
Abstract
BACKGROUND:
The Bioservo Ironhand® is a commercially available active hand exoskeleton for reducing grip-induced stress.
OBJECTIVES:
The study aimed at quantifying the effect of the Ironhand® exoskeleton on the myoelectric muscle activity of forearm flexor and extensor muscles in three relevant assembly grip tasks: 2-Finger-grip (2Finger), 5-Finger-grip (5Finger) and Full grip (FullGrip).
METHODS:
Twenty-two subjects were tested in three different exoskeleton conditions for each grip task (overall 3×3×10 = 90 repetitions in randomized order): Exoskeleton off (Off), Exoskeleton on, “locking tendency” 0% (On_LT0), and Exoskeleton on, “locking tendency” 85% (On_LT85). Muscle activity was measured at 25% of the participant’s maximum grip force using two EMG sensors at the M. flexor digitorum superficialis (M.FDS) and one at the M. extensor digitorum (M.ED).
RESULTS:
The effect of the Ironhand® exoskeleton varied depending on the grip task and the participant’s sex. A statistically significant reduction in muscle activity of the M.FDS was found only for male subjects in the FullGrip condition. No reduction of muscular activity in the M.FDS was found for the other grip tasks (2Finger, 5Finger). For the females in the 2Finger condition, mean muscle activity of M.FDS even increased significantly in On_LT0 compared to Off. Besides differences between grip tasks and sex, the current study revealed substantial individual differences.
CONCLUSIONS:
In addition to testing for statistical significance, a detailed exploratory analysis of exoskeleton effects at subject level should be performed to evaluate these from a safety and regulatory perspective.
Introduction
Exoskeletons have been attracting interest from industry for several years as a method of reducing physical stress at specific assembly workplaces for which conventional workplace design techniques and technologies e. g. technical aids, tools or organizational measures [1, 2] have been exhausted. In the context of physical work, the term exoskeleton refers to a body-worn support system that acts mechanically on the user’s body to reduce work-related stress [3]. However, there is neither a uniform definition of the term “exoskeleton” nor a uniform categorization for exoskeletons. For instance, exoskeletons can be classified according to the body region to be supported (legs, trunk, shoulder area, whole body), or according to the corresponding application area (industry, military, rehabilitation). Hard exoskeletons use rigid structures made of carbon or aluminum to transmit forces. Soft exoskeletons transfer forces using textile elements [4, 5]. Furthermore, a distinction is made between active and passive exoskeletons depending on the type of support. Active exoskeletons are usually powered electrically or pneumatically, while passive exoskeletons do not have a power source. Instead, they use the wearer’s movements to preload a spring mechanism, for example, which subsequently supports another movement.
The current state of scientific knowledge about the effectiveness of exoskeletons is contradictory. Some scientific studies have found a reduction in physical strain when exoskeletons are used for indu-strial activities [6–9]. Other studies report unexpected and potentially undesirable effects such as increased activity of other muscles, increased energy expenditure, restricted movement, altered movement patterns, or discomfort from local pressure peaks [10–12] at the contact points to the human body. There are no controlled longitudinal studies showing that exoskeletons prevent work-associated musculoskeletal complaints or musculoskeletal disorders [13]. Furthermore, there is insufficient evidence about the acute beneficial effects of exoskeletons in subjects with back pain, joint pain, or pain of the muscles and surrounding tissues in terms of symptom relief or preventing symptom exacerbation. Thus, based on current scientific knowledge and experience from occupational practice, no primary, secondary, or tertiary preventive effect can be substantiated [14]. Recent studies examining industrial pilot use of exoskeletons aimed at reducing stress on the shoulder during overhead work or of the lumbar spine during manual material handling (12, 13), and predominantly involve passive exoskeletons. Although diseases of the lower back and shoulder lesions are by far the most frequent causes of absenteeism from work, diseases of the finger-hand-arm system also account for a considerable proportion in total [15]. Studies in the automotive industry show an increase of discomfort in the finger-hand-arm system caused by high assembly forces, for example in clip connections and assembly tasks with short repetitive cycles and a high workload [16]. With hand exoskeletons already being used in rehabilitation [17, 18], companies are now trying to tap into their potential to support manufacturing personnel in specific industrial applications. Among commercially available hand exoskeletons [19, 20], the Ironhand® from Bioservo Technologies AB (Kista, Sweden) is the only active soft exoskeleton to support grip activities specifically in industrial settings [21]. The Ironhand® soft exoskeleton technology has shown improvement in activities of daily living and potential as a therapeutic and assistive device, at least in the rehabilitation of elderly patients with limited hand functionality [22–24]. However, the transferability of these findings to grip tasks in manual assembly is limited because of the substantially lower grip forces used in rehabilitation settings. To our knowledge, there is only one scientific study that has evaluated the effects of an active hand exoskeleton in the context of industrial physical work. Mayer et al. [25] investigated whether the Ironhand® has an effect on the muscle activity of the forearm flexors in three different assembly-relevant grip tasks (grips with extended fingers (2 and 5-fingers, Full grip). For this purpose, different support modes of the Ironhand® were tested for each grip task at 50% of the individual maximum grip force (Fmax). As a result, a reduction in muscle activity was only detected for one of the grip tasks tested (Full grip). No reduction effect was determined for the other two grip tasks. Interestingly, for up to one third of the subjects, muscle activity even increased by up to 120% compared to the reference level without Ironhand® support. However, the generalizability of the study results is limited due to the small sample size (n = 12, 3 female, 9 male subjects) and the lack of randomization of the experimental conditions. The lack of control for bias effects and confounding variables, such as fatigue effects or sex, are therefore addressed in the present study by adjusting the study design (larger sample, randomization of experimental conditions, reduced target force level, more EMG sensors).
Objective
The aim of the present study was to investigate the effects of Bioservo’s Ironhand® on the muscle activity of the forearm flexor and extensor muscles at 25% of the individual maximum grip force across three assembly-relevant grip types (in cooperation with the Audi AG, Ingolstadt, Germany). Therefore, muscle activity was analyzed while subjects wore the exoskeleton and performed the three most common grip types on automobile assembly lines [26]: 2-Finger grip (thumb / forefinger, relative frequency 9%, 2Finger) 5-Finger grip (thumb / 4-finger, relative frequency 27.4%, 5Finger) Full hand grip (relative frequency 13.5%, FullGrip)
Since the Ironhand® induced unexpected effects (increases in muscle activity) in our previous study [25], the following nondirectional hypotheses were tested:
H0: The support provided by the Ironhand® with 2 different profiles has no influence on the muscle activity of the forearm flexors or extensors.
