
Abstract
BACKGROUND:
with the increase of study and life pressure, the number of depressed college students showed an increasing trend year by year, and the drug treatment alone could not achieve a comprehensive recovery of depression patients, so it was more necessary to pay attention to the spiritual treatment.
OBJECTIVE:
this research aimed to better understand the relationship between college students’ depression and life events, social support, psychological pressure, and coping style, and the influence of systematic family therapy on depression degree, psychological stress, and social adaptability of college students with depression.
METHODS:
in this study, 105 college students with depression were selected as the research object, and healthy college students were taken as the control group. Through questionnaire, the differences in life events, social support, psychological stress, and coping styles between the groups were compared. The correlation between the degree of depression and various variables were analyzed, and the impact path of each variable on depression was analyzed using the path analysis model. Depression patients were then divided into a conventional group treating with conventional medications and an observation group treating with systematic family interventions. Differences in Hamilton Depression Scale-17, (HAMD-17), CPSS, and Social Adaptive Functioning Evaluation (SAFE) scores were compared and analyzed between the two groups before treatment (T1), during the treatment (T2), and after treatment(T3).
RESULTS:
there were significant differences in scores of life events, social support, psychological stress, and coping styles between the healthy control group and the depressed patients (P < 0.05). There was an obvious correlation between different depression degrees and life events, social support, psychological stress, and coping styles (P < 0.05). Life events, social support, and psychological stress had a direct and significant impact on depression (0.250, 0.218, and 0.392; P < 0.05), and they also had an indirect and significant impact on depression through coping styles (P < 0.05). The systematic family treatment model could significantly reduce HAMD-17 and CPSS scores (P < 0.05), and significantly improve SAFE scores (P < 0.05).
CONCLUSIONS:
adverse life events, lack of social support, excessive psychological stress, and negative coping styles can aggravate college students’ depression. Systematic family therapy can improve the degree of depression, reduce the psychological stress, and enhance the social adaptability of college students with depression.
Keywords
Introduction
Depression is one of the typical psychological disorders, which has the highest incidence among many mental disorders, and some studies have shown that the incidence of depression in women after the age of 18 is as high as 20%[1]. Depression is not a simple feeling of “bad mood” or “low mood”. Patients suffering from depression often experience the despair and boredom of life, as well as the loss of interest and fun in surrounding food, as well as a variety of physical symptoms [2]. If depression patients do not accept timely psychological intervention treatment, the patient may fall into a state of mania, or even despair, and it will affect the daily life of patients and lead to the tendency of suicide when serious. Numerous studies have shown that psychological stress, coping style, life events, and social support are closely related to depression [3–5]. The pressure of college students mainly comes from life, study, employment, and other pressures. In the existing research, interviews and questionnaires are often used to test psychological pressure [6]. At present, there is no specific definition of coping style, which mainly exists in the field of consciousness. Studies have shown that coping styles play an important role in the occurrence and development of certain diseases, for example, positive coping styles have a negative correlation with individual abnormal behavior disorders and diseases that harm health [7, 8]. Adverse life events have a great impact on the healthy growth of individuals, especially on the occurrence and development of psychological diseases [9]. Social support is mainly defined as financial, emotional, or psychological support from other groups, mainly from social groups such as family, friends, and colleagues. In the face of fierce social competition and great pressure, the lack of adequate social support will have a serious impact on individuals, thus increasing the risk of depression [10]. Therefore, it is of great significance to explore the influencing mechanism of depression for us to understand the course of depression and to propose appropriate treatment schemes.
Some studies have shown that the lack of family functions may be one of the factors causing the occurrence and development of depression [11]. Poor family environment will aggravate the degree of depression patients, and then cause the deterioration of family environment, and finally form a vicious circle [12]. The systematic family therapy model is based on the system theory and adopts the family as a whole to conduct psychological treatment. This treatment model can cause some adaptive changes in the families of patients with depression, and ultimately alleviate or eliminate the symptoms of patients with depression and their family members [13, 14]. This kind of treatment mode is helpful to break the vicious circle between the family adverse factors and the degree of depression, thus improving the mental state of depression patients, so it is often used in the clinical treatment of mental diseases in recent years. However, there is still relatively little research on the systematic treatment of depression in the current systematic family treatment model.
College students, as the frontier groups of new technologies and new ideas in society, are the pillars of social progress. Exploring the influence path of college students’ depression is of great significance to understand and care about college students and promote their upward mobility. In addition, the systematic family therapy model has achieved remarkable results in the treatment of mental illness, but there are relatively few studies on the systemic treatment of depression in college students. Therefore, the depression patients and healthy people were taken as research objects, and the differences between psychological stress, coping styles, life events, and social support, as well as their correlation with depression degree were compared and analyzed. Then a path analysis model was constructed to analyze the impact of psychological stress, coping style, life events, and social support on depression. Finally, the effects of conventional drug therapy and systematic family therapy on the degree of depression, psychological stress, and social adaptability of depressed patients were compared and analyzed. The results aimed to lay a foundation for understanding the pathogenesis of depression and the application of systematic family therapy in the treatment of depression.
