
Abstract
BACKGROUND:
Despite improved health and during a strong job market (pre-COVID-19), a substantial proportion of HIV+ adults remained unemployed. This study sought to provide time-limited counseling to promote employment goals.
OBJECTIVE:
To determine whether behavioral activation (BA) or supportive counseling (SC), would be more effective in promoting vocational goals (full or part-time, paid or volunteer).
METHODS:
The study included two groups: those with clinically significant fatigue, who were first treated with armodafinil. Once their fatigue diminished, they were enrolled in the counseling program. Those without fatigue were enrolled directly. Both BA and SC interventions were manualized, consisting of eight individual sessions plus a follow-up.
RESULTS:
116 participants entered counseling, including 87 assigned to BA and 29 to SC. Of these, 79 completed counseling or found a job by session eight. By follow-up, 51%of BA versus 41%of SC participants had found jobs, a non-significant difference either clinically or statistically.
CONCLUSIONS:
Multiple issues contributed to difficulty in employment, including gaps in resumes, loss of contact with former colleagues, and uncertainty about career direction. Ongoing barriers included substance use, housing instability, ambivalence about forfeiting government benefits, as well as inadequately treated depression. Success in employment for about half of participants is, in this context, a reasonable outcome.
Introduction
Despite the effectiveness of antiretroviral treatment in restoring or maintaining stable health, and a declining unemployment rate among the general population before the COVID-19 pandemic, a substantial number of HIV+ adults remained unemployed [1, 2]. Loss of income and often, financial independence are not the only casualties of unemployment. In addition to a paycheck, work may offer a sense of purpose, structure to the day, social interactions and belonging, and an overall improved quality of life [3]. Vance and colleagues [4] suggested that those who are unemployed do not receive the neurocognitive benefits (enriched personal and social environment) of employment. In their systematic literature review, Rueda et al. [5] found a beneficial health effect of returning to work in a variety of populations, times and settings. In an independent review, Hergenrather et al. [6] concur, considering employment as a social determinant of health. Grob et al. [7] suggest that a sense of “normality,” being a working member of the community, is another benefit of employment.
Return to work after a period of unemployment is more complicated for those with HIV/AIDS. Concerns include impact of earned income on long-term government benefits, which may range from barely sustainable (under $400/month cash plus rent and food stamps in New York City) to tax-free Social Security Disability Insurance (SSD) whose payments can reach $2800/month, depending on final salary before leaving the workforce. Other concerns include questions about having the physical stamina to work a full day (or shift), outdated skills, and need for some flexibility to attend medical appointments. In addition, as noted by Martin et al. [8], concerns about gaps in work histories, and ambivalence about working often serve as barriers. The challenge of re-employment is substantial, as seen in a prospective Canadian study by Lem and colleagues [9]. Of 392 persons on antiretroviral therapy with stable health who were unemployed at study entry, only 16%were working a year later.
Several observational studies have examined pre-dictors or correlates of unemployment among HIV+ adults. These include psychiatric comorbidities (dep-ression or substance use disorders) [10, 11], the “golden handcuffs” of benefits [12], fear of workplace stigma [13], possible neurocognitive impairment associated with HIV status [14], and medical co-morbidities. Kordovski et al. [15] studied the effects of aging and HIV disease on employment status and found that they have an additive effect on employment status, and that employment status is associated with both cognitive and medical risk factors among older (over age 50) HIV+ adults.
More generally, in a review of the literature concerning adults with musculoskeletal or psychiatric disorders, Etuknwa and colleagues [16] found that both personal (e.g. self-efficacy) and social factors (e.g. support of supervisors and coworkers) influence success in returning work and sustaining employment.
Another employment barrier among HIV+ adults is fatigue. Among HIV+ adults, estimates of fatigue prevalence vary considerably: Barroso et al. [17] reported rates ranging from 33%to 88%in 2015, and in their literature review, Merlin et al. [18] used an estimate of 30–80%in the modern treatment era. In this context, fatigue has played a prominent role as a barrier to work and even job-seeking efforts.
Few interventions specifically designed for HIV+ adults have been conducted. Kielhofner et al. [19] developed a theory-based study in which they evaluated an open-ended program of vocational services for HIV+ adults. Phase 1, which lasted 8 weeks, was devoted to self-assessment and refinement of vocational choice, development of job-relevant skills and gathering information, with emotional support for returning to work in weekly group sessions. Phase 2 included placement in volunteer positions, internships or temporary work experiences, to work through issues and develop confidence in the ability to manage the routine of working. Phase 3 supported successful employment, while Phase 4 was intended to sustain employment. The program was administered by two occupational therapists and a vocational placement specialist. Participation duration ranged from one to eight months depending on client readiness for change. Over a two-year period with semi-annual follow-up interviews including advice and offers of assistance, 47%of 129 participants achieved a goal that included employment, volunteering, enrolling in training or returning to school as determined during a study visit. Among completers, defined as 8 + weeks of participation, 67%achieved one of these outcomes.
