
Abstract
BACKGROUND:
Lateral epicondylitis (LE) can occur for many different reasons such as compelling repetitive movements in daily readings, incorrect posture use and work-related factors. Although several treatments are available for LE, the optimal evidence-based treatment remains uncertain. Joint protection techniques have been developed as a self-management intervention to reduce pain and disability and improve functionality by applying ergonomic approaches.
OBJECTIVES:
This study aimed to investigate the effects of telephone-based follow up on top of a home-based joint protection education programme on pain and functionality in individuals with LE.
METHODS:
Individuals were randomly assigned into 2 groups; 1) telephone-based group, receiving telephone-based follow-up on top of a home-based joint protection education programme, and 2) home-based group, receiving home-based joint protection education alone. Both groups were given training that increased awareness in LE and home-based exercise programme. In addition, telephone-based group was followed up by telephone three days a week for four weeks.
RESULTS:
Improvements from baseline to 4th week in Turkish version of the Patient-Rated Tennis Elbow Evaluation-pain (p = 0.001; effect size = 1.11) and function (p < 0.001; effect size = 1.77), Upper Extremity Functional Index (p = 0.001; effect size = 0.85) and The Turkish version of the Joint Protection Behavior Assessment-Short Form (p < 0.001; effect size = 1.54) in the telephone-based group were significantly higher than the improvements in the home-based group.
CONCLUSIONS:
Telephone-based follow-up in individuals with LE contributed to the awareness of pain, functionality and joint protection methods. Telephone-based joint protection education programmes can offer a health service within the scope of preventive and protective intervention programmes for LE.
Introduction
Lateral epicondylitis (tennis elbow, LE) is a painful musculoskeletal system disorder thought to occur due to the excessive use of wrist extensors, especially extensor carpi radialis brevis. It is estimated to affect 3% of the population and has significant personal, psychosocial and economic consequences [1, 2]. Etiological factors of LE include overuse, repetitive movements, physically forceful occupational activities, exercise errors, misalignments, flexibility problems, ageing, muscle imbalances and psychological (e.g. job strain) factors. The estimated incidence of LE ranges from 2.0–11.3 per 100 worker-years in specific activity sectors [3, 4].
Although several treatments are available for LE, the optimal evidence-based treatment remains uncertain. LE treatment should direct the individual to pain management, preservation of motion, improved grip strength and endurance, regaining normal function, and control of further clinical impairment. Identifying an effective treatment programme for individuals with LE is expected to offer significant benefits for the individual’s recovery and allow improved service delivery by healthcare providers [5].
Joint protection is a core component of Rheumatology Occupational Therapy underlying the rehabilitation for all individuals whose joints are at risk [6]. Joint protection techniques constitute a routine concept utilized in all patients with joints affected by arthritis. This concept, originally designed for rheumatoid arthritis (RA), has been expanded to include disorders such as osteoarthritis (OA) over time [6–8]. This technique is not just a physical intervention. It is also an active coping strategy to improve daily tasks and role performance, improving perceptions of control and psychological status [9]. Joint protection techniques aim to reduce pain and disability and improve functionality by applying ergonomic approaches such as changing movement patterns, modifying tasks and environment, and using assistive devices [10]. Such an approach helps individuals to understand that strain on joints when performing daily activities may increase joint pain and potentially, joint deformity. Certain principles widely accepted in joint protection techniques include respecting the pain, maintaining muscle strength and range of articular motion, using each joint in its most stable anatomical or functional plane, avoiding positions that can lead to deformity, using the strongest and largest joints available, ensuring correct movement patterns, maintaining rest-and-activity balance and reducing the force applied during activity [11].
The SARS-CoV-2 novel coronavirus (COVID-19) pandemic challenges us each day with sobering realities in the economy, health care, and politics in our society. The global pandemic has thrust the health profession and communities more towards digital apps and telehealth. The World Federation of Occupational Therapists [12] prefers to use the term telehealth to describe the service delivery model of telerehabilitation, telecare, or teletherapy, which is the use of information and communication technologies to access health-related services when the provider and client are in different locations. In addition to them, ‘telecommunication’ is an approach in ‘telehealth’ [13]. The use of telecommunication has emerged as a new method to provide healthcare services remotely [14, 15]. Telecommunication technologies include synchronous verbal communication such as videoconferencing and telephone calls and asynchronous non-verbal communication such as web-based programmes. Interventions via telephone have become currently more common to increase cost-effectiveness and utilize resources rationally in various healthcare programmes [16]. Telephone-based applications appear to be gradually increasing in the literature [17, 18]. However, to the best of our knowledge, there is no study in the literature evaluating the telephone-based application of the joint protection techniques in LE.
