
Abstract
BACKGROUND:
The physical factors associated with musculoskeletal pain in nursing personnel have been largely investigated, although the role of sleep and psychological factors resulting in musculoskeletal pain has not been addressed thoroughly.
OBJECTIVE:
This study aimed to explore the prevalence of musculoskeletal pain and investigate how sleep and psychological factors influence musculoskeletal pain in a nursing group.
METHODS:
Nordic standard questionnaires were distributed to 230 female nurses. Chi-square tests were performed to assess the associations between sleep problems, psychological problems, and musculoskeletal pain symptoms. Binary logistic regression analysis was also conducted to identify the primary factors influencing the prevalence of musculoskeletal pain.
RESULTS:
The highest prevalence of pain was observed in the lower back, neck, and shoulders, whereas the lowest prevalence of pain was observed in the ankles, feet, elbows, and hips/buttocks. Chi-square analysis and binary logistic regression showed that sleep duration, sleep onset time, and sleep quality all significantly contributed to the development of neck and upper back pain. With regard to the psychological factors, only occupational pride and stress had a significant effect on pain; in contrast, family support did not show any significant influence.
CONCLUSION:
Compared with other body regions, musculoskeletal pain in the lower back, neck, and shoulders requires more attention and preventive interventions. Special efforts should be made to shift the workday system of the nursing group because of the strong correlation between sleep problems and pain. Incentives other than penalty mechanisms should be considered seriously in nursing to boost occupational pride and relieve job stress.
Keywords
Introduction
Few epidemiological studies evaluating the prevalence of musculoskeletal pain among nursing personnel in China have been conducted or published. At the end of 2020, there were about 9 million beds in medical and health institutions nationwide, but only about 4 million registered nurses [1]. China only has 3.34 nurses per thousand people [1], while the United States has 11.8, Japan has 11.8, South Korea has 7.9 and Switzerland has 18.0 nurses per thousand people [2]. Statistics from the China Human and Social Security Department showed that most nurses have to perform night shift work and repetitive activities, such as stooping the wrist and inclining their neck, more frequently than the personnel belonging to other occupational groups [3]. Moreover, nurses need to maintain the balance between work and family life, thus increasing their risk for impaired sleep quality. With the development of the concept of high-quality nursing and increasing public demand for healthcare services, pressure on the nursing profession is increasing, which imposes a psychological workload on the nursing group.
Work-related musculoskeletal disorders (WRMSDs) are becoming increasingly prevalent among nurses [4]. The prevalence of musculoskeletal pain in the medical industry is relatively high and is 40%–92% in nurses [5–7]. The incidence rates of skeletal muscle pain in the lower back, neck, shoulder, and hip/leg were 72% [7], 61.21%, 57.82%, and 51.03%, respectively [8]. Musculoskeletal pain imposes large costs on the employees and society [9] and may have numerous consequences, such as reduced quality of life, occupational disability, absence of sickness, and changing or discontinuing a profession [10, 11].
The reasons for musculoskeletal pain have aroused the interest of researchers over the past decades. Musculoskeletal disease is a complex pathological condition caused by a number of factors. Environmental, psychological, individual, and other factors contribute to the occurrence of musculoskeletal diseases [12]. Epidemiological studies have shown that awkward postures, heavy manual handling and transfer of patients, repetitive movements, monotonous tasks, and standing for prolonged hours are ergonomic risk factors associated with nursing jobs [13–15]. Age, sex, workload, and work department are also important risk factors for musculoskeletal diseases [16, 24]. However, previous studies have mainly focused on examining the physiological factors related to musculoskeletal pain in nursing personnel, with little consideration on the effects of psychological factors and sleep deprivation.
The remainder of this paper is organized as follows: Section 2 introduces the study’s methodology. Section 3 presents the results of the study. Finally, the discussion and conclusions are presented in Sections 4 and 5, respectively.