Methodology
Research subjects
105 college students with depression who were admitted to the inpatient department and outpatient department of Hefei psychiatric hospital from December 2017 to December 2019 were selected as the study subjects. There were 47 males and 58 females aged 18 to 25 years old, with an average age of 21.33±2.48 years. Inclusion criteria: patients meeting the diagnostic criteria of Classification of diseases 10 (ICD-10) depressive episode; the score of Hamilton Depression Scale-17 (HAMD-17) was 17 or above; college students aged 18 or above; the subjects and their guardians have fully understood the content of this study and wished to participate in and complete this study and signed the informed consent. Exclusion criteria: persons with other psychiatric disorders; those who have received electroconvulsive therapy; patients with a history of alcohol or drug dependence; patients with previous craniocerebral injury or loss of consciousness for more than 1 hour; those who were suffering from infection, immunity, or other endocrine diseases; patients with previous epileptic seizures or family history; patients with previous history of mania, bipolar disorder, or recurrent or transient depression.
Healthy adolescents were selected as the healthy control group according to the principles of age, gender, education, and family background. The control group was scored according to the HAMD-17 scale, and the score should be 7 or less. Finally, 105 healthy adolescents were selected as the control group, including 48 males and 57 females, aged from 18 to 26 years old, with an average age of 22.08±2.59 years old. The depressed patients and healthy people finally included in the study were informed of the purpose and significance of the study before the trial began, and the subjects and their guardians have agreed the trial, which met the ethical standards.
Assessment tools
The control group and observation group were investigated by questionnaires. All subjects were accompanied by guardians to fill in the questionnaires. In the observation group, patients who could not complete the form at one time due to their illness could be treated separately. Finally, 103 valid questionnaires were collected from the observation group and 105 questionnaires were from the control group.
A general scale was used to investigate the general information of the subjects, including basic demographic data such as the subjects’ age, gender, educational level, family history, household registration, and family structure, as well as their height, weight, and cognition. The weight perception survey was: what body type do you think you are? The answer was: very thin, thin, normal, fat, very fat. According to the actual body mass index (BMI) of the subjects, the subjects’ weight perception can be divided into left shift (normal or high BMI, but the subjects thought they were thin or very thin; High BMI, but subjects considered themselves normal), right shift (normal BMI, but subjects considered themselves fat or very fat; BMI was low or normal, but subjects considered themselves normal, fat, or very fat), and accurate (BMI was basically the same as cognition).
The HAMD-17 scale [15] was adopted to investigate the degree of depression. The scale contained a total of 17 items, namely depression (1), guilt (2), suicide (3), difficulty falling asleep (4), poor sleep (5), early awakening (6), work and Interest (7), retardation (8), agitation (9), mental anxiety (10), physical anxiety (11), gastrointestinal symptoms (12), systemic symptoms (13), sexual symptoms (14), hypochondria (15), weight loss (16), and self-control (17). Items 1, 2, 3, 7, 8, 9, 10, 11, 14, and 15 in the scale were assessed by the five-level scoring method, which was divided into normal (0), mild (1), moderate (2), severe (3), and extremely severe (4). Other items were assessed using the three-level scoring method, which included normal (0), mild to moderate (1), and severe (2). A total score greater than 24 was considered severe and very severe depression, a total score greater than 17 and less than 24 was considered mild and moderate depression, and a total score less than 7 was considered normal.
The adolescent self-rating life events checklist (ASCLE) scale [16] was used to assess the physical and psychological characteristics and social roles of the subjects. The scale was used to assess the frequency and intensity of stressful life events. The scale contains 27 items, as well as 6 factors including interpersonal relationship, learning pressure, punishment, loss, health adjustment, and other factors. The assessment was carried out by the 5-level scoring method, which was divided into no influence (1 point), mild (2 points), moderate (3 points), severe (4 points), and extremely severe (5 points).
The social support scale [17] was used to evaluate the social support degree of the subjects and the utilization degree of their own social support. It included three dimensions: subjective social support, objective social support, and utilization of social support. The scale contained a total of 17 items, which were evaluated by the five-level scoring method, including non-conformity (1 point), relatively non-conformity (2 points), uncertainty (3 points), relatively conformity (4 points), and conformance (5 points).
Chinese perceived stress scale (CPSS) [18] was used to evaluate the psychological stress status of the subjects. The scale consisted of 14 items. The five-level scoring method was used for evaluation, with no (1), rarely (2), occasionally (3), often (4), and many (5).
Coping style questionnaire (CSQ) questionnaire [19] was used to investigate the coping style of subjects. The scale contained 62 items, and was divided into 6 scales of problem solving, self-accusation, seeking help, fantasy, retreat, and rational analysis. There were only two answers for all items on the scale: “yes” and “no”.
Social Adaptive Functioning Evaluation (SAFE) [20] was adopted to evaluate the subjects’ social adaptability. The SAFE contained 20 items in total, and the 3-level scoring method was used for evaluation: poor (1 point), moderate (2 points), and good (3 points).
