
Abstract
BACKGROUND:
Welding is one of the most hazardous professions across the globe. Several risk factors are associated with Indian unorganized welding units such as welding gases, fumes and dust particles resulting in various respiratory health problems.
OBJECTIVE:
The objective of the present study is to examine the prevalence of respiratory symptoms, their associated factors and lung function impairment amongst the welders of the unorganized sector in India.
METHODS:
A cross-sectional study was conducted across 283 welders of age group 18–55 years from Punjab, India who responded to the interviewer-administrated respiratory symptoms questionnaire. Also, the lung function parameters of 50 male welders (exposed group) and 50 male non-welders (control group) working in the same environment were evaluated.
RESULTS:
The prevalence of respiratory symptoms such as chronic cough (38.86%), phlegm (38.86%), shortness of breath (33.56%), wheezing (32.15%), chest tightness (36.40%,) and sputum (34.27%) was reported by the welders. The observed mean values of forced vital capacity (FVC), forced expiratory volume in 1s (FEV1) and FEV1/FVC ratio of welders were (3.37±0.175), (2.59±0.16) and (76.63±6.16) respectively and that of non-welders were (3.70±0.15), (3.05±0.25) and (82.49±7.62) respectively.
CONCLUSIONS:
The welders were found to be at significant risk of developing pulmonary diseases. Long working hours, low level of education, hazardous working conditions, lack of implementation of safety laws make welders more vulnerable to health risks. The welders of Indian unorganized sector work without any technical training related to welding and safety. Proper orientation sessions about the workplace hazards and to maintain hygiene at their workplace should be organized. Welders must be provided with Personal Protective Equipment (PPE). Welders should take proper health check-up and medication to sustain healthiness
Introduction
