
Abstract
BACKGROUND:
Work-related musculoskeletal disorders (WMSDs) are highly prevalent among people who work in sedentary jobs. The Cornell Musculoskeletal Discomfort Questionnaire (CMDQ) is a valid tool to assess WMSDs, but is not available in the local language of Sri Lanka (Sinhala).
OBJECTIVE:
To cross-culturally adapt the original CMDQ from English to Sinhala and evaluate its psychometric properties.
METHODS:
The linguistic and cultural adaptation of the CMDQ to the Sinhala (Si-CMDQ) language followed international guidelines. The adapted pre-version was tested for comprehensibility among 32 subjects from different educational and occupational backgrounds. The Content Validity Index (CVI) was computed with ratings from five experts. The questionnaire was validated further by 111 security guards employed at the university. The tool was validated with reference to the Numeric Rating Scale. Test-retest reliability was assessed at two time points one week apart and internal consistency was tested.
RESULTS:
The Si-CMDQ showed adequate cross-cultural, content and construct validity, internal consistency, and test-retest reliability. The Kappa coefficient showed excellent agreement between NRS and Si-CMDQ frequency scale. Spearman’s correlation coefficients showed a moderate to a strong significant positive correlation between NRS and the severity scale of Si-CMDQ. The Kappa values for test-retest reliability were moderate to excellent for the three scales of CMDQ. The internal consistency was high.
CONCLUSION:
The Si-CMDQ fulfilled the psychometric requirement for questionnaires. This tool will be beneficial to assess WMSDs among sedentary workers in different occupations in Sri Lanka.
Introduction
Musculoskeletal disorders are among the major health-related complaints among people of different age groups, occupations, and communities [1–3]. Musculoskeletal disorders can be pain or discomfort or reduced function in various regions of the body from head to toe [3]. It is often observed that most people develop musculoskeletal disorders associated with their profession. These disorders are classified as work-related musculoskeletal disorders (WMSDs).
WMSDs are observed across a variety of occupations. A high prevalence of WMSDs is observed in professions that involve a significant amount of physical exertion. WMSDs are commonly observed across a variety of professions such as carpenters, with a prevalence of 20-24% [4], hairdressers, with a prevalence of 63% [5], surgeons, with a prevalence of 37% [6], physical therapists, with a prevalence of 68% [7], nurses, with a prevalence of 89% [8], and dentists, with a prevalence of 61% [6]. The WMSDs are associated with posture, type of movements, and frequency of movements involved in the job. Repetitive movements, stressing the same body parts repeatedly, improper postures, prolonged positions, and job stress are some of the common causes of WMSDs [9, 10].
Both the employee and employer are affected by the prevalence of WMSDs. Significant loss of productive time at work and reduced performance are observed among brick workers [11], sewing workers, postal staff, computer operators, and nurses [12] who suffer from WMSDs in Sri Lanka. Employees with WMSDs might feel pain and discomfort during working hours which might jeopardize their work performance and quality. Other concerns about the WMSDs effect on employees are absenteeism. Several studies have found that WMSDs cause an increase in days of sick leave being observed across many workplaces [13–15].
Previous studies in Sri Lanka have assessed the prevalence of WMSDs among people involved in occupations such as tea pluckers [16], nurses [17], rubber tappers [18], computer operators, and sewing workers [12]. However, there is a wide range of occupations that are sedentary in nature in Sri Lanka that have not been explored yet. These occupations include teachers, academics in various work settings, university students, office workers, various desk jobs, security personnel, drivers, etc. The data collection tools used in the previous studies in Sri Lanka were interviewer-administered questionnaires developed by the research team [11]. In another study, four occupations were assessed using the CUPID questionnaire, which was interviewer-administered and assessed six anatomical regions for MSDs and the cultural and psychosocial influences. However, this tool was not validated in Sinhala and only a few steps of forward translation and back translation were followed [12]. It is evident that there are many occupations and employees that still require assessment for WMSDs, to identify disorders and address them in a timely manner. Future studies in Sri Lanka will be benefitted from the availability of a validated, feasible, and easy-to-understand tool in the local language. The researchers believe that the translation and cultural adaption of a valid tool will make it available in the local language for wide use among researchers, employers, and administrative authorities or groups that would intend to assess WMSDs.