In a subsequent project conducted with HIV+ adults living in supportive housing, Kielhofner and colleagues [20] established programs in 4 facilities. Two served as the sites for the intervention program, and two served as sites for the control program. In the two intervention facilities, residents who volunteered were offered 8 group sessions and optional drop-in individual sessions, with the overall goal of enhancing “productive participation.” The sessions covered multiple topics such as managing physical and mental health, skills for independent living, building vocational skills, and learning self-efficacy. The control programs consisted of 8 weekly educational groups designed to provide information about community resources and services to support productivity, followed by 9 monthly meetings on related topics. More participants in the intervention than control group found some kind of employment (not further defined) during the 9-month follow-up: 34%(13/38) vs. 19%(5/27).
We found only one randomized, controlled trial designed to promote employment for HIV+ adults, conducted by Martin and colleagues [21], which was based on findings from their earlier study (10). Participants were HIV+ adults who had stopped working due to disability, were receiving disability payments, and were considering employment. The purpose was to evaluate the efficacy of the intervention using work-related activities as the outcome measure. This included steps such as job training, volunteering, loo-king for a job, and finding paid employment. A second goal was a “dose-response analysis” to determine whether increasing amounts of the intervention led to more workforce reentry activities. In the randomized clinical trial, groups were stratified for education, ethnic minority status, and CD4 count. A comparison group received a single session plus community referrals, while the intervention group consisted of a mixed modality program:13 group sessions over 7 weeks, and 3 individual sessions; one at the beginning, middle and end of the 7 weeks. Thereafter, opti-onal individual sessions were offered throughout the 2-year semi-annual follow-up that included telephone calls to participants offering assistance in goal achievement every 30 to 60 days. They found that members of the intervention group engaged in more re-entry activities and, once employed, were more likely to remain employed, compared to controls. They did not find a difference between groups regarding re-entry into the workforce, which they suggested may be attributable to their extensive HIV illness histories. Number and percent of those who found employment in each group are not reported.
Overall, as of 2015 when their review of the inte-rnational literature was conducted, The Cochrane Library staff, Robinson, Okpo and Mngoma [22] concluded, “for vocational interventions, the one included study found no evidence of an intervention effect. We need more high-quality, preferably randomized studies to assess the effectiveness of RTW interventions for HIV+ persons” (p. 2).
The current study was intended to address this need. We sought to explore the effectiveness of a brief, manualized intervention suitable for application in real world settings, such as HIV service organizations. The intervention evolved from a series of clinical trials with HIV+ adults, beginning with randomized placebo-controlled trials of modafinil [23] and armodafinil [24] to treat clinically significant fatigue. In those trials, we asked patients what they would do differently if they had the energy. In the modafinil trial, 71 of the 115 patients enrolled said they wanted to return to work or take vocational/educational classes. Only 16 (23%) had done so by Week 26, even though they initially stated that fatigue was the barrier preventing employment [23]. We noted, “it seems likely that additional support and tailored interventions are needed to assist HIV+ patients in achieving these goals” (p. 714). We then conducted a pilot study combining a pharmacologic-behavioral approach for HIV+ adults with clinically significant fatigue who sought to return to work or initiate training to increase employment opportunities [25]. Patients whose energy improved after 4 weeks of armodafinil were seen for 8 biweekly sessions of behavioral activation counseling. Of the 46 who began BA sessions, 63%attained their vocational or training goal, 9%took meaningful steps, and the remainder (28%) showed little or no progress.
Building on this pilot study, we designed a clinical trial comparing two manualized 8-session bi-weekly counseling interventions, behavioral activation (BA) counseling and supportive counseling (SC). Inclusion criteria were broadened to include HIV+ participants without fatigue to increase generalization of findings. Those participants were randomized directly to either BA or SC, without the 4-week armodafinil treatment phase. Based on pilot study findings, we focused on employment (full-time or part-time, paid or volunteer), since educational or training goals generally entailed finding financial aid, which often could not be obtained during the study time frame. We also added a community site, Callen Lorde Community Health Center, to evaluate the real-world feasibility of our interventions.
We addressed the following questions: 1) Did more participants in BA counseling return to work compared to participants receiving SC; 2) What predictors or moderators were associated with successful employment? 3) Were there mediators (early changes on self-rating scales) associated with more success in finding a job? Were the changes different for BA and SC?
Methods
Sample
Recruitment
Participants learned about the study from flyers distributed at HIV–related social agencies and medical clinics in New York City, and referrals by their staff members. In addition, the two counselors assigned to this study at our collaborating site, Callen-Lorde Community Health Center, were responsible for recruiting potential participants. If eligible (determined at the Columbia site), and enrolled, the Callen Lorde staff members provided the counseling.
Study Eligibility Criteria
Eligible participants were HIV+, ages 18–70, English-speaking, currently unemployed, able and willing to give informed consent, and had an employment goal that was feasibly achieved within the study time frame of 6 months (including follow-up). Those participants who presented with significant fatigue, defined as having scores > 40 on the Fatigue Severity Scale (FSS) [26], and therefore eligible for armodafinil treatment, were asked to sign a release that allowed us to contact their medical provider to confirm that their health was stable and to get their agreement for the patient to take armodafinil. Other medical exclusion criteria for participants with fatigue included: EKG results suggesting left ventricular hypertrophy, having started testosterone within the past 6 weeks, untreated and uncontrolled hypertension, currently taking psychostimulant medication, conditions that may cause fatigue such as low testosterone, untreated hypothyroidism and anemia. Exclusion criteria for all participants, evaluated at the study screening visit by a doctoral level psychologist included: untreated major depressive disorder, clinically significant suicidal ideation or Hamilton Depression Scale score > 24, a history or current psychotic or bipolar disorder, and full criteria for a substance use disorder in the past 3 months. Participant report of substance use was confirmed using both urine dipstick and laboratory assay.