Systematic family therapy program and efficacy evaluation
Subsequently, patients with depression were randomly divided into the conventional group and the observation group. All patients with depression were given the conventional drug treatment of 25 mg/d sertraline hydrochloride tablets, which were taken after breakfast. According to the patient’s condition, the dosage of sertraline hydrochloride tablets can be adjusted to 50∼200 mg/d for 2 months of continuous treatment.
In the observation group, systematic family therapy theory and method were used to intervene on the basis of drug therapy. First, patients and their families were given psychological treatment. The specific treatment steps were as follows. I. The psychological status of the patients and their families was assessed through 2 h interview, and the relationship was established, hypotheses were proposed, and the relationship interaction pattern, family resilience, family capacity, stressors and symptoms were comprehensively evaluated. II. In the in-depth stage of treatment, the patient and his family members can express their feelings of conflict more freely through the forms of feedback, systematic questioning, multilateral alliance, and homework. III. At the end of treatment, the effect of treatment needed to be assessed through the family. In the treatment process, the therapist should record the process and method of each treatment by video and communicate with peers or supervisors in time. Interviews were conducted every 14d for 1.5 hours each time, and a total of 5 interviews were conducted for 2.5 months.
The HAMD-17 scale, CPSS scale, and SAFE scale were used adopted to evaluate the depression degree, psychological pressure, and social adaptability of college students with depression 1 week before treatment, 1 month after treatment, and 3 months after treatment.
Statistical analysis
SPSS19.0 software was used to collate and analyze the acquired data. Continuous variables were compared using independent-sample t test, and dichotomous variables were compared using χ2 test. The correlation analysis was to test the correlations among variables such as life events, social support, psychological pressure, and depression. The linear regression analysis and path analysis were to explore the impact path of depression. When P < 0.05, there were statistically significant differences.
Results
Analysis of general demographic characteristics
Differences in gender, age, origin, family structure, family history, and weight perception were compared between healthy control group and depressed patients. As shown in Table 1, there were no statistically significant differences in gender, age, and source between the two groups (P > 0.05). The proportion of single parent families, single child, positive family history of disease, and right shift of weight cognition in depression patients were significantly higher than those in healthy control group, and the differences were statistically significant (P < 0.05). The accuracy of weight perception and the proportion of left shift in depression patients were significantly lower than those in the healthy control group, and the difference was statistically significant (P < 0.05).