H1: The support provided by the Ironhand® with 2 different profiles has an influence on the muscle activity of the forearm flexors and extensors.
Methods
Sample
24 subjects participated in the study, and had to be free from injury at their dominant arm for a period of at least six months prior to the study, with no restrictions for handedness. Due to technical problems during data collection (data loss during the wireless transmission of the EMG signals), 2 subjects had to be excluded from further processing, and data from 22 subjects (7 female, 15 male, mean age 31.4 yrs, SD = 8 yrs) remained for data analysis.
Functional characteristics of the Ironhand®
Figure 1 gives an overview of the components and the functionality of the Ironhand® soft exoskeleton. The system consists of a glove and a backpack with an actuator unit including a battery and a control pad. The force support is transferred separately for each finger by two artificial tendons running medio-palmar and lateral-palmar in the glove fingers to the fingertip. Tension can be applied simultaneously to the two artificial tendons of each finger via the actuator unit in the backpack. The user can adjust the support force for the individual fingers with force sensors sewn into the fingertips of the glove. The more pressure is exerted on a force sensor, the stronger the actuation on the two artificial tendons of the respective finger. In addition, users can choose between two pre-configurable user profiles on the control panel. In these user profiles, for example, the overall sensitivity of the system or a fixed ratio of the support level of the fingers relative to each other can be set [27, 28]. Thus, the user can quickly adjust the Ironhand® to various external requirements.

Schematic of the Ironhand® modified (Bioservo Technologies AB 2019): 1 = Backpack with control unit and battery, 2 = Tube attachment of artificial tendons, 3 = Elastic arm straps, 4 = Ironhand® glove, 5 = Front fastening straps, 6 = Control panel, 7 = Control panel attachment, 8 = Side tie strap, 9 = Artificial tendons (red), 10 = Force sensors in Ironhand® glove.
A maximum support level of 75% was set on the control panel (3 of 4 LEDs). Higher maximum support levels were perceived as too strong during pilot tests and were rated as unpleasant by subjects. For the present study, two different user profiles with the following identical settings were configured via the IronConnect app: Sensitivity: 5.0 (sensitivity or reactivity of the force sensors); Locking tendency fingers: 0% (static holding function; see the next paragraph for an explanation); Activation threshold: 0.3 (required force to activate the system via the force sensors in the fingers); Finger balance: F1:100%, F2-4:90%, F5 80% (support ratio of the fingers to each other; in the present study, F5 was supported 10% or 20% less than the remaining fingers and thumb).
Profiles 1 and 2 only differed in the setting “locking tendency”. In profile 1 the “locking tendency” was set to 0%, in profile 2 to 85%. The higher the “locking tendency” value, the more the force sensors in the fingertips have to be unloaded for the Ironhand® to reduce the tensile force. Thus, a static holding force can be maintained with less muscular tension. Since pre-worn Ironhand® gloves were used in this study, and their sensitivity tends to level out after a break-in period, a sensitivity setting of 5.0 had to be used to achieve comparable levels of support with regard to our previous study [25] (sensitivity level of 2.6 with new sensors). Work gloves were worn over the the Ironhand® during testing, as recommended by the manufacturer (Towa ActivGrip XA-325).
Measurement instrumentation
To control and measure grip strength, a hand dynamometer (Deyard EH101) was modified and statically calibrated so that it could be operated on a data logger (Biometrics DataLOG MWX8). After calibration using dead weights, the maximum deviation of the measured force was 0.00022% of the nominal force (409 N). To ensure the best possible activation of the force sensors in the fingers (fingertips), 2 different handles were 3D-printed (flat contact surfaces for 2-fingers and 5-finger grip, enlarged round finger contact surface for the FullGrip). The customized handle variants ensured uncompromised load transfer onto the entire area of the Ironhand® force sensors. The activity of the forearm muscles was recorded using a surface EMG system (Trigno Wireless) from Delsys (Natick, MA, USA) with an interelectrode distance of 10 mm (Trigno Avanti sensor). Grip strength and EMG measurements were synchronized using a Delsys trigger box. Sampling rates were set to 2000 Hz for the dynamometer and 1926 Hz for the EMG, respectively. Linear interpolation was used to compensate for the differences in sample rate.
Study design
25% of the individual maximum grip strength (without the support of the Ironhand®) was defined a priori as the target force for the grip tasks. This level was chosen to be slightly higher than the continuous force limit for static work, which is around 10% of the maximum strength [29]. The 25% force level (only half of the force from our previous study [25]) allows repetitions over a long period (including short breaks), and also justifies ergonomic support in industrial practice. The activity of the forearm muscles was measured with three surface EMG sensors (Trigno Avanti sensors). EMG sensor 1 was positioned near the origin of the flexor digitorum superficialis muscle (M.FDS) at the ulna (M.FDSproximal), EMG sensor 2 at the most prominent point of the M.FDS in the direction of muscle fibers (M.FSDdistal), and EMG sensor 3 on the M. extensor digitorum (M.ED). Figure 2 left shows the EMG sensors applied to a subject’s forearm. The M.FDS and M.ED muscles were chosen because of their functionality for flexion and extension of F2 to F5 and their mostly superficial location, and thus good EMG accessibility. For the present study, the three most common grip types were selected: 2-finger grip (2Finger), 5-finger grip (5Finger), and Full grip (FullGrip).

EMG Sensors applied to subjects forearm and experimental setup.
Using a within-subject design for each of the above-mentioned grip types, we examined the effects of the independent variables without the support of the Ironhand® (Off), with the support of the Ironhand® and “locking tendency” 0% (On_LT0), and with the support of the Ironhand® and “locking tendency” 85% (On_LT85) on the dependent variables “muscle activity of the M.FDS and M.ED” (EMG sensors 1–3). To prevent possible bias of the study results due to systematic fatigue or routine, both the order of the grip tasks and the independent experimental conditions within the grip tasks were randomized. An exemplary experimental program for a grip task is shown in Fig. 3.
