
Abstract
BACKGROUND:
Musculoskeletal disorders (MSDs) are the most common work-related injuries identified among caregivers in the health sector as a high-risk group.
OBJECTIVES:
The study aimed to investigate the factors that influence musculoskeletal disorders among caregiver and to evaluate the relationship between work and non-work related factors with MSDs.
METHODS:
Data were collected from 104 caregivers using descriptive design and stratified cluster sampling. The survey included a demographic questionnaire and a Nordic Standardized Musculoskeletal Questionnaire. Logistic regression was performed to determine the risk factors associated with MSDs. The Odds ratio (OR) was calculated to define the influence of each risk factors. In addition, we used forward logistic regression analysis to validate the predictive model.
RESULTS:
In this cross-sectional survey, the results showed that 70 (67.3%) participants reported MSDs. MSD was highest at the lower back (46%), then knee (15.4%) and shoulder (11.5%). The overall success of the prediction is 90.4% (94.6 for having MSDs). The most important risk factors were manual handling (p < 0.001, odds ratio = 45.64) followed by bending (p = 0.008, odds ratio = 39.4).
CONCLUSIONS:
The results of this study reaffirmed the high prevalence of work-related MSD among caregiver’s primarily in the lower back. The most important risk factors were manual handling, followed by bending / twisting, and handling of an excessive number of patients. Therefore, it is necessary to consider appropriate policies for managing MSDs among caregivers.
Introduction
Musculoskeletal disorders are a pervasive and widespread work-related problem worldwide, and health caregivers have been identified as high-risk groups with injuries [1]. Increased risk has been established in professions involving extremely repetitive work, vigorous effort, uncomfortable posture, and heavy lifting [1, 2]. Other risk factors include mechanical overload, exposure time, repetitive activity, and postural requirements. In addition, physical requirements, working conditions, and workplace organization have been identified to distress the physical and mental health of the caregivers [3]. In addition, tight schedules, little participation in decision-making and task consignment, severe observation, lack of communication, absence of clarity of work functions and the time to perform them are considered situations for nurses [4].
In healthcare service, work-related MSDs are common, with rate of prevalence ranging from 28% to 96% over a one-year period [5]. In addition, work-related MSDs (WMSDs) are common causes of occupational disorders among healthcare authorities around the world [6, 7]. These are common among the caregivers worldwide (40–90%) [8, 9]. WMSD has been regarded as a major cause of absenteeism from nursing professionals [10]. Caregivers have a very high prevalence of MSD, according to data reported worldwide, i.e. 89% in Portugal [11], 32.8% to 57.1% in Brazil [12], 10% to 50% in France [13], 85% in Macedonia [14], 78.6% in China [15], 88% in Iran [16] and 35.1% to 47% in the United States [17].
Healthcare professionals suffer from a relatively high prevalence of back, neck, and shoulder disorders. The prevalence of work-related MSDs among nurses varies from study to study. Salama and Eleshenamie [18] reported that 99.0% of nurses were affected by MSD while studying risk factors for 300 nurses. Clari et al. [19] revealed one or more cases of upper limb disorders among 48.3% of nurses. Cheng et al. [20], used a standardized Nordic musculoskeletal questionnaire for 470 nurses with a prevalence of MSD at the waist (77.2%), neck (64.2%), and shoulders (58.7%). Chen et al. [21] conducted a survey of nurses’ musculoskeletal discomfort at 793 health facility and reported neck discomfort (63.5%), shoulder discomfort (62.6%), and lower back discomfort (59.3%). In addition, they concluded that there was a correlation between the amount of work done by nurses and their satisfaction with their work and the amount of discomfort in their musculoskeletal system.
As far as we know, the prevalence of WMSD among caregivers and related factors are significant for healthcare service policy managers and professionals to reduce the presence of problems. Therefore, it is necessary to determine the distribution of WMSDs among caregivers. In this study a Nordic standardized questionnaire was used to examine the prevalence of WMSD in caregiver employed in Saudi Arabian hospitals. Therefore, this study aims to serve as a survey paradigm for benchmarking for policymakers to apply the suggested guideline which can reduce musculoskeletal discomfort in caregivers and thereby improve the quality and performance of nursing care. This study assesses the exiting status and risk factors that affect WMSDs among caregivers. Therefore, the study aimed to investigate the factors that influence musculoskeletal disorders among caregiver and to evaluate the relationship between MSD and factors related to workload.
Method
Study design
The study aimed to investigate the factors that influence musculoskeletal disorders among caregiver in Saudi private hospitals in Saudi Arabia and also to evaluate the relationship between MSD and factors related to workload. The research protocol followed in this study was approved by ethics review boards in Saudi Arabia with permission from the Ministry of Health and University of Central Florida Institutional Review Board (IRB: SBE-15-11723). To be able to estimate the results, we calculated the sample size and implemented a sampling method to secure a representative sample. Full-time caregivers (26 male and 78 female) voluntarily participate in this study (only those who are eligible to receive benefits from a private hospital in Saudi Arabia) and report injuries while working in the hospital, and receive compensation, treatment, or holidays. However, participants were excluded if they did not meet the eligibility criteria or if they did not fully respond to the survey. All caregivers enrolled in the hospital are qualified and have at least a bachelor’s degree or diploma degree.
