
Abstract
BACKGROUND:
The job demands on nurses have increased. Conflict between work life and family life may lead to stress and lower work engagement. Consequently, nurses may choose a different career path or leave the profession.
OBJECTIVE:
Examine the extent to which perceived job demands (interpersonal conflicts at work and workload), work engagement, work-family conflict and family-work conflict are associated with turnover intentions, and examine a possible moderating effect of work-family conflict on the relationship between the intention to leave the nursing profession, job demands and work engagement.
METHODS:
Cross-sectional study using Hobfoll’s Conservation of Resources theory. Data were collected from a sample of 807 registered nurses (RNs) from western Sweden. Tests of moderation were conducted using the PROCESS software macro developed by Andrew F. Hayes.
RESULTS:
Work-family conflict was a significant moderator in the relationship between the intentions to leave the nursing profession and work engagement as well as interpersonal conflicts at work. Low work engagement, high work-family conflict and high job demands intensify turnover intentions in well-educated and well-experienced nurses.
CONCLUSIONS:
The results imply that work-family conflict has a greater impact when RNs experience lower work engagement. In other words, higher motivation implies a lower moderation effect of work-family conflict. Managers should promote a positive working climate by listening to and providing nurses with opportunities to develop their skills. By so doing, managers can gain better understanding of nurses’ resources, knowledge and work situation, thus strengthening nurses’ confidence and ability to practice their profession.
Keywords
Introduction
There are major problems with retaining registered nurses (RNs) in both Europe, including Sweden, and the United States. Many RNs have high turnover intentions and the retention is low [1]. Nurses decide to change their career path due to, for instance, exposure to stressful situations caused by the combination of high job demands and low job resources [2, 3]. Stress appears when there is an imbalance in the individual’s resources [4–7]. One important resource that nurses bring to work is their work engagement. If there is a shortfall in the RNs’ engagement, the risk of creating a bad job environment increases [8]. The RNs’ capability of providing safe and quality care is limited by interruptions, time pressure, performance limits and unclear tasks, which are associated with work stress and cognitive failures for RNs [9], which may lead to occupational injury for RNs and worsened health for patients [10]. These factors may make RNs feel negatively about their work [8] and they may bring such negative thoughts and feelings with them home [11]. A work-family conflict (WFC) arises when work-related requirements (e.g. irregular working hours, workload or overtime) affect the RN’s private and family life (e.g. participation in children’s activities, lack of childcare or care of parents). A family-work conflict (FWC) arises when family-related requirements and responsibilities affect work activities [12]. When a person’s roles, work role and family role, become irreconcilable, a role conflict arises which can create stress [11].
Work engagement (such as absorption, dedication and vigor) is a resource, which has a high correlation with motivation, and when an employee has high resources he or she manifests low turnover intentions, decreased stress and fewer decisions to change career path. This study focuses on investigating turnover intentions, job demands, work engagement (resource), WFC and FWC among RNs in Sweden.
Theoretical framework: Hobfoll’s conservation of resources theory
Hobfoll’s [5, 13] Conservation of Resources (COR) theory states that people strive to gain, increase, protect and retain the “resources” necessary to manage psychological suffering and, for example, to avoid work-family conflict (WFC) and family-work conflict (FWC). The COR theory includes four main categories of resources: objects, meaning socioeconomic possessions; personal qualities, meaning skills such as self-confidence; conditions, meaning different roles such as being employed or in a relationship; and energies, meaning contributing resources such as knowledge, time and money.
We constantly look for new valuable resources that we can use to avoid situations where stress can affect us negatively [5]. The COR theory contains two principles: (i) the impact of the gain or loss of resources is asymmetric, and (ii) individuals must use resources to limit any loss of resources. Individuals who have limited resources often become defensive in order to protect their resources, which makes them less successful under high pressure [5]. COR theory is a motivational theory. It explains behavior based on the evolutionary need to “acquire and conserve resources for survival, which is central to human behavioral genetics” [14].
Hobfoll [5] examined how the organization’s attitude can create interactions that are conducive to engagement by introducing the “camel caravan” as a new concept in the COR theory. This is a metaphor for the contextual conditions that enrich, promote, protect and support the resources of the individual, section, employee group, or entire organization. The starting point is the interaction between individuals in the workplace. By motivating individuals to maximize their work performance by using teams and mentoring one can increase resources and decrease stress. The rules of engagement serve as an important personal resource for the employee’s work performance.