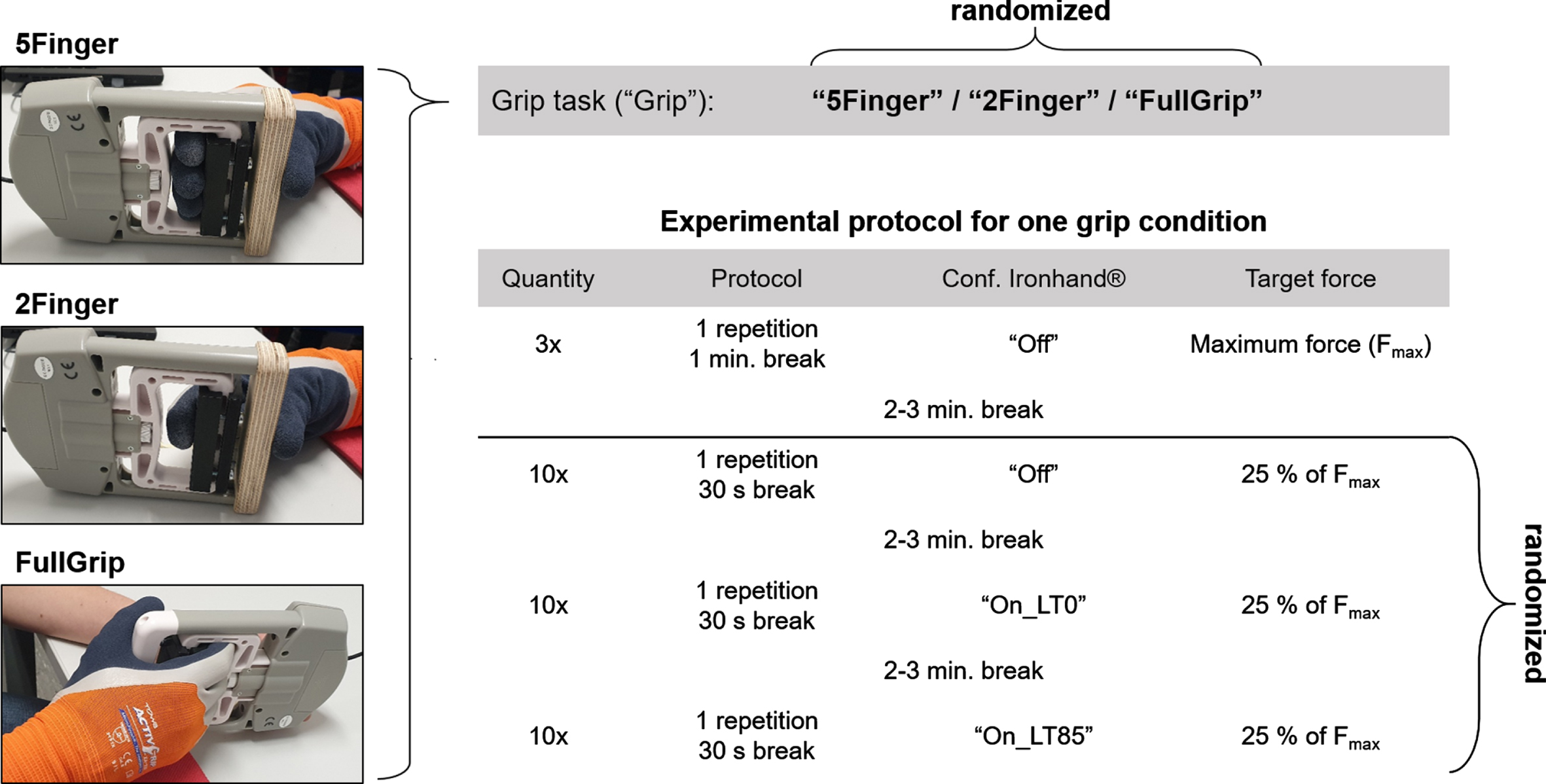
Grip tasks with corresponding example of experimental protocol.
After being instructed by the test supervisor and giving written consent to participate in the study, the test subject’s respective dominant forearm was prepared for the attachment of the EMG electrodes (shaving, light sanding to reduce skin impedance, cleaning the skin surface with alcohol swabs). Subject’s hand anthropometric measurements were taken and the appropriate glove size (Ironhand® and work glove) was determined using a size chart from the manufacturing company Bioservo. After fitting the Ironhand®, the test subjects completed an individual warm-up program of about 20 minutes to get used to the Ironhand® (gripping various objects, testing the “locking tendency” settings, practicing reaching a target force with the hand dynamometer, etc.). The experimental program started with the maximum force measurement of the randomized first grip task. The forearm was positioned in a standardized orientation to avoid uncontrolled effects on EMG signals between the different grip conditions. Correct wrist position was monitored visually by the test supervisor. The subjects were instructed to lay their arm on the table as relaxed as possible and to avoid flexion/extension of the wrist during the measurements. Figure 2 right shows the experimental setup. Using the EMG system, the test supervisor continuously monitored the complete relaxation of the forearm muscles before and after a measurement, and gave feedback if necessary. Subjects used their non-dominant hand to hold and position the hand dynamometer according to their individual needs, and were instructed to achieve the individual target force quickly but in a controlled manner, and to hold it for at least four seconds. For this purpose, the subjects were shown their force time-series data and the current scalar force value in Newton on a display during the measurements. The approximate attainment of the target force value was visually monitored by the test supervisor, with no pre-specified fixed target range. The initial 20-minute warm-up program ensured that subjects were able to reach their target force in a consistent manner across ten repeated trials for each condition. This resulted in a mean deviation from the individual target force of 0.39% (95% CI [0.23%; 0.56%]). The total duration of a measurement was approx. three hours per subject.
Data processing and statistics
Data processing and statistical analysis were performed using the R programming language/development environment [30].
Data processing
Measurement data were processed entirely algorithmically using custom-written R functions. The initial EMG offset was determined from a 2s interval of muscular inactivity prior to each trial, and all subsequent data for the specific trial was adjusted for this offset. The EMG time series were then filtered using a moving root mean square filter with a length of 300 ms [31]. Subsequently, the maximum EMG amplitude of the filtered data was determined for all maximum force measurements to get the subject-specific maximum muscle activity/excitation. EMG measurements at 25% Fmax were then normalized to the subjects’ individually achieved maximal muscle excitation (MVE), with % MVE as the reported unit of muscle activity.
To determine the muscle activity during the measurements at 25% of Fmax, the interval (length 2 s) with the smallest mean square deviation from the target force was identified, and the mean value of the EMG amplitude was calculated in this interval and used for further statistical processing. WLAN EMG transmission errors (resulting in consecutive zeros in the data stream) were identified in the data, and if the above-mentioned 2s interval was affected, the trial was excluded from further analysis. Out of a total of 1986 measurements, 218 (10.9%), 309 (15.6%), and 63 (3.2%) of the measurements had to be excluded for EMG Sensors 1, 2, and 3, respectively.