Data collection
Data were collected using a self-assessment questionnaire based on the internationally recognized “Standardized Nordic Questionnaire”. The reliability and validity of the assessment of musculoskeletal disorders by questionnaires have also been established in numerous other studies [20, 21]. The SNQ was used to assess areas of the body such as wrist / hand, upper back, shoulders, neck, lower back, knee, hip / thighs, and elbow / forearm. Questions were asked about workplace obligations and various other work factors, including questions about the employment sector, the number of patient movements or lifts per shift, and the occurrence of extreme psychological pressure throughout working hours. Specific questions were also asked about the occurrence of musculoskeletal disorders over the last 12 months and whether medical advice was sought or sick leave was taken. During the assessment, the participants were quizzed about the compensation claims and the amount received from those claims. Job-independent risk factors were asked about including their daily lives activity, which could affect their health. In addition to factors that increase the risk of MSD (such as the insufficient number of nursing staff and manual lifting of patients), we also assess the potential association of various other risk factors with MSD in the form of smoking habits and physical characteristics. Participants (caregivers) were contacted and asked to participate in the survey before the actual interview took place. An interview was conducted separately for each caregiver at a time. Participants were informed about the voluntary nature of our study and were not offered any penalties or rewards for participation or refusal to participate in the study. Informed written consent was implied before the participant answered and returned the questionnaire.
Predictive modelling and variable selections
Predictive models play an important role in establishing the relationship between the variables used in a particular model and the results achieved, and help predict the future of the proposed results. Predictive models provide information about the variables that determine the outcome, the strength of the association with the outcome, and specific values can be used to predict the future of the outcome. Variable selection means choosing from a large number of variables to include in a particular model, that is, choosing the right variable from the complete list of variables by removing irrelevant or redundant variables [22]. The purpose of such a choice is to determine the optimal set of variables for the model so that accurate predictions can be made. It is often advised that variable selection should focus on clinical knowledge and previous literature rather than on statistical selection methods alone [23]. The data often contains many additional variables that are not ultimately used in model development [24]. Therefore, careful selection of appropriate variables should be made so that the final model does not contain noise variables. With this approach the study predictive model analysis was performed using logistic regression analysis to predict the prevalence of MSDs in caregivers using gender, height, time, and stress: concern for health, performing strenuous physical activities, bending, manual handling, sleep, repetitive task, excessive quantity of patients, adjusting plinth/bed height to stretch and change posture, not resting frequently, fatigue, fixed position for prolonged time and physical satisfaction as predictive selection variables.
Statistical analysis
Data were analyzed using statistical version 20.0 of IBM SPSS software. Descriptive statistics were applied to analyze the prevalence of musculoskeletal disorder (MSD) from survey data. A chi-square test was used to examine fluctuations in the occurrence of MSDs. Logistic regression is used to get the odds ratio when multiple explanatory variables are present. The result is the effect of each variable on the odds ratio of the observed event of interest. The main advantage is to avoid confounding effects by analyzing the associations of all variables. Therefore, logistic regression analysis was executed to define the risk factors associated with MSD, and the odds ratio (OR) was used to define the contribution of each risk factors. In addition, to validate the predictive model a forward logistic regression was performed.
Results
Prevalence of MSD and association with participants’ demographics
The results of the survey showed that 20 women and 14 men did not have an MSD, while 58 women and 12 men reported an MSD (Fig. 1). The survey includes 84 participants from age group of 20–30 years, 12 participants from age group of 30–40 years and 8 participants from age group of 40–50 years. The results showed a significant effect of age group on the development of MSDS. In addition, MSD was highest at the lower back (46%), knee (15.4%) and shoulder (11.5%), neck (7.7%), wrist / hand (7.7%), hips / thighs (5.8%), upper back (3.8%) and elbow / forearm (1.9%) (Fig. 2). Figure 3 shows that 36 participants experienced their first MSD after 5 to15 years of graduation and 24 caregivers after 5 years of graduation, while 12 indicated before nursing training and 10 were unsure. In addition, 20 participants (19.2%) had changed fields of work, while 14 participants had changed careers due to the development of MSDs. Additional characteristic information was collected from the study sample population regarding the costs of MSDs. Questions regarding the cost of injuries revealed that the caregiver’s compensation was on average $ 685, while they spent an average of 3 days off work.
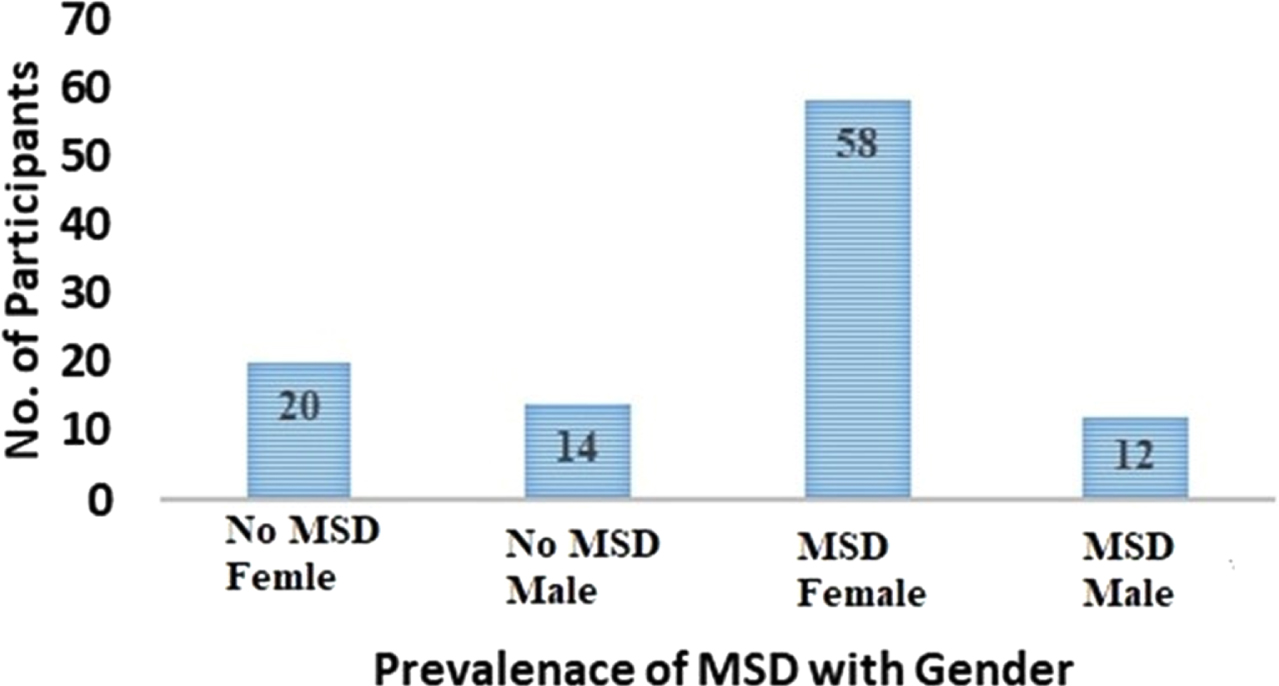
Development of MSDs in the participants with respect to gender.