Work and family life conflicts, turnover intentions, job demands and work engagement are tightly linked to how an individual manages his or her resources and stress. In this paper we use Hobfoll’s COR theory to explain the link between turnover intentions, perceived job demands, work engagement (resource), WFC and FWC among RNs.
Research on nurses and turnover intentions, job demands, work engagement, WFC and FWC
Research shows that RNs’ work dissatisfaction, stressful work environments and workload (especially as regards their responsibility for patients) are linked to poor well-being, feelings of stress and insufficient support [e.g. 8, 15–22], and stress on psychological health [23–26]. Job demands is an unavoidable stressor that leads to many negative consequences, such as lowering the quality of RNs’ working lives, and it connects directly to job dissatisfaction and turnover intentions [21]. There is a positive correlation between job demands, turnover intentions, and leaving the current workplace [4, 28]. RNs’ psychological engagement in their work depends on their workload and how satisfied they are with the care they can provide [29].
WFC conflict can be a severe stressor for RNs and is therefore one of the most investigated risk factors when studying different workplaces [19, 30]. WFC and FWC can trigger health-related problems [11, 31] and RNs’ work satisfaction is affected by their ability to achieve balance between their workplace and family life commitments [21]. The more support they receive from managers, the better RNs become at achieving balance between work and family life and at creating development opportunities [17].
Only a few studies on the work engagement (resources) of RNs using Hobfoll’s COR theory have been made. We found no Swedish research in this area. Generally, related studies focus on work-related stress and burnout in different occupational groups such as informal caregivers, lawyers, RNs, physicians, police officers and social workers. Only one study used COR theory focusing on work engagement (resources) among RNs in Poland [29].
Objectives and research questions
The objectives of this study are to examine the extent to which perceived job demands (interpersonal conflicts at work and quantitative workload), work engagement, work-family conflict (WFC) and family-work conflict (FWC) are associated with turnover intentions; and to examine a possible moderating effect of WFC on the relationships between the intention to leave the nursing profession and job demands and work engagement.
Because the overall number of working RNs is insufficient, we assume that the intention to leave the nursing profession entirely is more ‘dangerous’ for patients and society than the intention to leave one organization to begin nursing work in another organization. Further, based on past research, we expect that WFC is stronger than FWC. Consequently, if job demands, work engagement and WFC (but not FWC) are significant predictors of turnover intention, we would test the following hypotheses aiming to show a possible moderating effect of WFC on the relationship between the intention to leave the nursing profession and job demands and work engagement. Hypothesis 1: WFC moderates the relationship between quantitative workload and the intention to leave the nursing profession. Hypothesis 2: WFC moderates the relationship between interpersonal conflicts at work and the intention to leave the nursing profession. Hypothesis 3: WFC moderates the relationship between work engagement and the intention to leave the nursing profession.
Materials and methods
Study design, settings and sample
We implemented a cross-sectional quantitative design. The study used a purposive convenience sample. We asked 1,450 RNs working in hospital- and primary healthcare in western Sweden to respond to a questionnaire; 939 of the RNs responded (64.8%response rate). We excluded the data provided by RNs who did not report having children at home or a partner; in doing so, we focused only on RNs who had additional household chores and responsibilities regarding, for example, contacts with the children’s schools or different responsibilities with the children’s non-school activities. This subsample (n = 817) was examined regarding assumptions for multivariate methods, and we excluded 10 multivariate outliers on the independent variables, identified by Mahalanobis distances (p < 0.001). As a result, the current study sample consisted of 807 RNs (mean age = 42 years, SD = 11.3, range 23–70). Their average employment as a RN was 13.8 years (SD = 10.7, range 0.3–50 years). Around 38%of the RNs had two children or more living at home, a fact that can increase WFC. Descriptive statistics (demographic variables) for the included RNs are shown in Table 1.
Individual and professional characteristics of the nurses living with at least one child and/or living with a partner (N = 807)
Individual and professional characteristics of the nurses living with at least one child and/or living with a partner (N = 807)
aPostgraduate (Second Cycle) Program in Specialist Nursing. bHigher Education Credits.
Almost nine out of ten (88.5%) of the 807 RNs were female, reflecting the overall proportion of female RNs working in Sweden (88%) (Statistics Sweden, 2017) and other European countries (e.g. Poland 99.6%, Greece 89.0%and Switzerland 92.8%) [31]. More than two out of five (43%) of the responding and analyzed RNs were specialist nurses, indicating that the studied population was well-educated and well-experienced.