Welding is one of the most extensively used metal fabrication methods. Even though the welding is carried out all across the globe, the exposure to this profession adversely affects the health of welders [1]. The functioning of various body organs and physiological systems is badly affected [2] and it also causes poor respiratory health [3], musculoskeletal disorders [4], ocular injuries [5], cuts and burns [6]. Approximately one million people perform welding as a part of their duties [7]. When welding is performed, metal vaporizes and combines the air to produce toxic fumes [8]. Welders come in contact with poisonous metal fumes, depending upon process and material consisted of a combination of metals such as copper, nickel, cobalt, platinum, chromium, zinc and their oxides that leads to numerous respiratory ailments and metal fume fever [9–14]. Fumes, gases and particulate matter affect the respiratory system and lead to significant occupational hazards to the welders. The respiratory system is not only for breathing but it also transports oxygen to the different parts of body. The different parts of respiratory system are represented in Fig. 1. The main parts of this system are nose, trachea, alveoli and respiratory bronchiole.
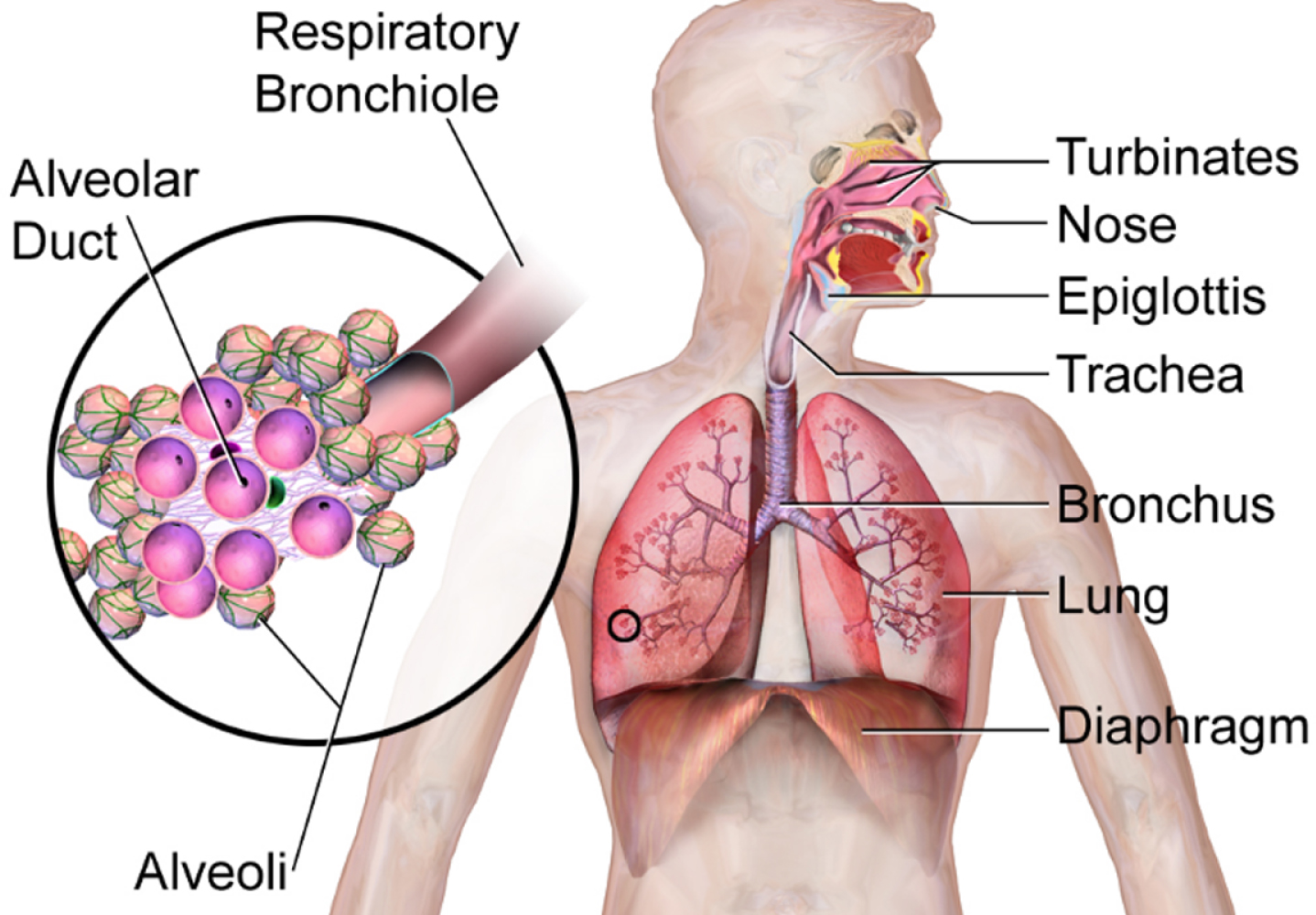
Respiratory System of Human Being (Source: https://commons.wikimedia.org/wiki/File:Respiratory_System_(Illustration).png).
Welding emissions contain Solid Particulate Matter (SPM) combined with soot particles enter into the lungs that increase the risk of pneumoconiosis and lung cancer [15]. Lack of use of Personal Protective Equipment (PPE) can cause exposure of the human body to spark, light, hot metal whereas chemicals can cause respiratory problems, ocular injuries, skin diseases, cuts and burns.
Around 80 different kinds of welding and associated processes in commercial use have been identified by The American Welding Society [16]. Different types of welding hazards were found to be associated with welding processes and the major categories of hazards identified were chemical, physical and radiations [7].
The welding workers suffer from various respiratory diseases such as a chronic cough, pneumoconiosis, lung cancer, asthma and Chronic Obstructive Pulmonary Diseases (COPD) [7, 18]. A chronic cough is defined as a regular phlegm production at any time during the day or night for at least three months of the year and at least two years. A chronic cough, chest tightness, wheezing or shortness of breath are named as work-related symptoms and become worse during working time and get improved during non-working days [19].