General demographic characteristics of depressed patients and healthy controls
General demographic characteristics of depressed patients and healthy controls
The differences in dimensions and total scores in the ASCLE scale between the healthy control group and the depressed patients were compared. As shown in Fig. 1, the dimensions of A, B, C, D, E, and F and the total score of patients with depression were significantly higher than those of healthy controls, and the differences were statistically significant (P < 0.05).

ASCLE scores of depressed patients and healthy controls. Note: A represented learning pressure; B was for interpersonal relationship; C was for punishment; D was for loss; E was for healthy adaptation; F was for the others; * indicated that the difference between the two groups was statistically significant, P < 0.05.
The scores differences of the social support scale between healthy controls and depressed patients were compared. As shown in Fig. 2, the dimensions (1), (2), and (3) and the total score of depression patients were significantly lower than those of the healthy control group, and the differences were statistically significant (P < 0.05).

Scores on the social support scale for depressed patients and healthy controls. Note:(1) objective support; (2) subjective support; (3) the degree of support utilization; * indicated that the difference between the two groups was statistically significant, P < 0.05.
The differences in CPSS scale scores between healthy controls and depressed patients were compared. As shown in Fig. 3, the CPSS score of depression patients was significantly higher than that of the healthy control group, and the difference was statistically significant (P < 0.05).
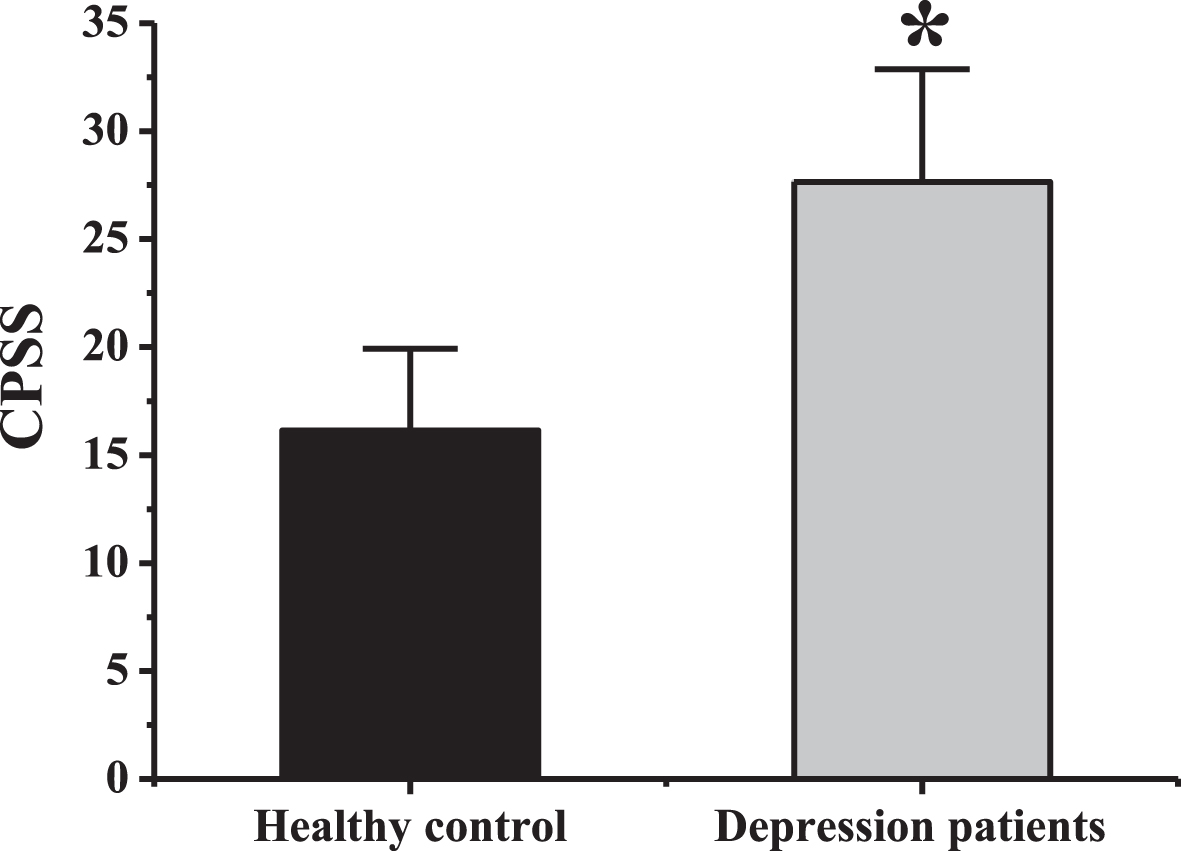
CPSS scale scores of depressed patients and healthy controls. Note: * indicated that the difference between the two groups was statistically significant, P < 0.05.
The differences of CSQ scale scores between the healthy control group and the depressed patients were compared. According to Fig. 4, C1 and C3 dimensions and total scores of depression patients were significantly lower than those of the healthy control group, and the differences were statistically significant (P < 0.05). The C2 and C5 scores of depression patients were significantly higher than those of the healthy control group, and the differences were statistically significant (P < 0.05).
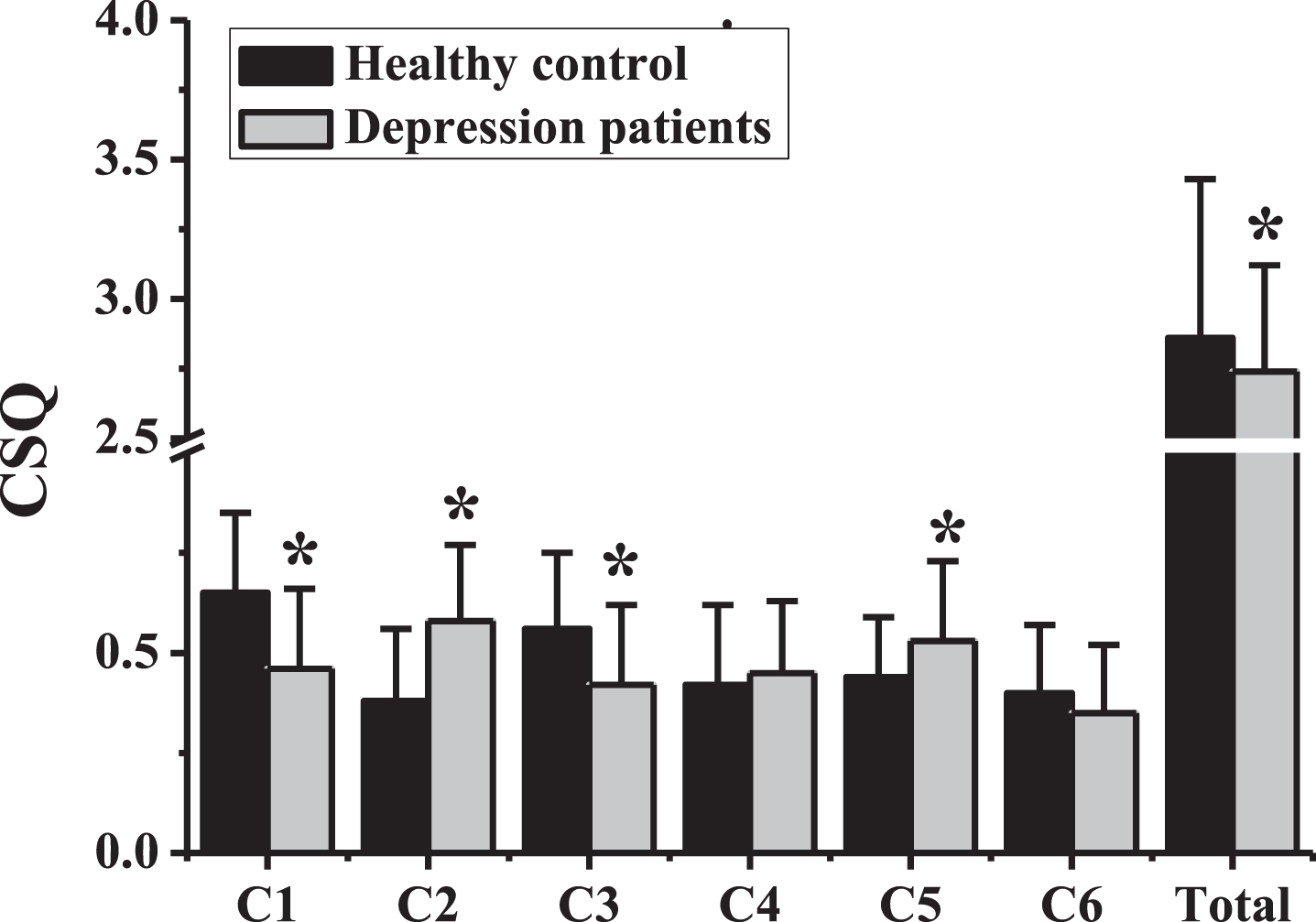
Results of CSQ scale in depressed patients and healthy control group. Note: C1 represented problem solving; C2 was remorse; C3 was for help; C4 was for fantasy; C5 meant retreat; C6 was for rationalization; * indicated that the difference between the two groups was statistically significant, P < 0.05.