Assessment Tools for WMSDs
Assessment tools are essential to identify the WMSDs. They help recognize the disorders at an early stage or even before they evolve. The risk of developing a disorder can be pointed out by an effective assessment tool. Studies suggest that there is a need for a holistic assessment tool that can be used to recognize both musculoskeletal disorders and their potential risk factors [19]. There could be various backgrounds to WMSDs, and its’ presentation is wide, therefore, the assessment tools should be able to assess a wide range and be specific, reliable, and valid. Though the numeric rating scale and visual analog scale are used to identify musculoskeletal disorders they fail to assess the function and work-related activities [20]. Although self-reported physical disability questionnaires are available such as the Roland-Morris disability questionnaire and the Oswestry disability questionnaire, they are confined to low back pain [21]. The Nordic Musculoskeletal Questionnaire (NMQ) focuses on comparing low back, neck, shoulder, and other complaints for epidemiological study purposes but not for clinical use.
The Cornell Musculoskeletal Discomfort Questionnaire (CMDQ)
When compared with the questionnaires described earlier, the CMDQ explores pain and discomfort throughout a wide range of body regions. It further asks about the frequency of pain, discomfort level, and interference with work [22]. Furthermore, the CMDQ is comprised of a single page, with well-presented diagrams for males and females, in a manner that the reader can understand easily and fill within a short period of time. CMDQ is applicable for professions ranging from desk jobs to professions that require a lot of physical exertion. Therefore, the CMDQ is a fair questionnaire to assess WMSDs.
The original CMDQ comprises 11 body regions marked with pointers, of these regions seven regions have further categorization as ‘right’ and ‘left’. The questionnaire comprises three scales- frequency, severity, and work interference and it assesses discomfort experienced during the previous week. The questions asked in the frequency scale include: ‘During the last week how often did you experience ache, pain, discomfort?’ and has 5 options: Never, 1-2 times last week, 3-4 times last week, once every day, several times every day. The question for the severity scale reads as: ‘If you experienced ache, pain, discomfort, how uncomfortable was this?’ and has 3 options: slightly uncomfortable, moderately uncomfortable, and very uncomfortable. The question included in the work interference scale is: ‘If you experienced ache, pain, discomfort, did this interfere with your ability to work?’ and has 3 options: Not at all, slightly interfered, substantially interfered. The options in the scale are scored as: Frequency scores: 0,1.5, 3.5, 5, 10, Severity scores: 1, 2, 3, Work interference scores: 1,2,3. Higher scores on each scale represent greater frequency, severity, and work interference. The method of scoring the questionnaire is to simply multiply the scores obtained in the 3 scales for each anatomical region. The developers stated that the studies that use the tool must determine the test-retest reliability for their study. The validity of the original tool was not determined in the US; however, it has been validated in different languages and has shown good validity and reliability.
The CMDQ was initially formulated in the English language [22]. Translated versions are available in languages including German, Turkish, and Iranian [23–25]. The readiness of the tool for use in local languages will enable wider and more effective use of the tool to identify work-related musculoskeletal discomfort among people in various occupations that are sedentary in nature. Sinhala is the language spoken by a majority (75%) of the Sri Lankan population which is 2.1 million [26]. There is need for a Sinhala version of the CMDQ to assess WMSDs among the Sinhala speaking population.
This study aimed to translate the CMDQ into Sinhala language to enable the Sinhala speaking population to gain the benefits of using the tool and the opportunity to be assessed for WMSDs using a validated and reliable self-reporting questionnaire. This was the first study in Sri Lanka to conduct cross-cultural adaptation and validation of the CMDQ for sedentary workers in Sinhala language.