Methods
Participants
From April 2021 to June 2021, a panel of registered female nurses working in a first-class hospital in Beijing were recruited, and their musculoskeletal pain and related factors were investigated. All participants from the intensive care units, wards, emergency rooms, operating rooms, and other departments had >12 months of work experience. The total sample size was 189, and the participants’ average age was 29.8 years. The average working age was 7.7 years, the average height was 162.4 cm, and the average weight was 56.9 kg. The study was approved by the Ethical Review Committee of the university, and written informed consent was obtained from all participants.
Inclusion criteria: (1) Worked in the hospital for ≥1 year; (2) Have a nurse practitioner qualification certificate; (3) No rotation to other departments within 12 months; (4) Voluntarily participation in the research and sign the informed consent form.
Exclusion criteria: (1) Nurses who are currently not on the job, such as those who go out for further study, maternity leave and sick leave; (2) Nurses who are pregnant and lactating within 1 year; (3) Nurses with musculoskeletal injuries caused by non-work factors such as congenital spinal disorders, tumors, and gynecological diseases; (4) Those with a clear history of trauma and surgery in the past 1 year; (5) Practical nurses.
Interview
Before the distribution of questionnaires, all experienced nurses were interviewed to identify the most probable risk factors for musculoskeletal pain. The first edition of the questionnaire was distributed to these nurses, and any suggestions for revising the questionnaire were obtained. The interviewed nurses from various wards were investigated to improve the reliability of the study and were found to have at least 3 years of nursing experience. The interview verified the questionnaire’s aptness for determining the employment characteristics and clarity of the included questions.
Questionnaire
The questionnaire used in this study was developed based on the Nordic standard questionnaire [17], translated into Chinese language by the corresponding author, and evaluated by a professional panel. It includes questions that assess the symptoms and duration of musculoskeletal pain over the last 12 months. The collected data were derived from three main aspects. The first part involved the collection of anthropological information (age, body mass index (BMI), marital status, current occupational ward, and nursing experience). The second part involved the collection of the following potential psychological and sleep factors: sleep quality, sleep duration, family support, work satisfaction, and stress. The last part involved the collection of pain reports from the nine body regions. Sleep quality can be classified into the following three levels: high, intermediate, and low. The sleep duration was grouped into three categories: <6 hours, short sleep; 6–8 hours, reference group; and >8 hours, exceeding level. The sleep onset time was divided into three categories: before 11 pm, 11 pm to 12 am, and after 12 am. The psychological factors included occupational pride and work stress, both of which had three levels: high, intermediate, and low. The outcome of musculoskeletal pain was measured using the Nordic standard questionnaire with an explainable picture in addition to the questions; the reliability and validity of this questionnaire have previously been validated [18]. The last part of the questionnaire involved the assessment of the nine body regions (neck, shoulders, elbows, wrists/hands, upper back, lower back, hips/buttocks, knees, and ankles/feet) marked in the picture to help nurses understand the appointed areas.
The participants were required to complete the questionnaire independently and anonymously to ensure that the data reflected the actual situation. We distributed 230 questionnaires to the nurses and received 205 (89%) answered questionnaires. The questionnaire response rate was higher than the minimum rate (70%) recommended by the National Institute for Occupational Safety and Health for epidemiological studies [19]. After filtering, a total of 189 questionnaires were retained for the study.
Data analysis
SPSS version 19.0 [20] was used to conduct the statistical analysis. Chi-square tests were performed to assess the associations between sleep problems, psychological problems, and musculoskeletal pain symptoms (yes or no). Binary logistic regression analysis was conducted to identify the primary factors affecting the prevalence of musculoskeletal pain. The odds ratio (OR) of chi-square and logistic regression can determine whether the factors’ changes are synergistic (>1) or antagonistic (<1). A P-value <0.05 was considered significant, and only associations with significance were reported.
Results
Statistics of general characteristics
Questionnaires were collected 3 days after distribution. The demographic data of the study sample, including age (18–58 years, mean: 29.8 years), assigned ward, marital status, and BMI (mean: 21.6), were presented. In the study conducted by the World Health Organization in the Asian population, the standard BMI was between 18.5 kg/m2 and 23 kg/m2, and a BMI of >23 kg/m2 was considered overweight. More than 50% of the participants had normal interregional BMI. Other data about our samples are presented in Table 1.
