
Abstract
BACKGROUND:
Virtual office work, or telework/remote work, has existed since the 1970s due to the widespread availability of new technologies. Despite a dramatic increase in remote office work, few studies have examined its long-term effects on work environments and worker well-being.
OBJECTIVE:
A prospective field intervention study was undertaken to examine the effects of a Virtual Office program on office workers’ psychosocial perceptions, mental and physical well-being, workplace satisfaction, and performance.
METHOD:
A large public service organization undertook a 12-month Virtual Office (VO) pilot program using a systems approach. The study included 137 VO employees (intervention condition), and 85 Conventional Office (CO) employees (control condition). The VO intervention used a work system approach consisting of establishing a steering committee, training programs, and VO resource website. Employee survey measures and follow-up focus group observations were used to examine the impact of the VO intervention.
RESULTS:
Virtual office participants reported higher job control, group interactions and cohesiveness, and quality of supervision than the CO participants. VO participants reported lower upper body musculoskeletal symptoms and physical/mental stress than CO participants. VO participants reported higher performance (customer satisfaction) than the CO participants.
CONCLUSION:
The study findings were sufficiently positive to provide a basis for work organizations to undertake similar pilot programs. Consideration of work system factors when designing an effective VO program can benefit employee’s well-being and performance. The rationale for implementing VO programs is underscored by the current COVID-19 pandemic. VO work will continue to some degree for the foreseeable future.
Introduction
Prior to COVID-19, telework, virtual offices and remote work have existed since the 1970s due to the widespread availability of new technologies. A dramatic increase in the demand for telework arrangements has occurred in the last several decades [1, 2]. New working patterns, alternative workspaces and the Information and Communication Technologies (ICT), including the internet, wireless networks, cell phones, computers, software, middleware, video-conferencing, social networking, and other media applications and services, have made it possible to work from any location for many employees [3–8]. Both private industry and government agencies have been in the forefront of promoting alternative work settings. The effects of VO and telework have been observed to be beneficial to the economy, environment, family and work integration, and employee’s performance and well-being [9]. However, the blur between the physical and organizational boundaries, between the workplace and home, may also negatively impact an individual’s physical and mental health due to extended hours, lack of or unclear delineation between work and home, and limited organization support and resources [10]. A sense of isolation and poor physical ergonomic workspaces may contribute to psychosocial stress and musculoskeletal symptoms [11–15].
Telework studies present a mixed picture of these effects, as both negative and positive results have been reported. It appears that the existing evidence is inconclusive and contradictory [2, 17]. Further, the issues of working in virtual offices is complex and requires a systems approach to better understand the interrelationships among the sub-systems elements of the organizational, physical, psychosocial and environmental factors and their impact on employees’ individual well-being and performance [2, 19–22]. Attention to human factors/ergonomics (HF/E) issues from both micro- (individual workers) and macro- (organization and environment) perspectives is essential to support and protect workers, ensure worker well-being and performance, and achieve the benefits of telework [23]. Organizations that plan and implement telework programs properly can experience positive outcomes. These successful telework factors are described in a work system, macroergonomics model that integrates the individual, microergonomics issues, the group level issues and the organizational, macroergonomics issues [22].
Few studies have examined the long-term effects of telework and virtual offices on workers’ well-being, mental and physical well-being, musculoskeletal health, supervisory/group relations and performance using an appropriate control group, as noted by a recent meta-analysis of 23 epidemiological studies [2]. To fill this gap, a prospective, repeated-measure field intervention study was implemented to examine the effects of a virtual office, telework program on office workers’ psychosocial perceptions, mental and physical well-being, workplace satisfaction and performance compared to a control group working in a conventional office setting. Given the abrupt shift in the nature of work systems across the globe that has occurred due to the COVID-19 pandemic, these study results can provide guidance in developing virtual office programs that are healthy, safe and productive. Fig. 1 shows our conceptual model, based on a theory of change, which guided our research model and questions [24]. A Virtual Office (VO) pilot program was developed and evaluated by a service organization in collaboration with the research team (authors) which included performance management and ergonomics training as well as office equipment to be used in the home work environment. Participants in the VO program chose to either adopt a new Virtual Office workstyle or continue working in their Conventional Office (CO) setting with the expectation to eventually transfer to a VO after the study completion.