Methods
Cross-cultural adaptation
Permission was obtained from the developer of CMDQ, Prof. Alan Hedge to translate it to the Sinhala language. The guidelines for cross-cultural adaptation were followed, including forward and backward translations [27, 28]. The questionnaire was translated into Sinhala from the English version.
Forward translation
The questionnaire was translated from English into Sinhala by two professionals who worked independently of each other and whose native language was Sinhala. One of them was familiar with the concept of the questionnaire. The other was a lecturer with a Physics background who was not familiar with the concept of the questionnaire. Both of their native languages were Sinhala. The differences in the written reports were checked against the original questionnaire and against each other regarding content, terminology, and language to arrive at the preliminary version. In this process, the two translators and two other individuals were involved. Of the two other individuals, one was a physiotherapist and the other was a technical staff with no knowledge of the concept of the questionnaire and was involved in recording the discussions.
Backward translation
This version was translated back to the original language by two individuals, of which one resides in Australia and is a citizen of Australia, but his native language is Sinhala, and the other individual has lived in the US for over 5 years and works as an English Instructor in the University, her native language is Sinhala too. The discrepancies between the original version, the translation, and the backward translation were discussed and sorted through discussions between the translators and two practicing physiotherapists, who understood the intent of measure and concepts of the questionnaire.
Content Validity Index (CVI)
After this, the questionnaire was given to 5 experts, comprising 2 medical doctors, 2 working physiotherapists, and a lecturer teaching physiotherapy to calculate the CVI. The CVI values vary according to the no. of experts in agreement. Accordingly, the acceptable item-level CVI for 3 to 5 experts is 1, and a scale-level CVI value of more than 0.80 is considered acceptable. To compute the item-level CVI, the number of experts in agreement was divided by the total number of experts. The scale-level CVI was calculated by computing the average of item-level CVI scores across all items. The item-level CVI for all items was 1 and the scale-level CVI was 1 [29]. Hence, the values for both item-level CVI and scale-level CVI were in the acceptable range.
Furthermore, the experts mentioned that the questionnaire was intended to assess musculoskeletal discomfort among sedentary workers who could experience aches, pain, or discomfort in the hand, foot, and ankle as well. However, the original questionnaire did not have the option to choose these body regions. This suggestion was conveyed to the developer of the questionnaire, Prof. Alan Hedge and he consented to add the body regions. Further, adding the body regions: hand, foot, and ankle to the questionnaire did not affect the scoring of the questionnaire because the scoring of the questionnaire involves grading each body region for frequency, severity, and work interference. Hence, adding the body regions would enable the identification of frequency, severity, and work interference for these body regions as well and would not change the scoring system or total score described by the developer.
Also, it was suggested that nude body diagram may not be acceptable in the Sri Lankan culture and clothed diagrams should be used. These suggestions were conveyed to the original developer of the Questionnaire, Prof. Alan Hedge, and permission was obtained to incorporate these changes.
Following this, the pre-final Sinhala version was developed. The graphics used in the Sinhala version were developed considering ethical values relevant to the Sri Lankan community and it was pretested.
Pre-test
The Sinhala version of the CMDQ for sedentary workers was pretested among 32 subjects because a sample size between 30 and 50 participants enhances the probability of detecting problems, like unclear questions, and unfamiliar words [30]. The CMDQ is a tool to assess WMSDs, hence, the pre-final version was pre-tested among a sample comprising a wide age range, different educational levels, and different occupations to assess the readability and understandability of the pre-final version. The age of the native Sinhala speakers ranged between 21 and 66 years and they were involved in different occupations such as: cleaning staff, typesetters, office employees, demonstrators, and computer analysts.
The subjects were met at their workplace, the pre-final version of the Si-CMDQ was given and they were asked to fill out the questionnaire and to mention any difficulties in the questionnaire’s structure, readability, and understandability of terms. The filled questionnaires were assessed for completeness and inconsistent findings. The subjects were instructed to fill in responses for all anatomical regions. If they did not have any ache, pain, or discomfort in a body region, they had to mark ‘Never’ in the frequency scale. It was expected that if a subject indicated pain or discomfort for a body region, they must mark the relevant options for severity and interference scale as well.