Demographics of the participants (N = 189)
Demographics of the participants (N = 189)
A total of 189 available nurses were included in the study. The most commonly reported musculoskeletal pain symptom was observed in the lower back, with an overall prevalence of 172 (91.0%). This was followed by musculoskeletal pain in the neck (170, 89.9%), shoulders (152, 80.4%), and upper back (149, 78.8%). Pain in these four body regions was more frequent than that in the other five regions. Pain in the hips/buttocks was the least reported pain (54, 28.6%). The percentage of musculoskeletal pain symptoms in all nine body regions is shown in Table 2.
Number and rate of the nurses with MSDs (N = 189)
Number and rate of the nurses with MSDs (N = 189)
The three groups of sleep durations, i.e., 6–8 hours, <6 hours and >8 hours a day, varied significantly based on the frequency of musculoskeletal pain in different body regions (as shown in Table 3 and Fig. 1). The frequency of neck musculoskeletal pain, upper back musculoskeletal pain, knee musculoskeletal pain, and ankle/foot musculoskeletal pain were 12.35 times (p = 0.002, OR = 12.35, confidence interval [CI] = 1.608–95.328), 4.12 (p = 0.002, OR = 4.12, CI = 1.611–1.467) times, 2.55 (p = 0.004, OR = 2.55, CI = 1.346–4.814) times, and 2.19 (p = 0.012, OR = 2.19, CI = 1.179–4.050) times higher in the group with a sleep duration of <6 hours a day than in the group a with a sleep duration of 6–8 hours. Relatively, nurses who slept >8 hours a day had 1.10 (p = 0.038, OR = 1.10, CI = 0.851–5.175) times higher risk of developing wrist/hand musculoskeletal pain than those who slept 6–8 hours. However, little difference was observed in the musculoskeletal pain of the shoulders, elbow shoulders, lower back, and hips/buttocks between the three groups.
Sleep problems associated with the presence of MSDs at multiple body regions
Sleep problems associated with the presence of MSDs at multiple body regions
*Whole participant showed MSDs symptom; 1Three different groups of duration of sleep: reference is the 6 to 8 hours, the other two are less than 6 hours and more than 8 hours; 2Three different groups of sleep onset time: reference is between 9 and 11 PM, between 11 PM and 12 PM and after 12 PM; 3Three different groups of sleep quality: reference is high, intermediate and low; 4Differences between groups evaluated using the Chi-square test.

Prevalence of MSDs by body regions at different sleep problems levels.
Based on the sleep onset time, the participants were divided into three groups, i.e., 9–11 pm group, 11 pm–12 am group, and after 12 am group, which only showed remarkable differences in the prevalence of neck musculoskeletal pain and upper back musculoskeletal pain. Sleep onset time at 11 pm–12 am was associated with a 3.75-fold higher risk (p = 0.039, OR = 3.57, CI = 0.998–12.815) of developing neck musculoskeletal pain, while sleep onset time at 9–11 pm was associated with a 3.45-fold higher risk (p = 0.008, OR = 3.45, CI = 1.334–8.864) of developing upper back musculoskeletal pain.
In terms of sleep quality (i.e., high, intermediate, and low), the following six regions were significantly affected: neck, shoulder, upper back, lower back, hips/buttocks, and knees. Low sleep quality was associated with a 35.8-fold (p < 0.001, OR = 35.8, CI = 4.367–294.040) higher risk of developing neck musculoskeletal pain, 5.39-fold (p < 0.001, OR = 5.39, CI = 2.087–13.922) higher risk of developing shoulder musculoskeletal pain, 4.76-fold (p = 0.001, OR = 4.76, CI = 1.834-12.390) higher risk of developing upper back musculoskeletal pain, 7.26-fold (p = 0.002, OR = 4.76, CI = 1.834–12.390) higher risk of developing lower back musculoskeletal pain, 2.9-fold (p = 0.040, OR = 2.9, CI = 1.016–8.275) higher risk of developing hip/buttock musculoskeletal pain, and 2.33-fold (p = 0.037, OR = 2.33, CI = 1.041–5.248) higher risk of developing musculoskeletal pain in the knees compared with high sleep quality. Meanwhile, intermediate sleep quality was associated with a 3.125-fold (p = 0.028, OR = 3.125, CI = 1.101–8.870) risk of developing neck musculoskeletal pain compared with high sleep quality and 2.96-fold higher risk (p = 0.017, OR = 2.96, CI = 1.190-7.372) of developing shoulder musculoskeletal pain.
