
Abstract
BACKGROUND:
Although studies have indicated significant effects of attention-deficit hyperactive disorder (ADHD) on work participation, the mechanism underlying work participation of adults with ADHD is still unclear.
OBJECTIVE:
Following the World Health Organization’s international classification of functioning, disability, and health concepts, this study compares sensory processing and sleep quality (body functions) with work participation among adults with and without ADHD and examines predictive relationships among adults with ADHD.
METHODS:
Sixty-nine adults with ADHD and 52 matched controls completed a sociodemographic questionnaire, the Adult/Adolescent Sensory Profile, the Mini Sleep Questionnaire, and the Occupational Questionnaire.
RESULTS:
The ADHD group had significantly poorer body functions, sensory processing (i.e., low registration, sensory-sensitivity, and sensation-avoiding patterns), sleep quality, and work performance compared to the control group (p < .001). For adults with ADHD, sensory sensitivity accounted for 10.9%, and sleep quality accounted for 22.0%, of the variance in their work performance.
CONCLUSIONS:
The deficient body functions of adults with ADHD may affect their work performance and therefore should be considered in further research, as well as in clinical applications.
Keywords
Introduction
Attention-deficit hyperactivity disorder (ADHD) is a neurodevelopmental condition defined by patterns of persistent age-inappropriate inattention, hyperactivity, and impulsivity that affect individuals across the life cycle. Although ADHD begins in in childhood, according to the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) definition [1] and other evidence, it does not disappear in adulthood. The prevalence of ADHD among adults ranges from 2.5% to 5.0% [e.g., 2].
Our study is based on the World Health Organization’s [3] international classification of functioning, disability, and health (ICF) model to further understand body functions that may influence work participation of adults with ADHD. Accordingly, ADHD is considered a health condition (disease, disorder, or injury), whereas sensory processing and sleep quality are body functions (physiological and psychological functions of body systems), and work is a major life area (domain). Figure 1 depicts the interplay among these elements.
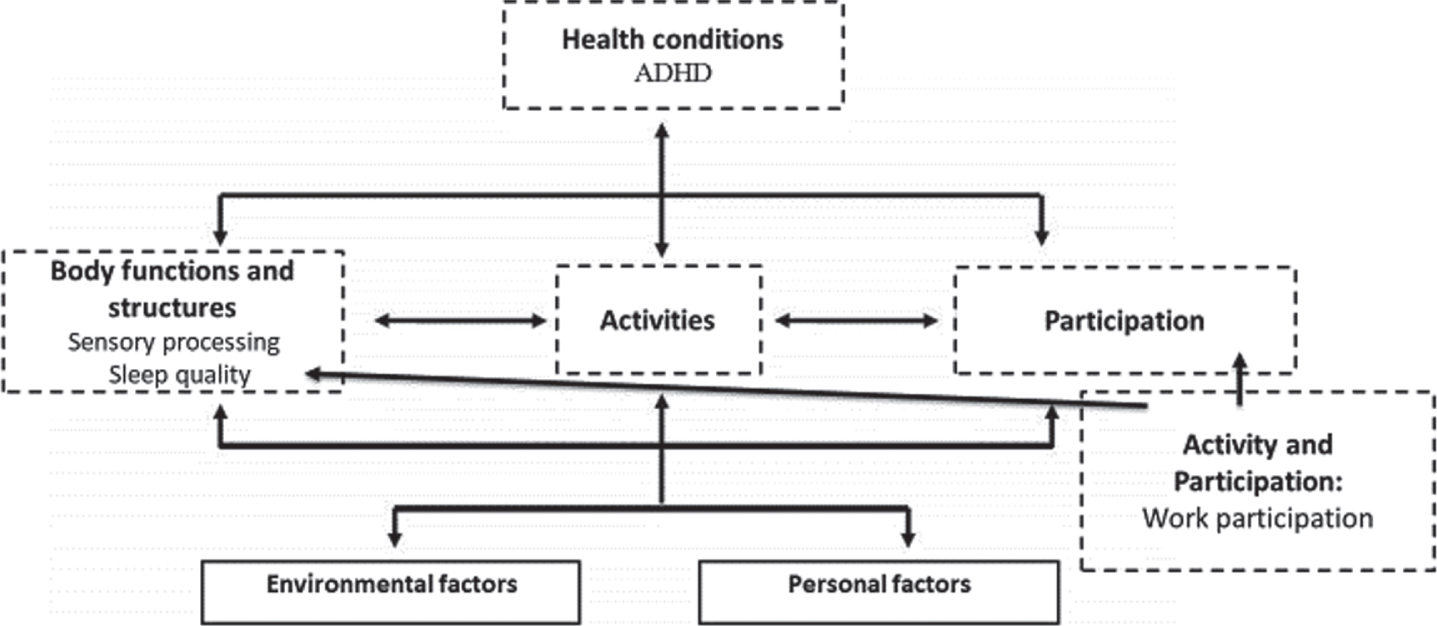
Components of the international classification of functioning, disability, and health model (WHO, 2001) with constructs examined in this study.