Statistics
Inferential statistical analysis of the data was performed for each of the three EMG sensors (dependent variables) using a Linear Mixed Effects Model (LMM) [32], analyses of variance (ANOVA), and intragroup (grip task and sex) Tukey post-hoc tests [33]. Missing values (NAs) in LMM were subjected to multiple imputation under the missing at random assumption (MAR). In the LMMs, the effects of the independent variables (fixed effects) “exoskeleton” (Off, On_LT0, On_LT85), “grip” (2Finger, 5Finger, FullGrip), and “sex” (male, female) on the dependent variable “muscle activity” were examined (including interaction effects). Subjects were modeled as random intercepts, with random slopes for “grip” and “exoskeleton”. Since isolated effects of the independent variables “grip”, “exoskeleton”, and “sex” were not in the scope of the present study, the interaction effects of the independent variables “grip: exoskeleton” and “grip: exoskeleton: sex” were essentially of interest in the ANOVA of the LMM. Graphical checks of the LMM assumptions [32, 35] revealed no obvious violations for the current data set. The significance level was set a priori at α= 0.05. Due to multiple inferential statistical tests for the three EMG sensors, all p-values in the present study were corrected using the Bonferroni method. Therefore, the corrected 5% significance level for the present study was α= 0.1666. Since we were unable to obtain valid effect magnitudes from previous studies applicable to our experimental setting, statistical power and sample size could not be specified a priori. However, the post-hoc statistical power of the study was calculated (observed power) [36].
To classify subject-specific changes in muscle activity, the within-subject root mean square error (RMSE) was calculated within grip task and sex groups. Subject-specific mean differences greater than the RMSE were classified as considerable changes.
Results
ANOVA of the LMMs
Effects on M.FDS proximal activity
For EMG sensor 1 (M.FDSproximal), both independent variables “exoskeleton” with p = 0.0005 and “grip” with p < 0.0001 were statistically significant in the Anova. The statistical power (observed power) was 95% for “exoskeleton” and almost 100% for “grip”. The independent variable “sex” was not statistically significant for EMG sensor 1. The interaction effect of the independent variables “exoskeleton” and “grip” in the LMM was also statistically significant for EMG sensor 1 with p < 0.0001. The statistical power of the interaction effect was 99.9% (observed power). Further interaction effects, such as “exoskeleton: sex”, “grip: sex”, and “exoskeleton: grip: sex”, did not reach statistical significance for EMG sensor1.
Effects on M.FDS distal activity
LMM results indicate a statistically significant effect of “grip” on muscle activity (p < 0.0001), with a power of 99.9%. Additionally, the interaction effects “exoskeleton: grip” and “exoskeleton: grip: sex” were statistically significant with p < 0.0001 and p = 0.0063. The statistical power for these two interaction effects was 99.9% (“exoskeleton: grip”) and 87.9% (“exoskeleton: grip: sex”). No other statistically significant effects were found for M.FDSdistal.
Effects on M.ED activity
Linear mixed-effects model means of EMG sensors
Linear mixed-effects model means of EMG sensors
In the Anova of the LMM for EMG sensor3 (M.ED), “exoskeleton” and “grip” (both p < 0.0001), as well as “sex” (p = 0.0051) showed a statistically significant effect. The statistical power for “exoskeleton” was 99.8%, for “grip” 99.9%, and for “sex” 85.2%. In addition, the interaction effect “exoskeleton: grip: sex” was statistically significant with p = 0.0013 (statistical power 94.3%).
Since either the interaction effects “exoskeleton: grip” and/or “exoskeleton: grip: sex” were statistically significant in all Anovas, Tukey post-hoc tests were calculated separately by sex for all EMG sensors within the respective grip task groups (2 fingers, 5 fingers, hand grip).
Tukey post-hoc tests for M.FDSproximal (EMG sensor 1) showed no statistically significant effects for either females or males in the grip task 2Finger (see Fig. 4, top left; Table 1). For the male subjects, the LMM mean values of muscle activity were nearly identical with exoskeleton turned off (Off), exoskeleton turned on without “locking tendency” (On_LT0), and exoskeleton active with “locking tendency” 85% (On_LT85) (see Table 1). Females showed similar results in the three exoskeleton conditions (Table 1).
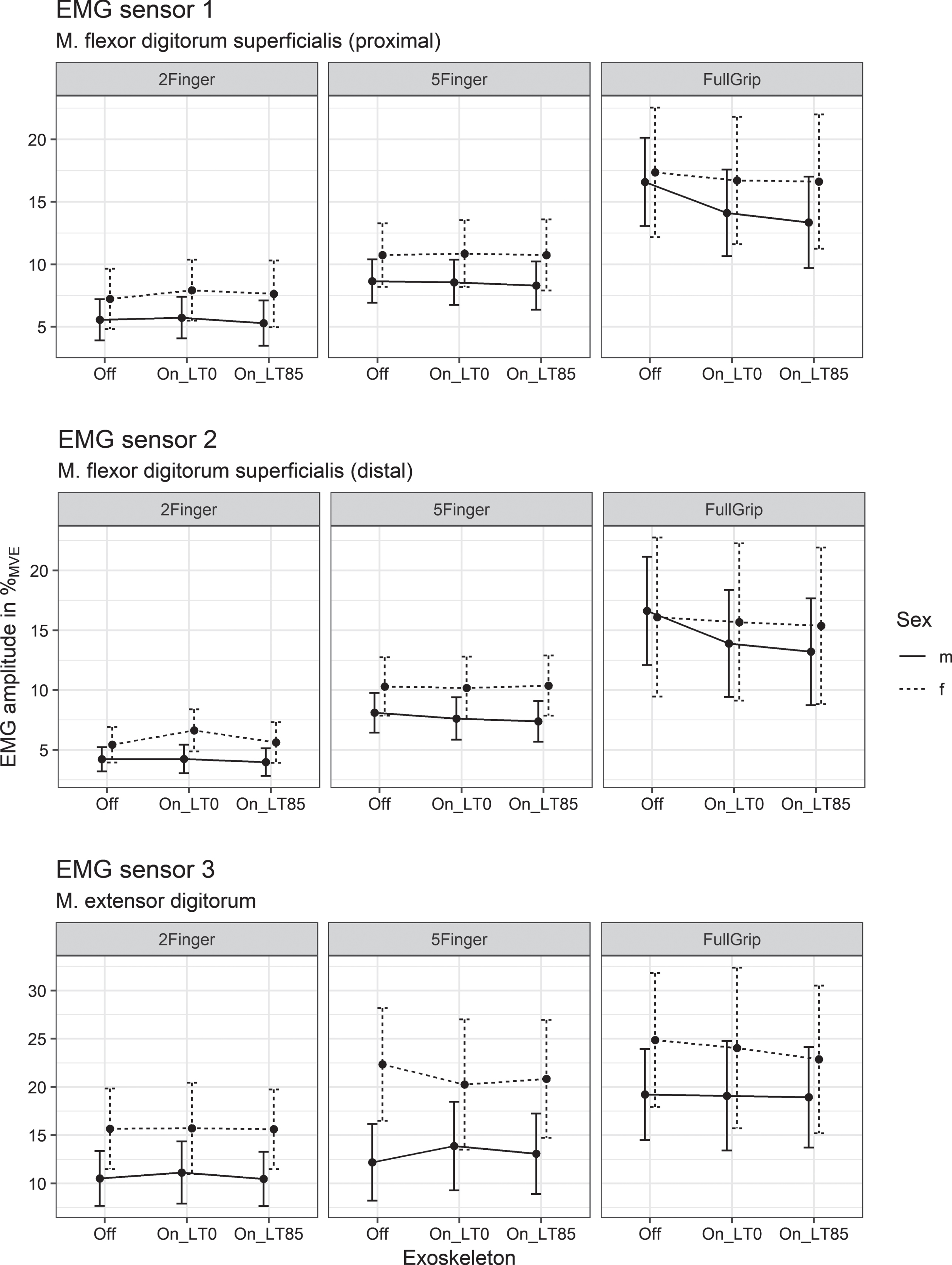
LMM means and 95% confidence intervals for EMG-sensors 1–3.