Compared with the previous two factors, the association between psychological problems and musculoskeletal pain symptoms was less significant (as shown in Table 4 and Fig. 2). The levels of occupational pride, stress, and family support were divided into three groups: high, intermediate, and low. Results indicated that nurses with low occupational pride were 8.80 times (p = 0.004, OR = 8.80, CI = 1.602–48.386) more likely to experience neck musculoskeletal pain and 2.48 times (p = 0.039, OR = 2.48, CI = 1.306–5.950) more likely to experience wrist/hand musculoskeletal pain than those with high occupational pride. Relatively, intermediate stress was associated with a 0.376-fold higher risk (p = 0.035, OR = 0.376, CI = 0.148–0.951) of hip/buttock musculoskeletal pain than low stress, while high stress was associated with a 2.897-fold higher risk (p = 0.027, OR = 2.897, CI = 1.099-7.637) of upper back musculoskeletal pain than low stress. Moreover, occupational stress had a slight effect on other body regions, while the effect of family support was not remarkable according to the result.
Psychology problems associated with the presence of MSDs at multiple body regions
Psychology problems associated with the presence of MSDs at multiple body regions
1The three levels of occupational pride: reference is high, intermediate and low; 2The three levels of the stress: reference is high, intermediate and low; 3The three levels of family support: reference is high, intermediate and low; 4Differences between groups evaluated using the Chi-square test.
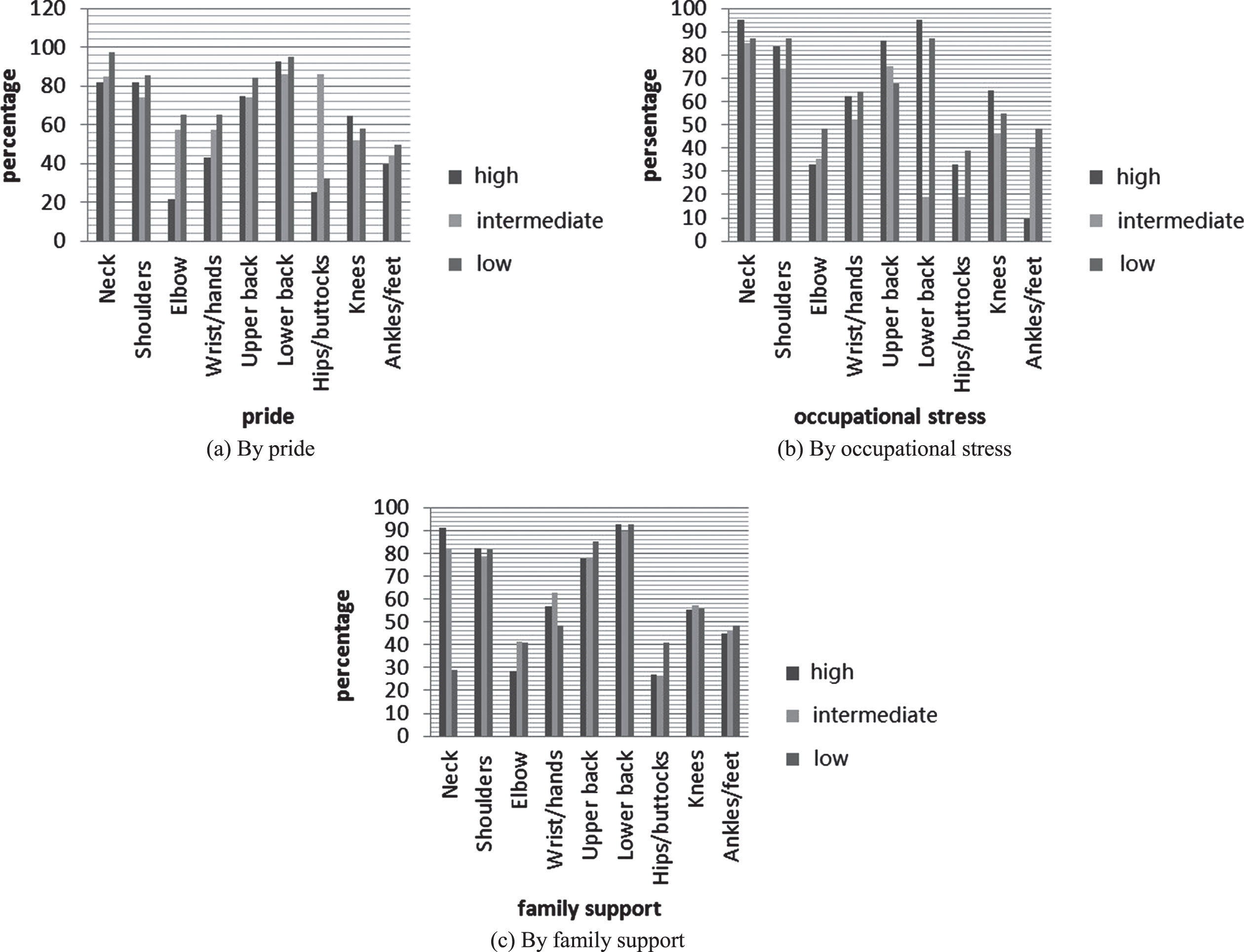
Prevalence of MSDs by body regions at different psychological levels.
