1 and 2 out of 9), average quality (scores 3 to 6 out of 9), and high quality (scores 7 to 9). Three studies were of low quality, 15 were of medium quality, and 91 were of high quality.
The results related to the heterogeneity of studies
High heterogeneity was observed in the results of the studies. The results of meta-analysis indices (Q, 95% CI, df, I2), p-values, and the overall incidence of perforation for all study variables have been presented in Table S.2 in the supplementary data.
The results of the meta-analysis
Overall incidence of glove perforation
Out of the 130 datasets extracted from the 109 studies, 89 reported overall perforation. The overall incidence of perforation (95% confidence interval) was 14.44 % (12.94% –15.93%). The overall incidence of glove perforation.
Based on Fig. 2-a, 14 studies reported the incidence in ‘single-layer gloves’, 20 studies reported the incidence in ‘double-layer gloves’, 22 studies reported the incidence in ‘double layer and single layer gloves’, and two studies reported the incidence in ‘triple-layer gloves’, with the incidence of perforation (confidence interval) being 12.39% (15.81% -8.98%), 13.65% (16.51% -10.80%), 12.62% (9.44% –15.80%), and 5.20% (7.10% -3.29%), respectively. However, 31 studies did not report glove configu-ration.
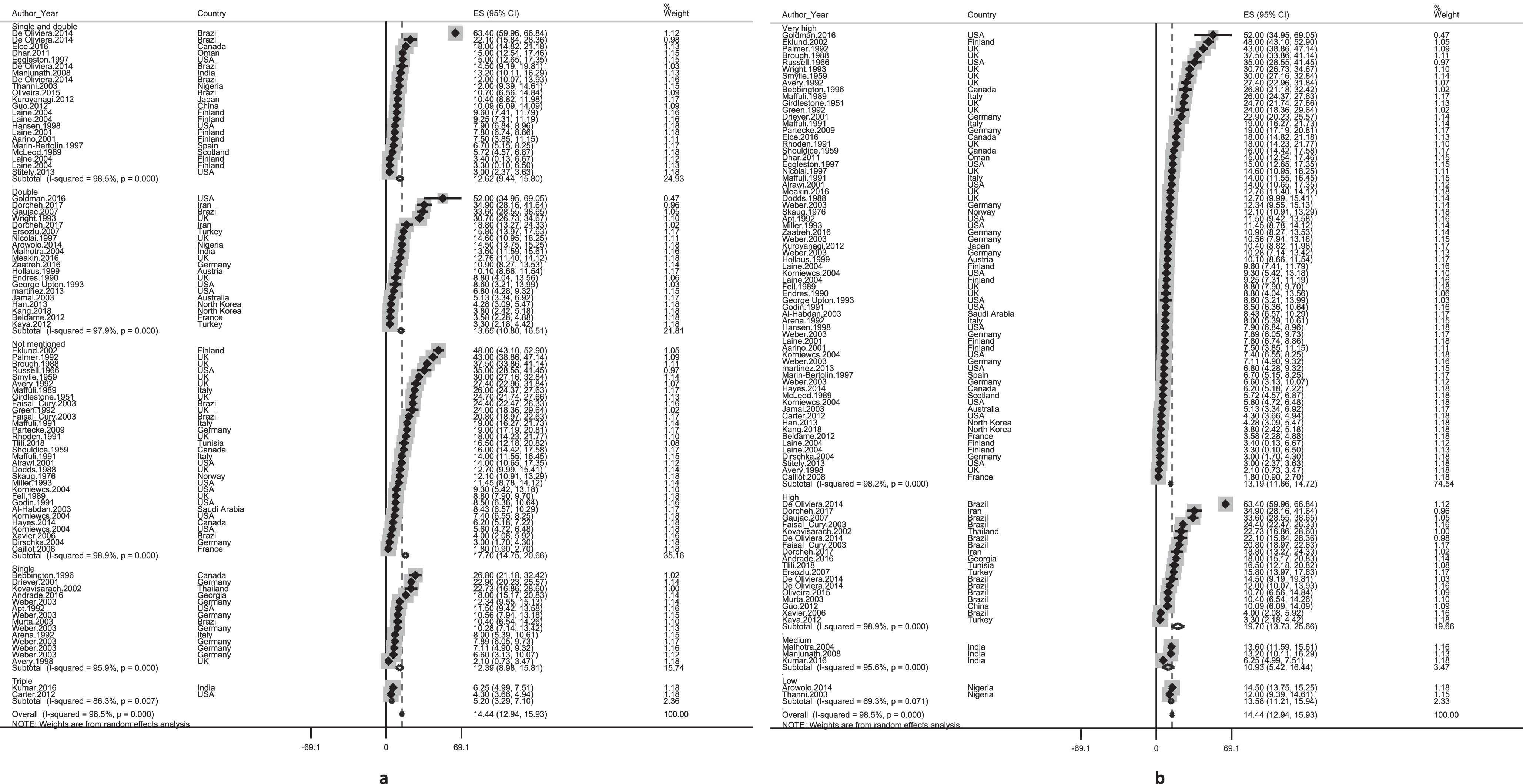
The incidence of overall perforation amongst the included studies categorized by (a) glove layers and (b) Human Development Index.
The highest perforation rate; i.e., 19.70% (25.66% -13.73%), was observed in the countries with high HDI (Fig. 2-b).