In EMG sensor 2 (M.FDSdistal) we observed a statistically significant increase in muscle activity for female subjects from exoskeleton Off to OnLT0 (1.21% MVE, 95% CI [0.41% MVE; 1.99% MVE], p = 0.0084, see Fig. 4 middle left; Table 1). This corresponds to a 22% increase in muscle activity between these conditions. However, the sign of the effect was opposite from the intended effect of stress reduction through the Ironhand®. A non significant decrease of 5.62% MVE in muscle activity was observed between On_LT0 and On_LT5. For the male subjects, no statistically significant changes in muscle activity were observed, with levels of M.FDSdistal nearly constant across the exoskeleton conditions Off, On_LT0, and On_LT85 respectively.
Muscle activity of the M.ED (EMG sensor 3) was nearly constant for both sexes across the exoskeleton conditions Off, On_LT0, and On_LT85, with no statistically significant effects (see Fig. 4, bottom left, Table 1).
In general, for the grip task 2Finger, hardly any systematic subject-specific effects were detected in the raw data across exoskeleton Off, On_LT0, and On_LT85 for the three EMG sensors (Fig. 5, left column).
For M.FDSproximal (EMG sensor 1), the electrical muscle activity increased considerably from exoskeleton Off to On_LT0 for 4 (2 female, 2 male) out of 22 subjects (>RMSE; male subjects: 1.15% MVE; female subjects: 1.07% MVE), and from Off to On_LT85 for 3 subjects (2 female, 1 male). The maximum increase in mean M.FDSproximal muscle activity for was 5.68% MVE.

Subject means for EMG-sensors 1–3 (raw data).
For EMG sensor 2 (M.FDSdistal), muscle activity increased considerably from Off to On_LT0 for 5 subjects (2 female, 3 male) (>RMSE; male subjects: 0.91% MVE; female subjects: 1.300% MVE), and from Off to On_LT85 for 3 subjects (1 female, 2 male). The maximum increase in the mean muscle activity for the M.FDSdistal was 5.23% MVE.
For the M.ED (EMG sensor 3) and experimental condition On_LT0, muscle activity increased considerably compared with Off for 5 subjects (1 female, 4 male) (>RMSE; male subjects: 2.00% MVE; female subjects: 2.43% MVE), and for On_LT85 for 2 male subjects. The maximum increase in mean muscle activity was 7.32% MVE for M.ED.
Relative to exoskeleton Off, the subject-specific increases in muscle activity, classified as considerable, for the M.FDS (proximal and distal) ranged from 13.10% to 97.79% (Mean On_LT0 = 52.73% (SD = 25.23%), Mean On_LT85 = 32.55% (SD = 11.68%)). For the M.ED, the relative subject-specific increases (considerable) in muscle activity (starting from Off) ranged from 12.52% to 48.27% (see Fig. 5, bottom left; Mean On_LT0 = 30.62% (SD = 14.81%), Mean On_LT85 = 21.17% (SD = 2.06%)).
5Finger post-hoc tests
For the M.FDSproximal (EMG sensor 1), the mean values across the exoskeleton conditions Off, On_LT0, and On_LT85 were approximately constant for both sexes (see Fig. 4, top center; Table 1). No statistically significant effect was found.
Similar effects were found for M.FDSdistal (EMG sensor 2) for the female subjects (see Fig. 4, middle; Table 1). For the male subjects, the mean values decreased slightly across Off, On_LT0, and On_LT85. However, this slight decrease in M.FDSdistal muscle activity did not reach statistical significance (see Fig. 4, middle; Table 1).
M.ED (EMG sensor 3) activity also did not show statistically significant changes for either sex across exoskeleton conditions (see Fig. 4, bottom center; Table 1).
5 Finger subject-specific effects
Similar to the 2-finger grasp condition, systematic subject-specific effects across the experimental conditions exoskeleton Off, On_LT0, and On_LT85 were not evident for the 5Finger grip task, (Fig. 5, middle column).
For M.FDSproximal (EMG sensor 1) and exoskeleton condition On_LT0, myoelectrical muscle activity increased considerably for 3 (2 female, 1 male) out of 22 subjects (>RMSE; male subjects: 1.44% MVE; female subjects: 1.12% MVE), and with On_LT85 for 5 out of 22 subjects (3 female, 2 male). The maximum increase in the mean muscle activity for M.FDSproximal was 3.21% MVE.
At EMG sensor 2 (M.FDSdistal), muscle activity increased considerably from Off to On_LT0 for 2 subjects (1 female, 1 male) (>RMSE; male subjects: 1.18% MVE; female subjects: 1.30% MVE) and from Off to On_LT85 again for 2 subjects (1 female, 1 male). The maximum increase in mean muscle activity was 3.14% MVE for M.FDSdistal.
For M.ED (EMG sensor 3) and On_LT0 exoskeleton condition, muscle activity increased considerably compared with Off for 3 male subjects (>RMSE; male subjects: 2.31% MVE; female subjects: 2.49% MVE), for On_LT85 for 3 subjects (1 female, 2 male; Fig. 5, bottom center). The maximum increase in mean muscle activity was 19.06% MVE for M.ED.