Binary logistic regression analysis showed the most influential factors in the eight body regions, excluding wrists/hands. In the regression model, as shown in Table 5, sleep quality was the primary factor contributing to the occurrence of musculoskeletal pain in the neck, shoulders, and upper back (pneck = 0.005, pshoulders < 0.001, plower back = 0.003). The duration of sleep was observed only in the shoulder model (p < 0.001), and the sleep onset time was the same in the upper back model (p < 0.001).
Binary logistic regression of risk factors
Binary logistic regression of risk factors
*No variable entry the logistic regression equation as important influential factors.
Prevalence of musculoskeletal pain in nurses
The prevalence of musculoskeletal pain among nurses is higher than expected. The trend of musculoskeletal pain in nurses has either emerged or even deteriorated in both developed and developing countries.
According to an investigation on the trend of musculoskeletal pain in nursing personnel in China [21], the prevalence rates of musculoskeletal pain in the lower back, neck, shoulder, and upper back were 56.7%, 42.8%, and 38.9%, respectively. However, the rates in our study were obviously higher than those reported in 2004, which were 91.0% for lower back, 89.9% for neck, 80.4% for shoulder, and 78.8% for upper back, indicating that the measures taken for musculoskeletal pain have not achieved great progress. In clinical practice, nursing interventions primarily focus on changing the shift frequency to help nurses prevent musculoskeletal pain. Takahashi et al. [22] found that inappropriate shift work can lead to sleep problems among nurses and induce musculoskeletal pain. Moreover, rapidly aging societies may limit the effectiveness of such preventive interventions.