Procedures
Patients presenting with significant fatigue (FSS scores > 40) were treated with armodafinil, a fast-acting stimulant medication (classified as Schedule IV by the Food and Drug Administration). We have shown in placebo-controlled clinical trials that off-label use of armodafinil (and modafinil, a similar medication) are safe and effective in this population [19, 20]. If participants’ fatigue diminished after 4 weeks, they became eligible for the counseling phase, during which armodafinil treatment was maintained. Participants without fatigue were entered directly in the counseling component of the study (See Fig. 1 for Study Diagram).
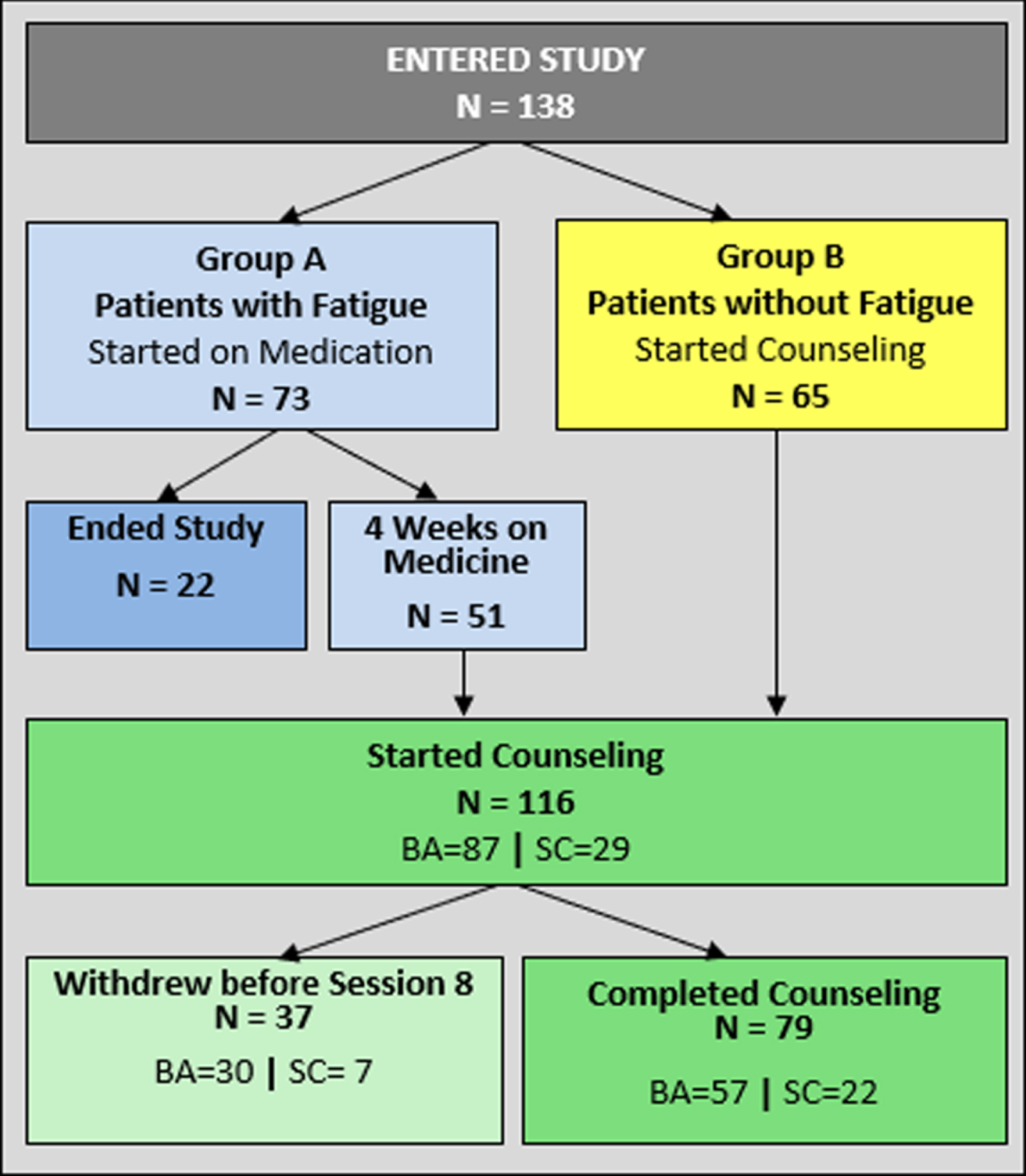
Study diagram.
Participants were assigned randomly to receive either BA counseling or SC in blocks of four, using a computer-generated list, subject to counselor availability. At the Callen Lorde site, counselors recruited potentially eligible clients. One counselor provided SC and the other, BA. At the Columbia site, there were two BA and one SC counselors.
Before the first counseling session, trained study personnel (MMc or JGR) met with the participant and prospective counselor to establish their goals in operational terms. We also elicited one or two other goals that the participant sought to achieve in the next few months, such as increasing social activities or going to the gym regularly. We rated progress on these goals at Sessions 4, 8 and follow-up using a modified Goal Attainment Scale (described below). The study was approved by the New York State Psychiatric Institute Institutional Review Board, and all participants gave written consent after being informed of the procedures, and risks and alternatives to study participation. Data collection began in 2014 and ended in 2018.