Sociodemographic data on the RNs, their turnover intentions (outcomes), as well as their perception of their job demands (measured by workload and interpersonal conflicts), work engagement (i.e. resources) (absorption, dedication and vigor), work-family interface, were collected using an Internet-based questionnaire (Google Forms [2018], www.google.com/forms/about/). A small portion of the data was obtained through a standard paper questionnaire administered to RNs undergoing further specialist education in diabetes care, mental health care, pediatric care, primary healthcare and theatre care at University West in Sweden. Like the other RNs included in this study, these RNs also worked in hospitals or primary healthcare centers in western Sweden.
Ethical approval
This study was conducted in accordance with the applicable ethical rules [32]. Written informed consent was obtained from all subjects. The participants were not under the age of 16. The study was conducted in accordance with applicable ethical rules (the Helsinki Declaration) and was reviewed by the local ethics committee (DNR 2014/730 B 22, University West).
Outcome variables
A RN’s turnover intention was measured by two single-item scales [29, page 5]: “During the recent period I have considered leaving this hospital/organization to begin work in another hospital/organization” (the intention to leave the current work-place), and “During the recent period I have considered leaving the nursing profession” (the intention to leave the profession). The two single-item scales were answered on a 0 to 4 scale (0 = Never; 4 = All the time). High scores (values of 3 or 4) indicate a high turnover intention.
Explanatory variables
Sociodemographic variables. To describe the group, the RNs were asked about their individual and family characteristics. A number of variables were used as control variables, due to the fact that they may indicate the extent of different household chores and other duties within a family relating to WFC and FWC. Because we were interested in discussing possible differences in the studied variables between Swedish and Polish RNs, we used similar variables as Dåderman and Basinska [29], i.e. the RN’s age, number of children (we have, however, asked about “the number of children at home”, and not “the number of children”), and whether the RN’s partner was employed (coding 0 = Partner unemployed; 1 = Partner employed).
Independent variables. To assess the work-family interface, we used the Work-Family Conflict (WFC) and Family-Work Conflict (FWC) scales [12]. The Swedish versions use the term “private life” instead of “family”. The scale constructor, Professor Netemeyer, granted the researchers permission to make this terminological change. The scales measure “how work life and family life affect each other” [12, page 400]. Each scale has five items that are answered on a 1 to 7 scale (1 = Strongly agree; 7 = Strongly disagree). An example of a WFC scale item is “The amount of time my job takes up makes it difficult to fulfil family responsibilities” (see Appendix, [12] page 410). An example of a FWC scale item is “I have to put off doing things at work because of demands on my time at home”, thus mirroring the item of the WFC scale by reversing the source of conflict. In this study, Cronbach’s alpha was 0.95 for WFC and 0.80 for FWC.
The quantitative workload was measured using the 5-item Quantitative Workload Inventory (QWI) [33]. The responses are provided using a 1 to 5 scale (1 = Less than once per month or never; 5 = Several times per day). An item example is “How often does your job require you to work very fast?” The sum of the item scores indicates the respondent’s workload, i.e. his or her amount of work within a given period. A high overall score indicates a high workload. In this study, Cronbach’s alpha was 0.90.
Workplace conflicts with other people were measured using the 4-item Interpersonal Conflict at Work Scale (ICAWS) [33]. The items concern how often an event occurs at work, and are answered on a 1 to 5 scale (1 = Less than once per month or never; 5 = Several times per day). An item example is “How often do you get into an argument with others at work?” A high overall score indicates frequent interpersonal conflicts at work. In this study, Cronbach’s alpha was 0.81.
We measured work engagement (i.e. resource) using the 9-item Utrecht Work Engagement Scale (UWES-9) [34]. The UWES-9 measures vigor (“At my work, I feel that I am bursting with energy”), dedication (“I am enthusiastic about my job”) and absorption (“I feel happy when I am working intensively”). The items are answered on a 0 to 6 scale (0 = Never; 6 = Always/every day). A high score indicates that the person has a higher level of engagement. In this study, Cronbach’s alpha was 0.74, 0.83 and 0.86 for absorption, dedication and vigor, respectively. In our regression analyses we used a total scale of work engagement Cronbach’s alpha = 0.92, because these three subscales were highly correlated with each other (> 0.70, Table 2) and this circumstance caused spurious results in the analyses. Missing data (<1%) in continuous predictors (but not demographic variables) were filled in with the sample’s means.
Correlations and descriptive statistics of the variables for the Swedish nurses (N = 807)
Correlations and descriptive statistics of the variables for the Swedish nurses (N = 807)
Note. *p < .05 after the Bonferroni correction (0.05/36 = 0.0014). S = skewness; K = kurtosis; WFC = work-family/private life conflict; FWC = family/private life-work conflict. Results are based on 1,000 bootstrap samples (BCa CIs are not shown).