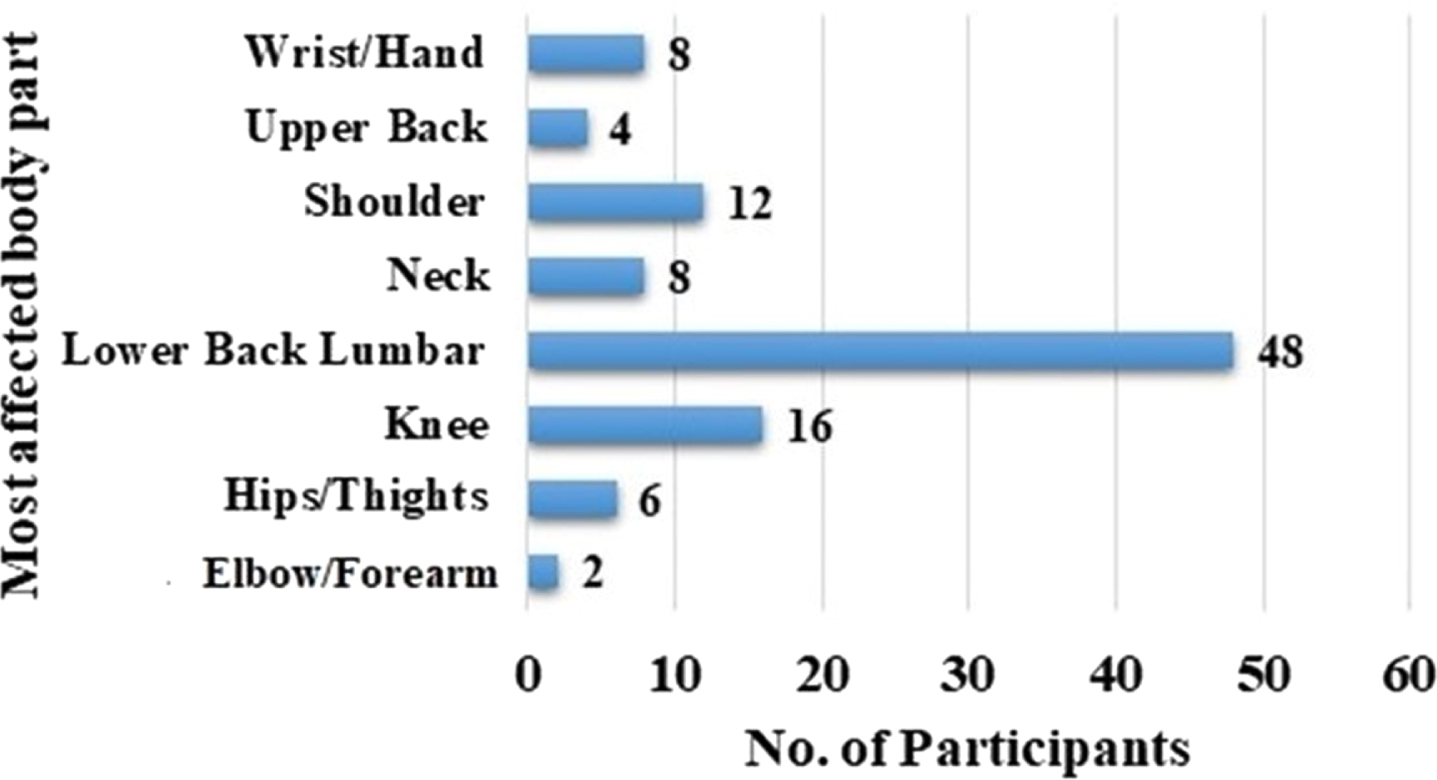
Most affected body parts with respect to participants.