Based on the job group, the highest incidence of overall perforation (confidence interval) was 16.28% (19.07% -13.48%) reported in the studies conducted on ‘surgeons, surgeon assistants, and nurses’ (Fig. 3-a). The highest overall perforation rate (confidence interval) was 23.63% (12.06% –35.21%) reported in the studies performed on cardiovascular surgery (Fig. 3-b). It should be noted that the incidence of perforation (confidence interval) was 63.4% (59.96% –66.84%) in a study on gastrointestinal surgery.
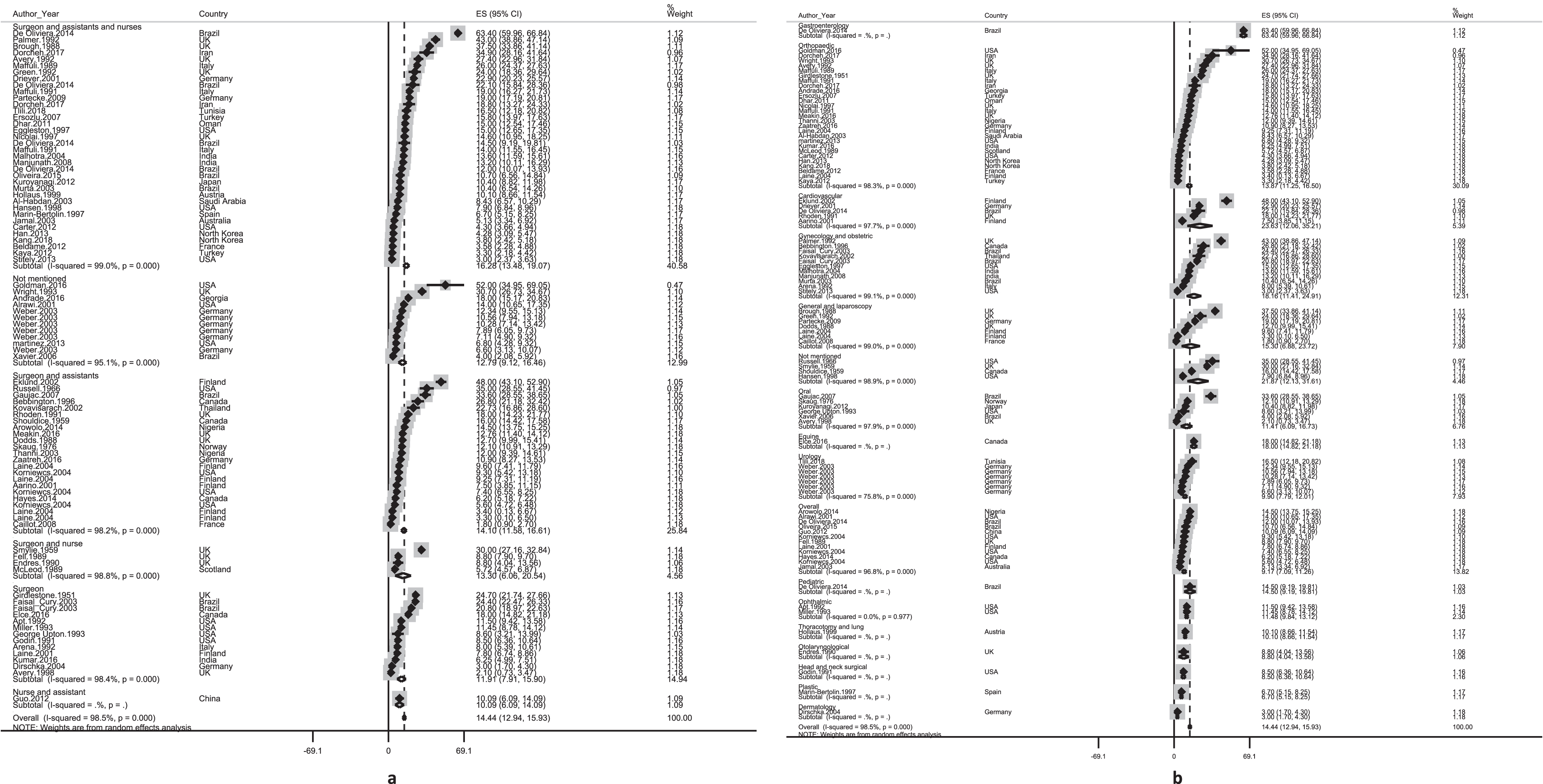
The incidence of overall perforation amongst the included studies categorized by (a) population and (b) type of surgery.
Occupations for which perforation was reported separately included surgeon (49 studies), first assistant (48 studies), scrub nurse (33 studies), and second assistant (13 studies). The incidence of perforation (confidence interval) in surgeons, first assistants, scrub nurses, and second assistants were 23.09 % (19.44% –26.72%), 12.23 % (10.13% –14.14%), 17.14 % (13.76% –20.52%), and 8.99 % (6.04% –11.94%) respectively (Figs. S1, S2, S3, and S4). The incidence of glove perforation by job detailed in the supplementary data(section S.1.).
The incidence of perforation by perforated layers
The layer where the perforation occurred was classified into two types of the outer layer (44 studies) and the inner layer (37 studies). Glove configuration was also divided into single gloving (24 studies) and double gloving (12 studies). Due to the limited number of studies on triple