Despite the relatively high prevalence in the literature, there is no single and universally accepted management algorithm (e.g. controlling elbow pain, improving grip strength, preventing further deterioration) in LE that is considered effective and consistent [19, 20]. Therefore, evidence-based studies employing methods that can be used in LE management are warranted. The present study aimed to investigate the effects of an additional telephone-based follow up to a home-based joint protection technique education on pain and functionality in individuals with LE and to provide new insights to the literature based on the results obtained herein.
Methods
Study design and participants
Ethical approval was obtained from the Trakya University Faculty of Medicine Scientific Research Ethics Committee. An informed consent form was obtained from each participant at the beginning of the study.
A single-blinded randomized controlled trial was conducted using the checklist and flow diagram [21]. The flow chart of the study is shown in Fig. 1.
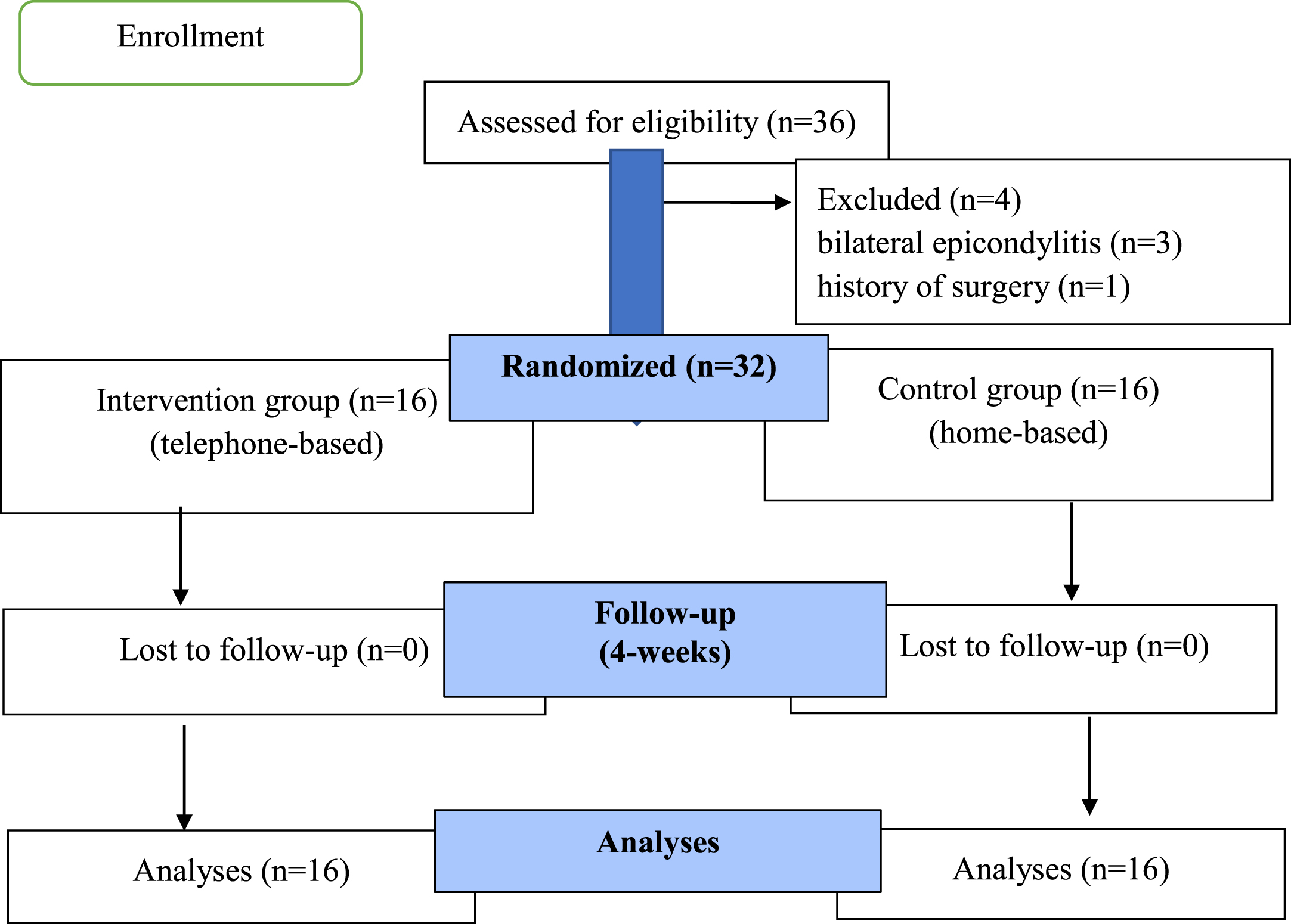
CONSORT flow diagram.