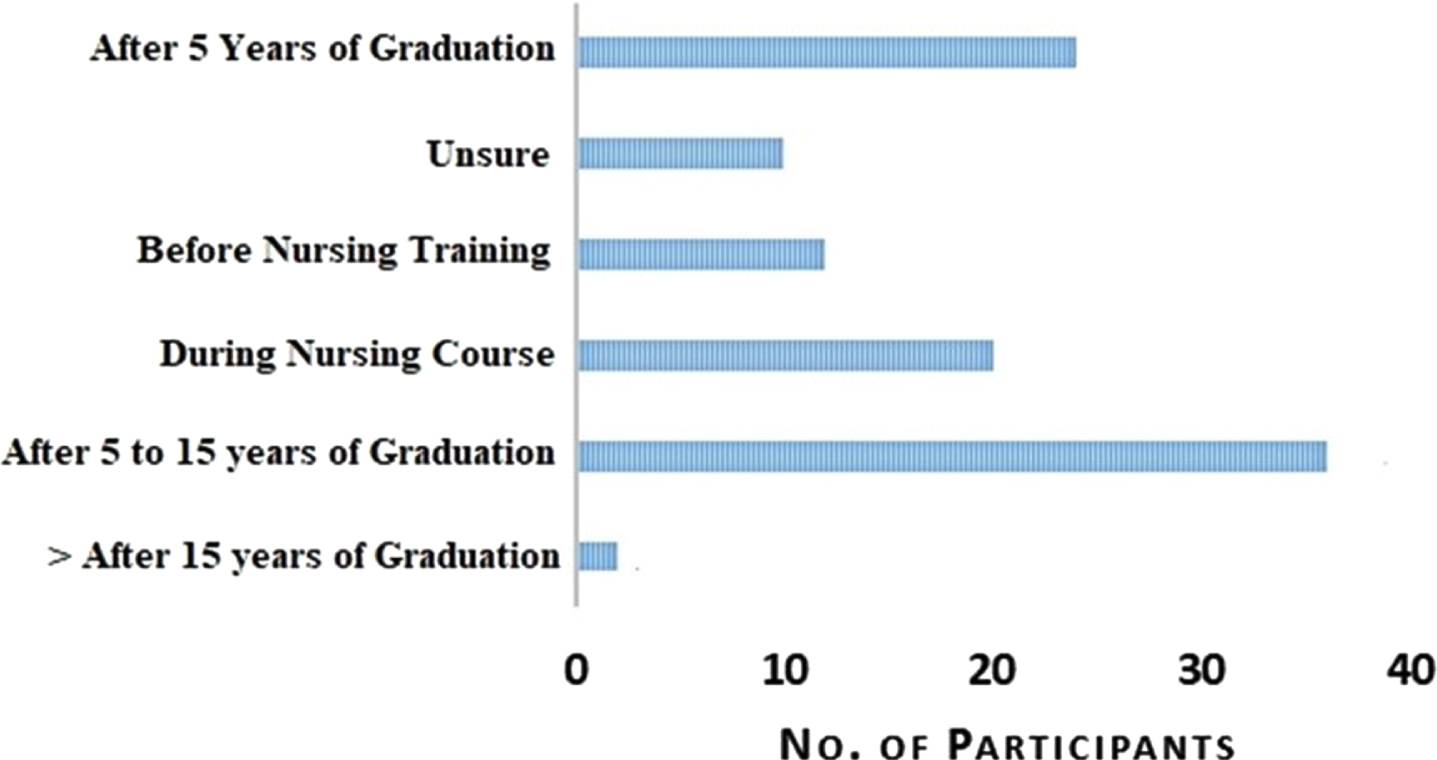
Development of first MSDs based on experience of the participants.
A better understanding of the relationship between various risk factors and MSDs to define which risk factors are controllable and can impact the development of policies aimed at improving the overall quality of occupational health among healthcare workers/ caregivers. To meet this requirement, a predictive model was developed using logistic regression analysis based on work-related and non-occupational risk factors that identifies and prioritizes high risk factors related to MSD. Therefore, assessment of these risk factors has the potential to avoid the prevalence of MSD and its impact on both patients and caregivers. The predictive model analysis was performed using logistic regression analysis to predict the prevalence of MSDs in caregivers using height, time, and stress: concern for health, performing strenuous physical activities, bending, manual handling, sleep, repetitive task, and excessive quantity of patients as predictors.
Predictive model based on the association of demographic data strategies
Predicted MSDs = 140.98 + 0.14 *(weight) – 0.09 *(height) + 3.37 *(gender).
Predictive model based on association of injury prevention strategies
Predicted MSDs = 0.38 + 1.66 *(not resting frequently) – 1.12 *(Adjusting plinth/bed height to stretch and change posture).
Predictive model based on association of physical health
Predicted MSDs = – 4.32 + 1.72 *(body pain) – 2.04 *(physical satisfaction) + 3.24 *(fixed position for prolonged time) + 1.70 * (feel worn out) + 1.58 *(fatigue) – 2.29 *(full energy) + 1.13 *(stress) – 1.89 *(concern for health).
The final predictive model equation: comprises nine variables for predicting MSDs, which are arranged by their odds ratios.
Predicted MSDs = – 27.10 + 3.82 *(manual handling) + 3.67 *(bending) + 2.89 *(large nos. of patients) + 2.53 *(repetitive task) + 1.31 *(physical activity at home) + 0.95 *(stress) – 2.76 *(sleep) +0.18 *(weight) – 0.24 *(height).
Predictive model summary
Testing the complete model against a constant model is statistically significant, and the predictor as a whole emphasizes making sure that there is a distinction between the presence and absence of MSDs (chi-square = 84.21, p < 0.001). In addition, Nagelkerke’s R-Square (0.794) shows that there is a robust association among prediction and grouping. In addition, the Cox and Snell R-squared statistics (0.555) imply that approximately 56% of the variation in expression is explained by the predictive model. The overall success rate of the prediction is 90.4% (94.56 with MSD, 80.1 without MSD) (Table 1). In addition, Wald’s criteria show that only the following factors contributed significantly to the prediction: manual handling (p < 0.001 and odds ratio = 45.64), bending (p = 0.079 and odds ratio = 39.4), excessive number of patients (p = 0.035 and odds ratio = 18.05), repetitive task (p = 0.038 and odds ratio = 12.58), performing strenuous physical activities at home (p = 0.024 and odds ratio = 3.69), emotional stress: concern for health (p = 0.011 and odds ratio = 2.6), sleep (p = 0.041 and odds ratio = 0.064), weight (p = 0. 041 and odds ratio = 1.2), height (p < 0.001 and odds ratio = 0.79). The results showed that the use of lift devices was not a significant predictor of MSD prevalence. However, it had the highest odds ratio for manual handling and was 45.64 times more likely to affect MSD than other factors.