Work creates a framework for individuals’ daily routine and is essential for their independence and social belonging. Because it contributes to self-esteem and shapes identity by defining a meaningful role, work supports health and promotes subjective well-being and life satisfaction (e.g., [4, 5]). Unsurprisingly, students with ADHD stated that work makes them feel worthy and valuable [6]. However, studies also associated ADHD with reduced work-task performance and productivity and with tendencies toward unemployment, job-switching, terminations, work accidents, and sickness absences (e.g., [7–9]). For instance, ADHD is prevalent in 3.5% to 4.2% of working adults in various countries, and workers with ADHD experience employment dysfunction between 22.1 days and 35.0 days annually (e.g., [10]. In the United States, this equates to as much as 120 million days of annual lost work, or $19.5 billion lost human capital [10, 11]. Although the extant literature documented reduced work participation by adults with ADHD, limited studies have investigated underlying factors that may be associated with this population’s work participation difficulties.
Body functions, such as sensory processing and sleep quality, may contribute to the poor work participation of adults with ADHD. The hybrid neuropsychological model suggests ADHD is a deficit in executive functions—the ability to self-regulate across time to attain goals, typically in a social context [12–13]. The self-regulation deficit that characterizes ADHD according to this model can help in understanding individuals’ difficulties with processing sensory input and attending to and maintaining sleep.
Sensory processing and sleep quality may be part of the underlying mechanism that restricts ADHD work participation. Sensory processing, as an ICF body function [3], refers to ways individuals manage incoming sensory information, including reception, modulation, integration, and organization of sensory input [14]. Dunn’s theoretical model presents the relationship between a neurological threshold continuum and a behavioral response–regulation continuum. Dunn described four sensory processing patterns based on those relationships: low registration, sensation seeking, sensitivity to stimuli, and sensation-avoiding. Some people exhibit extreme sensory patterns [15], which are common among children with ADHD, as reflected in their limited participation in daily living, academic, play, and leisure activities (e.g., [16]). Studies among adults also found associations of ADHD and learning disabilities with inferior sensory processing (e.g., [17, 18]). However, despite the extensive research with children, few studies examined the relationships between specific sensory processing deficits and participation of adults with ADHD as a whole [19] or work participation specifically. One study related to sensory processing and work participation noted that women with ADHD reported that sensory sensitivity to stimulation at the workplace affected their work performance [20].
This study addresses sleep quality as an ICF body function that may be associated with work-participation difficulties of adults with ADHD [3]. Poor sleep refers mainly to insomnia, a dissatisfaction with sleep quantity or quality that causes clinically significant distress or impairment. Poor sleep appears in 23.2% of U.S. working adults [1, 21], and studies have indicated that 43% to 80% of adults with ADHD have more sleep-disorder symptoms and more frequently than does the general population (e.g., [22]). Further, the literature highlighted significant associations of insomnia or other sleeping problems with work participation, manifested in reduced work performance, productivity and capacity, greater absenteeism (missed workdays), and presenteeism (low performance at work) (e.g., [23, 24]).