A massive amount of population is involved in different types of occupations in an unorganized sector. In India nearly 90%of overall population is directly involved in unorganized sector with different jobs which includes 60%self-employed and 30%without regular jobs [20, 21]. A big chunk of the Indian workforce is working in the unorganized sector. The First Indian National Commission on Labour (1966-69) provides the following definitions to distinguish between workers of unorganized sector and organized sector:
“The unorganized sector consists of all unincorporated private enterprises owned by individuals or households engaged in the sale and production of goods and services operated on a proprietary or partnership basis and with less than ten total workers” [22]. The definition of unorganized or informal employment is “Unorganized workers consist of those working in the unorganized enterprises or households, excluding regular workers with social security benefits, and the workers in the formal sector without any employment/ social security benefits provided by the employers” [22].
In India, the unorganized units are generally of single ownership. There are a variety of drawbacks for the unorganized sector. The units are normally small in size with low capital investment per employee [23]. With poor infrastructure and resources, organizations also do not have much scope for entrepreneurship development. Another challenge for unorganized units is to compete with organized manufacturing units [24]. The largely illiterate working population is unaware of the dangers associated with their occupation [25]. Unorganized enterprises also lag behind in terms of technology as they are still using poor and obsolete technology. There is also an urgent need of technology upgradation. The usage of old obsolete technology reduces the productivity and income of the workers.
Health related issues are of prime concern among the unorganized workers in India [26]. Unhygienic conditions more prevalent in the unorganized workplaces often cause occupational health hazards to the workers [27]. Due to lack of awareness of the workers on the safe material handling and no systematic legislation of work safety, this sector is largely undermined despite of huge turnover every year from this sector.
Constantly changing economic conditions and easily available work force without any social benefits unlike organized sector, the health-related problems are more prevalent among workers of unorganized sector in India. Workplace environment is the vital aspect that can impact a worker’s health greatly. Most of the workstations are not ergonomically constructed. Unsafe material handling due to lack of knowledge also reveals higher risks related to accidents and injuries.
A large part of Indian economy depends upon unorganized workforce and welders from unorganized welding units are an integral part of it. The welders from unorganized welding units were considered for the present study for the reason that the negligible attention was paid on this workforce. Their health conditions are very little known to the world. The problem becomes more intense in the case of welders belonging to roadside manufacturing units being a part of the unorganized sector. Several occupational diseases reported in the studies among workers of the unorganized industrial sector of India and these workers create the bottom layer of the working class [22]. In comparison with the Indian organized sector, the welders from organized welding industry were equipped with protective equipment and ergonomically designed tools but in case of unorganized sector, no such equipment and tools are provided to the workforce. Therefore, the present study examined the prevalence of respiratory symptoms, their associated factors and lung function impairment amongst the welders of unorganized welding units of Punjab, India.
Study design
Snowball sampling method was used for deciding the sample size for the reason that there is no availability of data regarding the unorganized welding units and their workers. The questionnaire was administrated across 283 welders from 22 cities of Punjab.