Summary of data of the predictive model analysis
Summary of data of the predictive model analysis
Figure 4 shows how the model reflects well-defined relationships based on independent variables. In addition, the independent variable (predictive variable) with a lower predicted probability values corresponds to the defendant’s variable of zero observations. While, it also shows the relationships based on the independent variable (predictive variable) with a large predicted probability value corresponds well to the observed value with the value of the defendant variable. Therefore, the logistic regression curve has the ability to fit the data reasonably well. Figure 5 shows the changes in deviance and prediction probability. This figure helps identify observations that do not fit the model. The first curve extending from the lower left to the upper right represents (0 / No) to have an MSD. The second curve extending from the lower right to the upper left represents having an MSD (1 / Yes).
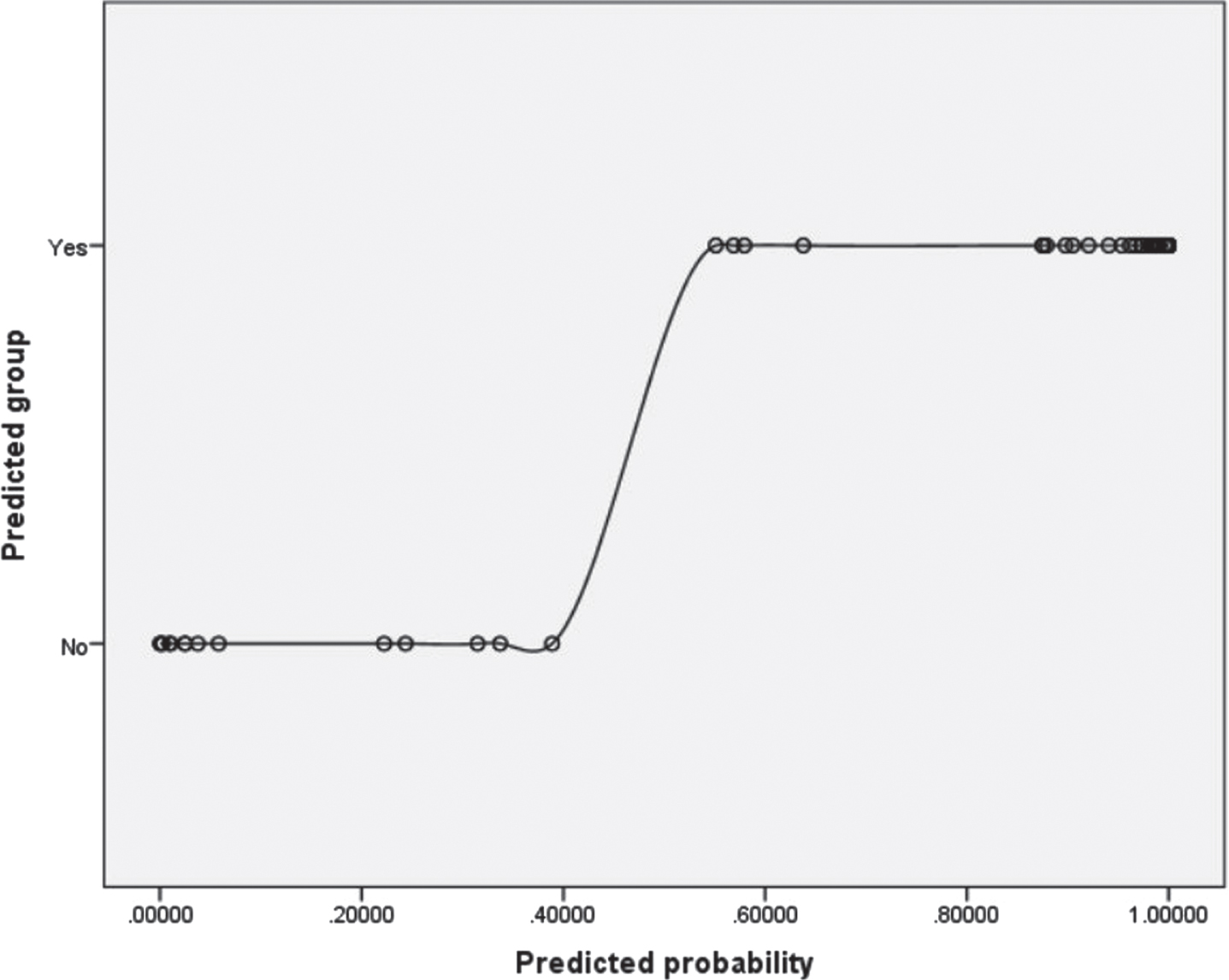
Predicted probability versus predicted group.