The data were summarized using standard descriptive statistics. Exact p-values were presented. Analyses were performed using the Statistical Package for the Social Sciences (version 25) software tool. The variable distributions were inspected for severe normality deviations. Two variables (ICAWS and FWC) were positively skewed. Transformations did not improve the distributions. The results from the initial analyses were approximately the same. Consequently, they were bootstrap-corrected and 95%bias-corrected. Accelerated confidence intervals (BCa CIs) around the means, estimated for 1,000 samples, were given. For both ICAWS and FWC, non-parametric tests (Spearman’s Rho, Kendall’s tau) were performed. The median values of WFC and FWC were reported (Fig. 1) and the values for these variables were compared using the Wilcoxon signed-rank non-parametric test. Using a z-score, the effect size estimate was calculated [35]. The significance tests were subjected to the Bonferroni correction.

Illustration of the distribution of the scores of the two variables, work-family conflict (WFC) and family-work conflict (FWC), for the group of Swedish RNs included in this study (N = 807). (The Swedish versions of the scales use the word “private life” instead of “family”). The figure shows the minimum and maximum values, the medians (the dark lines inside the boxes), the lower quartiles (the bottom lines in the boxes), the upper quartiles (the top lines in the boxes), and the extreme values (outliers) of the FWC.
First, we tested if job demands, work engagement and WFC (but not FWC) are significant predictors of turnover intention. We performed correlations between the investigated variables and two separate hierarchical regressions. One regression analysis examined the extent to which perceived WFC, FWC, job demands and engagement (resource) are linked to the intention to leave the current workplace, while the other one examined how these variables are linked to the intention to leave the nursing profession. The control variables were introduced in step 1, and other variables were used in step 2. For the purpose of generalizing the results to different nurse groups, the model was cross-validated by providing adjusted R2.
Second, moderation analyses were conducted using the PROCESS macro [36] in SPSS-v25, using an ordinary least-squares approach and a bootstrap method (with 5,000 bootstrapped samples) to estimate the conditional (moderated) effects. If moderation was found, we followed the analysis with simple slope analysis. To test our hypotheses, we examined whether the relationship between the intention to leave the nursing profession and the examined variables (quantitative workload, interpersonal conflicts at work, work engagement) is stronger for RNs with high rather than low WFC.
All instruments used in this study were developed in past research and are extensively used. Above we provide references where the reader may find more information regarding the used instruments. Translations have been made from the original languages. Standard procedures were used to maintain the validity of the translated instruments. Briefly, these procedures included translation and reverse translation. A five-stage translation and adaptation process was used to adapt the instruments to Swedish: forward translation by two different bilingual experts, synthesis, reverse translation, revisions, and pilot data samplings, previously reported in several unpublished B.Sc. theses. The psychometric properties of these instruments were good, approximating the original instruments. In addition, the psychometric properties of the instruments used in this study were good (see above).
Results
Descriptive statistics
As predicted, the RNs’ intention to leave the current workplace was positively correlated with their intention to leave the profession. These turnover intentions were correlated positively with both work-family conflict (WFC) and family-work conflict (FWC). WFC was correlated positively with FWC (Table 2). These relationships remained significant after the Bonferroni correction. The effect sizes were minor in accordance with Bosco et al. [37] (except for a weak relationship between turnover intentions and FWC). Table 2 shows that WFC and FWC were related positively to job demands, and negatively to work engagement. The correlation strengths, and therefore the effect sizes, were moderate for WFC and weak for FWC.
We additionally examined the relative strength of WFC and FWC by applying the linked samples’ Wilcoxon signed-rank test. The results showed that the WFC levels were significantly higher (Mdn = 19) than the FWC levels (Mdn = 6), T = 1,043.50, p < 0.001, r = –0.82. The effect size of –0.82 corresponds to a major difference in the levels of these two measures. It is obvious that the average intensity of the experienced WFC was greater than that pertaining to the experienced FWC (Fig. 1).
Turnover intentions
A relatively high percentage of the RNs (36.6%) had a strong intention to leave the current workplace for another, while 21.8%had a strong intention to leave the nursing profession. The mean value for the intention to leave the current workplace was larger than for the intention to leave the nursing profession (Table 2). We compared these values by applying a paired t-test. The difference, 0.59, BCa 95%CI [0.50, 0.68], was significant t (806) = 14.06, p = 0.001.