The study included 32 people diagnosed with LE by an orthopedist. This study has been carried out with individuals aged 18–40 years, working full time at a job, who had a diagnosis of unilateral epicondylitis, without a history of surgery, physiotherapy or previous training on joint protection techniques. The sample size was calculated as 14 patients for per group with a calculated effect size of 1.1 based on pain in the work of Yürük et al. [22], with an alpha level of 5%, and with a power of 80% (G*Power 3.1.9.2). We decided to examine 16 patients for each group considering probable missing values.
Individuals who met the inclusion criteria (n = 32) were stratified into 2 groups; 1) telephone-based group, receiving telephone-based follow-up on top of a home-based joint protection education programme, and 2) home-based group, receiving home-based joint protection education alone by simple random allocation according to participant numbers, with a 1:1 allocation ratio [23].
Descriptive characteristics of individuals such as age, gender, occupation and whether they have previously received a health report due to LE were recorded at the beginning of the study.
Jamar hand dynamometer [24–26] was used to determine handgrip strength, the Turkish version of the patient-rated tennis elbow evaluation (PRTEE-T) [27] was used to assess the outcome of the intervention of LE, the Turkish version of the Upper Extremity Functional Index (UEFI) [28] was used to assess upper extremity functionality, and The Turkish version of the Joint Protection Behavior Assessment-Short Form (TUR-JPBA-S) [29] was used to evaluate the joint protection behaviour. All these evaluations were made before and after interventions by the first investigator.
Jamar hand dynamometer is a method recommended by the American Society of Hand Therapists (ASHT), which has high validity and reliability across several studies and is therefore accepted as the gold standard for the measurement of handgrip strength. In line with the standard position recommended by ASHT, the handgrip strength was measured in sitting position, with the shoulder in adduction and neutral rotation, elbow flexed at 90° forearm in mid-rotation and supported, and the wrist in the neutral position. In the test procedure for the handgrip force, three measurements were taken allowing one-minute intervals between measurements, and the average value was recorded [24].
The patient-rated tennis elbow evaluation (PRTEE) questionnaire consists of two parts: (i) pain in the affected arm, (ii) function and daily activities in the affected arm [30]. This questionnaire is specially designed to evaluate patients with LE. In the questionnaire, the pain and function score can be calculated separately, and the total score can be calculated alone. Higher scores indicate more pain and a negative impact on functionality. Turkish version of the patient-rated tennis elbow evaluation (PRTEE-T) was used in this study [27]. In the Turkish version; Cronbach alpha coefficient was calculated 0.837 and 0.920 was found for test-retest reliability.
The UEFI covers twenty activities which the patient scores according to the difficulty they experience while completing these activities [31]. The highest score is “80” and the lowest score is “0” in this index. Lower scores indicate increased difficulty with the relevant activity resulting from the individual’s condition involving the upper limb. The Turkish version of the UEFI was used in this study [28]. In the Turkish version, Cronbach’s alpha coefficients for the UEFI were found 0.89 and 0.89 (at time 1 and time 2). Average measure intraclass correlation coefficient was found 0.80.
Joint Protection Behavior Assessment-Short Form (JPBA-S) was developed to evaluate the behaviour of individuals during daily activities that require using the hands [32, 33]. The scale consists of 10 different tasks. The individual gets 2 points for each correct behaviour and 1 point for each partially correct behaviour. The maximum score for the ten tasks is 20. The Turkish version of the Joint Protection Behavior Assessment-Short Form (TUR-JPBA-S) was used in this study [29]. Internal consistency was found at 0.89. Study results demonstrated excellent intra-rater (ICC:0.99) and inter-rater (ICC:0.99) reliability.
Education aimed at raising awareness about LE was provided for the telephone-based and home-based groups. During the education, information on LE was given, including the mechanisms of its development and the means to protect upper extremities in daily life. Besides, a brochure prepared by the study team to show the “principles of joint protection”, describing how to prevent damage while using the arms during daily life activities was provided. The brochure was prepared within the scope of the study, considering the literature and consisted of principles aimed at protecting the joints, especially during daily life. Also, considering the literature, all individuals were instructed to follow a home-based exercise programme consisting of eccentric strengthening exercises and stretching exercises and to complete three sets of ten repetitions a day at their pain limit [34–36]. Finally, the study team contacted the individuals with the telephone-based group by telephone three days a week for four weeks. Awareness training and all phone calls were made by the second investigator (the second investigator had a PhD degree in Occupational Therapy and had been working in rehabilitation for nearly 20 years). During each phone call session, the principles of joint protection were reminded and then, the participants were asked about the usability of joint protection techniques in daily life and whether they exercised regularly. The difficulties they experienced during the applications were discussed with the individuals and the information about the training given at the beginning of the intervention was repeated in line with the needs of the individuals. However; individual in home-based group was not called by phone. At the end of 4 weeks, the baseline evaluations of all individuals were repeated, and the results were compared.