Despite the possible empirical and clinical applications of sensory processing and sleep quality as body functions, limited studies have investigated them as factors that may influence work participation of adults with ADHD. Thus, the aims of this study were to: (a) describe sensory processing challenges, sleep quality, and work participation of adults with ADHD (research group) compared to those of controls without ADHD and (b) analyze predictive relationships between those body functions and work participation in the research group.
Procedure
This research was designed as a quasi-experimental case-control study. The Ethics Committee of University of Haifa provided ethical approval (Confirmation No. 032/17). Data were collected between March 2017 and April 2018. We recruited a convenience community sample of 121 adults in Israel, inviting people with and without ADHD via e-mail or social networks to participate. Those who contacted the researcher to be in the research group were asked to provide proof of a formal medical ADHD diagnosis by an expert neurologist, psychiatrist, or family doctor based on the DSM-5 criteria, at any point in their lives. After signing informed consent, all participants completed the following measures to confirm the inclusion criteria: Adult ADHD Self-Report Scale (ASRS) version 1.1 [11], Brown Attention-Deficit Disorder Scales (BADDS) [25], and Behavior Rating Inventory of Executive Function-adult version (BRIEF-A) [26]. Following, they received a website link to the demographic questionnaire, Adolescent/Adult Sensory Profile (AASP) [27], Mini Sleep Questionnaire (MSQ) [28], and Occupational Questionnaire (OQ) [28]. Although participants submitted the questionnaires anonymously and independently, the main researcher was available by telephone for assistance and support. All participants received a voucher reward for their time and effort.
Participants
A sample size of 113 participants was calculated using the guidelines of G*Power software, considering the medium effect size of f2(V) = 0.0625, significance of α= 0.5, and power of 0.80 [30]. Inclusion criteria for all participants were (a) aged 20 to 46 years, (b) worked at least 3 months at the same worksite, and (c) read and wrote Hebrew fluently. Additional inclusion criterion specific to the research group was the formal medical diagnosis of ADHD, supported by their ASRS version 1.1 screening [11] and BADDS scores [25]. Considering the central role of executive functions deficits in adult ADHD [31, 32], all research group participants had at least one executive function deficit according to the BRIEF-A [26]. It is important to note that participants who self-reported comorbid mental health disorders were included in the research group because we wanted the sample to reflect the high incidence of comorbidities that characterizes the population of adults with ADHD. That is, about 75% of this population deals with at least one additional psychiatric diagnosis (e.g., [33]). Control group members were without both ADHD (per the ASRS final score or low probability per the BADDS) and a learning disability diagnosis (per self-reports). Further, they had no executive function deficits (per the BRIEF-A) or additional psychiatric diagnoses (per self-reports) that might affect their participation or performance. People with motor or neurological disabilities, chronic diseases, or significant injuries that could affect participation and performance were excluded from study sample.
The final sample included 121 adults who match inclusion and exclusion criteria: 69 with ADHD (research group) and 52 without (control group). The two groups were matched for gender, age, education level, and socioeconomic status (α> 0.05).
Measures
Inclusion criteria measures
The following instruments were used to create the sample according to the inclusion and exclusion criteria:
2.3.1.1ASRS
The ASRS [11] version 1.1 is a standardized, well-validated, and reliable self-report screening scale for adult ADHD (e.g., [34, 35]). We implemented the validated Hebrew version in our study [36].
2.3.1.2BADDS
The BADDS [25] is a standardized, well-validated, and reliable self-report scale for adults that measures a range of symptoms beyond ADHD inattention criteria. Thus, it can be used also as a screening tool for adult ADHD (e.g., [25, 37]). We used the validated Hebrew version in our study [25].
2.3.1.3BRIEF-A
The BRIEF-A [26] is a standardized, well-validated, reliable, and ecological self-report. It captures adults’ views of their own executive functions in their everyday environments (e.g., [26, 38]). The validated Hebrew version was implemented in our study [39, 40].
2.3.1.4Sociodemographic questionnaire
The self-report questionnaire designed specifically for this study includes 13 questions related to participants’ sociodemographic status, five questions related to their diagnoses, and nine related to their current employment status.