gloving, this category was excluded. The incidence of perforation (confidence interval) in outer layer, inner layer, single gloving, and double gloving were 25.67 % (19.10% –32.25%), 7.96 % (6.58% –9.35%), 14.18 % (10.64% –17.73%), and 17.07 % (0.01% –34.15%) respectively (Figs S5, S6, S7, and S8). The incidence of glove perforation by perforated layers is detailed in the supplementary data (section S.2.).
Unnoticed perforation by practitioners
Out of the 130 datasets of 109 studies included, 23 reported unnoticed perforation in gloves (Fig. S9). The incidence of unnoticed perforation was 68.58 % (61.41% –75.74%). Unnoticed perforation was classified based on glove configuration, studied population, and type of surgery. Unnoticed perforation by practitioners detailed in the supplementary data (section S.3.).
Perforation in different areas of hands
21 reported glove perforation in the non-dominant hand (Fig. S10). The incidence of glove perforation in the non-dominant hand was 58.24 % (49.18% –67.29%). The incidence of glove perforation in non-dominant hands is detailed in the supplementary data (section S.4.). The overall incidence of perforation in different areas of the hand has been illustrated in Fig. S11 and the incidence of perforation in the left and right hands has been depicted in Fig. 4. Accordingly, the highest incidence of perforation was reported in the index finger (35.98%) and thumb (21.03%). Indeed, the left hand, which is the non-dominant hand in most people, had a much higher incidence of perforation compared to the right hand.