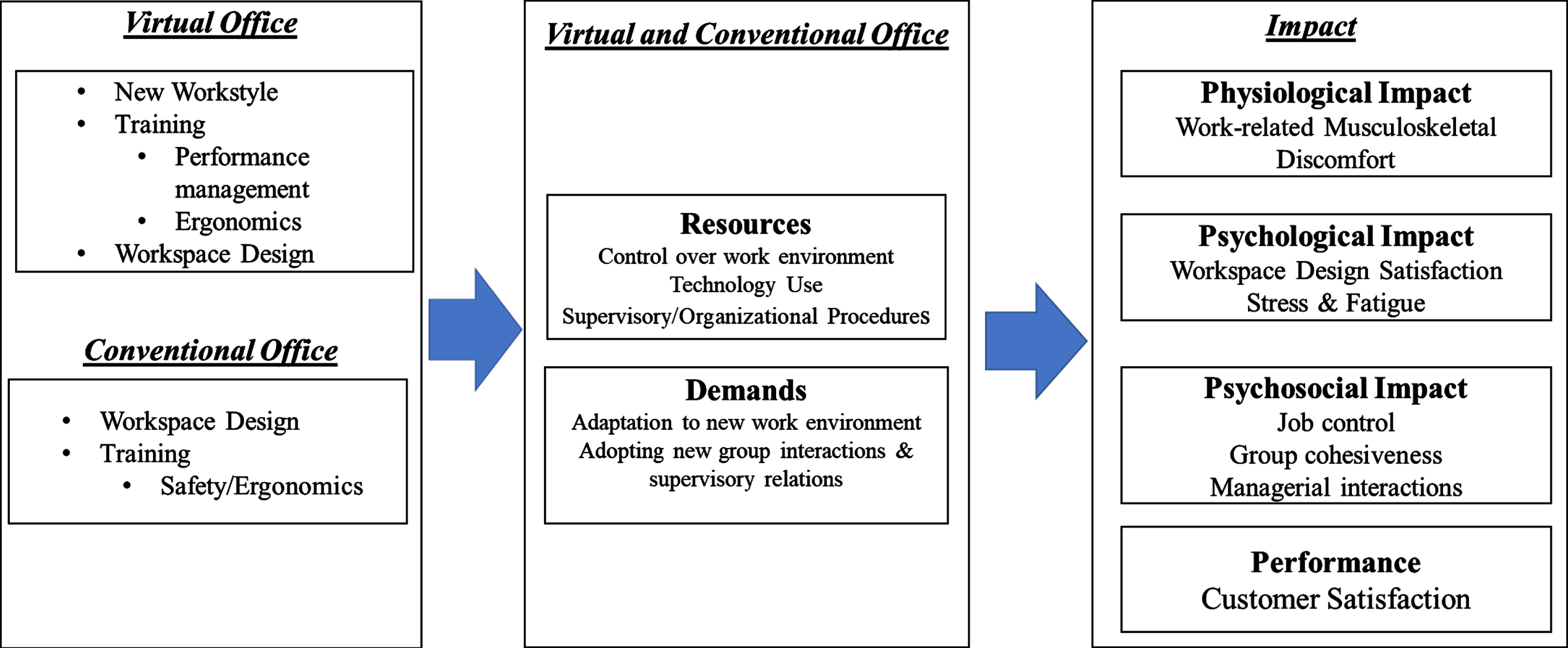
Conceptual model of the present study adapted from the theory of change [24]. This model depicts the expectation that when a Virtual Office (VO) program is implemented, an increase in control and knowledge will motivate workers to adapt to a new workstyle and to adopt healthy computing behaviors (e.g., break patterns, workstation set-up). The VO program, including performance management and ergonomics training, is expected to improve job and environmental control, the psychosocial work environment and computing behaviors that will decrease musculoskeletal symptoms and improve well-being and performance.
The current study focused on both process and outcome measures of the VO intervention. Specifically, the first two hypotheses addressed how the VO work arrangement can affect the work environment and work procedure. It was postulated that the VO intervention will improve the overall quality of the work environment.
H1. The VO employees will report increased job control over psychosocial and physical environment of work and greater group participation and group interaction compared to the CO group.
H2. The VO employees will report a more positive virtual office experience in terms of the quality of supervision, work-life boundary, and workflow (i.e., less work interruption) compared to the CO group.s
The following hypotheses were made regarding the psychological, behavioral, and physiological effects of the VO intervention. It was postulated that the employees in the VO intervention condition will report greater satisfaction and less psychological stress and strain compared to the employees in the CO condition, while their performance would not significantly differ.
H3: The VO group will report higher workspace satisfaction compared to the CO group.
H4. The VO group will experience a lower frequency of fewer work-related musculoskeletal symptoms compared to the CO group.
H5. The VO group will report lower mental and physical stress and commuting fatigue compared to the CO group.
H6. The VO and the CO groups will be comparable in regard to customer satisfaction, an indicator of performance.