A longitudinal comparison of musculoskeletal pain among nurses in different countries is discussed further. Studies have shown that the prevalence of musculoskeletal pain among clinical nurses has been increasing in recent years, and the risk in developing countries is higher than that in developed countries [14]. The prevalence rates of musculoskeletal pain among nurses were 69% in the United States, 74.9% in Brazil [23], 88.8% in Turkey [24], 70.8% in South Korea [25], and 61% in Iran [26]. Due to the differences in the levels of economic and medical development in various countries, the health management systems, human resources, nursing work content, working conditions, and geographical environments vary. The prevalence of musculoskeletal pain is inconsistent, and the location of the disease differs. Chinese scholars have reported that the prevalence rate of musculoskeletal pain among healthcare workers in China is 84%–87.46%, which is relatively high. The main reason for this difference is that with the continuous development of medical technology and the improvement in people’s healthcare needs, the load of medical work is constantly increasing every year, and nursing shortage occurs, resulting in heavy work, high work pressure, and high risk of musculoskeletal pain in nurses. The organizational management of relevant support facilities and protection training programs remains inaccurate, leading to work overload for a long-term period and the high prevalence of musculoskeletal pain among nurses. Some regulations are aimed at preventing the occurrence of musculoskeletal pain among healthcare workers in the European Union [27] and the United Kingdom [28].
Risk factors of sleep problems and musculoskeletal pain among nurses
The chi-square test showed that sleep quality had a more significant impact on musculoskeletal pain compared with sleep duration and sleep onset time, especially pain in the neck, shoulders, upper back, and lower back. Furthermore, through a comparison with the other factors in this study, sleep quality acts as the main function in the binary logistic model of the neck, shoulder, and upper back. The binary logistic results showed that the different factors were not in the same status when analyzing different body regions. The result of the chi-square test on the three factors of sleep problems is consistent with that reported in other studies [22]. In addition, the effect of sleep quality is greater in the neck, shoulders, and upper back. One of the body regions that was severely influenced by sleep problems was the neck. Improvement in sleep quality could lead to a reduction in the severity of musculoskeletal pain. Taking regular naps and establishing regular waking time and sleep time would improve sleep quality.
Based on the results of previous studies on sleep area, non-restorative sleep is one of the reasons for the occurrence of pain, thus requiring a deeper understanding of the link between these two factors. Some studies have attempted to explain the mechanism by which sleep accelerates pain the next day. Poor sleep quality may not relax the muscles at night, causing disturbance in the blood circulation [29]. Sleep deprivation induces hyperalgesia by decreasing the descending pain-suppressing activity and increasing the descending pain-facilitating activity [30], as well as inducing agitation, a high stress response, and unpleasant emotional and psychological reactions in patients, and even leads to more severe complications [31]. Sleep deprivation among medical staff may cause sleepiness while working night shifts, sudden insomnia and tardiness. The biological clock plays an important role in human health, and disruption of the biological clock has adverse effects on the body [32]. Nurses often work night shifts, which can lead to disturbance of the biological clock, affecting their sleep, diet, family life, and social activities and causing changes in the endocrine system. In addition, involuntary neurological symptoms such as immunosuppression, colds, gastrointestinal infections, and allergies can also occur. Staying up late for long periods leads to insomnia, forgetfulness, irritability, anxiety, and other neurological and psychiatric symptoms. This study showed that nurses with irregular work schedules, who frequently work night shifts, or who stay up late had the highest prevalence of WRMSD.
Following regular sleeping patterns to improve the sleep quality can help nurses relieve pain. Healthy sleep requires good sleep quality, reasonable time to fall asleep, and proper sleep duration, which can help reduce the development of musculoskeletal pain. Good sleep habits, proper exercise, avoidance of alcohol and caffeine, and attention to the details of sleep habits can improve the sleep quality. In addition, it is necessary to establish a reasonable shift system, and nurses who work night shifts should live in an area that is close to the hospital that they are working in to avoid further delay in sleeping.
Psychological factors that increase the risk of musculoskeletal pain among nurses
In the last 10 years, an increasing number of researchers have reported an association between psychosocial factors and musculoskeletal pain. A study by the National Institute for Occupational Safety in the United States suggested a correlation between psychosocial factors and the occurrence of occupational musculoskeletal injuries [33]. Dinora et al. [34] conducted a meta-analysis of 24 articles on psychosocial risk factors of hospital nurses and showed that the psychosocial risk factors of nurses in the workplace were related to WRMSDs. This result is consistent with the conclusions of other researchers [35, 36]; i.e. psychosocial factors are important factors influencing WRMSDs. This study showed that among the psychological factors, professional pride and stress had significant effects on pain, while family support had no significant effect on pain.