Socio-demographic variables at baseline included: age, education, ethnicity/race, type of housing, and income including government or private benefits. Medical variables included: current and past CD4 count, HIV RNA viral load, AIDS diagnosis, and time since tested HIV+. We asked about substance use history, and time since last use. We also asked about work history including time since last employed, and reasons for leaving work.
Psychiatric measures at baseline include the psychotic screen, substance use disorders screen, depression and bipolar disorders modules of the Structured Clinical Interview for DSM-IV (SCID) [27] as well as the Structured Interview Guide for the 21-item Hamilton Rating Scale for Depression [28]. The following self-report measures were administered at baseline and then again at sessions 1, 4, 8, and the follow-up visit: Beck Depression Inventory-II (BDI-II) [29], Patient Health Questionnaire (PHQ-9) [30]. The Fatigue Severity Scale (FSS) [26], also given at sessions 1, 4, 8, and follow up, assesses mostly physical symptoms of fatigue. Examples of items include: “Exercise brings on my fatigue,” “Fatigue prevents sustained physical functioning,” and “Fatigue interfered with my work, family or social life.”
In addition, six self-report measures were administered at sessions 1, 4, 8, and the follow-up visit. The self-report scales were the Apathy Evaluation Scale [31], Behavioral Activation for Depression Scale (BADS) [32] and Environmental Reward Observation Scale (EROS) [33], both of which were developed to evaluate change in BA; Pearlin Mastery Scale [34], Quality of Life Enjoyment and Satisfaction Questionnaire (QoL) [35], and Ways of Coping [36]. Table 1 provides a description of these measures, number of items, score range and cut-offs where applicable.
Counseling measures: Items, content, score range, and cut-offs (if applicable)
Counseling measures: Items, content, score range, and cut-offs (if applicable)
After enrollment began, resources allowed us to add a neuropsychological sub-study, in which 48 participants agreed to participate. It included detailed interviews about substance use and their assessment including the MINI [37] for diagnostic confirmation (DSM-5). We used the neuropsychological tests in the NIH Toolbox [38] cognitive section, which includes seven modules that are summarized in composite scores measuring Crystalized and Fluid cognition, as well as a Total Cognition composite score. Crystallized scores reflect accumulated store of verbal knowledge and skills while Fluid cognition is a global assessment of current functioning. All results get summarized as transformed standardized scores with a mean of 50 and standard deviation of 10 points.
A primary outcome measure was created to rate progress, if any, toward employment. We used a modified version of the Goal Attainment Scale (GAS) [39]. It is scored as follows: 1 = minimal or no action; 2 = some steps taken; 3 = actively engaged in finding work, and 4 = achieved goal of employment.
Both forms of counseling were manualized. Counseling consisted of eight 60-minute sessions. The first three sessions were conducted weekly, and the remainder were biweekly, with a follow-up visit after 3 months. Senior clinicians, expert in each method, provided initial training for the counselors that included listening to recordings of example sessions as well as role-playing. Biweekly supervision was offered throughout the study and included listening to audiotaped sessions provided by each counselor.
Behavioral Activation
The Behavioral Activation manual for goal achievement was adapted from BA for the Treatment of Depression - Revised (BATD-R) [40], and was described in more detail in our earlier study [25]. Briefly, the focus of the eight BA sessions is directed towards encouraging the participant to actively engage in employment-related activities and to address emotional and behavioral barriers to success. Homework was assigned at each visit, using a workbook we provided, to list goal-related activities for the week and to note when they would be attempted. For example, goals for the week might include: revising resume, searching for jobs on the internet, and submitting 2 applications.
Supportive Counseling
The Supportive Counseling (SC) manual was developed to provide an intervention that would control for contact time with the counselor, homework assignments, as well as nonspecific effects such as therapeutic alliance [41]. The goal of the sessions was to facilitate an atmosphere where the participant could talk about their thoughts and feelings regarding the pursuit of their goals. The counselor did not provide advice, but used techniques such as reflective or active listening, empathic statements, and open questions to encouraged the participant to arrive at their own solutions. Patients were asked to keep daily journals of their thoughts and feelings about the steps they needed to take to achieve their goals.
Statistical analyses
Primary Outcome
The primary outcome was success in achieving employment. This was defined as a score of 4 on the 4-point GAS scale; those with scores 1–3 were not employed. We anticipated that 60%of participants in BA counseling and 25%of SC participants would achieve their work goal, based on our prior work.
Baseline differences by counseling treatment group were assessed using chi-square tests for categorical measures, t-tests for normally distributed continuous measures, and Wilcoxon-rank tests for skewed continuous measures. To assess the effect of counseling treatment assignment on work outcome at session 8 and follow-up, a longitudinal logistic regression model was fit using generalized estimating equations with an autoregressive covariance structure to account for within-subject variance. These models utilized a logit-link function, therefore model estimates are interpreted as log-odds ratios. The model contained the main effect of counseling treatment assignment (behavioral activation vs supportive counseling), time (session 8 visit vs follow-up), and their 2-way interaction. A second model was fit additionally adjusting for the covariates of age, years of education, history of stimulant use, and current depression diagnosis, which were potentially related to work goal achievement. To assess the effect of counseling treatment assignment on progress towards work goal achievement, similar models as above were fit to goal achievement using a cut-off of 3. These models were fit unadjusted and adjusted by the same set of covariates as the primary outcome.