Methods
Study participants
All participants were employees from a large public sector service organization. Specifically, three Business Units (BUs) were involved in the VO pilot study where the employees were considered knowledge workers. Participants worked in sedentary, computer-intensive jobs requiring at least 4 hours per day working at an office computer. A memo was sent to all employees in these targeted BUs announcing the Virtual Office program and inviting them to volunteer their participation in the VO pilot program, along with a wait-list control group that remained in the conventional office setting. It was planned by labor-management agreement that all employees in the proposed study groups would eventually become virtual office workers. In spite of the efforts of the researchers to obtain demographic data (e.g., age, sex, race, job title, job tenure), no Personally Identifiable Information (PII) was collected due to labor-management policies. The exclusion criteria included: 1) less than 1-year work experience for the job title, 2) less than 1-year work experience in the organization, and 3) not “fully successful” on their 1-year performance appraisal. Based on these exclusion criteria, a total of 239 employees were invited to participate in the study. Approximately 140 of the study volunteers were selected to telework. Volunteers who signed up and not selected were wait-listed for the next planned phase of implementing a VO program. The organization did attempt to accommodate all of those who did volunteer for the VO program; however, the final selection was dependent on the BU budgetary allowance. Enrollment for the study was opened over a 2- to 3-week period and managers provided details about the study in their departmental meeting to allow potential participants enough time to consider the new workstyle of virtual office, home-based work.
Participants for both the Virtual Office (intervention condition) and the Conventional Office (control condition) groups were recruited from three work groups or Business Units. All VO employees and their managers signed a Memorandum of Understanding (MOU); the union was involved in the selection process to ensure eligibility and fairness. Union-Management negotiations regarding the selection and conditions of the VO pilot program were completed prior to the implementation of the VO program. This study was approved by and complied with the New England IRB for the Protection of Human Subjects. Final study data for hypothesis testing included 85 participants in the VO condition and 137 participants in the CO condition, after the omission of the data from 17 participants whose responses to either of the pre- and post-intervention measures were incomplete.
Organizational workplace setting for the Virtual Office intervention
A large public sector service organization undertook a VO pilot program to study the feasibility of adopting VO throughout the organization. A VO Steering Committee was created to explore the capabilities and limitations of a VO environment. They directed the efforts of designing, implementing, and evaluating the effects of working in a VO environment compared to a CO setting. The VO Steering Committee established sub-teams to focus on the following areas concerning introducing a VO: training, communications, measures, IT infrastructure, and rules. The organizational goals were to gather information on the effectiveness of VO prior to making decisions regarding a large-scale implementation. Specifically, their organizational objectives were to assess the feasibility of implementing a VO program and to examine the organizational impact of a VO on participating office workers’ psychosocial perceptions, mental and physical well-being, workplace satisfaction, and performance compared to a CO setting group.
Virtual Office intervention
After the circulation of the memo announcing the VO study, and subsequent enrollment, those participants who volunteered to become VO workers received, along with their managers, training on how to perform as a VO worker. This training included what the expectations were regarding communications with their managers; how best to collaborate with their co-workers; and how to set up their homebasedwork environment. All VO employees received a laptop, printer, cell phone, and a two-drawer file cabinet to set up in their home office environment. A formal employee-manager VO agreement was signed after the training was completed to ensure that the rules guiding virtual work were clearly communicated and understood. The CO employees were provided with the organization’s standard occupational safety and ergonomics training and were provided with the ergonomics services available in the organization. Both study groups were informed about the VO project and when the administration of the surveys would take place, along with the focus groups over the 12-month study period. Participants were asked to assess the various psychosocial, physiological, and behavioral attributes that might be associated with the VO program. Further instruction on the logistics of those participants moving from a CO to a VO home-based work environment, was given by the organization.
Study design
This study was a prospective, field investigation, with non-randomized groups, using pre- and post-intervention measurements that examined the effects of a Virtual Office intervention on knowledge workers engaged in computer and office work tasks [25]. Two groups were involved in the study consisting of: 1) Virtual Office employees (intervention condition), and 2) Conventional Office employees (control condition) who were studied over a 12-month period. Each group included both employees and managers who worked in one three BUs. Managers were supervising employees that were either participating in the VO program or were in the CO group.
The 12-month study timeline and participant recruitment process are shown in Fig. 2 where two groups were asked to complete a survey at two-time intervals (pre- and post-intervention). In order to supplement the Workstyle Environment and Health (WSEH) survey administered pre- and post-VO intervention, focus groups were conducted near the end of and after the study (i.e., Month 12–14) as a follow-up of the intervention program. The post-VO intervention focus groups involved both managers and employees.