The correlation between different levels of depression and life events was analyzed. According to Table 2, it can be found that non-depression, mild/moderate depression, and severe/extremely severe depression all had significant positive correlation with all dimensions of life events (learning pressure, interpersonal relationship, punishment, loss, and health adjustment) (P < 0.01).
The correlation between depression levels and life events
The correlation between depression levels and life events
Note: ** indicated P < 0.01.
The correlation between different levels of depression and social support was compared. According to Table 3, it can be found that non-depression, mild/moderate depression, and severe/extremely severe depression all had significant negative correlation with each dimension of social support (objective support, subjective support and support utilization) (P < 0.05).
The correlation between depression level and social support
Note: *indicated P < 0.05; **indicated P < 0.01.
The correlation between different levels of depression and psychological stress was compared. According to Table 4, non-depression, mild/moderate depression, severe/severe depression all had significant positive correlation with psychological stress (P < 0.01).
The correlation between depression level and social support
Note: **indicated P < 0.01.
The correlation between different levels of depression and social support was compared. As shown in Table 5, no depression, mild/moderate depression, severe/severe depression were negatively correlated with problem solving and help seeking (P < 0.01). There was a significant positive correlation with self-accusation, fantasy, retreat, and rationalization (P < 0.01).
The correlation between depression level and social support
Note: *indicated P < 0.05; **indicated P < 0.01.
According to the results in Fig. 4, there were statistically significant differences between the healthy control group and the depressed patients in solving problems, self-reproach, seeking help and retreat (P < 0.05). Therefore, these four dimensions were selected for the correlation analysis of life events, social support, and psychological pressure, as shown in Table 6. There was no significant correlation between life events and problem solving, self-reproach, help seeking and retreat (P > 0.05). Social support was positively correlated with problem solving and assistance (P < 0.01), and negatively correlated with self-accusation and withdrawal (P < 0.05). Psychological stress was negatively correlated with problem solving and seeking help (P < 0.01), and positively correlated with self-accusation and withdrawal (P < 0.01).
Relationship between coping style and life events, social support, and psychological stress in depressed patients
Relationship between coping style and life events, social support, and psychological stress in depressed patients
Note: *indicated P < 0.05; **indicated P < 0.01.
In order to explore the factors that cause college students’ depression, the demographic variables, life events, social support, psychological pressure and coping style were taken as independent variables, and depression score as dependent variables to analyze the influencing factors of college students’ depression. In order to simplify the analysis process, this study classified the coping style of “solving problems, seeking help, and rationalizing” as “positive coping style” and the coping style of “self-accusation, fantasy, and retreat” as “negative coping style” for subsequent analysis. As shown in Table 7, single parent families, only child, life events, social support, psychological pressure, positive coping style, and negative coping style were included in the regression equation and tested, and the determination coefficient was found to be statistically significant (P < 0.05). According to the β value, social support and positive coping style had significant negative predictive effects on college students’ depression (P < 0.01), while single parent families, only child, life events, psychological pressure, and positive coping style had significant positive predictive effects on college students’ depression (P < 0.05). The predicted variation of single parent families, only child, life events, social support, psychological pressure, positive coping style, negative coping style of depression was 28.8%, 26.4%, 47.0%, 60.9%, 65.2%, 52.9%, and 59.8%, respectively.
Regression analysis of depression affecting factors
Regression analysis of depression affecting factors
In order to further explore the influence mechanism of social psychological factors on college students’ depression, based on the above results, the following hypotheses were proposed. a. Life events have an impact on depression; a1. Life events influence depression through positive coping styles; a2. Life events affect depression through negative coping. b. Social support affects depression; b1. Social support influences depression through positive coping; b2. Social support affects depression through negative coping. c. Psychological stress has an effect on depression; c1. Psychological stress affects depression through positive coping; c2. Psychological stress affects depression through negative coping. The corresponding impact path was built, and the results were shown in Fig. 5.