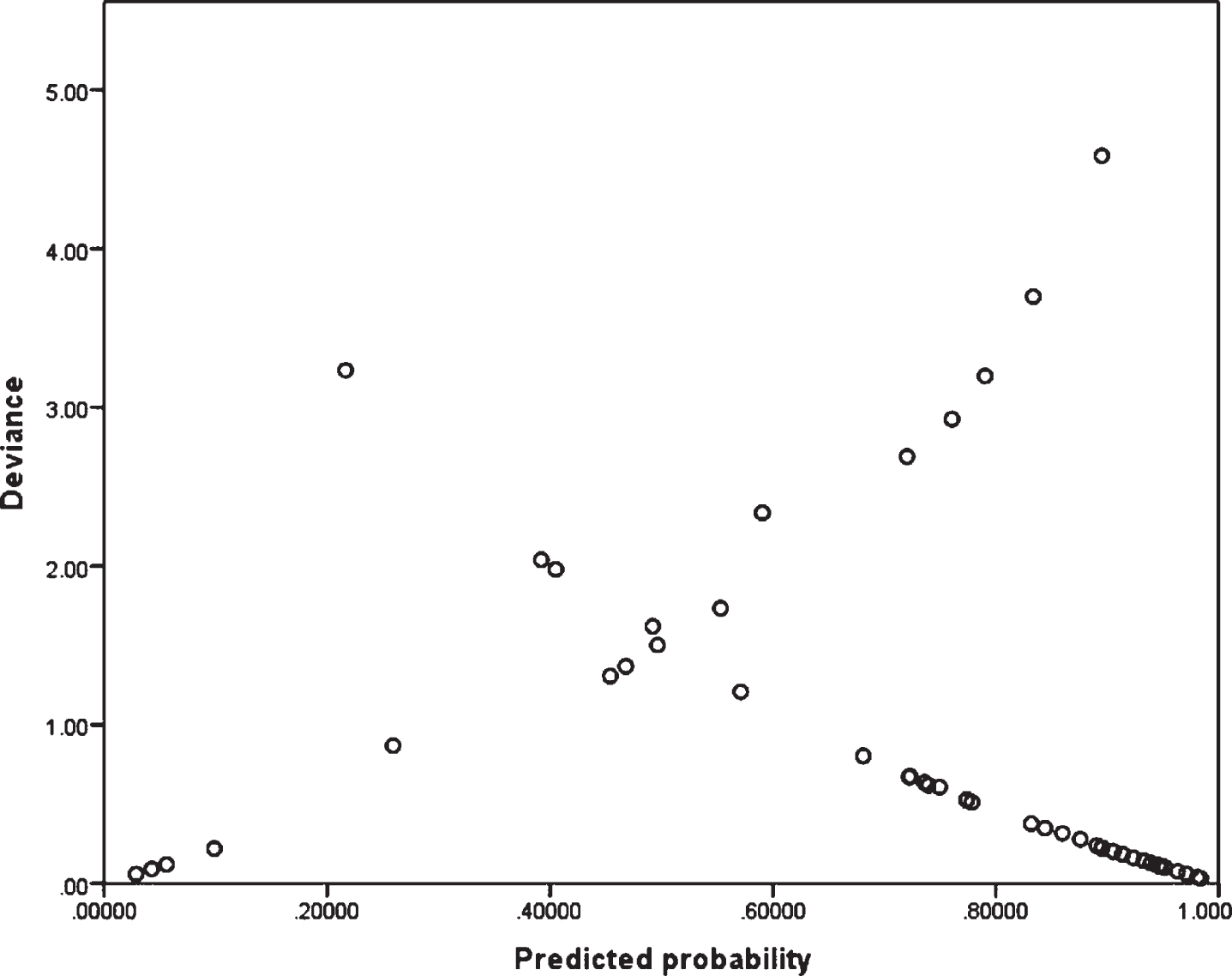
Change in deviance versus predicted probabilities.
The present study used forward logistic regression to validate a predictive model involving 42 participants. This validation (Fig. 6) revealed that the model was 92.86% accurate in predicting whether a caregiver would develop MSD. There are three cases where the model made inaccurate predictions, mispredicting two cases of MSD when the caregiver does not have MSD, and unable to predict the MSD of the caregiver who has one. In addition, the model also found that the equipment handling variables excluded from the final model were not statistically significant, confirming that the presence of the equipment did not help the caregiver by reducing the risk of MSD.
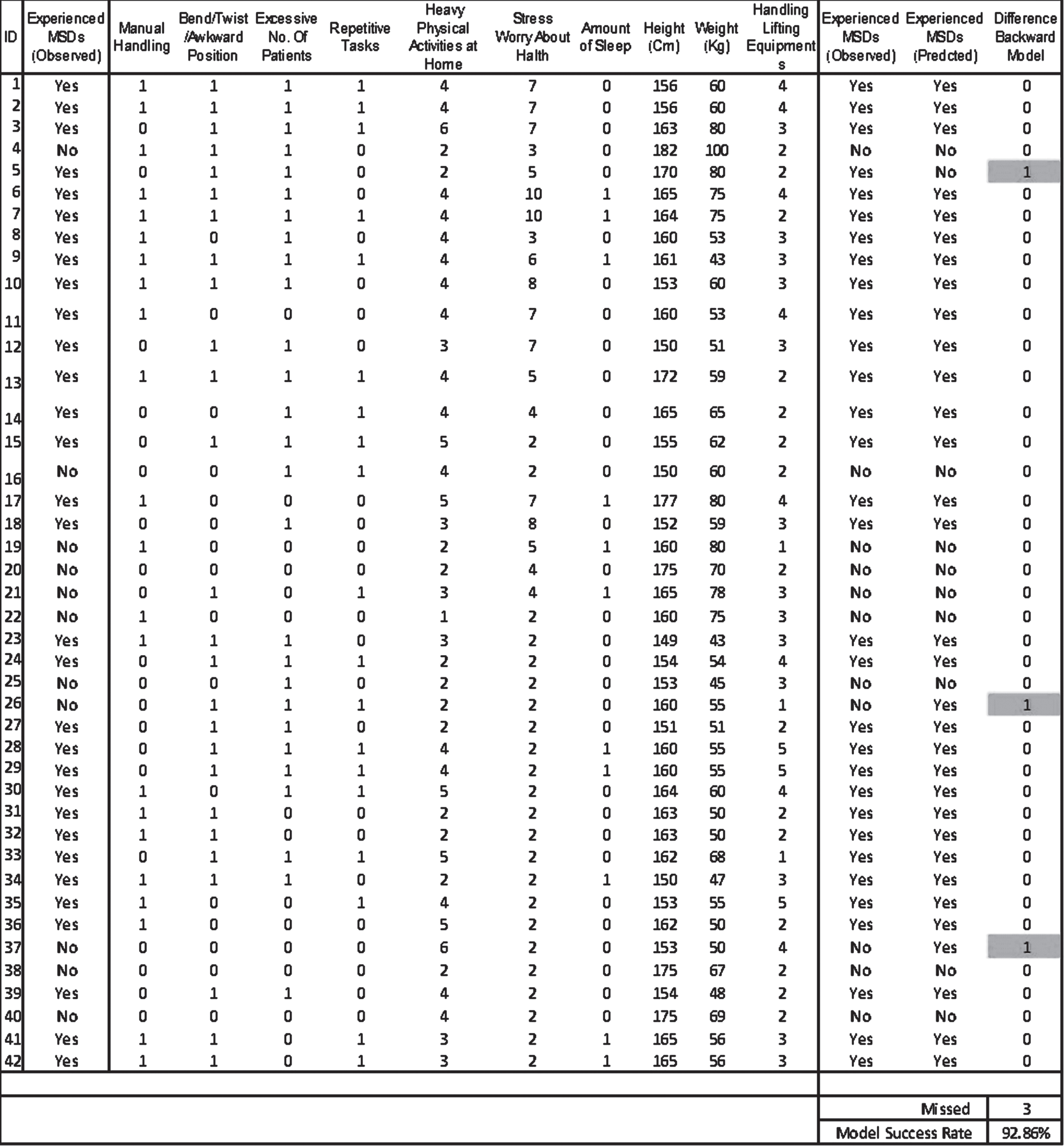
Model validation using forward logistic regression.
In this cross-sectional survey of 104 caregivers, the results showed that 70 (67.3%) participants reported MSDs while 34 (32.7%) participants did not report MSDs (20 women and 14 men had no MSD, while 58 (55.8%) women and 12 (11.54%) men reported MSD). The data on the prevalence of MSDs reported in the present study were higher than those reported in France (10% to 50%) [13], USA (35.1% to 47%) [17] and Brazil (32.8% to 57.1%) [12]; while lower than those reported in Portugal (89%) [11], China (78.6%) [15] and Iran (88%) [16]. There were perhaps three reasons for these conflicting results: first, it depends on nursing working conditions and the characteristics of each country and region; secondly, due to the amount of symptoms of MSD appearing in questionnaire; and the thirdly may be due to the size of the sample used in the survey. The current study involved all probable related symptoms and used the Nordic Standardized Musculoskeletal Questionnaire (SNQ), which was comprised in other studies [20, 21].
The present study showed that the lower back (46%) was the most commonly affected area. In Pakistan, 49.7% of nurses reported lower back MSDs [25]; another study in Iran [26] and Hong Kong [27] reported that nursing staff had lower back MSDs of 40% and 42% respectively. A study in Nigeria (Africa) reported a prevalence of MSDs in lower back (44.1%) [28]. Most studies have shown that the lower back is the most commonly affected area, but this prevalence remains modest when related to other studies: Japan (71.3%) [9], Iran (65.3%) [29], China (64.83%) [15], Portugal (63.1%) [30] and Slovenia (85.9%) [31].