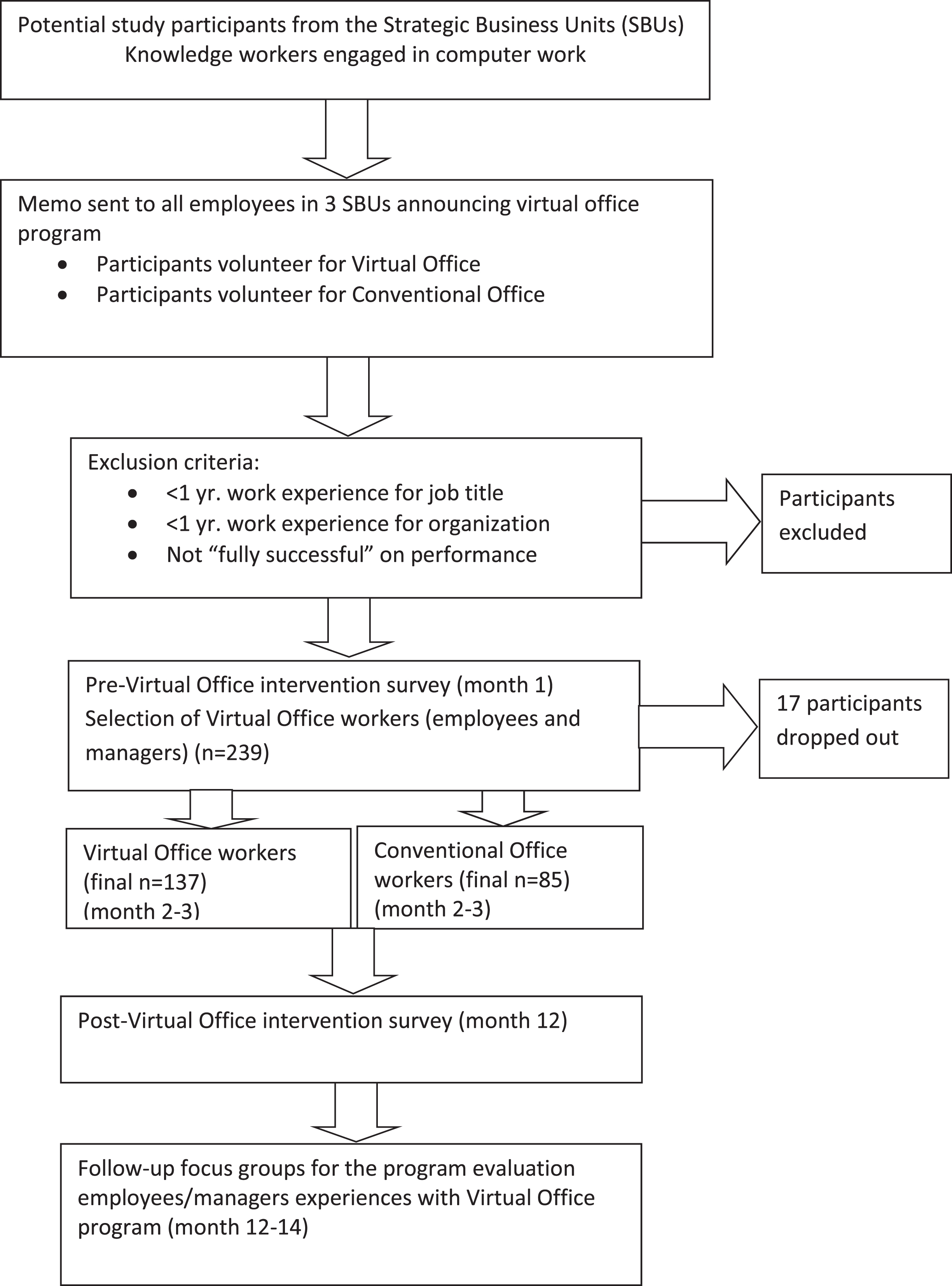
The Virtual Office (VO) program 12-month study timeline and participant recruitment process.
Survey instrument
We developed the WorkStyle Environment and Health survey (WSEH), adapted from Amick et al. [24] and Robertson et al. [26], which asks workers to report their perceptions regarding the process of the virtual and conventional office workstyle arrangements as well as their outcomes. Specifically, job control, group participation and decision making, group interaction and cohesiveness, quality of supervision, rest break behavior, and work interruption were assessed as indicators of the psychosocial and physical work environment. Also, workspace design satisfaction, musculoskeletal discomforts for the upper/lower body areas, physical/mental stress, and physical/mental commuting fatigue were measured as outcomes of the VO program intervention. Additionally, customer satisfaction was used as a surrogate to assess work performance. Table 1 shows the questions used to assess each study variable. All variables were assessed with a self-report Likert scale except for the work-related musculoskeletal discomfort (lower/upper body) variable, which was assessed with a dichotomous Yes/No question. Table 4 shows the ranges of the scale metrics.