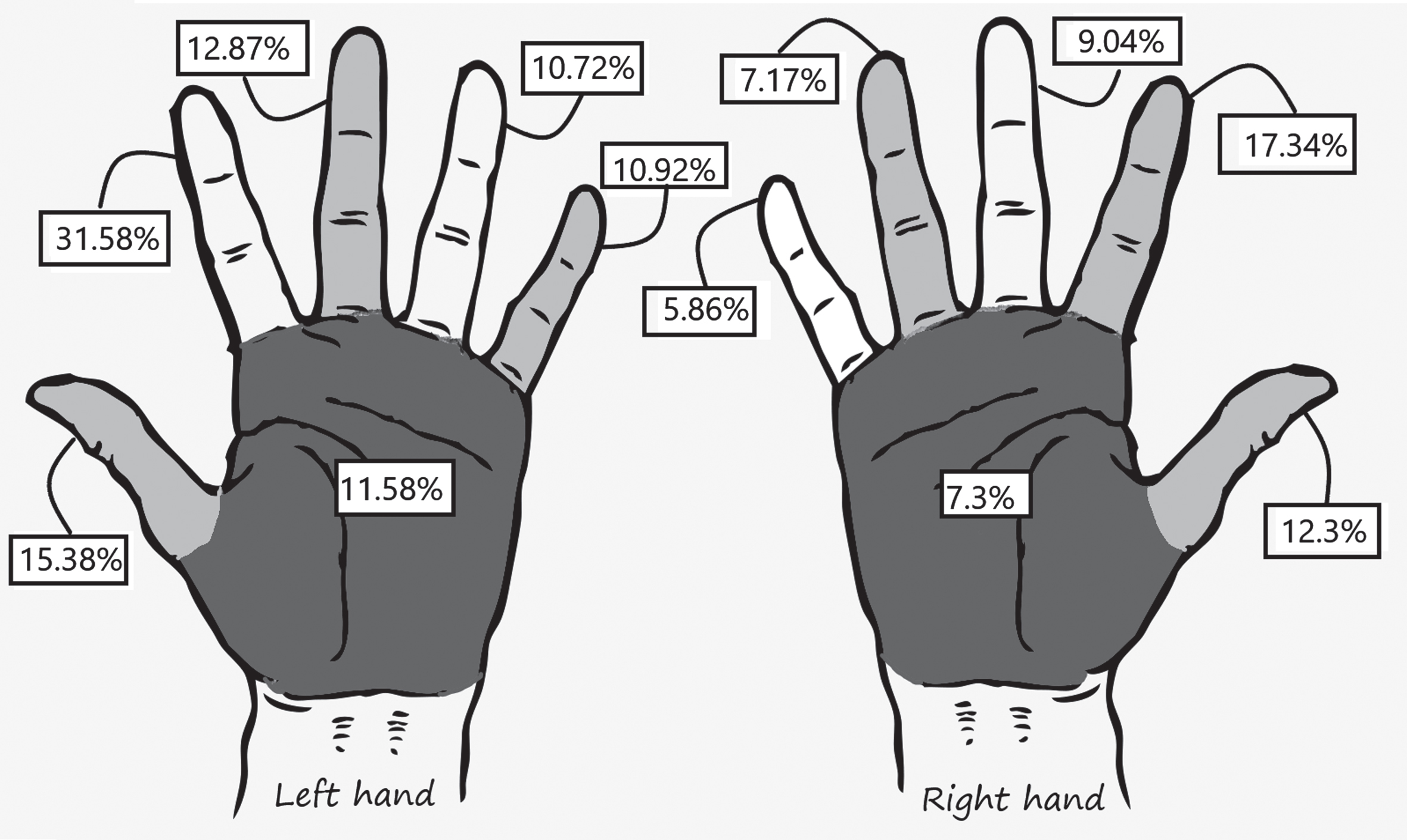
The incidence of glove perforation in the right and left hands (%).