Potential moderators of the effect of counseling treatment on successful work goal achievement were also assessed. They were fit in a similar fashion to the unadjusted model described above except additionally included a 3-way interaction between treatment assignment, time, and moderator, as well as all subsequent 2-way interactions. The potential moderators included: age, years of education, history of stimulant use, current depression diagnosis. A separate model was fit for each moderator.
Some of the analyses were run using SAS version 9.4, and all statistical tests were two-sided with an alpha level of 1%. All analyses were assessed using the counseling completer sample (n = 79), defined as completion of the 8 sessions, or employment at any point before. Unobserved values were assumed to be missing at random given that analyses of dropouts led to no meaningful differences between those who dropped out prior to the final visit compared to those who completed the study or discontinued counseling due to attaining work prior to the final visit.
Results
Sample
After an initial phone screen, 213 potentially eligible participants were seen for an evaluation. Of these, 138 were eligible and chose to enroll in the program. Seventy-three participants had clinically significant fatigue and 65 did not. The 65 participants without fatigue were randomized directly, while the 73 with fatigue first began treatment with armodafinil, and then were eligible for counseling after four weeks if their fatigue diminished and they continued to want to pursue employment. Of these 73, six found jobs within the first four weeks of armodafinil treatment, 16 dropped out during the medication phase, and 51entered the counseling phase. Thus, a total of 116 participants were randomized to start counseling with 87 assigned to BA and 29 to SC (Fig. 1).
Characteristics of the 116 participants, and for the BA and SC groups separately, are shown in Table 2, including demographic, living and financial circumstances, medical, psychiatric variables, and for a subgroup, results of neuropsychological testing. All were HIV+ gay men who were, on average, in their late forties, about half were men of color, and most had post-high school education. When they enrolled, 52%were living on public assistance (cash income of about $5,000/year) plus food stamps, rent, and Medicaid through HASA (HIV/AIDS Services Administration). Three quarters had their own apartments, some with rent provided by HASA; the others were in congregate facilities (own room and bathroom, social services on premises), or SRO’s (single room occupancy hotels). Half of the participants had an AIDS diagnosis based on health history and all were taking antiretroviral medications. Mean time since HIV diagnosis was 15.5 years (range: 2 months to 33 years), and 37 (32%) are long-term survivors (diagnosed before 1996).
Demographic, medical, and psychiatric characteristics at counseling baseline for the total sample and by counseling group: Behavioral Activation (BA) vs. Supportive Counseling (SC)
Demographic, medical, and psychiatric characteristics at counseling baseline for the total sample and by counseling group: Behavioral Activation (BA) vs. Supportive Counseling (SC)
aDifferences are assessed using one-way ANOVA for normally distributed continuous measures, Wilcoxon rank tests for right-skewed continuous measures, and chi-square test for categorical measures. bRight-skewed measure shown with median and interquartile range.
Depression and substance use disorders were prevalent in this sample. Thirty-eight percent were diagnosed with dysthymia, major depressive disorder in partial remission, or undertreated major depression. More than half reported a problematic substance use history, predominantly methamphetamine use disorder, and 14%reported a recent methamphetamine use problem.
We asked, “When did you last work regularly at your usual occupation?” (we did not include “gigs” like dog-walking or other short-term sporadic work). Occupations varied widely, from doorman or waiter/cater jobs to corporate positions. On average, time elapsed since last job was 39 months (range = 1–300 months). The most common reasons for leaving their last job were substance use-related (28%), illness (HIV–related) (16%) and depression (14%).
Reasons for Attrition
Attrition during counseling did not differ significantly between treatments (BA: 34%dropout vs SC: 24%dropout, χ2(1) = 1.07, p = 0.301).We were able to identify reasons for 35 of the 37 participants. The most common were: 1) “didn’t like” counseling; (38%),2) = methamphetamine relapse (24%), 3) change of goals - e.g. to training programs or no work at this time (22%). Two participants moved away, and 2 had worsening medical/psychiatric conditions.
Question 1: Did more participants in BA counseling return to work compared to those receiving SC counseling? Treatment effect on Goal Achievement
There were no significant baseline differences between those who found jobs compared to those who did not as shown in Table 3. Unadjusted model estimated proportions of subjects successfully achieved employment are presented in Table 4 and Fig. 2. At session 8, 32%of BA participants and 36%of SC participants found jobs, while at follow-up, 51%BA participants and 41%SC participants did so. The model estimated treatment effects are presented in Table 4. At session 8, there were no significant difference in the odds of successful employment goal achievement between groups at either session 8 (OR = 0.80 95%CI = [0.28, 2.34], p = 0.690) or at follow-up (OR = 1.32, 95%CI = [0.46, 3.77], p = 0.609), nor was there a difference in odds of goal achievement between groups at follow-up compared to session 8 (2-way interaction: OR = 0.62 95%CI = [0.14, 2.75], p = 0.520).