Statistical analysis
Statistical analyses were performed with the IBM SPSS Statistics for Windows, (Version 20.0., IBM Corp., Armonk, NY, USA) package programme. Numerical variables were reported as mean±standard deviation or median (min-max), and categorical results were shown number and percentages. Shapiro-Wilk test was used to check the normal distribution of numerical variables. The similarity of group variances was investigated with the Levene’s test.
Descriptive characteristics of individuals
Descriptive characteristics of individuals
n (%), Mean±Standard Deviation, Median (Min –Max). aYates Chi-square test, bPearson Chi-square test, cStudent t test, dMann Whitney U test.
The Student t-test was used in a comparison of numeric variables between the groups (telephone-based vs home-based) in the presence of parametric test assumptions, and the Mann Whitney U test was used otherwise. Baseline and 4th week measurements of the patients for each group were compared by the paired t-test in the presence of parametric assumptions, and the Wilcoxon test otherwise. The categorical variables were compared by using the Pearson or Yates chi-square test.
Changes from baseline to four weeks in terms of handgrip strength, pain, function and joint protection techniques between the groups were compared ANCOVA test in the presence of parametric assumptions, Quade rank ANCOVA test was used otherwise. Significance level was accepted as p < 0.05.
Values of the telephone-based and the home-based groups in terms of handgrip strength, pain, function and joint protection techniques at baseline and at four weeks of the study
Mean±Standard Deviation. aPaired t test, bWilcoxon test, cQuade’s Rank ANCOVA test, dANCOVA test. Hedges’ Bias corrected Effect Size (Hedges’ Bias corrected Effect Size can be interpreted as follows: 0.01 “very small”, 0.20 “small”, 0.50 “medium”, 0.80 “large”, 1.20 “very large” and 2.0 “huge” effect size. PRTEE-T:Turkish version of the Patient-Rated Tennis Elbow Evaluation, UEFI: Upper Extremity Functional Index, TUR-JPBA-S:The Turkish version of the Joint Protection Behavior Assessment-Short Form.
The sample size was calculated as 14 patients for per group with a calculated effect size of 1.1 based on pain in the work of Yürük et al. [22], with an alpha level of 5%, and with a power of 80% (G*Power 3.1.9.2). We decided to examine 16 patients for each groups considering probable missing values.
The study was completed with a total of 32 individuals (10 female and 6 men in the telephone-based group; 8 female and 8 male in the home-based group). Two groups were similar in terms of descriptive characteristics (p > 0.05) (Table 1).
In the study, a statistically significant difference was noted in terms of PRTEE-T pain (p = <0.001), PRTEE-T function (p = <0.001), UEFI (p = <0.001) and TUR-JPBA-S (p = <0.001) values for the telephone-based group intragroup evaluations. There was a statistically significant difference in terms of PRTEE-T function (p = 0.002), UEFI (p = 0.005) and TUR-JPBA-S (p = <0.001) values of the home-based group.
Improvements from baseline to 4th week in PRTEE-T pain (p = 0.001; effect size = 1.11) and function (p = <0.001; effect size = 1.77), UEFI (p = 0.001; effect size = 0.85) and TUR-JPBA-S (p = <0.001; effect size = 1.54) in the telephone-based group were significantly higher than the improvements in the home-based group (Table 2).
Discussion
In this study, it was determined that telephone-based follow-up in individuals with LE contributed to the awareness of pain, functionality and joint protection methods. It was found that applying for the home-based programme alone contributed to the awareness of functionality and joint protection methods but had no effect on pain. Improvements in pain and function from baseline to week 4 were significantly higher in the telephone-based group than improvements in the home-based group.
Individuals working full-time were included in the study. Twenty-seven individuals suffered from pain due to LE stated that they stopped working by getting a health report at least once. Five individuals stated that they had a hard time working when they had pain, but they did not receive a health report due to the fear of losing their job and they continued to work in this way. Although psychosocial factors in the workplace are the focus of research on many musculoskeletal disorders, they are rarely encountered in the study of tennis elbow. Ono et al found a weak but significant association between tennis elbow and poor job definition, difficult interpersonal relations and organisation among Japanese nurse assistants [37]. In another study; tennis elbow among women was associated with low social support at work [38]. Most work-related upper extremity problems are resolved quickly. Although most work-related upper extremity problems are resolved quickly, it can cause long-term absenteeism in employees who have this problem. Yassi, et al. [39], examining upper extremity repetitive strain injuries, reported that the mean time lost (71.4 days) was significantly greater than non-repetitive strain injuries (33.6 days).