To determine an efficient measurement that can help decrease the risk, some studies attempted to explain the mechanism of stress with the indication that the interaction between stress and musculoskeletal pain is complex, contributing to the development of musculoskeletal pain [37]. Pain conduction starts from the spinal cord and continues to the brain center. Human pain sensation is the result of the combined action of many ascending and descending facilitation and inhibition pathways [38]. Persistent stress can induce, sustain, and intensify pain sensitivity, thereby modulating pain perception [39]. Chronic pain triggers dysfunction in the pain-related regions of the central nervous system such as the insula, limbic system, and anterior cingulate gyrus. These areas have been related to people’s psychological emotions, which shows that chronic pain not only is a complex process of central lesions but also causes changes in psychological emotions. Mindfulness therapy [40], founded by Dr. Kabat-Zinn in 1979, is effective in treating chronic pain. Mindfulness therapy can change a patient’s perception of pain, strengthen the acceptance of pain sensation, and improve physical function by reducing psychological pressure. In addition, because of the differences in male and female psychology, the level of musculoskeletal pain also differs. The difference between women and men in terms of the level of musculoskeletal pain is mainly associated with the inherent psychological characteristic because women are passive when receiving interventions.
Therefore, nursing managers should pay more attention to decreasing the prevalence of musculoskeletal pain among nurses, reducing the known occupational risk factors from a management perspective, focusing on the mental health of the medical staff, helping them relieve psychological pressure, improving professional pride, and striving to create a safe and harmonious cultural environment.
Limitations of the study
It is necessary to elucidate the findings of this study with a certain degree of caution. This conservatism is due to the limited sample size owing to the demographic characteristics or musculoskeletal pain classification. The possible selection bias cannot be dismissed because our investigation excluded nursing students, retired nurses, male nurses, and nurses in common class hospitals. Sometimes, nursing students undertake the most physical work tasks, and some nurses resign due to serious musculoskeletal pain. Moreover, in some countries, male nurses account for a considerable proportion of nursing staff, and the condition of musculoskeletal pain among nurses may vary in different classes of hospitals. In addition, the effect of smoking, alcohol consumption, and being overweight on musculoskeletal pain in nurses was not addressed in this study. Nurses’ educational background and lack of formal on-the-job training are both factors that should be considered in future studies. The results may also be influenced by recall bias since the data analysis was based on self-reported questionnaires. Research efforts using more objective measures to assess musculoskeletal pain in nursing personnel, for example, widely accepted clinical tests [36] or approaches utilizing electromyography, would be required to verify the results. Further longitudinal epidemiological research should be conducted to identify the common trajectories.
Conclusions
This study evaluated the prevalence of musculoskeletal pain and the associated risk factors among Chinese female nursing personnel, i.e. sleep and psychological problems. Compared with other body regions, musculoskeletal pain in the lower back, neck, and shoulders requires more attention and preventive interventions. Sleep problems may explain the casual musculoskeletal pain in the neck, shoulders, and upper back. Psychological factors such as occupational pride and job stress also have a potential influence. To help alleviate the burden of musculoskeletal pain, great measures should be taken to improve work organizations, create good work schedules, and ensure psychological guidance. Special efforts should be made to shift the workday system of the nursing group because of the strong correlation between sleep problems and pain. Incentives other than penalty mechanisms should be considered seriously in nursing to boost occupational pride and relieve job stress. The multifactorial course for musculoskeletal pain highlights the need for research on preventive interventions from organizational and psychosocial considerations.
Footnotes
Acknowledgments
The authors are grateful to all the nursing personnel who participated in this study and to the specific hospital in Beijing for their assistance in conducting this study. The authors would also like to express their gratitude to the University of Science and Technology Beijing for providing administrative and technical support.
Conflict of interest
None of the authors have any conflicts of interest to declare.
Funding
The authors do not have any funding to disclose.
Ethical considerations
The study was approved by the Ethical Review Committee of the university.
Informed consent
Written informed consent was obtained from all participants.