The highest incidence of perforation was 39.86 % (31.25% –48.47%) in ‘more than 180 minutes’ and the lowest incidence was 11.52 % (8.72% –14.33%) in ‘less than 30 minutes’ (Fig. 5).The results showed that the heterogeneity of the studies included was above 50% and, consequently, the random effects model was used to calculate OR. The results were evaluated based on the shortest surgery time (less than 30 minutes). This section included the studies reporting perforation at two times (less than 30 minutes and other times). The results showed that the odds of glove perforation during 30 to 60 minutes, 60 to 90 minutes, 60 to 120 minutes, 90 to 120 minutes, more than 120 minutes, and more than 180 minutes of surgery was respectively 3.91, 3.08, 1.66, 3.95, 2.36, and 9.48 times higher compared to ‘less than 30 minutes’ (Fig. S12).
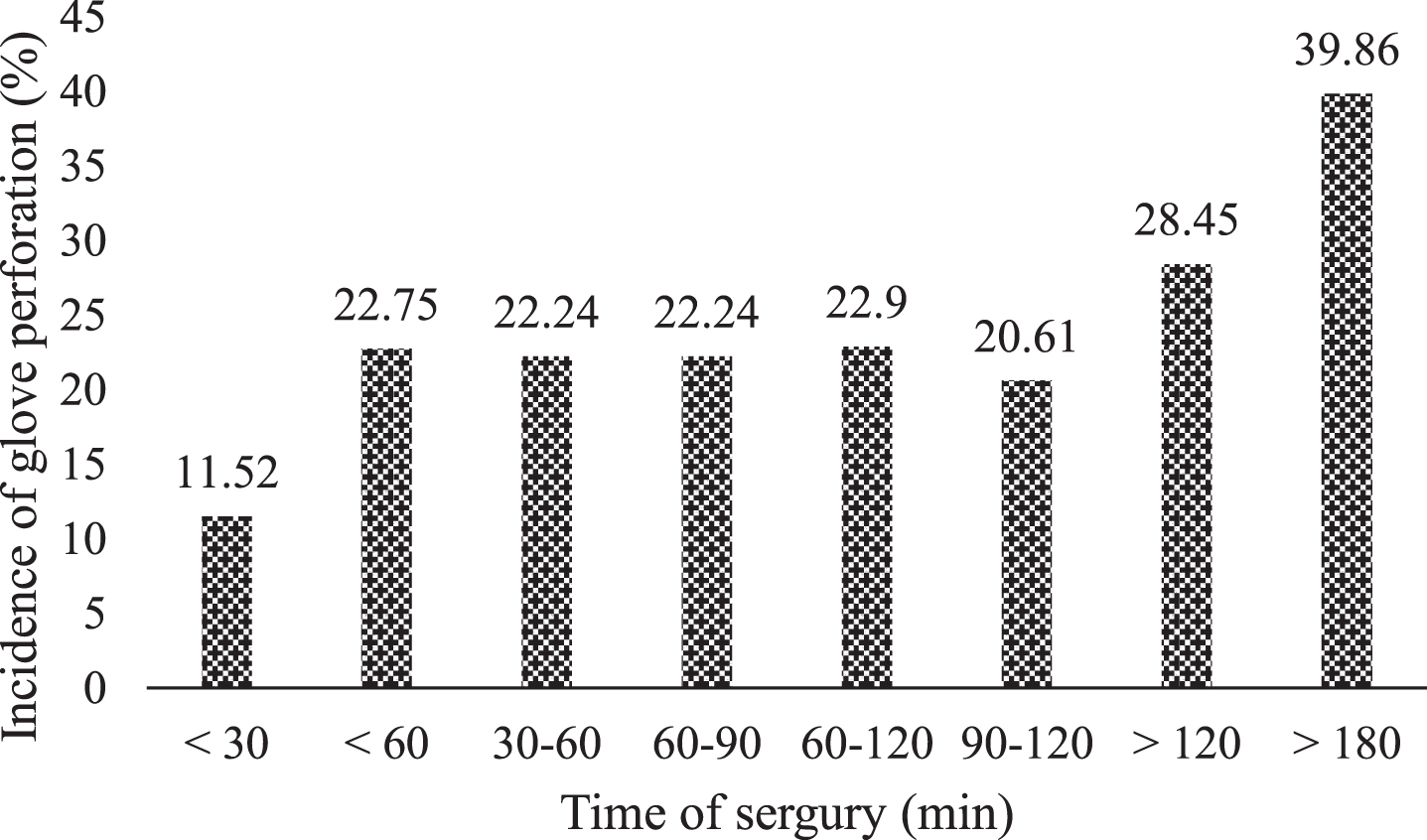
The incidence of glove perforation based on the time of surgery amongst the included studies.