All subjects involved in the pre-test stated that the content of the questionnaire was readable and understandable, some of them mentioned that the font size was small. Only one subject out of all 32 subjects indicated the frequency of pain and severity but did not check any response for work interference for the same anatomical region. This was thought of as the subject’s perception of interference with work, despite the pain. All other responses were consistent between the three scales of the questionnaire. Hence, as pointed out by a few subjects the font size was increased in the final version, which was used for validation of the questionnaire.
Validation
Sample
The developed Sinhala version of the CMDQ was given to security guards working at the University of Peradeniya, Sri Lanka. There are 119 University security guards, and six of them were not willing to partake in the study. Hence, the tool was given to 113 security guards for validation. Of the 113 security guards, 12 were female and the rest were male. They were between the ages of 30-60 and their educational qualification was Ordinary level (O/L), Advanced Level (A/L), or a degree. Initially, the subjects were met at their workplace, the procedure of filling in the questionnaire was explained clearly and they were allowed to seek clarifications, if any. This procedure was repeated after one week and the subjects were requested to fill in the questionnaire for the second time.
Concurrent validity assessment
The Numeric Rating Scale (NRS) is a validated and reliable tool to assess pain severity [31]. Therefore, this study included the NRS to test the validity of the Sinhala version of the CMDQ (Si-CMDQ). The NRS tool has points between 0-10, where ‘0’ indicates no pain and ‘10’ indicates most severe pain. The subjects had to mark the NRS for all body regions that were included in the Si-CMDQ. The security guards were asked to fill the Si-CMDQ and the NRS on the same day. They had to mark the number indicating the intensity of pain on the NRS and they had to fill the Si-CMDQ. Then, the responses from both tools were assessed to determine the validity of Si-CMDQ. In the NRS tool, the subjects could mark a score between 0-10. In the frequency scale of Si-CMDQ, they had to mark one of the five options between ‘Never’ to ‘several times each day’ and the scores range for the five options were as follows: 0,1.5, 3.5, 5, 10. It was expected that if a subject marked ‘0’ in the NRS, which would indicate that the subject had no complaint of pain, he/she should mark ‘Never’ under the frequency column of Si-CMDQ. Similarly, if they indicated a score for pain in the NRS, they were expected to choose an option other than ‘Never’ in the frequency scale of Si-CMDQ.
To assess the association between the NRS and the severity scale of Si-CMDQ, it was expected that the scores of the two tools should correlate positively. To assess this correlation Spearman’s correlation test was used. The study that carried out translation and validation of the CMDQ in the German language also used the NRS to determine validity [23].
The strength of agreement between NRS and the frequency scale of Si-CMDQ was statistically analyzed by Kappa coefficients (k). According to Landis and Koch, Kappa values between 0.00 –0.2 are slight, 0.21 –0.4 are fair, 0.41 –0.6 are moderate, 0.61 –0.8 are substantial and 0.81 –1 are excellent [32]. Similarly, the correlation between NRS values and the severity scale of the Si-CMDQ was analyzed using Spearman’s correlation. These values were interpreted as weak if the value was between 0.1 to 0.3, moderate if it was between 0.4 to 0.6, strong if between 0.7 to 0.9 and it was perfect if the value was between 0.9 to 1 [33].
Reliability assessment
The Si-CMDQ was given to 113 security guards working at the University of Peradeniya, Sri Lanka. Each security guard had to fill out the Si-CMDQ at an interval of 7 days (one week) to assess the test-retest reliability to determine the reliability of the tool when given at two different time points. The 7-day interval was decided to compromise the memory bias and clinical alteration [34]. It was made sure that none of the participants sustained injuries or initiated any form of intervention during this time gap. Test-retest reliability for the frequency, severity, and work interference scales was analyzed using the Kappa coefficient. According to Landis and Koch, Kappa values between 0.00 –0.2 are slight, 0.21 –0.4 are fair, 0.41 –0.6 are moderate, 0.61 –0.8 are substantial and 0.81 –1 are excellent [32]. The internal consistency for frequency, severity, and work interference was assessed using Cronbach’s Alpha statistics.