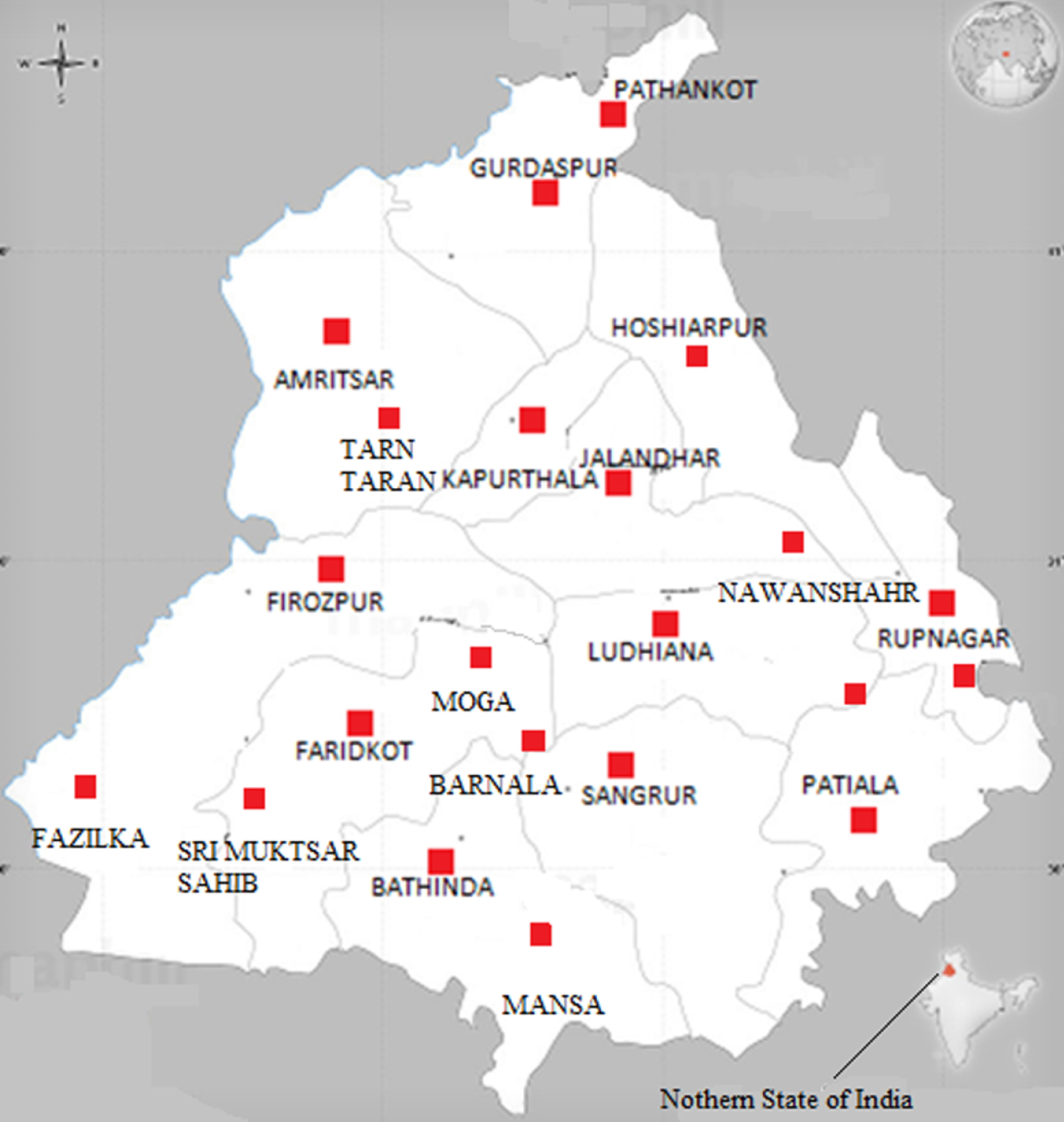
Map of Punjab showing data collection sites.
Punjab is a state situated in the northern region of India. The economy of Punjab is agriculture based and repair of agriculture equipment, tools and household equipment is done through the welders. Small industries of hand tools, sports goods, agriculture equipment are the part of manufacturing sector of Punjab. Approximately 12 welders were chosen from each city randomly for present study. These welders were from roadside welding units belonging to the unorganized sector.
The welders were thoroughly explained the purpose of the study in their regional/local language and they were convinced to participate in the study. The questionnaire included questions on socio-demographic details, job description, personal history, welding exposure, respiratory symptoms and PPE usage. After administrating the questionnaire and getting the responses of all questions the participants were acquainted with the various health hazards associated with welding.
Age: Welders of age period between 18–55 years employed for at least 1 year in above-cited location and 12 months of welding experience; do not have any previous medical history; the existence of some respiratory symptoms; performing welding work for at least 4 hours per day. All welding units were located in the unorganized sector. Welders were currently working at an unorganized welding unit for at least the last one year in the aforementioned geographic location. The non-welders considered for the study were also working in the same working environment but had never been involved in the welding profession.