Summary
For M.FDS (proximal and distal), the considerable relative subject-specific increases in muscle activity (starting from Off) ranged from 9.10% to 43.58% (Mean On_LT0 = 27.00% (SD = 10.35%), Mean On_LT85 = 17.64% (SD = 8.05%)). For M.ED, the considerable relative subject-specific increases in muscle activity ranged from 23.66% to 90.24% (see Fig. 5, middle bottom; Mean On_LT0 = 64.88% (SD = 35.57%), Mean On_LT85 = 41.57% (SD = 29.39%)).
FullGrip post-hoc tests
For the male subjects, the LMM mean muscle activity of M.FDSproximal (EMG sensor 1) decreased from 16.59% MVE for exoskeleton Off to 14.11% MVE (On_LT0) and then to 13.36% MVE (On_LT85, see Fig. 4, top right; Table 1). In this context, both the decrease in muscle activity from exoskeleton Off to On_LT0 of 2.48% MVE (p < 0.0001, 95% CI [1.57% MVE; 3.39% MVE]), and from Off to On_LT85 of 3.23% MVE (p < 0.0001, 95% CI [2.37% MVE; 4.10% MVE]) were statistically significant. Relative to exoskeleton Off, On_LT0 decreased muscle activity by 15% (95% CI [9%; 20% ]) and On_LT85 by 19% (95% CI [14%; 25% ]). For both statistically significant effects, the null hypothesis had to be rejected and the alternative hypothesis accepted (intentional decreasing effect). For M.FDSproximal, the female subjects showed no statistically significant decrease in muscle activity.
For M.FDSdistal (EMG sensor 2), the muscle activity of the male subjects decreased from Off to On_LT0 and On_LT85 (see Fig. 4, middle right; Table 1). Again both decreases were statistically significant (Off to On_LT0 by 2.73% MVE, p < 0.0001, 95% CI [1.71% MVE; 3.74% MVE]; Off to On_LT85 by 3.41% MVE, p < 0.0001, 95% CI [2.40% MVE; 4.43% MVE]). Relative to Off, On_LT0 decreased muscle activity by 16% (95% CI [10%; 23% ]) and On_LT85 by 21% (95% CI [14%; 27% ]). For both statistically significant effects, the null hypothesis had to be rejected and the alternative hypothesis accepted (intentional decreasing effect). The female subjects again showed no statistically significant decrease in muscle activity for the M.FDSdistal (see Fig. 4, middle right; Table 1).
Mean muscle activity of M.ED (EMG sensor 3) showed almost no change for the male subjects over the exoskeleton test conditions (see Fig. 4, bottom right; Table 1). For the female subjects, muscle activity of M.ED decreased from Off to On_LT0 to On_LT85. However, this decrease in muscle activity did not reach statistical significance due to high variance (see Fig. 4, bottom right; Table 1).
FullGrip Subject-specific effects
For M.FDSproximal (EMG sensor 1) and exoskeleton On_LT0, electrical muscle activity increased considerably for one female subject (>RMSE; male subjects: 2.69% MVE; female subjects: 2.91% MVE) and with On_LT85 again for 1 female subject (Fig. 5, top right). The maximum increase in the mean muscle activity for M.FDSproximal was 4.22% MVE. 6 of 15 subjects in the group of male subjects that showed statistically significant decreases in myoelectric muscle activity for the M.FDSproximal showed increases in muscle activity for either On_LT0 or On_LT85 (Fig. 6, top), but none of these increases were classified as considerable (>RMSE).
For M.FDSdistal (EMG sensor 2), On_LT0 considerably increased electrical muscle activity for 1 male subject (>RMSE; male subjects: 2.91% MVE; female subjects: 3.59% MVE) and On_LT85 for 1 female subject (see Fig. 5, middle right). The maximum increase in the mean muscle activity for M.FDSdistal was 5.24% MVE. In the group of male subjects that showed statistically significant decreases in muscle activity for the M.FDSdistal under the On_LT0 and On_LT85 experimental conditions, increases in muscle activity were again seen in 6 of 15 subjects for either On_LT0 or On_LT85 (Fig. 6, bottom). For one subject, the increase in muscle activity from Off to On_LT0 was classified as considerable (>RMSE). The muscle activity of this subject’s M.FDSdistal increased by 3.70% MVE. Based on exoskeleton Off, this corresponded to a relative increase of 9.98%.
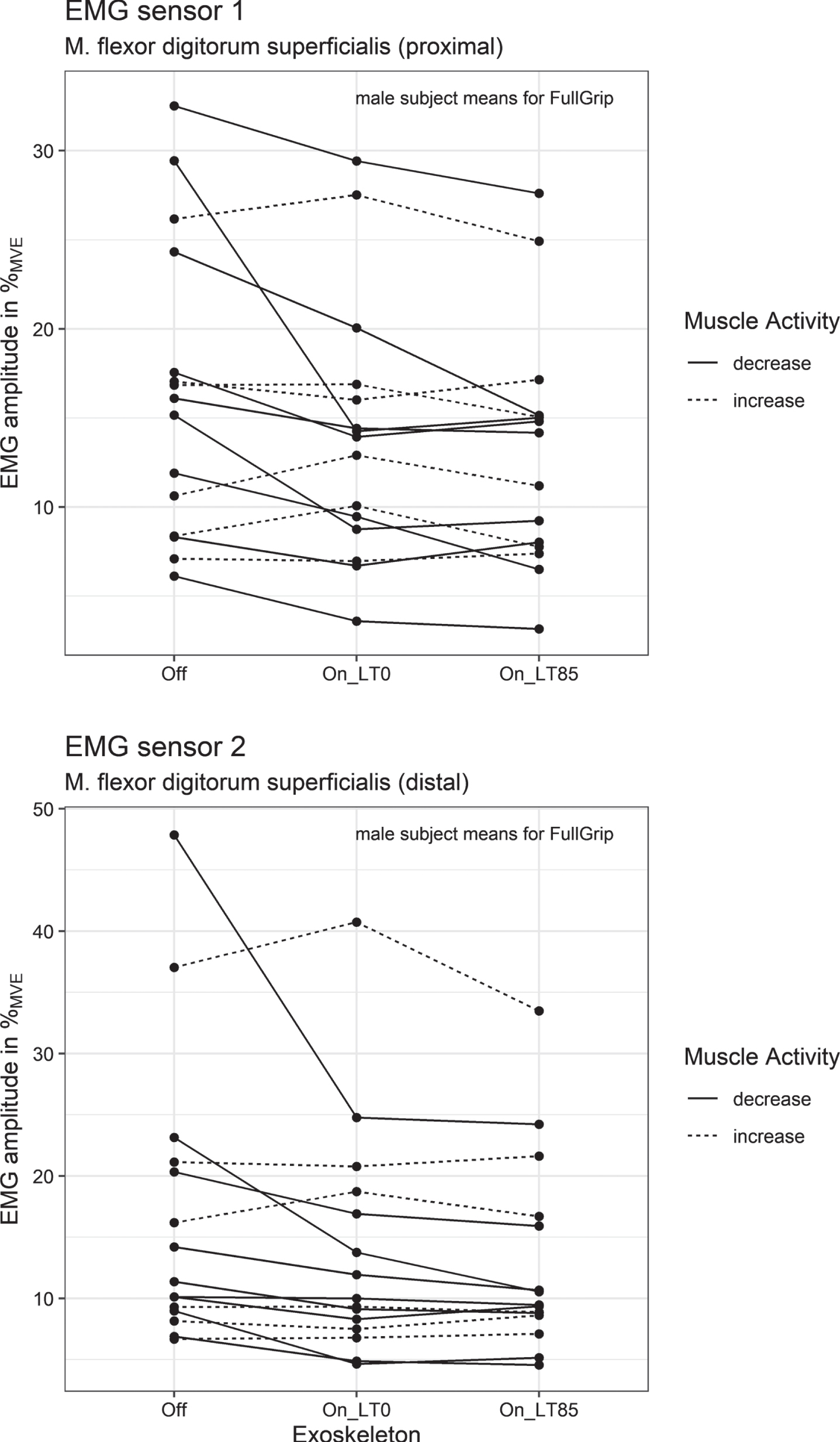
Subject means for male subjects and FullGrip (EMG-sensors 1-2, raw data).