Ethical approval
Ethical approval for this study was obtained from the Ethics Review Committee of the Faculty of Allied Health Sciences, University of Peradeniya (AHS/ERC/2021/070). Informed consent was received from each participant who was recruited in the study.
Data analysis
The data analysis was conducted using SPSS Statistics v.26. To assess concurrent validity, Kappa coefficient was determined to analyze the strength of agreement between NRS and the frequency scale of Si-CMDQ. Simultaneously, the correlation between the NRS and the severity scale of the Si-CMDQ was analyzed using Spearman’s Correlation Test. To assess the test-retest reliability for the scores obtained for frequency, severity, and work interference scales between the two time points, Cohen’s Kappa coefficient was computed. Internal consistency was assessed using Cronbach’s Alpha statistics.
Results
Sample
Out of 113 respondents, 111 (98.2%) of them were included in the analysis. Of the 111 subjects, 89.1% were male and the rest were female. The age range of the subjects was between 26 to 60 years and the mean age was 46.37±7.7. When considering the educational qualification, 62.2 % of the subjects had low-level educational qualifications, 36.9% of subjects had intermediate-level qualifications and only one subject (0.9%) had completed a degree.
Concurrent validity
The Kappa value for the strength of agreement between NRS and the frequency scale of Si-CMDQ ranged between 0.92 –0.98. The strength of agreement was excellent in 100% values of the Kappa coefficient between the frequency scale of Si-CMDQ and NRS. Further, the scores of the severity scale of Si-CMDQ showed a positive correlation with the NRS scores, the strength of correlation ranged from 0.41 to 0.78. This showed that there was a moderate to <s>a< /s>strong correlation between the severity scale of Si-CMDQ and NRS. There was a moderate correlation for the right and left shoulders, right and left upper arm, right forearm, right and left wrists, right and left-hand joints, upper back, lower back, right and left thigh, hip/buttocks, right and left knee, right and left lower legs, right and left ankle, and right foot (87.5%), and there was a strong association seen for the neck, left forearm and left foot (12.5%) (Table 1).
Validity Results (n = 111)
Validity Results (n = 111)
**p<0.001.
The Kappa coefficient ranges for the strength of agreement between test and retest values were 0.53-0.89, 0.52-0.93, and 0.56-0.96 for frequency, severity, and work interference scales of Si-CMDQ respectively (Table 2). The strength of agreement for the frequency scale on two different time points was moderate for the neck. There was a substantial agreement for right and left shoulders, upper back, right upper arm, lower back, right and left wrists, right and left-hand joints, hip/buttocks, right thigh, right and left knees, right and left lower legs, right ankle, right and left feet. While, the left upper arm, right and left forearm, left thigh, and left ankle showed excellent strength of agreement.
Reliability Results (n = 111)
Reliability Results (n = 111)
When considering the severity scale, the upper back and right lower leg showed moderate strength of agreement. Neck, right shoulder, right upper arm, lower back, left forearm, right and left wrists, right carpal joints, hip/buttocks, right thigh, right and left knees, left lower leg, and right and left feet showed substantial strength of agreement. There was excellent strength of agreement for the left shoulder, left upper arm, right forearm, left-hand joints, left thigh, and right and left ankles.
Further, for the interference scale, the right wrist, hip/buttocks, and right and left feet showed moderate strength of agreement. There was a substantial agreement for right and left shoulders, upper back, right and left upper arms, lower back, left for arm, left wrist, right and left-hand joints, right and left thighs, right and left knees, right and left lower legs, and right ankle. The neck, right forearm, and left ankle showed excellent strength of agreement.