List of the study variables, outcomes, and their sources
List of the study variables, outcomes, and their sources
*WMSD Work-Related Musculoskeletal Discomfort.
Mean scores and (SD) for the Virtual Office (VO) and Conventional Office (CO) groups
*WMSD = Work-Related Musculoskeletal Discomfort; the values indicate raw scores.
Six focus groups were conducted separately for both the managers and VO participants to discuss and comment openly among their peers regarding their experiences of working in and/or managing a VO program. Focus groups were facilitated and analyzed by an internal service resource group of the organization and these results provided in-depth opinions regarding the VO workstyle. Limited data of the focus groups responses were provided to the researchers at the group level due to labor-management policies.
Data analysis
To test the study hypotheses an analysis of covariance (ANCOVA) approach was conducted to assess whether the post-intervention scores differed between the CO and VO conditions. In the ANCOVA, the primary focus is on whether outcome scores in one group are higher after the intervention. The pre-intervention scores in the ANCOVAs were used as co-variates to adjust the post-intervention scores for the purpose of making comparisons between the VO and CO groups.
In addition to the pre-intervention scores of the target dependent variables, attitude toward virtual office, and satisfaction with organizational support for the VO arrangement were used to remove the variance associated with these co-variates. The ANCOVA model was built as follows:
Certain factors can be systematically associated with the intervention processes (e.g., compliance) and outcomes (e.g., effectiveness). Specifically, outcomes encompassing psychosocial and environment variables as well as performance and well-being variables can be affected by their own initial states and favorable attitudes in general regarding the intervention efforts and goals. Thus, our analyses statistically removed the variances from the pre-intervention scores of the select dependent variables: attitude toward virtual office and satisfaction with organizational support for the VO arrangement. By doing so, our analyses comprehensively took into account both pre- and post-intervention measures for the hypothesis testing. Also, it should be noted that the main statistics reported in the result section are not arithmetic difference scores between the CO and VO conditions after the intervention, but the ANCOVA model-based estimation of the differences (i.e., β2 of the ANCOVA model presented earlier). Open source statistical analysis package R [27] was used for the statistical analyses.
Results
Descriptive statistics
Correlations and internal consistency statistic, Cronbach’s α, are presented in Table 2 for pre-intervention variables and Table 3 for post-inter-vention variables. The Cronbach’s α statistics were all greater than 0.70 suggesting satisfactory internal consistency in general. The only exception was for the post-intervention measure of work interruption (α= 0.68), which is close to the 0.70 criterion, and is attributable to the small number of items and individual item’s distinctive nature. Table 4 presents the means, and standard deviations for the VO and CO groups.
Correlations and internal consistency –Pre-intervention measures
Correlations and internal consistency –Pre-intervention measures
Job control, Group participation and decision making, and Group interaction and cohesiveness are Work environment characteristics variables; Values on the diagonal are Cronbach’s α statistics; **p < .01; *p < .05. *WMSD = Work-Related Musculoskeletal Discomfort.
Correlations and internal consistency –Post-intervention measures
Job control, Group participation and decision making, and Group interaction and cohesiveness are Work environment characteristics variables; Values on the diagonal are Cronbach’s α statistics; **p < 0.01; *p < 0.05. *WMSD = Work-Related Musculoskeletal Discomfort.
Job control
Job control attribute of the work environment was significantly different across CO and VO conditions after the intervention such that it was 0.39 (8%; i.e., [raw coefficient × 100]/[max available raw score]) greater among VO employees than CO employees (p < 0.01; F(1,171) = 31.99). Participation and decision-making attribute of work environment was significantly different across CO and VO conditions after the intervention such that it was 0.08 (2%) greater among VO employees than CO employees (F(1,171) = 7.44; p < 0.01). Interaction and cohesiveness attribute of work environment was significantly different across CO and VO conditions after the intervention such that it was 0.04 (1%) greater among VO employees than CO employees (p < 0.05; F(1,172 = 6.40). Hypothesis 1 was fully supported. In summary, the VO intervention was associated with enhanced job control, participation and decision making, and interaction and cohesiveness.
Supervisory and work organization
Supervision quality was significantly different across CO and VO conditions after the intervention such that it was 0.22 (6%) greater among VO employees than CO employees (F(1,170) = 10.46; p < 0.01:). Work interruption by technology was not significantly different across CO and VO conditions after the intervention (F(1,170) = .04; p = 0.84). Also, rest break skip was not significantly different across CO and VO conditions after the intervention (F(1,172) = 0.00; p = 0.95). In sum, virtual office intervention was not associated with compromised supervision quality, workflow, and rest breaks. Hypothesis 2 was partially supported.