Factors associated with turnover intentions
A summary of the regression model testing the independent variables as potential antecedents of the RNs’ intentions to leave their current workplace is presented in Table 3. The used control variables had significant impact. The adjusted R2 value of 0.03 was significantly different from zero at the end of the first step, indicating that 3%of the variability in RNs’ intentions to leave their current workplace is predicted together by age, number of children, employed partner; only low age contributed weakly at both steps.
centerline Linear model of antecedents of an intention to leave the present workplace, with 95%bias corrected and accelerated (BCa) confidence intervals (CI) in parentheses, among Swedish nurses (N = 0 807)
centerline Linear model of antecedents of an intention to leave the present workplace, with 95%bias corrected and accelerated (BCa) confidence intervals (CI) in parentheses, among Swedish nurses (N = 0 807)
Note. R2 = 0.03, adjR2 = 0.03 for Step 1 (p < 0.001). ΔR2 = 0.40. AdjR2 = 0.42 for Step 2 (p < 0.001). B =unstandardized coefficient. SE = standard error; β=standardized coefficient; WFC = work-family/private life conflict; FWC = family/private life-work conflict. CIs and SEs are based on 1,000 bootstrap samples.
The adjusted R2 value of 0.42 indicates that almost half of the variability in the RNs’ intentions to leave the current workplace is predicted by the control variables, WFC, FWC, job demands and work engagement. This regression model indicates that a low level of work engagement and a high level of WFC contribute the most to that prediction, while a high level of job demands contributes weakly. Low age contributed very weakly. FWC did not add substantially to the prediction.
We present the regression model of the potential antecedents of the RNs’ intention to leave the nursing profession (Table 4). As it is shown, also in this model, R2 was significantly different from zero at the end of both steps, meaning that the control variables impacted this prediction. In this model, the control variables had a very small impact. The adjusted R2 value of 0.008 indicates that only almost 1%of the variability in the RNs’ intentions to leave the nursing profession is predicted by the control variables; only low age contributed very weakly at the end of the first step.
centerline Linear model of antecedents of an intention to leave the nursing profession, with 95%bias corrected and accelerated (BCa) confidence intervals (CI) in parentheses, among Swedish nurses (N = 0 807)
Note. R2 = 0.01, adjR2 = 0.01 for Step 1 (p = 0.025). ΔR2 = 0.38. AdjR2 = 0.38 for Step 2 (p < 0.001). B =unstandardized coefficient. SE = standard error. β=standardized coefficient. WFC = work-family/private life conflict. FWC = family/private life-work conflict. CIs and SEs are based on 1,000 bootstrap samples.
The adjusted R2 value of 0.38 indicates that over a third of the variability in the RNs’ intentions to leave the nursing profession is explained by the control variables, WFC, FWC, job demands and work engagement. We suggest that a low level of work engagement and a high level of WFC contributed the most to that prediction, while high job demands contributed weakly. High FWC and low age contributed very weakly to the prediction.
The contribution of the control variables to the regression analysis with the intention to leave the nursing profession was non-significant, so we did not use the control variables to test our hypotheses.
Hypothesis 1 could not been confirmed (moderation did not occur), because the relationship between the quantitative workload and the intention to leave the nursing profession was not significantly stronger (p = 0.178) for RNs who experienced high WFC than for those who experienced low WFC.
Hypothesis 2 could be confirmed. The model explained 25%of the variance in the intention to leave the nursing profession (F(3, 803) = 89.66, p < 0.001). There was a significant WFC and interpersonal conflicts at work main effect, and a significant interaction effect, which explained an additional 0.4%of the variance (F(1, 803) = 4.05, p = 0.044). The single slope coefficients were 0.04 (p = 0.155) for low, 0.07 (p < 0.001) for average, and 0.10 for high WFC (p < 0.001), demonstrating that the relationship between interpersonal conflicts at work and the intention to leave the nursing profession was stronger for RNs who experienced high WFC than for those who experienced low WFC (Fig. 2).