Exclusion criteria
Participants with physical deformities were excluded from the study. The welders working in organized welding industries or firms were excluded because their working environment is equipped with mechanized ventilation and supplied with PPE by the authorities. Also, the working pattern and duration of work of these individuals were likely to vary.
Statistical analysis
To identify the prevalence of respiratory symptoms, the descriptive statistics of their frequencies were used. To determine the risk factors related to the presence of respiratory symptoms like chronic cough, phlegm, shortness of breath, chest tightness, sputum and wheezing logistic regression analysis was used to examine the association between respiratory symptoms and independent variables. Model fit was determined using an α= 0.05, with p < 0.05 indicating statistical significance. The student’s t test was used to analyze the association between the spirometry data of welders and non-welders. The analysis of the data was performed by using software IBM SPSS version 22.0.
Validity and reliability
After performing the pilot survey, the questionnaire used in this study was developed by the researchers and was modified after consulting the expert committee in accordance with Indian society, culture and the welders’ workplace environment. Experts tested the validity of the questionnaire whereas the reliability was calculated by using (Cronbach’s α= 0.75). The questionnaire was tested on 50 welders who were not included in the study.
Measurements
Social and psychological factors were measured through socio-demographic information, including age, gender and education. Lifestyle risk factors were evaluated by assessment of the welders’ daily living habits, including smoking. Economic risk measurements involved assessing the welders’ work characteristics, including the amount of breaks per working period, the number of working days per week and hours worked per week. Variables in this study consisted of independent and dependent variables. Independent variables included the socio-demographic factors (age, gender and education), lifestyle factors (including smoking) and economic factors (including hours worked per week, number of breaks per work period, working days per week), safety and health of the work environment (Including PPE usage). The dependent variables namely chronic cough, phlegm, wheezing, shortness of breath, chest tightness and sputum are considered as the respiratory symptoms.
Pulmonary function test
After administrating the questionnaire, 50 welders and 50 non-welders were subjected to pulmonary function test using spirometer RMS Helios 401 (Recorders & Medicare Systems Pvt Ltd, India) reusable mouthpiece and nose clip. The guidelines of the American Thoracic Society were followed during the conduct of the test [28]. Each participant was subjected to perform the three trials of the test taking rest break of 1–2 minutes in between. Out of three trials, the best one was recorded. The lung function parameters such as FVC, FEV1 and FEV1/FVC ratio were studied. The test was conducted for both the groups i.e. exposed as well as the control group. After the completion of the test, data was compiled in Microsoft Excel 2010 and the spirometry test results of two groups were compared by using Student’s t test.
Results
A total of 283 participants, who were working in the profession of welding included in the study. Table 1 reveals the demographic information of the participants. Majority of welders were under age group of 30–40 years. Majority of them were experienced, non-smokers and had low level of education. While performing welding operation only 20.8%of welders always use PPE.
Demographic data of welders
Demographic data of welders
The prevalence of respiratory symptoms among welders is given in Table 2.
Prevalence of respiratory symptoms among welders
Prevalence of respiratory symptoms among welders
Using a Bivariate analysis, in Table 3 the risk factors for the prevalence of chronic cough, phlegm, shortness of breath, wheezing, chest tightness and sputum were evaluated among welders, with p < 0.05. Table 4 represents the logistic regression analysis of respiratory symptoms and independent variables e.g., age, experience, smoking habits, hours worked per day and PPE usage. The welders of age group≥40 years (OR 13.400, 95%CI 2.834–63.352) were at more risk of chronic cough. Also, the welders who worked for≥40 hours per week (OR 7.642, 95%CI 2.306–25.327) were found with an increased risk of a chronic cough when compared with the welders of age≤30 years.