Work participation, sensory processing, and sleep quality evaluations
The following instruments were used to evaluate the study variables:
2.3.2.1OQ
The self-report OQ [29] was developed to measure volition subsystems and everyday occupational-activity patterns. Participants indicate their main activity during each waking half hour on a typical day; classify each activity as one of five occupational domains (including work); and, on a 5-point Likert scale, rate the degree of personal performance, importance, and enjoyment for each activity. Summarized by percentages, results indicate participants’ percent of time engaged in each occupational domain, perceptions of their performance, and importance and enjoyment of the activity. Higher scores indicate lower performance, importance, or enjoyment of the scored activity. In this study, we calculated only scores regarding activities in the work domain (work performance, work importance, and work enjoyment). The Hebrew version has been validated [41].
2.3.2.2AASP
A self-report questionnaire, the AASP aims to examine participants’ sensory processing [27]. Participants indicate how often they respond to the sensory event in the manner described using a 5-point Likert scale. To score, the 60 items are sorted into four quadrants reflecting sensory-processing patterns of low registration, sensation seeking, sensory sensitivity, and sensation-avoiding [42]. Cut-off scores indicate when the respondent’s scores significantly differ from peer responses. Each age group has its own norms: much less/much more than most people (4% of the population), less/more than most (28%), and similar to most (68%) [27]. The questionnaire has good internal consistency content validity and moderate convergent validity (e.g., [43, 44]). The standardized Hebrew version was reported to have good internal consistency, psychometric properties, and discriminant validity between adults with and without learning disabilities (e.g., [18, 42]).
2.3.2.3MSQ
The self-report MSQ [28] assesses respondents’ sleep quality and risk for insomnia. Using a 7-point Likert scale, respondents indicate how often they face different sleep difficulties. Two scores are calculated: (a) a mean of the 10 items for a final score of sleep quality and (b) an insomnia score calculated by summing items 1, 2, and 7. The questionnaire has good internal consistency and acceptable reliability and concurrent and predictive validity [45–47]. The Hebrew version was reported to have discriminant validity between adults with and without posttraumatic stress disorder and learning disabilities and to be sensitive to change in sleep quality following intervention among women who suffer from headaches [18, 49].
Statistical analysis
Descriptive statistics were calculated to describe the sample, and the two groups’ demographic variables were compared using chi-square tests. Independent t-tests and multiple analyses of variance (MANOVA) were applied to analyze differences in dependent variables between the groups. Subsequent univariate analyses of variance (ANOVA) were applied to find the source of significance across the scale components. We applied regression predictive models to examine the predictive relationships among the variables.
Results
Sociodemographic characteristics
As presented in Table 1, the majorities in both the research and control groups were women (65.2% and 69.2%, respectively). Ages ranged from 21 to 46 years. No significant group differences were found regarding age, gender, socioeconomics, familial status, or education level. Participants in both groups had similar occupational characteristics, such as employment type, working environment, occupational seniority, and percentage of weekly work hours. However, significant group differences were found regarding the number of places worked since age 20 years: Research group participants had almost six workplace transitions during their adult work life, whereas control group participants averaged only 3.81 workplaces, t(119) = 2.67, p = 0.008. Among the research group participants, the most common mental health disorders (together, 3.3% of the sample) were posttraumatic stress disorder (n = 2) and depression (n = 2).
Demographic and occupational characteristics of the group of adults with ADHD and the group of adults without ADHD
Demographic and occupational characteristics of the group of adults with ADHD and the group of adults without ADHD
Note. aSocioeconomic status is based on self-reported income levels. **p < 0.01
The MANOVA across the OQ productive work variables (work participation) yielded statistically significant group differences, F(3, 78) = 9.35, p < 0.001, η2 = 0.26. Further, as presented in Table 2, the subsequent univariate ANOVA revealed that research group participants had significant differences between the mean scores for two of the three work variables (work performance and importance). That is, compared to the control group, the research group rated their work performance as lower and their work as less important.
Means and standard deviations of work participation variables per the Occupational Questionnaire (OQ)
Means and standard deviations of work participation variables per the Occupational Questionnaire (OQ)
Note. Not all participants in each group answered all the questions. *p < 0.05; ***p < 0.001.