The basic structure of the influence pathway of depression.
Subsequently, the life events, social support, and psychological pressure were taken as independent variables to conduct regression analysis with positive coping style and negative coping style as dependent variables. It can be found from Table 8 that life events and psychological pressure had an obvious negative predictive effect on the positive coping style of college students with depression (P < 0.05), while social support had an obvious positive predictive effect on the positive coping style of college students with depression (P < 0.05). However, life events and psychological pressure had obvious positive predictive effects on the negative coping style of college students with depression (P < 0.05), while social support had obvious negative predictive effects on the negative coping style of college students with depression (P < 0.05).
Regression analysis of influencing factors of depression coping style
Note: ** indicated P < 0.01.
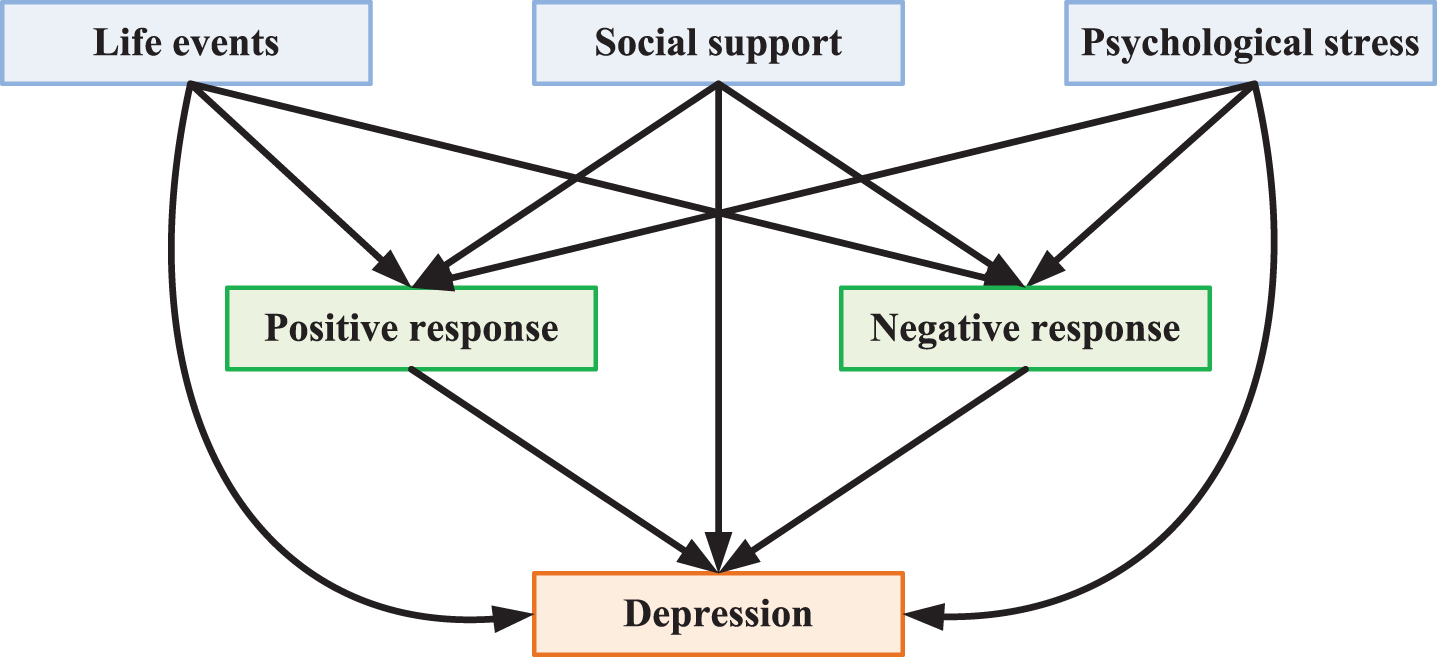
The impact path structure of depression can be changed to Fig. 6. Life events, social support, and psychological stress all led to the occurrence of depression. Moreover, life events, social support, and psychological stress can affect depression through positive coping style and negative coping style, indicating that all the hypotheses presented in this study were valid.

Complete structure of the influence pathway of depression.
Differences in HAMD-17, CPSS, and SAFE scores were compared between patients in the conventional group and the observation group 1 week before treatment (T1), 1 month after treatment (T2), and 3 months after treatment (T3). The results were shown in Fig. 7A, 7B, and 7C. There was no significant difference in HAMD-17 score, CPSS score, and SAEF score between the conventional group and the observation group at time T1 (P > 0.05). With the passage of treatment time, HAMD-17 score and CPSS score of the two groups showed a trend of gradually decreasing. HAMD-17 score and CPSS score at T2 and T3 were significantly lower than that at T1, and the difference was statistically significant (P < 0.05). Moreover, the HAMD-17 score and CPSS score at T3 were significantly lower than those at T2, and the difference was statistically significant (P < 0.05). The HAMD-17 score and CPSS score of the observation group at T2 and T3 were significantly lower than those of the conventional group, and the differences were statistically significant (P < 0.05).