Accordingly, the agreement between the responses on two different time points for the three scales of the Si- CMDQ was adequate and acceptable. The details of test-retest reliability are presented in Table 2, the internal consistency values for Cronbach’s Alpha for the frequency, severity, and interference scales were 0.91, 0.87, and 0.89 respectively. Thus, the internal consistency for the 3 scales of Si-CMDQ was reliable and strong. The results of internal consistency for the frequency, severity, and work interference scale are presented in Table 3.
Internal Consistency Results (n = 111)
This research focused on cross-culturally adapting the original version of the CMDQ to a Sinhala version and validating it, thus, enabling the Sinhala-speaking population to use the Si-CMDQ for research and clinical purposes, which is their native language. A few changes that were made to the original CMDQ include: clothed body diagrams for the male and female versions of the Si-CMDQ and the inclusion of pointers for hand, ankle, and foot in the image of body regions. The Si-CMDQ is presented in Figs. 1 and 2 depicting male and female diagrams respectively.
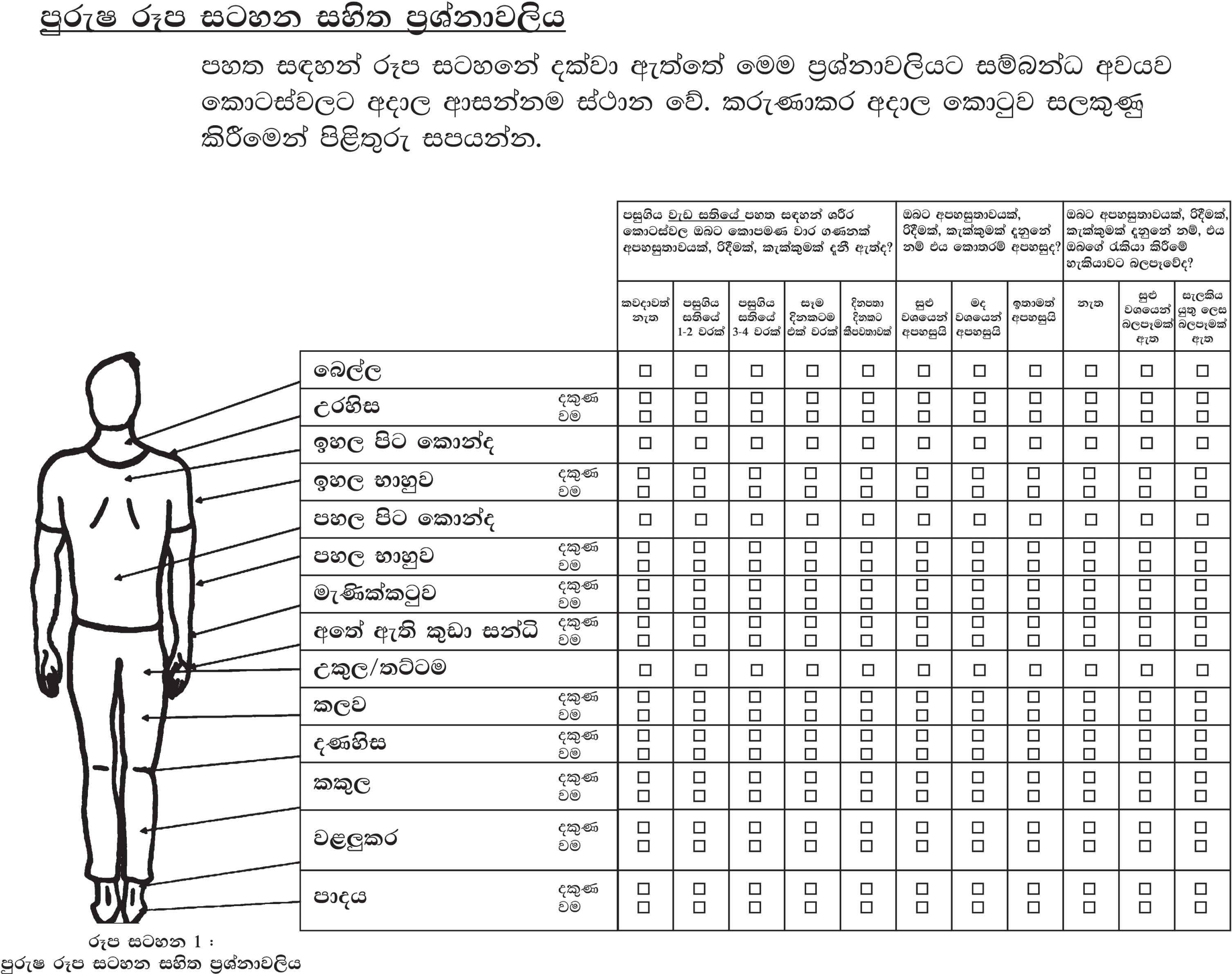
Male version of the Si-CMDQ for sedentary workers.