Bivariate analyses of sociodemographic, lifestyle and safety & health factors as they relate to respiratory symptoms (N = 283) n (%)
Logistic regression analysis of factors associated with respiratory symptoms among welders (N = 283)
Notes: OR = Odds Ratio. aThe Logistic regression of Chronic cough symptom = –2LL = 294.749(p < 0.001); Cox & Snell R2 = 0.255; Nagelkerke R2 = 0.346. bThe Logistic regression of Phlegm symptom = –2LL = 266.061(p < 0.001); Cox & Snell R2 = 0.327; Nagelkerke R2 = 0.444. cThe Logistic regression of Shortness of breath symptom = –2LL = 280.988(p < 0.001); Cox & Snell R2 = 0.247; Nagelkerke R2 = 0.342. dThe Logistic regression of wheezing symptom = –2LL = 283.244(p < 0.001); Cox & Snell R2 = 0.225; Nagelkerke R2 = 0.315. eThe Logistic regression of chest tightness symptom = –2LL = 268.182(p < 0.001); Cox & Snell R2 = 0.305; Nagelkerke R2 = 0.417. fThe Logistic regression of sputum symptom = –2LL = 230.542(p < 0.001); Cox & Snell R2 = 0.376; Nagelkerke R2 = 0.519.
The participants of experience between 11–15 years had increased risk of phlegm than who had been working for 1–5 years. Also, welders who had experience of 16 + years (OR 11.301, 95%CI 2.139–59.708) were found to be associated with an increased likelihood of phlegm.
The welders who had been working for > 5 days per week (OR 14.950, 95%CI 4.090–54.645) were associated with shortness of breath. The welders of 16 + years of experience (OR 14.018, 95%CI 2.766–71.038) were found to be associated with an increased likelihood of wheezing. The group of welders who were smokers (OR 1.966, 95%CI 1.060–3.647) and also, who worked > 5 days per week (OR 6.750, 95%CI 2.265–20.117) had an increased risk of chest tightness. The welders who were smokers (OR 21.978, 95%CI 10.560–45.741) found to be associated with an increased likelihood of sputum.
Table 5 represents the lung function impairment of welders and non-welders. The mean values of lung function parameters FVC, FEV1 and FEV1/FVC ratio of welders were 3.37±0.175, 2.59±0.16 and 76.63±6.16 respectively and that of non- welders were 3.70±0.15, 3.05±0.25 and 82.49±7.62 respectively. The results of the pulmonary function test show the significant difference between the mean values of lung function parameters of welders and non-welders (p < 0.05). The mean age of non-welders is more than that of welders. Also, the Body Mass Index (BMI) of both the groups was not found to be significantly different (p < 0.05).
Pulmonary function impairment among welders
Pulmonary function impairment among welders
Note: BMI = Body Mass Index; FVC = Forced Vital Capacity; FEV1 = Forced Expiratory Volume in 1 s.
The current study aimed to assess the prevalence of respiratory symptoms and lung function parameters among the welders in unorganized welding units of Punjab state of India. The results of the study revealed significant association of some of the respiratory symptoms with age, experience, smoking habits, working hours and PPE usage. However, the welders of higher age group, welders who spend more time in welding and welders who were smokers are more likely to develop respiratory symptoms in them. Therefore, these findings support the idea that exposure to welding fumes and gases in welding units is significantly associated with increase in respiratory symptoms and significant deterioration in lung function parameters among welders. Although there are enormous welding processes, yet the welders from Indian unorganized welding units indulge themselves in manual metal arc welding or stick welding and gas metal arc welding [29].
This study was among very few studies conducted in developing country like India in the northern region especially in the state of Punjab. All the participants in the present study were male. Male participants tend to engage themselves in hazardous work, which is understood from our findings.
It was found that 63.6%of welders had attained education whereas 36.4%of welders were illiterate. It is reflected from the results of the present study that many workers working in the unorganized sector in developing country like India are deprived of primary education. Illiteracy and low level of education is still a problem in India. The percentage of illiterate welders in the present study is more as compared to participants in the study conducted by Chauhan et al. [30]. Majority of welders do not know about the harmful effects of the hazardous fumes and gases generated from the welding. This may be due to the lower level of education, lack of awareness and technical or formal welding training.