The basic principles in the treatment of LE are pain relief, accelerating the recovery process, reducing overload in the arm and allowing restoration of daily life activities of the affected individual. Prevention and protection are essential in the treatment [20, 40]. For this reason, the present study evaluated the effectiveness of telephone-based follow-up in LE based on joint protection principles.
Joint protection techniques include self-management strategies to reduce pain, inflammation and the risk of deformity. Furthermore, these techniques constitute an approach that is used to improve the performance in daily tasks by improving the individual’s perception of control during movement [41, 42]. Randomized studies with high levels of evidence for the effectiveness of joint protection techniques in patients with RA have shown significant improvement in pain relief [32]. For patients with hand RA and OA, two systematic reviews [43, 44] documented the effects of joint protection versus usual care or control for pain, hand function, and grip strength performance. In this study, education on joint protection techniques provided a reduction in pain scores in the group that received telephone-based education. The results of the study support the literature.
In LE, repeated concentric contractions of the wrist and increased eccentric overload in the LE cause pain [45, 46]. In this study, limitations of rotational movements that may cause increased pain in LE and the restriction of activities that may increase tendon tension were thought to be effective in reducing the spread of pain. The literature reflects proper rest as the golden key during the acute period treatment of tendinitis [47]. Decreasing or eliminating the stresses the affected tendon is exposed to reduces pain and the spread of pain in tendinitis. In patients with LE, a recovery response may be initiated by limiting the activities likely to cause stress in the tendon, thereby preventing microtrauma. In this study, the finding that pain was reduced only in the telephone-based education group may be resulting from the fact that regular follow-up was performed every week, with necessary arrangements implemented through discussions with these individuals. This may have increased the awareness about restricting stressful activities and preventing microtrauma.
Providing pain control is one of the main goals of LE treatment [20]. In LE, the activity of the forearm muscles may be reduced due to pain. Movement of forearm muscles against resistance may be painful or loss of strength may occur in these muscles. Therefore, muscle strength should be evaluated concerning pain [48, 49]. Since muscle strength is reduced especially due to pain in patients with LE [19], the effects of the training given in this study on muscle strength were also investigated herein, with the assumption that the interventions applied to the individuals may decrease pain, and potentially contribute to muscle strength. There was no difference in muscle strength in either group in the present study. This may be due to the study being limited to four weeks. In the literature, it has been noted that conservative treatment is effective in most patients with epicondylitis, however, it has been stated that the period leading to recovery may be long (6–12 months) [50]. Besides, providing the strengthening exercises as a home-based exercise programme and not performing them under the supervision of a therapist may also be a factor in the lack of difference in muscle strength. Although there is evidence in the literature for different strengthening exercise programmes applied in patients with LE, the results are inadequate in terms of generalizability [51]. Pain may lead to muscle weakness. In this study, a significant reduction in pain scores was observed only in the group that received telephone-based education. This finding draws attention to the fact that long-term results of the telephone-based education programme should also be investigated.
Strengths and limitations
There are certain strengths and limitations of this study. The strength of this study is that there are no studies on this subject that we have come across in the literature. For this reason, we think that this study will provide new information to the literature on this subject. Other strengths of the study include the randomized study design and the fact that the descriptive characteristics of the groups were similar at baseline. The limitation of the study is that the results of the intervention cover one month, and the long-term effect remains unknown.
Conclusion
It was determined that telephone-based joint protection education in patients with LE was more effective in reducing pain and increasing awareness of functionality and joint protection behaviour compared to the home-based programme. Telephone-based joint protection education programmes can be a preventive and protective health service approaches for LE patients, especially in periods of limitation in face-to-face healthcare services such as living away from a health center or a pandemic situation.
In future studies, the effect of telephone-based joint protection technique should be evaluated with individuals of different ages and diagnosis and compared with different intervention methods. Besides, following the results of telephone-based intervention studies in the long term; these practices are considered to be important for determining in terms of costeffectiveness.
Footnotes
Acknowledgments
The authors would like to thank Biostatistician Prof. Dr. Necdet Süt (Trakya University) for his assistance in the statistical analysis of the study.
Conflict of interest
No potential conflict of interest was reported by the authors.
Funding
None to report.