Simple slopes equations of the regression of intention to leave the nursing profession on interpersonal conflicts at work at three levels of WFC. With increases in WFC the strength of the shown relationship goes from a very weak positive effect (B = 0.04) to a somewhat stronger (still weak) positive one (B = 0.10)
Hypothesis 3 could be confirmed. The model explained 37%of the variance in the intention to leave the nursing profession (F(3, 803) = 158.62, p < 0.001). There was a significant WFC and work engagement main effect, and a significant interaction effect, which explained an additional 0.43%of the variance (F(1, 803) = 5.49, p = 0.019). The single slope coefficients were –0.41 (p < 0.001) for low, –0.48 (p < 0.001) for average, and –0.56 for high WFC (p < 0.001), demonstrating that the relationship between work engagement and the intention to leave the nursing profession was stronger for RNs who experienced high WFC than for those who experienced low WFC (Fig. 3)
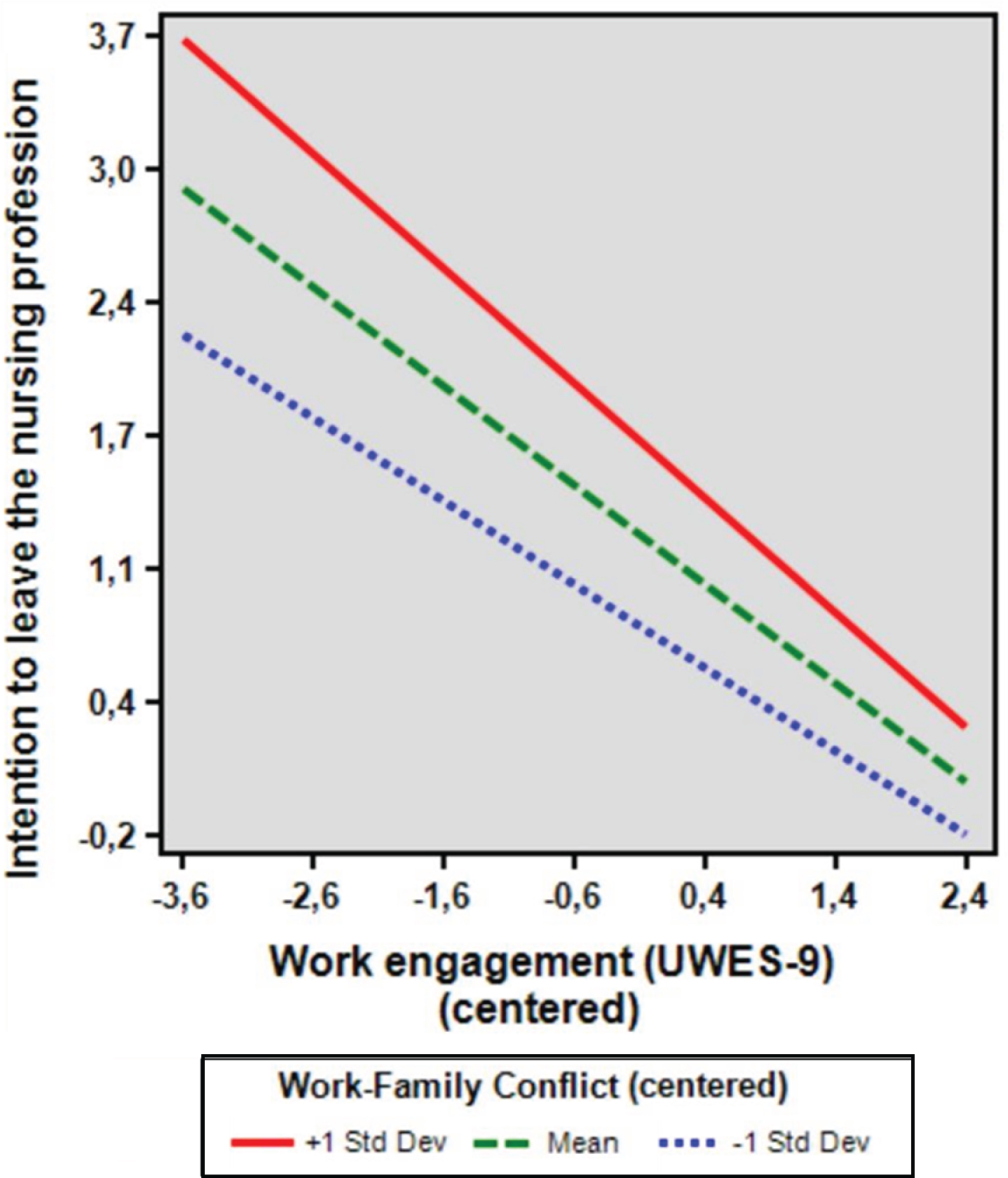
Simple slopes equations of the regression of intention to leave the nursing profession on work engagement at three levels of WFC. With increases in WFC the strength of the shown relationship goes from a weak negative effect (B = 0–0.41) to an almost moderate negative one (B = –0.56).