Ergonomic workspace design satisfaction
Ergonomic workspace design satisfaction was significantly different across CO and VO conditions after the intervention such that it was 0.38 (10%) greater among VO employees than CO employees (F(1,172) = 19.12; p < 0.01). Hypothesis 3 was fully supported.
Individual self-reported musculoskeletal discomfort symptoms
Work-Related Musculoskeletal Discomfort (WMSD) symptoms in the upper body was significantly different across CO and VO conditions after the intervention such that it was 0.11 (11%) less among VO employees than CO employees (F(1, 173) = 4.67; p < 0.05). WMSD symptoms in the lower body was not significantly different across CO and VO conditions after the intervention (F(1,173) = 1.67; p = 0.20). Fewer reports of upper body WSMD symptoms were found under VO conditions; however, this was not the case in the lower body. Hypothesis 4 was partially supported.
Self-reports of physical and mental stress and fatigue
Physical stress was significantly different across CO and VO conditions after the intervention such that it was 0.78 (16%) less among VO employees than CO employees (F(1, 160) = 32.38; p < 0.01). Mental stress was significantly different across CO and VO conditions after the intervention such that it was 0.81 (16%) less among VO employees than CO employees (F(1, 159) = 34.25; p < 0.0). Additionally, the physical attribute of commuting fatigue was marginally significantly different across CO and VO conditions after the intervention such that it was 0.40 (10%) less among VO employees than CO employees (F(1, 172) = 3.27; p = 0.07). Mental attribute of commuting fatigue was not significantly different across CO and VO conditions after the intervention (F(1, 174) = 1.62); p = 0.21). In sum, VO intervention was associated with reduced physical and mental stress as well as physical commuting fatigue, but not with reduced mental commuting fatigue. Hypothesis 5 was partially supported.
Self-reported performance regarding customer satisfaction
Customer satisfaction was significantly different across CO and VO conditions after the intervention such that it was 0.21 (5%) greater among VO employees than CO employees (F(1,172 = 21.72; p < 0.01). Hypothesis 6 that there would be no difference was not supported, yet study participants’ performance in terms of customer satisfaction was greater in the VO condition than the CO condition.
Focus group observations of VO
Table 5 presents the employees and managers observations and experiences of the VO pilot program. These comments were grouped in several qualitative categories as organized by a research department within the public sector organization.
Key focus group feedback and experiences regarding the Virtual Office (VO) pilot program
Key focus group feedback and experiences regarding the Virtual Office (VO) pilot program
Telework and VO have been a prevalent workstyle for some time since the emergence of new technologies and the digital age. However, due to the COVID-19 pandemic, a rapid shift to VO and work from home occurred and this change in working conditions is impacting many who were not prepared to adopt this new and unfamiliar work mode. It also affects others who were not used to functioning with complete physical and social separation from the organization. Our investigation examined the effects of a planned VO program using a systems approach on employees’ well-being and performance to better understand the feasibility of implementing a VO program and to inform the development of guidelines to support employers in designing optimal working conditions in a VO. For this prospective study, we evaluated the effects of a VO program, consisting of ergonomic and performance management training along with home office equipment, on office workers’ psychosocial perceptions, mental and physical well-being, workplace satisfaction, musculoskeletal discomfort, and performance compared to a conventional office group. The VO workstyle was shown to have a positive impact on VO employees’ overall work environment as well as their health and well-being, suggesting that using a systems approach to design and implement a VO program can be beneficial. Led by the VO steering committee, a thoughtful plan was developed that included designing comprehensive training regarding VO practices and policies, including ergonomics and safety training, on how to successfully adopt the VO workstyle. Participants involved in the VO program study were from three BUs where participants volunteered to work in either a Virtual Office workstyle or in a Conventional Office work setting. Managers in these BUs were managing both VO and CO employees. Additionally, there was management-union support and commitment to the implementation and evaluation of the VO program.
Virtual Office participants reported a significant increase in job control indicating that an enhanced control over optimizing their job flexibility and work environment was positively experienced compared to the Conventional Office group. With the increase in job control, VO participants gained a sense of control in managing their work pace and deadline pressures. As noted in the focus group results, employees reported their ability to manage their workload and concentrate better in a VO environment due to individually optimizing and streamlining their work procedures. Similar findings of improved quality of work life, through increased autonomy, has been reported for teleworkers [28]. Interestingly, an analysis by gender found this relationship was true for males, but not for females. It appears that some of the benefits of VO may not be equitable across genders, suggesting that adaptable strategies to ensure the needs of different employees should be targeted [2, 28].