A meta-regression test was used to investigate various factors affecting the overall perforation incidence. The results of the year of study and incidence of perforation showed that the incidence of glove perforation significantly decreased over time (p = 0.035). The results of meta-regression also showed that most studies examined up to 4,000 samples and the sample size included more than 8,000 participants in only one study. With the increase in sample size, the incidence of perforation decreased and this correlation was statistically significant (p < 0.001). The results of the investigation of various factors using meta-regression have been presented in Fig. S13.
Discussion
The present study aimed to evaluate the perforation rate of surgical gloves in the world. In this study, 109 articles from all over the world were evaluated and the incidence of perforation was determined based on the studied jobs, type of surgery, different layers of gloves, glove configuration, different areas of hand, and time of surgery, the unnoticed perforation, and dominant or non-dominant hand. The perforations not noticed by practitioners were identified, as well.
The overall incidence of perforation in surgical gloves was 14.44%, and the incidence of perforation (depending on the type of surgery) was reported to range from 1.8% to 63.4% in various studies. The difference between these results can be attributed to variations in conditions such as surgical instruments, equipment, and techniques, type and depth of tissues, glove manufacturing, duration of use, duration and type of surgery, and role of staff in the surgical team, have the potential to perforate gloves (23–25). The US Centers for Disease Control and Prevention (CDC) also stated that any of these factors might be a break during surgeries and lead to glove perforation [26]. However, whether the incidence of glove perforation is high or not, failure in glove integrity can affect the safety of patients and surgical team members and expose them to serious risks. Microbes can pass from patients to surgeons and vice versa through the micro-holes and transmit viral diseases, such as hepatitis B, hepatitis C, and HIV, which can cause serious health problems [24]. The risk of infection and exposure to various pathogens increases when practitioners are unaware of glove perforation and continue to use the gloves until the end of the process [27, 28]. The likelihood of contamination increases with an increase in the duration of skin contact with germs and blood products [21].
According to the results of the present study, 68.58% of the perforations were not identified by individuals and, unfortunately, practitioners continued to work with defective gloves. Depending on the type of surgery, 30–100% of the perforations were not noticed in various studies. This is a very important issue, because if arrangements were made to make individuals aware of the holes, they would quickly replace the gloves and reduce the time of exposure to infections.
Methods for reducing the risk of gloves perforation include the use of two layers of standard surgical gloves (double gloving), use of double gloving with an inner indicator layer to facilitate earlier identification of glove perforation, and use of special reinforced gloves (thicker latex, cloth, or steel mesh) in high-risk surgeries [29]. In the indicator system, a standard surgical glove that is colored (usually green or blue) is worn as the inner glove and the outer glove is white. This system detects perforations better than simple double gloving and facilitates the user’s recognition of perforation [30]. The use of indicator gloves for surgeons has been reported to halve the time for hole identification and increase the proportion of identified holes by 10 folds [31]. However, the issue of increased thickness and decreased tactile sensitivity and skills using double gloving has always been of interest [32]. Besides, gloves have been recommended to be replaced within a period of 60 to 120 minutes, depending on the surgical sensitivity and the exposures of the hands. To reduce the likelihood of open surgical wound infection, continuous replacement of gloves minimizes the friction of gloves, reducing the incidence of perforations.