The working conditions in the healthcare organization have increased RNs’ workload [38–40]. The current study examined the extent to which perceived job demands and work engagement as well as work-family conflict (WFC) and family-work conflict (FWC) are linked to RNs’ turnover intentions in western Sweden. The study showed that work-family conflict was a significant moderator in the relationship between the intentions to leave the nursing profession and work engagement as well as interpersonal conflicts at work. Moreover, low work engagement (work engagement being a personal resource that employees bring to the organization) and high WFC were the most important predictors of turnover intentions, which confirms past research. However, Dåderman and Basinska [29] concluded that, contrary to previous research, WFC does not exacerbate turnover intentions. Their result could be due the fact that Poland, contrary to Sweden, is a country with a post-transformational economic system with different family traditions. Another explanation may be their relatively small sample size in relation to that of this study. In our study, low work engagement (resources) was twice as ‘important’ as WFC, which indicates that the RNs’ resources, i.e. absorption, dedication and vigor, have been reduced; the RNs have given up and feel no particular work engagement (Table 2). The RNs’ reported low levels of energy (i.e. low work engagement).
Almost 37%of the RNs reported a strong intention to leave the current workplace for another in the field of nursing. The relationship between low energy (low work engagement) and high WFC is in line with Hobfoll’s [13] COR theory. This indicates that RNs lack energy, are vulnerable and less capable of gaining resources, and are less successful under pressure. This study showed that RNs often believe that working conditions will be better in a new workplace. For such nurses, turnover is a strategy for winning resources, decreasing stress and increasing work engagement. Over 40%of the responding RNs were specialist nurses, which indicates that the respondent group was well-educated and well-experienced. It should be noted that 22%of the RNs reported a strong intention of leaving the nursing profession. When a RN decides to leave the profession, the healthcare organization loses substantial capital in terms of nursing knowledge and experience [41].
RNs with high WFC experienced high work demands, which indicates low work engagement and low resources. Netemeyer, Boles and McMurrian [12] showed that conflicts between work and family are correlated with job stress, role conflict and burnout. Leineweber, Chungkham, Westerlund, Tishelman and Lindqvist [39] concluded that the leadership at all levels of the healthcare organization should strive to increase RNs’ opportunities to influence their workplace, and ensure that there are sufficient numbers of healthcare personnel in order to promote a positive work environment.
This study found that WFC was experienced more intensely than FWC, which confirms previous research [29]. Possible explanations can be that the average age of the RNs in our study was 42 years and that 60%of the RNs had one child or more living at home. The vast majority of the RNs in our study were female (88.5%) and previous research shows that women often have the greatest responsibility for the family (e.g. taking care of old parents and relatives) and household [11, 30], and that the perception of the female partner’s greater responsibility for household duties is a significant predictor of WFC [42]. This indicates that women often have high levels of stress at home after work. If the workplace has a negative impact on the RN’s private life, an inter-role conflict may emerge [12], and the RN may experience lowered self-esteem and self-confidence.
This study showed that lack of work engagement (a low resource) was four times more ‘important’ than conflicts in the workplace and high workload. Only 8%of RNs in Sweden can work fully in accordance with their profession’s principles and regulations; 31%of Swedish RNs indicate that they can comply with the professional guidelines very little or not at all [43]. Consequently, the nursing profession may be experienced as psychologically demanding. The fact that RNs often cannot provide safe patient care, due to insufficient time and resources, may cause them feelings of dissatisfaction and stress. It appears that recovery during working hours is valuable for the experience of health [44].
This study has also shown that work-family conflict is a significant moderator in the relationship between the intentions to leave the nursing profession, on the one hand, and work engagement and interpersonal conflicts at work, on the other. First, an examination of the interaction plot resulting from testing Hypothesis 2 (see Fig. 2) showed an enhancing positive moderation effect of work-family conflict: as interpersonal conflicts at work increased, the RNs’ intention to leave the nursing profession increased. Second, an examination of the interaction plot resulting from testing Hypothesis 3 (see Fig. 3) showed an enhancing negative moderation effect of work-family conflict: as work engagement increased, the intention of leaving the nursing profession decreased. To balance their work and private lives, RNs can reduce their work engagement in order to preserve their remaining resources and reduce the stress experienced at work. This is in line with the COR theory, which suggests that people’s experience of what constitutes a valuable resource or a perceived threat is influenced by their values [13].