It is worth noting that both the VO and CO groups reported a significant increase in work interruptions associated with technology issues, such as internet and phone service, computer- and printer-related issues, while no significant difference was found between the two groups after the intervention. Several VO participants expressed the need to be trained specifically on using the IT equipment, along with establishing a turn-key type procurement process for purchasing home-based office equipment. Several researchers have reported that effective VO programs need to provide appropriate equipment and high-quality technology support in conjunction with training in the necessary software and systems needed by employees [29, 31].
Group interactions and cohesiveness were significantly higher among the VO employees than the CO employees, suggesting that the VO workers had to make a concerted effort to communicate with their co-workers to clearly understand the group project goals and work processes. Furthermore, the finding that the VO participants reported greater participation in the decision-making processes indicates the positive efforts of the employees to articulate and discuss with their colleagues in a positive group manner. Organizational support systems need to be created so that both managers and colleagues can facilitate effective formal and informal support. Establishing formal and regular communication strategies and policies can mitigate a feeling of disconnect that VO employees may have from their managers and colleagues [2]. In the follow-up focus groups, the VO participants stated that using group scheduling technology, such as Outlook calendars, was beneficial; however, it was essential that group members maintain a current and up-to-date calendar for scheduling efficiency. VO participants created agendas and managing tele-conferences more effectively and their quality of communication improved, possibly due to the training and managerial support to engage in efficient group decision-making efforts.
VO participants appear to have arranged their workspace to fit their computing and work needs as the VO group reported a significant increase in workspace design satisfaction compared to the CO group. Since VO employees showed a significant increase in job control, their sense of control may allow them to exert control over setting up their home environment to use their workspace for long periods of time comfortably. These results are corroborated by earlier office ergonomics interventions findings of enhanced job and environmental control over one’s work environment can create a sense of workspace design satisfaction [32, 33].
The significant finding for the VO group regarding supervisory quality suggests that the VO program training and the performance management agreement (MOU) may have positively influenced the employee-managerial communication patterns compared to the CO group. Specific policies and procedures were outlined concerning when and how often the manager and employee would connect to discuss job tasks and goals. Since the job roles and responsibilities were clearly articulated in the performance management agreement for the VO participants, it encouraged the managers and employees to maintain and continually improve their interactions. Providing this type of training and assistance for managers in supervising VO employees is essential [30, 34]. Several managers noted changes in their employees’ behavior becoming more results-oriented, possibly due to the focus on setting expectations for goal attainment. Moreover, their management style moved from a management by presence and control to management by objective and trust.
Participants in the VO group did report significantly fewer upper body musculoskeletal symptoms compared to the CO group. Having a greater sense of control over the workspace set-up and arrangement, the VO participants may have arranged their workstations ergonomically for the upper body region minimizing musculoskeletal discomfort [33]. However, no significant difference was found between the VO and CO groups regarding lower body musculoskeletal discomfort, possibly due to the chair design and features. On the other hand, high levels of musculoskeletal discomfort (40%) were observed in employees working from home during COVID-19 where participants reported moderate to severe discomfort of the upper and lower body [13]. Perhaps this was due to the suddenness of the change and a lack of proper planning and equipment. An earlier study of teleworkers also showed that 54.5% of teleworkers complained of pain in their upper limbs, back or neck, which they attributed to inadequate furnishings [35]. Three of these teleworkers had musculoskeletal injuries that resulted in a total of 80 days absence in the preceding year and it is speculated that static posture, computer use and lifting heavy objects had caused these injuries [35].
Interestingly, there was no significant difference between the VO and CO groups regarding skipping scheduled rest breaks. With the increase in job control, it was expected that the VO participants would take micro-stretch breaks to gain the benefits of changing one’s posture while computing. Managers and employees in the VO group expressed that their workday schedule could be more flexible to accommodate the completion of tasks and attend to personal family appointments. Also, not having long commutes, VO participants commented that they gain more flexibility in their work and family schedule. Other telework studies have noted that workers gain more flexibility in VO work arrangements with the reduction in commuting and not having to worry about lost commuting time, heavy traffic, traffic jams, fear of being late for work and the sense of always being on the run [36, 37].
Self-reports of physical and mental stress for the VO group were significantly less compared to the CO group, as expected. The enhanced notion of job and environmental control allows VO participants to adopt a positive VO workstyle and contributes to workers well-being, health and performance. In fact, a decrease of stress was shown, attributable to the perception of having control over their work (environment and work schedules), as well as their personal and family life [35]. One key issue in the work/life balance that needs to be addressed, however, is the notion of creating functional and healthy boundaries. Employees and managers need to develop formal policies on balancing this blur between work and family and learning how to disengage from work [38]. The only marginally significant finding, however, for the physical attribute of commuting fatigue as well as the non-significant finding for the mental attribute of commuting fatigue was unexpected. The direction of the VO group reports was indicating less physical commuting fatigue than the CO and this is supported by the VO group reporting less physical stress.