The MANOVA indicated significant group differences for the AASP scales, F(4, 113) = 43.80, p < 0.001, η2 = 0.61. The subsequent univariate ANOVA revealed that research group participants had significantly higher mean scores in all AASP quadrants (p < 0.001) except sensory seeking (Table 3). Additional analyses reflected that more than half of the research group members struggled with limited sensory processing (above norm) in the low registration (68.1%), sensory sensitivity (62.3%), and sensation-avoiding (52.2%) quadrants. Only a few participants (10.1%) were above norm in the sensory-seeking quadrant.
Means and standard deviations of Adult/Adolescent Sensory Profile (AASP) quadrant scores
Note. ***p < 0.001.
Significant group differences were found for the MSQ scale, t(119) = 7.93, p < 0.00, and risk for insomnia, t(119) = 7.93, p < 0.00. Participants in the research group had lower quality sleep and higher risk for insomnia compared to those in the control group (Table 4).
Means and standard deviations of sleep quality and insomnia scores per the Mini Sleep Questionnaire (MSQ)
Note. ***p < 0.001.
Regression analyses revealed that the AASP sensory sensitivity quadrant and MSQ sleep quality scores significantly predicted variance in work performance (per OQ) among the research group. Sensory sensitivity accounted for 10.9% of the variance, F(1, 43) = 7.02, p < 0.01, and sleep quality accounted for 22% of the variance, F(1, 44) = 12.42, p < 0.001 (Table 5). Together, these two variables predicted 32.9% of the variance of work performance.
Prediction of Occupational Questionnaire (OQ) work performance by Adult/Adolescent Sensory Profile (AASP) quadrant and Mini Sleep Questionnaire (MSQ) scale scores: Research group (adults with ADHD)
Prediction of Occupational Questionnaire (OQ) work performance by Adult/Adolescent Sensory Profile (AASP) quadrant and Mini Sleep Questionnaire (MSQ) scale scores: Research group (adults with ADHD)
Note. **p < 0.01; ***p < 0.001.
This study describes work participation, sensory processing, and sleep quality (body functions) of adults with ADHD compared to controls. It also reports the analysis of the predictive relationships between these body functions and work participation of adults with ADHD. The innovation of this study is demonstrated in the identification of body functions that contribute to poor work performance (work participation variable) of adults with ADHD.
While interpreting the results, it is important to note that research group included additional diagnoses because comorbid neurodevelopmental diagnoses are common among this population, but those diagnoses may have influenced the results. Although most demographic and occupational characteristics of adults with and without ADHD did not differ in this study, the group with ADHD had significantly more workplace transitions since the age of 20 years. This difference contributes to evidence of tendencies that adults with ADHD present (remaining unemployed, switching jobs, or being terminated; e.g., [50, 51]).
Differences between adults with and without ADHD were found in work participation and body-function levels; adults with ADHD rated their work performance and importance lower than did the controls. These results fit well with previous findings on work performance difficulties among adults with ADHD and self-reports in particular (e.g., [8]). Moreover, they correspond with evidence about restrictions on activity and participation of individuals with ADHD, such as difficulty undertaking multiple tasks, managing time, and planning activities (e.g., [17, 52]). Because these skills are needed to perform well at work, restrictions on them can explain the low performance found in this study. Despite the work performance difficulties the adults with ADHD reported, no significant differences were found between the research and control groups regarding work enjoyment. This demonstrates the need for continued comprehensive perception and evaluation of work-related aspects (e.g., enjoyment and importance) in further investigations with targeted and accurate evaluation tools.
The adults with ADHD had significantly more sensory processing difficulties in the AASP low registration, sensory sensitivity, and sensory-avoiding quadrant patterns than had adults without ADHD. These findings expand the limited literature on relationships between sensory processing deficiencies and ADHD among adults. They also reinforce studies that identified those three quadrants as lacking among adults with learning disabilities [17, 18]. Like previous studies with children with ADHD (e.g., [53]), this study highlights the importance of distinguishing the behaviors that are considered derivatives of sensory processing deficits from the behaviors that are simply consistent with general ADHD diagnostic criteria. Such distinction will enable a more comprehensive understanding of the participation challenges that characterize the adults-with-ADHD population. The results also indicate that these adults tend to have lower quality sleep and higher risk for insomnia than do the controls, which aligns with prior reports on the relationships between sleep quality deficiencies among adults with ADHD [22, 54].