Demographic, medical, and psychiatric characteristics at counseling baseline for the sample of counseling completers and by outcome group at session 8: Goal Achieved vs. Not Achieved
Demographic, medical, and psychiatric characteristics at counseling baseline for the sample of counseling completers and by outcome group at session 8: Goal Achieved vs. Not Achieved
aDifferences are assessed using one-way ANOVA for normally distributed continuous measures, Wilcoxon rank tests for right-skewed continuous measures, and chi-square test for categorical measures. bRight-skewed measure shown with median and interquartile range.
Observed prevalence of successful employment goal achievement (left panel) with unadjusted model estimated results of successful goal achievement by time-point and treatment group (right panel)
*Model adjusting for the following covariates: age, years of education, history of methamphetamine use, and current depression diagnosis, led to results similar to unadjusted model.
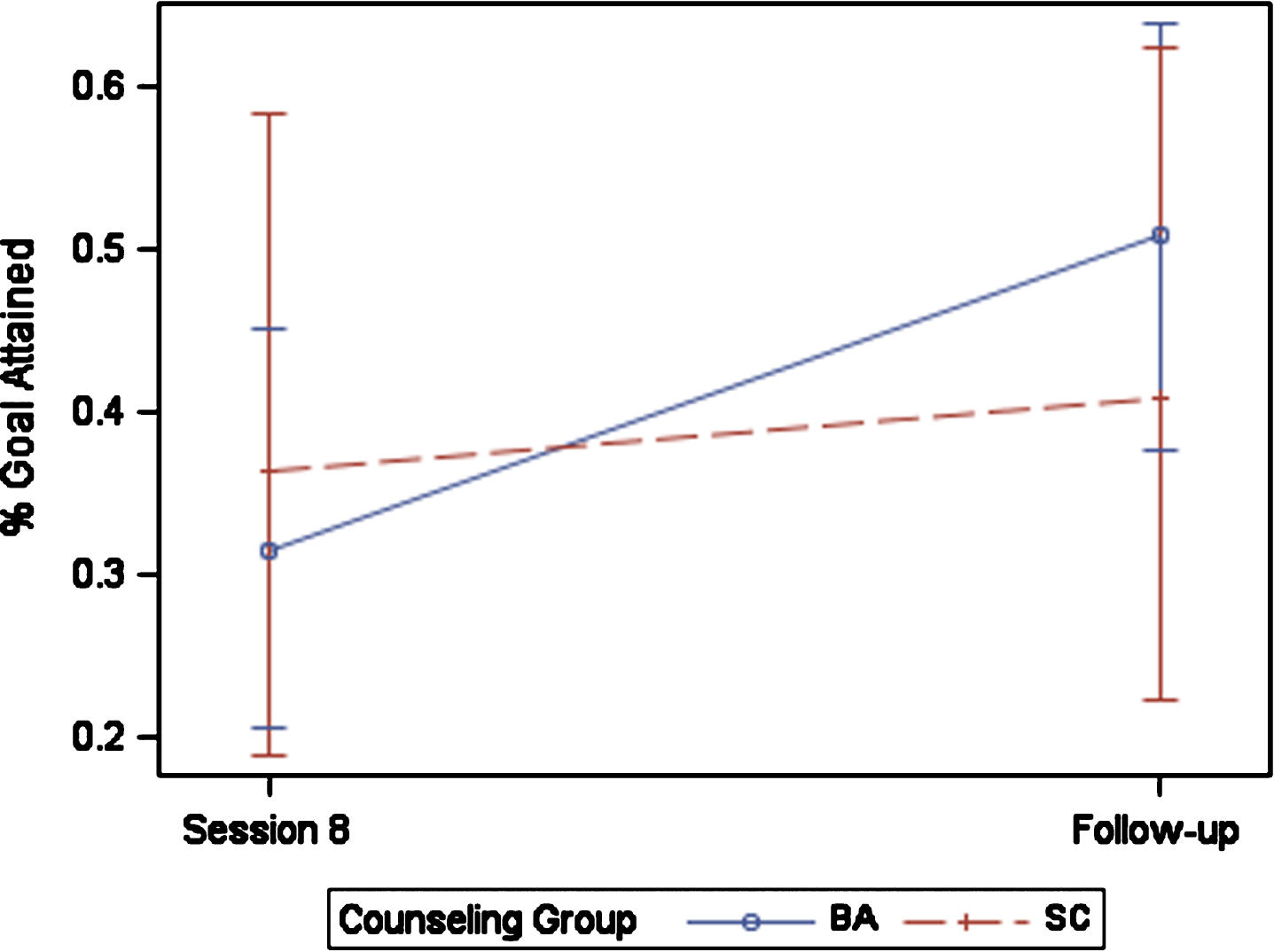
Unadjusted model estimated prevalence of goal achievement by counseling treatment group and time along with 95%confidence intervals.
Similar results were found when adjusting by covariates. In sensitivity analyses using a cut-off of 3 on the modified GAS score, at session 8, 60%of BA participants and 55%of SC participants either succeeded or made meaningful progress towards their goals, while at follow-up, 55%of BA participants and 55%of SC participants had done so. There was also no difference in the odds of progress towards work goals between groups at either time point (all p > 0.05).
Proportion of participants receiving armodafinil for pre-existing fatigue did not differ between BA and SC groups (41%in BA group, 52%in SC group, X2 = 1df, p = 0.812). There was no difference in outcome compared to participants without baseline fatigue (data not shown).