Many studies have shown that shoulder, neck, and lower back MSDs is a common health problem for nurses [1, 33]. Lin et al. [34] reported that the right shoulder (85.8%), left shoulder (80.9%), neck (62.4%) and the lower back (60.4%) are the locations of the body where the prevalence of MSDs was most often experienced in participants. However, in the present study the locations of the body where the prevalence of MSDs was most often experienced in participants were highest at the lower back (46%), then knee (15.4%) and shoulder (11.5%), neck (7.7%), wrist / hand (7.7%), hips / thighs (5.8%), upper back (3.8%) and elbow / forearm (1.9%). Similarly, Kalkim et al. [33] also reported lower back (78.5%) with the highest prevalence rates of MSDs followed by upper back (74.9%), then knee joint (63.1%), neck (61.2%), and shoulder (59.6%) during a survey of 498 nurses. In contrast, Lee et al. [35] reported self-perceived musculoskeletal discomfort in the shoulder in 303 participants (78.9%), neck in 268 participants (70%) and lower back or waist discomfort in 240 participants (62.7%) based on a survey of 386 workers. Hsieh and Hsu [36] found that 41.31%, 32.25% and 31.03% of the participants felt musculoskeletal discomfort in the shoulders, neck, and lower back or at the waist respectively.
In present study, the lower back, shoulder, neck and wrist were the places on the body where the greatest amount of respondents sensed musculoskeletal disorders. In addition, the causal analysis indicated that the number of transfers or lifts of patients per shift, manual lifting of patients and the occurrence of extreme mental pressure during working hours have become more common. Other risk factors include mechanical overload, exposure time, repetitive activities, and postural demands. However, there is presently no suitable method of personal protection for the shoulder and neck musculoskeletal discomfort for the nurses. Only certain nursing station or work platforms have employed ergonomically developments to correct prolonged poor working posture. Such measures can reduce the prevalence of musculoskeletal discomfort in the shoulders and neck of nurses.