The prevalence rate of chronic cough, phlegm, shortness of breath, wheezing, chest tightness and sputum were higher among the welders. Some of these symptoms were in accordance with the studies conducted by Qin et. al., Sidhagodra et. al. and El-Zein et. al. [31–33]. The implementation of hazards control methods like replacement/substitution of hazard, engineering controls and administrative controls in the unorganized sector is a cumbersome task, although the PPE are the least effective among the hazards control methods. Use of PPE in unorganized sector is best fit among all the hazard control methods. It is possible that PPE usage is able to act as a barrier in between the hazard and a welder. From our study it is clear that welders were reluctant in the use of PPE. The values of spirometric parameters were lower in the welders than in the controls. Many other studies had reported the lower values of lung function parameters. The lowering in FVC, FEV1 and FEV1/FVC ratio were due to inhalation of the welding fumes and gases. A study by Chinn et al. [34] on welders and caulker-burners found a decline in FVC, FEV1, PEF and FEF 50%also, this reduction was equally due to welding and smoking. Therefore, our results were found to be in agreement with many of the studies where welders had deteriorated spirometric indices in contrast with controls [35–38]
Our study presented the work-related deviations in lung function parameters in the welders. Also, the time duration spent in performing welding operation might have an imperative role in the generation of respiratory symptoms among welders. Instead, the type of welding operations, time duration spent on welding operation, the material used for welding and work environment were very crucial factors in the developing respiratory symptoms and lowering of the lung function parameters. In our study, there is a significant association between smoker welders and the respiratory symptoms. The smoking may be an additional risk factor affecting the respiratory health of welders. Therefore, it is our strong recommendation for the welders to quit smoking. Not only welding fumes exposure but above said influencing factors must be explored [39].
The present study is limited to the welders of unorganized sector. The study may be extended or comparison can be made with the welders of organized sector. Additionally, this study is limited in the accuracy of the measured prevalence of the addressed respiratory symptoms, which may differ from those found in other studies, due to the small sample size of this study. Future research based on intervention programs of the occupational health could be done to measure the effectiveness of health programs in the welding units of an unorganized sector. The roles of welding materials, welding tasks and welding in confined areas must be explored in future studies. Information regarding comorbidities like COPD, asthma, pneumoconiosis and tuberculosis were not included in the study.
Conclusions and recommendations
The present study highlights the respiratory health status of welders working in unorganized sector. Welders experienced an increase in respiratory symptoms and the decrement in the pulmonary function parameters. The respiratory symptoms reported by welders were chronic cough (38.86%), phlegm (38.86%), shortness of breath (33.56%), wheezing (32.15%), chest tightness (36.4%) and sputum (34.27%). The decreased pattern of mean values of lung function parameters of welders than controls; FVC (3.37±0.175 vs 3.70±0.15), FEV1 (2.59±0.16 vs 3.05±0.25) and FEV1/FVC ratio (76.63±6.16 vs 82.49±7.62) was observed.
Long working hours, low level of education, hazardous working conditions, lack of implementation of safety laws make the welding group more vulnerable to health risks. The welders of Indian unorganized sector work without any technical training related to welding and safety. Result of which, they are unaware of working in a safer environment and health hazards. Moreover, safety norms and laws are not followed by employers and employees in India. Also, the welders do not bring the PPE in use.
Recommendations suggested to the welders and the owners of the unorganized manufacturing units: Welders should adopt control measures like proper ventilation and exhaust systems. While performing welding operation, welders must be provided with PPE like face shield, welding helmet, goggles, gloves and mask or respirators to reduce the effect of welding hazards up to certain extent. Proper orientation sessions about the workplace hazards and to maintain hygiene at their workplace should be organized by government, employers and non-government organizations. Welders should not ignore the minor respiratory problems as they can lead to serious health issues and should take proper health check-up and medication to sustain healthiness. Proper welding training should be taken by welders before starting welding as profession to make them skilled. It is recommended to welders that they should quit smoking.
Conflict of interest
The authors have no conflicts of interest to declare.