For M.ED (EMG sensor 3), muscle activity incr-eased considerably (>RMSE; male subjects: 3.91% MVE; female subjects: 5.90% MVE) from Off to On_LT0 for 3 subjects (1 female, 2 male), and from Off to On_LT85 again for 3 subjects (1 female, 2 male; Fig. 5, bottom right). For M.ED, the maximum increase in mean muscle activity was 20.90% MVE.
Based on exoskeleton Off, for M.FDS (proximal and distal), the considerable relative subject-specific increases in muscle activity (starting from Off) ranged from 9.98% to 61.20% (Mean On_LT0 = 35.59% (SD = 36.21%), Mean On_LT85 = 23.24% (SD = 9.96%)). For M.ED, the relative subject-specific increases in muscle activity classified as considerable ranged from 27.76% to 310.58% (see Fig. 5, middle bottom; Mean On_LT0 = 142.91% (SD = 145.31%), Mean On_LT85 = 112.55% (SD = 131.65%)).
Discussion
Requirement prerequisite for the use of an exos-keleton in industrial assembly is that it can effectively and reliably reduce work-related stress. The work-related stress on the hand and forearm in gripping activities is mainly determined by the required intensity and volume of the manual activity (e. g. applied force and the number of repetitions). For a given activity, stress reduction translates into decreased myoelectrical muscle activity of the forearm flexors and extensors when supported by an active hand exoskeleton (Ironhand®). Therefore the present study was conducted to investigate the effect of the Ironhand® exoskeleton on the myoelectrical activity of the M.FDS and M.ED muscles at 25% of Fmax. The three most common grip tasks in automotive assembly were selected as experimental conditions.
Exoskeleton effects due to grip tasks and sex
The results show that effects of the Ironhand® vary depending on the respective grip and sex. A statistically significant decrease in muscle activity of M.FDS was found only for the male subjects and the FullGrip condition across exoskeleton support levels. In our previous work [25], significant decreases in muscle activity were also exclusively seen in the FullGrip experimental condition. However, the results cannot be compared directly because the design of the two studies differs considerably (e.g., no investigation of sex-specific differences). For the remaining grip tasks (2Finger, 5Finger), no decrease of muscular activity in the M.FDS was found (equivalent to [25]). For the female subjects, the muscle activity even increased by 1.21% MVE (95% CI [0.41% MVE; 1.99% MVE]) from exoskeleton Off to On_LT0 in the 2Finger grip task. Based on exoskeleton Off, this corresponds to 22% higher muscle activity of the M.FDS. This effect does not correspond to claims or any hypothesis of a reduction in muscle activity. The results for M.FDS in the present study are nearly an exact replication of the effects found in our previous study [25] (23%), which is remarkable given the vastly different study design characteristics (50% Fmax, non-randomized design, only one EMG sensor, brand-new Ironhand® glove, n = 12 subjects, and no testing of sex-specific effects). In contrast to M.FDS, no statistically significant effects were found for M.ED activity (extensor side of the forearm) in the present study.
The most likely reason for sex differences in activity decrease of M.FDS in the FullGrip condition is the considerably lower (mean) force level of females. The mean target force (25% Fmax) of females for the FullGrip experimental condition was 49.86 N (SD = 12.86 N), compared to 77.76 N (SD = 15.85 N) for men. As expected, the linear regression between target force and sex showed a highly significant relationship, with R2 = 0.43 and p < 0.0001. At lower target forces, Ironhand® support does not seem able to effectively decrease M.FDS muscle activity. However, with the present study design, it was not possible to determine whether characteristics of the subjects with lower maximal grip strength or the lower target force level itself caused this effect. It is more likely that at low target force levels, the sensors in the fingertips of the Ironhand® cannot be loaded sufficiently to ensure adequate support of the exoskeleton. The pre-worn condition of the Ironhand® gloves may have contributed to this circumstance in the present study. Experience shows that the sensitivity of the force sensors in the fingertips decreases rapidly during use at the beginning of use and then levels out for a longer period of time. In practice, this would suggest that Ironhand® support in FullGrip at lower force requirements (< = approx. 50 N) may be insufficient with pre-worn gloves and deteriorated sensor sensitivity.
Differences between anatomic and Ironhand® force vectors
Another possible cause for the observed discre-pancy between the different grip tasks are the directions of the resulting grip force vectors (difference between the natural force vectors of the hand and the artificial tension force vectors of the Ironhand®). The latter depends largely on the alignment of the tension cables (artificial tendons) in the soft gloves of the exoskeleton and may –depending on the position of the fingers –substantially deviate from the anatomically optimal direction. In contrast to the real tendons of the fingers, which are tightly connected to the phalanges by ring and cruciate ligaments, artificial tendons of the Ironhand® glove cannot mimic this characteristic in every finger position. Technically, this is almost impossible to achieve with artificial tendons in a textile glove, since a very tight-fitting glove with radial tensile strength would impair both finger mobility and blood flow to the more distal phalanges. Furthermore, the artificial tendons of the Ironhand® only attach to the fingertips, which induces shear forces on the finger joints in grips with rather stretched fingers, such as the 2Finger and 5Finger conditions, and reduces the efficiency of the Ironhand®. The observed increase in muscle activity of M.FDSdistal in female subjects during the 2Finger grip could be the result of a compensatory activity of the M.FDS in response to the shear forces artificially induced on the finger joints by the exoskeleton. This assumption is further supported by the fact that the FullGrip condition, which potentially has the most favorable alignment between the artificial tendons of the glove and the tendons of the hand/fingers, is the only grip to show a reduction in neuromuscular activity of the M.FDS.