Potential moderators of treatment effect on successful goal achievement were also assessed. The 3-way interaction between moderator, treatment group, and time was not significant for any of the moderators (all p > 0.05). This suggest that age, years of education, history of stimulant use, nor current depression diagnosis did not significantly moderate the effect of treatment on successful goal achievement.
Cognitive Assessment
A subset of 68 patients participated in the Cognitive study. We compared cognitive performance for those who completed counseling (N = 48) and dropouts (N = 20). Completers had higher (better functioning) scores than study dropouts on the Total Composite score, the Crystalized Composite and the Fluid Composite score (all p’s <0.01). However, there were no differences on any of these scales for participants in BA vs. SC (data shown in Table 3) nor for those who attained their work goal vs. those who did not (data shown in Table 2).
Achievement of secondary goals
In addition to work goals, we asked participants to identify another goal they hoped to accomplish during the study time frame. The three most common of these ancillary goals were future classes or job-related training (40%), socializing more (34%), and maintaining sobriety (31%). There were no differences in achievement of these secondary goals between BA and SC groups (data not shown).
Changes in depressive symptoms
For the sample of 116 who entered counseling, Beck Depression Inventory (BDI) scores were higher in the BA group than SC group (means of 17 vs. 12, ANOVA, p = 0.01). PHQ-9 scores, in contrast, did not differ significantly (means of 9 and 7, p = 0.12). Similarly, for the completer sample of 79, the difference on the BDI between treatment groups was not significant (ANOVA, p = 0.059). We compared change scores on both measures at sessions 1, 4, 8, and follow-up. For the completer sample, scores on both tests declined significantly (less depression) between session 1 and sessions 4, 8 and follow-up. There was no difference in amount of change on either test when comparing BA and SC participants at any data point. Similarly, when comparing counseling completers vs. dropouts who completed at least 4 sessions, the change was not statistically significant.
Mediators of return to work outcome: Changes during counseling
We compared changes in scores from study entry to Week 4 on the BDI and PHQ as well as the six self-report scales, in order to identify possible “signals” of future success. As shown on Table 5, significant t-test changes are noted for those who achieved their work goal by Session 8 on the BDI, PHQ, BADS total and subscale scores, and Quality of Life scale. Similar changes are seen in for those who did not achieve their goal on the BADS total and subscale scores. When comparing the outcome groups and controlling for baseline scores, only the Quality of Life scale showed nearly significant differences reflecting more life satisfaction (ANCOVA, p = 0.017).
Within and between-group differencesa from session 1 to session 4 in self-report measures for goal achievers and non achievers at Session 8 (n = 79)
Within and between-group differencesa from session 1 to session 4 in self-report measures for goal achievers and non achievers at Session 8 (n = 79)
aWithin-group and between-group differences are assessed using ANCOVA model adjusting for baseline values with grand mean centering.
Our primary goal was to determine whether par-ticipants engaged in behavioral activation (BA) cou-nseling were more likely to return to work than participants in supportive counseling (SC), whether initially treated for fatigue or not. For study comp-leters, we had anticipated that 60%of BA participants and 25%of SC participants would return to work. What we found is that 51%(29/57) of BA participants and 41%(9/22) of SC participants did so, a non-significant difference both statistically and clinically. In addition, 53%made substantial progress regarding finding a job: 54%in BA and 50%in SC.
The unanticipated success of SC cannot be attributed to any of the moderator variables we assessed (age, education, depression, medical status, substance use disorder), differential attrition, or differential change in depression, levels of apathy, ratings of self-efficacy, mastery, behavioral activation, or environmental reward ratings. At counseling baseline, only one of the many variables we assessed differed between groups: severity of depression symptoms was greater in the BA group on one of the two depression scales.
We compared counseling completers vs. drop-outs and found no baseline differences. We repeated these analyses to compare those who found employment (goal achievers) to those who did not, again finding no differences. We also examined mediator variables (Table 5) to see whether early changes (at Week 4) on any of these scales was associated with goal achievement and found only a measure of Quality of Life predicted goal success.
Compared to results of the previous “return to work” studies we described [20, 21], as well as other observational employment programs [42, 43], our results for both BA and SC are broadly comparable to theirs. In our pilot study, where training or employment were the outcome measure, 63%attained their goal. We have been unable to identify a “return to work” program for HIV+ adults with a higher success rate, using job achievement as the criterion. All intervention programs were more effective than the observed rate of employment in our randomized clinical trial of modafinil [23] for fatigue, which elicited goals at study entry but did not provide counseling. In that trial, 23%of participants succeeded in returning to work of the 71 who aspired to do so at study entry.
Our inclusion criteria were lenient with respect to both depression severity and recent substance use. For the 116 participants who began counseling, we considered the possibility that those in early remission from methamphetamine use disorder (SCID diagnosis), and those scoring in the “severe” range of depression on the PHQ (scores of > 15) might be contributing to the relatively low success rates of counseling. However, when we compared those with PHQ scores of > 15 at the time of their initial evaluation (N = 30) to those with lower scores (N = 86), there was no difference in goal achievement (37%vs. 31%, X2 = 0.281, 1df, p = 0.596). Similarly, when we compared participants with early remission from methamphetamine use (N = 21) to the rest of the sample (N = 95), there was no significant difference in rate of goal achievement (19%vs. 36%, FET = 0.199). Finally, we looked at the those who had either severe depression and/or were in early remission (N = 48) and again did not find a statistically or clinically significant difference in goal achievement (31%vs. 34%, X2 = 0.085, 1df, p = 0.771). Evidently, these subgroups did not differ from the rest of the sample in terms of goal achievement.