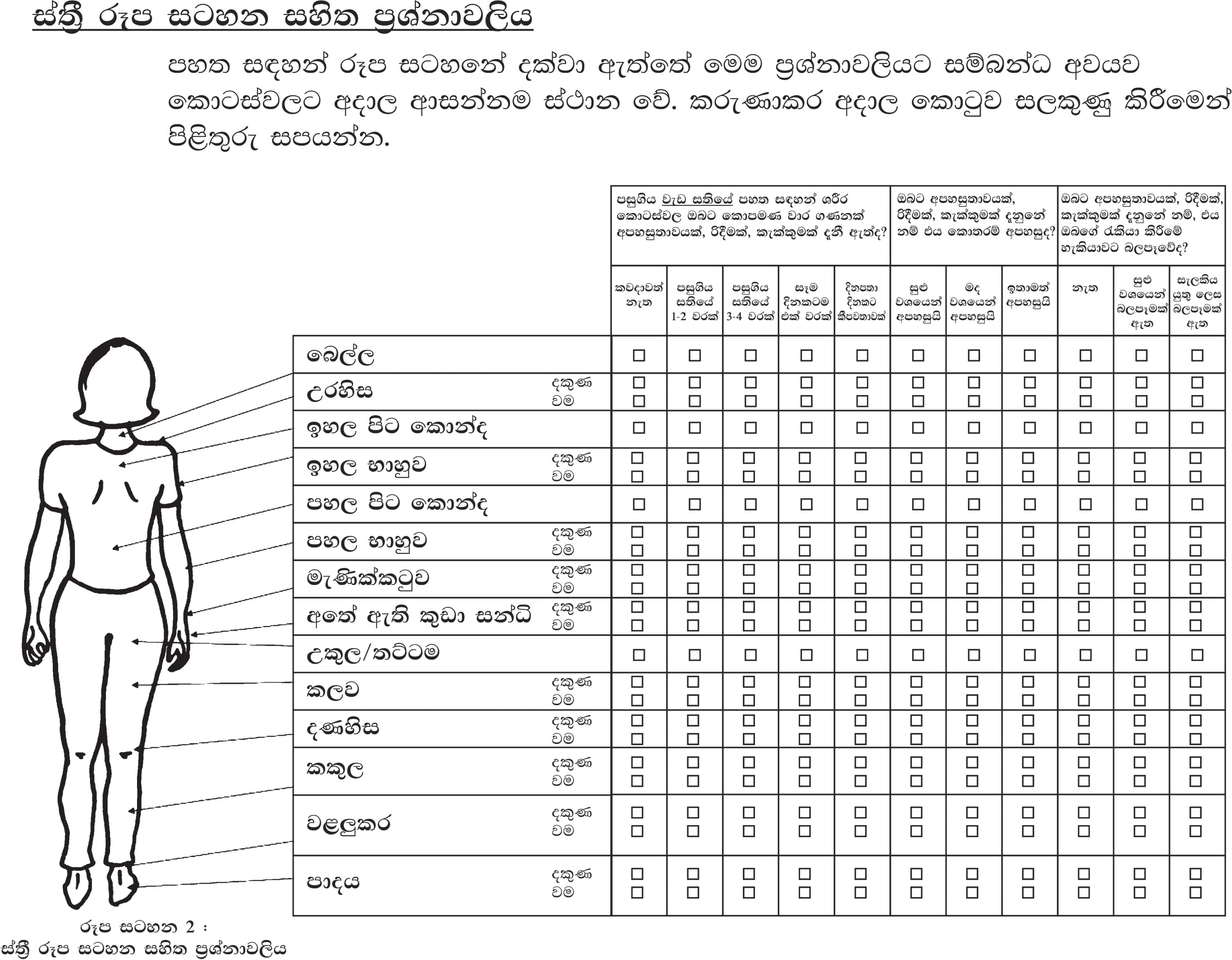
Female version of the Si-CMDQ for sedentary workers.