For the practical use of the Ironhand® or comparable hand exoskeletons in industrial assembly, such a compensation mechanism would be undesirable. Especially since grip types with extended fingers, such as the 2Finger or 5Finger grip conditions [37], have a high potential to increase work-related strains and occur frequently [26].
Subject-specific differences
The effects of the Ironhand® in the respective grip conditions were further characterized by individual differences between the subjects (Fig. 5). For example, for the 2Finger and 5Finger experimental conditions, some subjects showed substantial increases in muscle activity when using the Iron-hand® above the intraindividual measurement error (RMSE). For the 2Finger grip, muscle activity of M.FDS increased by up to 97.79% (reference level exoskeleton Off) for up to 23% of subjects (depending on EMG sensor and exoskeleton condition). The activity of M.ED increased up to 48.27% for up to 23% of the subjects (depending on exoskeleton condition). For the 5Finger grip, increases in muscle activity of M.FDS from 9.10% up to 43.58%, and of M.ED from 23.66% up to 90.24% were recorded for up to 23% of the subjects. In the FullGrip condition, considerable increases in muscle activity (> RMSE) of M.FDS of 9.98% and 61.20% only occurred for two subjects. For M.ED (FullGrip), 3 out of 22 subjects showed increases in muscle activity ranging from 27.76% to 310.58%.
Therefore, in addition to statistical significance tests, which are performed on a group level and marginal group means, a detailed exploratory analysis of exoskeleton effects at subject level should be performed to evaluate them from a safety and regulatory perspective. The lack of a statistically significant effect in the 5Finger condition on muscle activity obscures the fact that decreases and increases in muscle activity cancel out in this case, with 23% of subjects showing an undesirable increase in muscle activity. Even in the group of 15 male subjects in the grip condition FullGrip, which showed statistically significant decreases in muscle activity for M.FDS, muscle activity increased from Off to On_LT0 and from Off to On_LT85 for 6 subjects, with one of these increases being of considerable magnitude. With this in mind, the question for companies and decision makers in occupational safety is whether increases in muscle activity can be tolerated, and if so, what kind of threshold should be applied. This remains an open question and can only be assessed in future studies involving continuous use of exoskeletons under ecologically valid conditions.
Furthermore, the effectiveness of the Ironhand® might interact with the individual skill of the subject. In our study, we allowed each subject a 20 minute accommodation period to get used to the Ironhand® and to practice the different grips with the exoskeleton. Skilled subjects might be able to use the support of the Ironhand® more effectively, possibly resulting in a steep learning curve. This assumption is strongly supported by the extreme increases in muscle activity of M.ED in 2 and 3 subjects in the experimental conditions 5Finger and FullGrip, respectively (Fig. 5 bottom center and right).
Moreover, the observed differences in muscle activity can also be attributed to interindividual anatomical differences (e. g. hand size, finger length, lever geometry). Despite determining glove size according to the manufacturer’s size specifications, an individually optimal fit of the glove can hardly be achieved with only 3 sizes available. This may potentially affect the effectiveness of the exoskeleton. However, there was no negative feedback from the subjects on the fit of the gloves. One subject with particularly large hands reported slight difficulty gripping the hand dynamometer, but was still able to complete the entire experimental protocol.
Other factors, such as the subjective perception of the support or the fatigue or training status of the muscles, were not controlled for in the present study. However, for a more comprehensive evaluation of the measurable and perceptible effects of hand exoskeletons, they might be considered in future studies.
Validity of the measurement results
The validity of the EMG signal cannot be conclusively assessed. In principle, myoelectric signals cannot be used directly to infer the target variable hand force or stress in general, as EMG signals depend on a variety of factors, such as the recruitment and frequency characteristics of the motor units involved or, more generally, the characteristics of the muscles [31, 38]. Moreover, the isolated measurement of a single muscle in the forearm is hardly possible with surface electrodes. In addition to M.FDS, partially overlying muscles such as the M. flexor carpi radialis and M. palmaris longus are innervated during vigorous flexion of the fingers. During finger extension, in addition to the target muscle M.ED, the M. extensor carpi ulnaris is also innervated (among others). Therefore, the simultaneous innervation of different muscles with different characteristics in a confined space such as the forearm almost inevitably leads to crosstalk when measuring myoelectrical muscle activity with surface electrodes. An isolated effect on the muscle activity of deeper muscles in the forearm is considered rather unlikely due to the close interaction of the muscles in the forearm, but cannot be completely ruled out. Therefore, invasive EMG applications may be necessary to specifically assess the effects of exoskeleton support on specific (non-superficial) muscles. However, exoskeletons themselves may prevent the use of invasive EMG, so this remains an open issue for scientific debate and future studies.
Conclusion
Besides differences across three grip conditions, the current study revealed substantial individual and sex-specific differences in muscle activity across exoskeleton support levels. Therefore, in addition to statistical significance tests, a detailed exploratory analysis of exoskeleton effects at subject level should be performed. The lack of a statistically significant effect can obscure the finding that decreases and increases in muscle activity cancel out. Even in groups with a statistically significant effect, some individuals can show opposite effects. For example, in the present study this was true for 6 out of 15 subjects. Future prospective studies may address the long-term effects of such opposite effects and thus allow for a more comprehensive evaluation of their potential harms. Despite minor differences in the respective study designs, the results of the present study closely resemble the findings of our previous work with a similar setup [25]. Both studies illustrate the high degree of complexity that exoskeleton designers face when developing devices to support human performance in occupational settings.
Ethical approval
The present study was approved by the ethics committee of Chemnitz University of Technology on 05/12/2020 (reference number: V-410-17-AKH-Hand-Exoskelett-13112020).
Informed consent
All subjects were fully informed about the study before the start of the measurements and gave written consent to participate in the study. Consent to participate could be revoked at any time (even during the measurements).
Conflict of interest
The co-author Dr.-Ing. Hensel-Unger is employed by Audi AG. There is no conflict of interest.
Footnotes
Acknowledgements
We would like to thank Lisa C. Peterson for her excellent linguistic support and proofreading.
Funding
The Audi AG provided financial and material support for the present study.