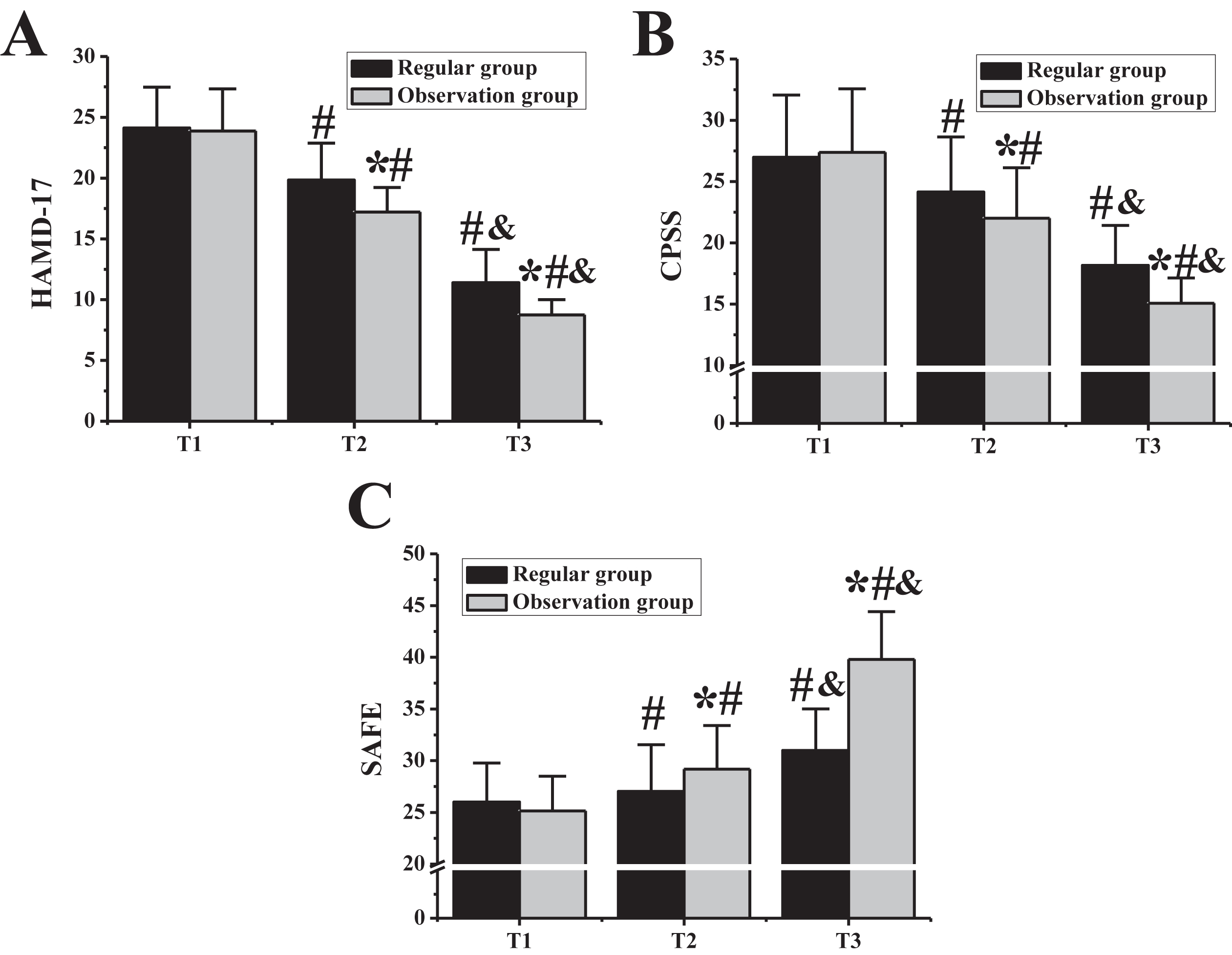
Comparison of treatment effect of depression in different treatment stages. Note: figure A was the HAMD-17 score; Figure B showed the CPSS score results. Figure C showed the SAEF score. * indicated that the difference was statistically significant compared with the conventional group, P < 0.05; # indicated that compared with T1, the difference was statistically significant. P < 0.05; & meant that the difference was statistically significant compared with that at T2, P < 0.05.
With the passage of the treatment time, SAEF scores of the two groups showed a trend of gradually decreasing. SAEF scores at T2 and T3 were significantly lower than those at T1, and the difference was statistically significant (P < 0.05). Moreover, the SAEF score at T3 was significantly lower than that at T2, and the difference was statistically significant (P < 0.05). The SAEF scores of patients in the observation group at T2 and T3 were significantly lower than those in the conventional group, and the differences were statistically significant (P < 0.05).