In addition to significant differences at the work-participation and body function levels (i.e., sensory and sleep), this study identifies the body functions as predicting 32.9% of work performance variance among adults with ADHD. Sensory sensitivity was responsible for 10.9%, reinforcing evidence regarding sensory processing’s broad influence on every aspect of daily life [55]. As such, the findings identify sensory sensitivity as a specific pattern that affects work performance. Sensory sensitivity relates to impulsive errors, inattention, and poor organization in time abilities among adults with and without ADHD and learning disabilities [19, 56]. Such capabilities are needed to perform well at work (e.g., [17]); thus, their associations may explain the connection between sensory sensitivity and work participation we found. According to Dunn’s [27] theoretical model of sensory processing, people with sensory sensitivity notice more sensory stimuli than do others. Thus, they are easily distracted, and others may perceive them as overly precise or picky. Distractions of movement, sound, or smell may occur while in a group [16, 55], such as during work meetings, or in open-work locations. The tendency to be precise or picky can reflect negatively in their interpersonal relationships with coworkers and work supervisors. Evers et al. [57] suggested that people with sensory sensitivity experience their work environments as chaotic—a bombardment of strong, senseless stimuli that causes work to be incomprehensible and unmanageable. Schreuer and Dorot [20] supported that statement in a report on women with ADHD who described manifestations of their sensory sensitivity at work.
Our study found sleep quality to be responsible for 22% of work performance variance, contributing to the wide acknowledgment that sleep is essential to performing daily activities and occupations (e.g., [23]), and presence of sleeping problems seems to further increase the functional disability in ADHD population (e.g., [58, 59]). The extant evidence that sleep enhances memory and cognitive functioning, regulates learning, and is important to emotion regulation can explain the results (e.g., [60]). Because effective performance at work requires those abilities (e.g., [52]), the negative influence of low sleep quality appears to be an obvious and expected consequence. Dan et al. [61] found that compared to controls, adults with ADHD who experienced sleep deprivation made more errors during task performance. Perhaps adults with ADHD, who already struggle with work performance and participation limitations from their ADHD symptoms and executive function deficits (e.g., [52, 62]), are more vulnerable to the negative influences of low sleep quality. Accordingly, adults with ADHD reported fatigue and were found to be sleepier during cognitive tasks than were controls, which affected their occupational and cognitive performance [6, 63]. Helfer et al. [63] suggested the cognitive performance deficits routinely attributed to ADHD are largely due to on-task sleepiness and not exclusively to ADHD symptom severity.
Our study reinforces that assumption and adds to the scarce existing literature regarding the effects of each body function to the reduced work participation of adults with ADHD. The results support existing literature that demonstrated the importance of a holistic assessment of people with ADHD, focusing not only on symptomatology, but also on sleep problems and functional outcomes [64]. However, further investigation is required to fully understand the ramifications and influences body functions have on work participation. Furthermore, this study’s results were obtained through participants’ subjective self-reports. We recommend combining additional objective performance-based measures for more comprehensive understanding regarding the relationship of the body functions identified in this study with work participation domains (e.g., work enjoyment and importance).
Conclusions
This ICF-based study sheds light on the mechanisms underlying poor work performance of adults with ADHD, recognizing specific sensory sensitivity patterns and sleep quality impairments that predict work performance. The findings highlight the importance of a comprehensive analysis of individuals with ADHD—one that considers not only ADHD symptoms, but also body function features—to understanding more of this population’s unique challenges. Such understanding may help clinicians implement more accurate evaluations and support adults with ADHD in personally adapted interventions to improve work participation and well-being.
Footnotes
Acknowledgments
We thank all those who participated for their cooperation and interest in the study. We also thank the National Insurance Institute of Israel for their support.
Conflict of interest
We have no known conflict of interest to disclose.