We have shown that family size (number of children at home) or the partner’s employment status were not significantly linked with either WFC or turnover intentions. Only the intention to leave the current workplace was (weakly) predicted by low age (Table 3). This suggest that RNs who do not have many years of practice as nurses may intend to leave the current workplace. This also suggests that RNs who are not comfortable in their current workplace believe that they may feel more comfortable in another, in Sweden or abroad, and therefore choose to remain in the nursing profession. Studies have found that RNs aged from 25 to 49 years are often willing to return to the profession if they were to receive higher wages, greater control over their work situation and a more reasonable workload [43]. Therefore, it is of importance to achieve balance between work demands and resources in order to manage and prevent stress in the workplace and to increase work engagement.
Practical implications
Considering the need to reduce RNs’ intentions of leaving the nursing profession, and the fact that WFC intensifies the relationship between RNs’ intention to leave the profession, their level of work engagement (absorption, dedication and vigor), and their feelings of stress and interpersonal conflicts at work, it would be valuable to develop WFC-reducing strategies.
The basis for such WFC-reducing strategies could be that managers should promote a creative and positive working climate by:
Strategy 1: Social support
Listening to the RNs’ questions and concerns in order to understand their resources, knowledge and work situation
Strategy 2: Practical support
Conducting regular dialog with the RNs in order to sort and prioritize their tasks and to develop strategies enhancing their personal resources Organizing regular interprofessional meetings for constructive and reflective discussions about the working conditions Providing the RNs with opportunities for skills and career development
These WFC-reducing strategies may allow RNs to strengthen their confidence in terms of their ability to practice the profession in a safe and satisfactory manner with decreased stress.
Strengths and limitations
One strength of this study is the large sample size, which is sufficiently large to allow us to draw more general conclusions from our results. Another strength is the relatively high response rate to our questionnaire.
When several contemporary scales are being used, a commonly-stated, almost automatic, concern is about common-method variance. This common-method variance concern states that correlations between variables measured using the same method (e.g. with self-reports), as was the case in the current study, may be inflated due to the ‘action’ of common-method variance. Some researchers [45] have shown that a more complex view of method variance exists when using multiple sources of data. Thus, if we could use more objective physiological measures of job demands, for example stress in the form of hormone levels and cardiovascular responses, and if we could use other resources to measure work engagement (and other relevant variables) in the form of co-worker or family member assessments, and then were to examine the associations of such measures with turnover intentions, we would be concerned by other sources of bias.
One limitation of this study may be that the study includes the use of a purposive convenience sample with all of the RNs being recruited in western Sweden. However, we know that the work situation of RNs is difficult all over the country, and that this region has similar resources and population as the rest of the country [43]. Another limitation may be that the RNs were not asked whether their children had already left home. If a RN has children who have left home, the RN may be expected to take part in their lives in different ways, which may increase the RN’s perceived WFC. Further limitations may be that we did not assess possible marital conflicts and did not obtain information about the RNs’ living arrangements, which may considerably affect a RN’s WFC. Lastly, the cross-sectional design of our study is an overall limitation. This design does not make it possible to identify causal directions of the relationship between the intention to leave the nursing profession and job demands and work engagement.
This study complements the existing literature by identifying important factors influencing RNs’ turnover intentions.
Conclusion
Low work engagement (absorption, dedication and vigor) and high work-family conflict (WFC) and job demands predict turnover intentions among registered nurses (RN). A high percentage of the RNs in our study were well-educated and well-experienced and declared strong turnover intentions. This is a major problem that needs to be taken seriously by decision-makers. Our study shows that low work engagement was the most important predictor of turnover intentions, and that WFC intensifies the relationship between RNs’ intention to leave the nursing profession and their work engagement. To motivate RNs to stay and be more engaged, and to reduce their experience of stress, managers should promote a positive working climate. This can be achieved by actively listening to RNs’ opinions and questions and by providing them with opportunities to develop their skills in a context of interprofessional cooperation. By so doing, managers can gain better understanding of RNs’ resources, knowledge and work situation, thus strengthening RNs’ confidence and ability to practice their profession in a safe and satisfactory manner.
Footnotes
Acknowledgments
We thank the participants for volunteering their time to complete the questionnaire required for the study, Lisa Dahlström for designing the initial version of the web questionnaire, Johan Linder for producing the mailing list used for distributing the questionnaires to nurses, Åke Hellström for providing valuable comments on the data and statistical analyses, and Patrick Reis for proofreading our manuscript.
Author contributions
Both authors (SP, AD) have made substantial contributions to conception and design, acquisition of data, analysis and interpretation of data; drafted the manuscript and revised it critically for important intellectual content.
Conflict of interest
The authors declare no conflicts of interest.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.