The results of baseline data show that the proportion of single-parent families, only child, positive family history of disease, and right shift of weight cognition among college students with depression were significantly higher than those of healthy people (P < 0.05). This may be because the lack of family care in daily life is more likely to produce loneliness, which in turn leads to an increase in the probability of depression. Such results were consistent with the research findings by Liang [21]. In addition, depression may have the possibility of heredity, which is basically consistent with the results of Magliano et al. [22]. However, patients with depression often think that they are fat and are prone to use extreme methods such as dieting to lose weight, which is in line with the behavioral characteristics of patients with depression [23]. The results showed that the scores of coping style, life events, social support, and psychological stress of college students with depression were different from those of the healthy control group, and the differences between the two groups were statistically significant (P < 0.05). In terms of coping style, college students suffering from depression mostly adopt negative coping methods such as self-accusation and retreat, rather than positive coping methods such as problem solving and seeking help, which was consistent with the research results of Abdollahi et al. [24]. In addition, the study of Chen et al. showed that negative coping style was correlated with depression and stress, and that negative coping style can not only help individuals solve problems, but also can increase negative emotions in the face of stress and stress [25]. Positive coping style can effectively protect college students from severe and severe depression, which also indicated that college students with depression extremely lacked of positive coping strategies, while negative coping style often existed. College students with depression had more adverse events in life, and their scores in interpersonal relationship, learning and health were all lower than those in the healthy control group, which was consistent with the study results of Meltzer-Brody et al. [26]. Research by Daches et al. showed that about 30%of adolescents suffer from depression, and these depression patients had conflict with others and were mostly in single parent families [27]. Such results consistent with the findings of this study that the proportion of single parent families in patients with depression was significantly higher than that in healthy control group. It was found that the scores of subjective support, objective support and social support utilization of depressed patients were significantly lower than those of the healthy control group, which was consistent with the findings of Uchino et al. that lack of social support was a predictor of adolescent depression [28], suggesting that people with depression lacked the help of the surrounding community and were unable to effectively use the resources of social support to increase their ability to cope with stressful events. In addition, it also reflected that college students with depression were not able to integrate well into the surrounding groups, so they often put themselves in a solitary interpersonal relationship.
Subsequently, it was found that psychological stress had an obvious correlation with depression in different degrees, which indicated that college students had a close relationship with depression and psychological stress they felt [29]. Social support and positive coping style significantly negatively predicted college students’ depression (P < 0.01), while single parent families, only child, life events, psychological pressure and positive coping style significantly positively predicted college students’ depression (P < 0.05). The predicted variation of single parent families, only child, life events, social support, psychological pressure, positive coping style, and negative coping style of depression was 28.8%, 26.4%, 47.0%, 60.9%, 65.2%, 52.9%, and 59.8%, respectively, suggesting that the model can effectively predict college students’ depression in terms of adverse life events, social support, psychological pressure, positive coping style, and negative coping style; in addition, it showed that reducing the occurrence of adverse life events in college students’ life and giving more encouragement and help can help depression patients alleviate their symptoms [30, 31]. The analysis results of college students’ influence path showed that life events, social support, and psychological stress had indirect influence on depression through positive coping style and negative coping style, and also had direct influence on depression. suggesting that in the face of stress or conflict, individuals who often adopted positive coping methods, such as problem solving and seeking help, suffered from less severe depression, and escape from reality through negative coping methods would cause greater destruction. Therefore, the best way to improve depression was to strengthen college students’ grasp and use of positive coping methods, analyze problems objectively, adjust their mentality in time, and find appropriate ways to solve problems.
Systematic family therapy model is a method to improve the family environment and personnel relationship by improving the patients and their families. Based on this mode of treatment, some adaptive changes can be made in the families of patients with depression, and the existing conditions of family members can be alleviated or eliminated. The family therapy model did not deny the individual’s depressive symptoms, but treated them through a broader therapeutic horizon. In this study, the family therapy model was adopted for the intervention treatment of college students with depression. It was found that compared with drug treatment, HAMD, CPSS, and SAFE scores could be effectively improved, indicating that this treatment can effectively improve the depression degree of patients with depression, reduce their psychological pressure, and improve their social adaptability.
Conclusion
The influence mechanism of life events, social support, psychological pressure, and coping style on college students’ depression was analyzed, and the influence of family treatment mode on depression degree, psychological pressure, and social adaptability of college students with depression was explored. The results were as follows. There was a significant correlation between college students’ depression degree and life events, social support, psychological pressure, and coping style. College students with depression mostly adopted negative coping style, and life events, social support, psychological pressure, positive coping style and negative coping style had significant predictive effects on college students with depression. Life events, social support, and psychological stress can have a direct impact on depression, as well as an indirect impact on depression through positive and negative coping styles. Systematic family therapy can effectively improve the degree of depression, reduce the psychological stress, and enhance the social adaptability of college students with depression.
In the study, the influence mechanism of life events, social support, psychological stress, and coping style on college students’ depression was analyzed, as well as the therapeutic effect of family therapy model. It did not explore the mechanisms by which family treatment patterns affected people with depression. Further research is needed to explore the molecular mechanisms of intervention in patients with depression. In a word, the results can provide reference for the intervention treatment of college students with depression and improve the treatment effect.
Footnotes
Acknowledgments
The authors acknowledge the Anhui Province philosophy and social science planning project, “The Practical and Innovative Research of improving the quality of individualized education for local university teachers” (Grant: AHSKY2016D33).
Conflict of interest
None to report.