In addition, the present results showed that most important risk factors, depending on the size of their effect, were manual handling (45.64), bending (39.4), excessive number of patients (18.05), repetitive tasks (12.58), strenuous physical activity at home (3.69), emotional stress (2.6), weight (1.2), height (0.79) and sleep (0.064). Interestingly, some studies have published results similar to the present study. Cheng et al. [20] found that when MSD occurred as a result of nurses turning or transporting patients, the prevalence was highest in the lower back (77.2%) and neck (64.2%) and shoulders (58.7%). Chen et al. [21] reported that nurses who moved or transferred patients were absorbed to have the highest prevalence in the neck (63.5%), followed by shoulders (962.6%) and hips (59.3%). However, Kjellberg et al. [37] concluded that lower back MSDs in nurses are related with the professional job of supporting patients during the transfers. Thus, it was obvious that poor working practices affected MSDs, as also reported in the present study, that manual handling had the highest odds ratio, (p < 0.001 and odds ratio = 45.64) more likely to influence MSDs followed by bending (p = 0.008 and odds ratio = 39.4).
Another findings of the present study suggest that the locations of MSD was closely related to age. Age was one of the most important predictor of lower back, shoulder, and neck MSD, with caregivers aged 20 to 30 years or younger at a higher risk than those over 30 years. Similarly, Yang et al. [38] found that younger nursing staff were at greater risk. The reason may be that the nursing skills of young staff are not sophisticated, care is not accurate, and there is a high risk of lumbar musculoskeletal discomfort. Tinubu et al. [28] reported having nurses with more than 20 years of clinical work experience were more uncomfortable with work-related MSDs than nurses with 11–20 years of work experience. In addition, present results showed that thirty-six participants experienced their first MSD after 5 to 15 years of graduation, and 24 caregivers experienced it after 5 years of graduation. One study showed that underweight was strongly associated with MSD [39]. This finding may indicate that lack of weight is associated with lack of physical fitness. Vietnam’s Vietiep Hospital (Haiphong) showed several factors related to MSD, such as gender, stress and age [40]. Similarly, the present study also showed that the weight (p = 0. 040 and odds ratio = 1.20) significantly affect the rate of development of MSDs.
Absence of the workplace was also a factor related to MSD [41]. Current results show that this absence is one of the possible risks of work-related MSD. However, it was the limit of this study because it did not take into account the effects of workplace absenteeism and other consequences. The European Agency for Safety and Health at Work reported in a 2010 that “due to the prevalence of MSDs in members of the European Union, absences are often long” [42]. Further research is needed to reach this conclusion.
In addition, the injury prevention and physical health risk factors were found to be related to the development of MSDs. Caregivers who reported physical discomfort were more probable to have MSD, and caregivers who stated satisfaction with their physical fitness were related with a lower incidence of MSD. In addition, long-term fixed positions, whether sitting or standing, increased the chances of developing MSD, as well as fatigue. Conversely, caregivers who stated being healthy and happy with their overall health were found to be less likely to get an MSD. These findings show that self-confidence in physical health is significant for caregivers in dropping the risk of MSD, long hours of work and fatigue are detrimental to their health. This indicate the immediate importance of training and education in ergonomic and biomechanical principles in patient handling to prevent WMSDs among caregivers at hospitals [43].
Recommendation and guideline for policy makers
Policy makers may need to limit the number of hours a caregiver works per week. This attempts to limit the prevalence of caregivers to MSD. In addition, policy makers may highlight a break while lifting the task and a stop when the caregiver begins to feel pain while performing the task. Other policy improvements may attempt to completely redesign the lifting operation to escape movements recognized as high risk factors. Policies are needed aimed at raising awareness of workstation injuries, their significances, and preventative methods considered to minimize injuries. Essential training in work-related accident, prevention policies and ergonomics will also assist caregivers. This study contributes in the field of human factors and ergonomic risk management by suggesting a framework for identifying factors related to MSDs and creating predictive models. Practitioners can use these results to help caregivers change their working conditions and implement preventive policies.
Limitations and future research
This study had some limitations. First, it is not normal practice for the hospitals to keep records of caregiver injuries and claims. Therefore, it was essential to obtain this information from a caregiver limited to 104 participants. As a result, further analysis can be performed within a healthcare facility that has a more consistent history of caregiver injuries, providing broader research opportunities. With regard to demographic restrictions, more accurate and relevant results may be obtained as the population composition of the sample population increases and the gender-age balance improves. The data on the development of MSDs are based on the self-reported data provided by the participants and have not been tested physiologically to approve the diagnosis. Therefore, the reported prevalence of MSD may be overestimated. Finally, future studies can reproduce this study using alternative tools for logistic regression. Artificial neural networks (ANN) may provide different results have the potential to understand the association between risk factors and MSD.
Conclusions
The results of this study reaffirmed the high prevalence of work-related MSD among Saudi Arabia caregiver’s primarily in the lower back, and the frequency of symptoms was consistent with that reported by other studies. The most important risk factors were manual handling, followed by bending / twisting, and handling of an excessive number of patients. Therefore, preventive strategies for these conditions require a multifaceted approach that incorporates psychosocial, workplace, and ergonomic considerations. In addition, it is necessary to consider appropriate policies for managing MSDs among caregivers.
Conflicts of interest
The authors declare that they have no conflicts of interest.
Funding
The authors state that they have not received funding for this project.
Footnotes
Acknowledgments
The authors would like to thank the staff and managers of hospitals in Saudi Arabia for making it possible to obtain data from caregivers / nursing staff. In addition, the authors are grateful to the Ministry of Health, Saudi Arabia, for approving the research protocol.