The results of the present study also showed the benefit of using double gloving instead of single gloving. The incidence of perforation in single gloving and double gloving was 14.18 and 17.07, respectively. The higher incidence of perforation in double gloving may be since double gloving is often used in surgeries where the practitioners are aware of the potential risks of further perforation of the gloves, such as open surgeries that have bone bumps in contact with the practitioners’ hands. However, the incidence of perforations in the outer and inner layers of double gloving was 25.67% and 7.96%, respectively. It is clear that the outer layer prevents the perforation of the inner layer and helps maintain glove integrity [25, 33]. Laine et al. reported that the risk of blood contamination in single gloving was 13 times higher than in double gloving [34]. Double gloving is used when the risk of glove perforation is high as in orthopedic surgery, during surgeries on patients with blood-borne diseases or when the consequences of the infection are catastrophic for the patient as in implanting a prosthesis [35]. However, most professionals resist the use of double gloving, claiming to reduce touch sensitivity and hand skills [12].
The results revealed that most damages occurred in the index finger (35.98%) and the thumb (21.03%). Additionally, the incidence of perforations was higher in the non-dominant hand than in the dominant hand. The greater damage in these areas can be due to the increased use of these areas, their greater involvement with damaging and sharp agents, and their higher contact with the patients’ tissues and bones [25]. The fact that the surgical team members handle sharp instruments using their dominant hands is a possible cause of the occurrence of accidents in the opposite hand [36].
Conclusion
The present study carried out a complete review of studies conducted in the world on the prevalence of perforation of surgical gloves. This study examined all areas related to the perforation of gloves and its results can be used in all topics related to the perforation of surgical gloves. This study was the final confirmation of the high prevalence of perforation in surgical gloves and expresses the need to provide preventive solutions. The overall prevalence of perforation was very high in different areas. This prevalence was particularly noticeable on the index finger. Due to the high incidence of surgical glove perforations, most of which have not been identified, it is imperative to consider strategies to minimize the incidence of perforations. Such practices include using double-gloving and triple-gloving, using knitted gloves and glove liners, changing gloves more frequently in extended surgeries, and adopting a perforation indicator system [30]. On the other hand, due to the higher incidence of perforations in the non-dominant hand, the time interval for glove replacement of the non-dominant hand should be shorter compared to the dominant one. Moreover, professional training sessions are recommended to be held to highlight the importance of implementing these strategies in everyday practice. Furthermore, measures are recommended to be taken for constant vigilance and surgical team members’ feedback to improve the quality of care provided to surgical patients.
Limitations
This study had some limitations. Most of the included studies in the meta-analysis were cross-sectional and, consequently, reverse causality cannot be ruled out. Another important limitation was the use of the random effects model, assuming that the included studies were representative of their hypothetical populations. Hence, the heterogeneity among the studies might be represented by a single variance granting too much weight to the studies with small sample sizes. Furthermore, studies without positive or statistically significant findings may be less likely to be published by journals. The articles included in this study were from around the world, and there may be interfering factors in comparing the results, including differences in facilities, the way tasks are performed, the number of employees during the operation. It is suggested that future studies examine the causes of the surgical glove perforation by considering interfering factors.
Implications
The use of gloves by healthcare workers has increased over recent years. Despite the many advances in the design and production of surgical gloves, the integrity of these gloves is still problematic. While employees have a professional responsibility to control the rate of gloves perforation as much as possible, employers may also contribute through better education provisions, stricter monitoring and control of glove usage, and purchasing gloves that are safer. Glove manufacturers should identify the problems in their gloves, the health risks involved and undertake new research to produce better gloves. The results of the present study can be used to identify the factors affecting perforation and high-risk parts of gloves and to integrate information related to the rate of perforation of surgical gloves in different surgeries.
Footnotes
Acknowledgment
The authors would like to thank Ms. A. Keivanshekouh at the Research Improvement Center of Shiraz University of Medical Sciences for improving the use of English in the manuscript.
Conflict of interest
The authors have no conflict of interest to report.