Customer satisfaction as reported by the VO program participants was significantly greater for the VO group compared to the CO group, indicating that the VO workstyle did not negatively affect performance. This is especially important as the VO program participants were in the SBUs where some employees were VO workers and some were CO workers needing to collaborate and work tougher to deliver internal services to the organization. These findings are similar to those reported by previous studies [9, 29], suggesting that the ability to telework fosters well-being, which in turn contributes to productivity. The ability to work away from the office enabled a better work-life balance on telework days, which engendered a positive attitude towards work. Working away from the office allowed for alternate activities (e.g. an hour of walking instead of commuting), which energized workers, resulting in less stress and allowing for more productive work [29].
Lessons learned and practical implications
The organization’s internal VO Steering Committee and researchers (authors) noted several programmatic features that needed to be addressed going forward with a full implementation of Virtual Offices. This VO program was implemented prior to the COVID-19 pandemic; however, the lessons learned from this intervention study are valuable and can be applicable to designing VO programs or a hybrid type of workstyle where employees work at home some amount of agreed-upon time, and then work in the collaborative office workspace with their co-workers and managers. Several managers remarked that their work groups were establishing agendas for future meetings after the study was completed to meet and collaboratively work. These collaborative meetings would be coordinated and organized with the clear understanding of what each individual was responsible for and to be prepared when everyone met face to face so it would be a productive and engaging time. Three major learnings emerged following this intervention study. 1) the importance of senior management communication about the goals and policies of the VO program, 2) the essential need to design training on specific topics regarding video-conferencing technologies, setting up and maintaining office equipment, managerial training on how best to manage VO workers, and establishing a website to post resources, such as IT support, security VPN issues, office equipment purchasing, health, safety and ergonomics guidelines and recommendations for home office environments, and 3) the need to create a network of VO workers who can exchange experiences and ideas on how they are best working at home and to create a sense of connection with their managers, their work group and their organization. As noted by several cross-sectional telework studies and reviews, the importance of organizational, coworker, technical & training, and boundary management support is imperative for protecting employees’ health, safety and well-being, including addressing gender inequities [2, 35].
Study limitations and strengths
One limitation of the study was the degree to which threats to internal and external validity can be addressed given the study field design, and the lack of random assignment to the VO and CO conditions. Also, the study was limited to one company with specific job types and caution should be used when generalizing the results to other VO programs and workers. There is always the possibility of participants answering the survey questions to match their perceived expectation of the experimenter (social desirability) [e.g., 25]. Additionally, measures of the study variables were based on self-reports that may be susceptible to subjectivity and bias issues. However, the repeated measure design of the present study can address an important limitation of the cross-sectional self-report methodology because the unique variance due to the self-report method can be controlled for to a certain extent by considering both pre- and post-intervention measures for hypothesis testing [40]. That being said, future studies should incorporate the use of a randomized design, systems approach and objective assessments of outcome variables to examine the effectiveness of virtual office interventions. Another limitation of the present study is that the organizational policies did not allow for the control of potential group differences in job type and demographic characteristics that may have affected the intervention outcomes.
Strengths of this study are its systems approach to designing and implementing the Virtual Office Workstyle program, including ergonomics and managerial training; a formal employee-management VO agreement; presence of a control group; high participation rate; limited loss to follow-up; the full participation of the managers, including strong support of senior management and union; and its study design being long-term longitudinal in nature with several individual level measures ranging across physical, psychosocial, supervisory and work group relations, technology interruptions, stress, and performance guided by a work system, macroergonomics framework.
Conclusion
Overall, our study findings suggest that implementing a Virtual Office program may have a positive impact on employees’ well-being and performance. Using a systems approach to develop and implement a formal plan, a VO program can be beneficial. Working virtually is likely to enhance control over one’s environment and job, thus optimizing flexibility, job accommodations and health which outweigh the potential challenges posed by the virtual office workstyle. Further field intervention research is needed to replicate and extend these findings with different Virtual Office workstyle programs. Given the abrupt changes in the workplace due to COVID-19 and correspondingly sharp increases in home-based knowledge workers, these findings would contribute to a knowledge base regarding how to design and implement Virtual Office programs that create healthy and productive work environments for office workers.
Footnotes
Acknowledgments
The data in this study were collected while the authors (MR, JL, EH) worked at Liberty Mutual Research Institute for Safety. The authors wish to thank the following team member for invaluable assistance: Peg Rothwell, for manuscript preparation, editing and general assistance. We would also like to express our appreciation to the service organization in our study, and its leaders who partnered with the authors to evaluate the VO program.
Conflict of interest
None to report.