Attrition rates were substantial. Of the 37 who started counseling and dropped out, 60%said they didn’t like counseling or had changed their goals. This likely reflects the ambivalence that was common to most participants, as Martin and colleagues noted repeatedly in their studies [11]. Working meant loss of needs-based benefits which 52%of the sample were receiving. Work also meant remaining sober, giving up leisure time, coping with anticipated discomfort about HIV status with colleagues at work, concerns that stress might exacerbate HIV–related health issues, and whether they could manage a full-time or even part-time job in terms of energy and stamina.
Study limitations
Our sample does not include women. The major sources of referrals and self-referrals in response to flyers were community agencies that have a 90%male clientele. Of the 213 people who were screened by phone and who came for their initial evaluation, only 4 were women, and they were either not interested or not prepared to return to commit to the program. In our pilot study of BA counseling plus armodafinil to promote return to work [21], 96%were male. HIV+ women may have care-giving responsibilities (children or parents), substance use issues of their own, or lack of job preparedness which was an inclusion criterion in our study since we did not offer job training skills. Under-representation of women in HIV studies of all kinds is an ongoing problem, seen as well in vaccine and treatment trials internationally [44].
Overall, our Return to Work program did not take into account the real-life situations of a substantial number of participants who were simultaneously confronting housing and/or psychiatric issues such as depression or substance use problems. It is difficult to pursue employment while living in transient housing and seeking better housing options at the same time. Methamphetamine use as well as symptoms of depression were continuing problems for many and interfered with both the job-seeking process and successful employment. Thus, our inclusion of participants having significant challenges in other areas of their lives may have hindered our ability to learn any differences in effectiveness of the two counseling strategies.
Staffing turnover was an issue and contributed to the imbalance in size of our counseling groups: 87 participants were offered BA counseling, and 29 SC counseling. At the Columbia site, counselors included both permanent doctoral level staff, and research assistants who often stayed only a year before moving on to graduate school. At the community site, only one counselor saw a substantial number of participants. There was considerable variation in number of patients treated by each counselor in the course of the study. Retention also varied by counselor. Of those who counseled at least 5 participants, drop-out rates ranged from 15%to 91%.
Conclusions
How do we interpret these results? Given the limited samples sizes and specific population of HIV+ gay men, we can draw only tentative conclusions. SC may be as effective as BA because both approaches share a structure in common. Both are effective treatments for depression. For both there is an initial meeting to outline specific vocational goals, and ongoing consideration of goals and encouragement by a sympathetic counselor in a program with scheduled visits. Both types of counseling are offered in the context of a “return to work” study. Participants attended each visit, aware that progress toward their study goals would be addressed, either directly (BA) in a focused and concentrated manner, or in a broader conversation about how they are doing (SC). Every 4 sessions, their goal progress was directly ascertained and rated, so that they reflected on their goals and progress. This structure, along with the aspect of accountability, may have been common “active ingredients” in both strategies.
In addition, the complex and multidimensional nature of returning to work may have contributed to the difficulty in identifying marked differences between the two approaches or any predictors or moderators. There were many issues that had to be addressed in returning to work, including practical details, such as gaps in resumes and loss of contact with past colleagues. There were also more complex and emotional aspects, such as fear of failure and uncertainty about career direction –whether to return to the kind of work previously done or try something new. Other significant considerations, as noted, housing instability, substance use, uncertainty about giving up government benefits in exchange for a salary, and above all, relinquishing the familiar for the unknown after months to years of relatively unstructured time. In addition, lingering depression and other psychiatric issues were common and were beyond the scope of the program. Success in employment for about half of our participants is, in this context, a reasonable outcome.
The fact that both counseling approaches were time-limited, focused and manualized make them amenable to adaptation in various vocational settings. Because they did not generate differences in the context of the study, one should not conclude that they offer the same value. In a real-world context, the clinician might use aspects of both BA and SC counseling strategies to fit their experience and the client’s situation and expectations. For example, a client who needs support formulating and implementing actionable goals, might benefit from the more hands on aspects of BA, aspects of which resemble career coaching as described by Reid [45]. While the client who is in the early process of exploring employment options, might benefit more from the empathic listening of an SC or career counseling approach.
We should note that the COVID-19 pandemic will probably transform the workplace, including work opportunities and practices. Flexibility, willingness to adapt and modification of work-related goals will be central to returning to work.
Footnotes
Acknowledgments
This work has been supported by the National Institute of Mental Health grant R01 MH 102161 (PI: Rabkin). The authors would like to thank Dr. Asa Radix and the staff at Callen Lorde Community Health Center for their assistance in conducting this study. Several research assistants and coordinators have given invaluable help working as counselors and wrangling data: Shantelle Little, Emily Joyner, Erin Timperlake, and Peter Arden. We are particularly grateful to the participants for their time, effort and patience.
Conflict of interest
None to report.