The individuals involved in the forward and backward translation procedures were professionals with excellent proficiencies in English and Sinhala language. The guidelines for cross-cultural adaptation were followed throughout the formulation of the Sinhala version of the CMDQ [27, 28]. After the initial translation procedure, the Si-CMDQ was shared with experts for their comments and suggestions, it was modified accordingly, and a pre-version was prepared. In accordance with the suggestions and with permission from the original developer, the body images were presented as clothed images that made the tool more culturally acceptable. The experts suggested that the image in the questionnaire did not provide a chance for the subjects to present pain or discomfort in the hand, ankle, and foot, although sedentary workers could present with complaints in these body regions as well. Pointers were added for the hand, ankle, and foot in the body image in the Si-CMDQ. Similarly, in the German version [23] elbow and foot have been added in addition to the body regions given in the original questionnaire. Thereafter, the pre-version was pretested and the final satisfactory version of the Si-CMDQ was drafted.
The previous translations of the CMDQ concluded that CMDQ is a valid and reliable tool to assess WMSDs. Studies have shown that the NRS and VAS are highly associated [35]. The Turkish and Iranian versions of the CMDQ used the Visual Analog Scale (VAS) to determine concurrent validity. The German version used the NRS to assess concurrent validity [23]. To determine the concurrent validity of the Si-CMDQ the NRS was used. To check the association between the NRS and the frequency scale of the Si-CMDQ, if a subject marked ‘0’ on the NRS across a body region it indicated that they had no pain in the body region, accordingly, it was expected that they should mark ‘never’ under the frequency scale of Si-CMDQ, which would indicate no ache, pain, or discomfort. The strength of agreement in the responses for the two tools was assessed using the Kappa coefficient and the results revealed excellent strength of agreement between NRS and the frequency scale of Si-CMDQ (Table 1). All body regions showed excellent strength of agreement between the frequency scale of Si-CMDQ and NRS. In the German study, 39% of body regions showed very high and high strength of agreement, 17% revealed moderate agreement and 4% showed low agreement. These results showed that the CMDQ is a valid tool across different languages.
The association between the NRS and severity scale of the Si-CMDQ was assessed using Spearman’s correlation test and a positive correlation was expected between the scores. This positive correlation was noted in both the German and Sinhala versions [23]. In the German version of the CMDQ, there was a statistically significant correlation between the CMDQ and the NRS in most joints. In the present study, there was a significant positive correlation between the scores for NRS and the severity scale of Si-CMDQ for all body regions ranging from moderate to strong association. The correlation was strong for the neck, left forearm, and left foot. The correlation was low for the right forearm, right wrist, hip/buttocks, right thigh, and right ankle. All other body regions showed moderate correlation (Table 1).
The test-retest reliability for Si-CMDQ was satisfactory. The strength of agreement for frequency, severity, and interference scales ranged from moderate to excellent (Table 2). The values were moderate for body regions such as the neck, upper back, right wrist, hip/buttocks, right lower leg, and right and left feet. It can be observed that the correlation was moderate for only one scale at a time for a body region. A reason for this could be the difference in perception of the subject about frequency, severity, or work interference for the body region during the second time point of assessment. Perhaps the duty shift hours (12 or 24 hours) and rest between shifts during the previous week influenced the perception of severity and work interference. All other parts showed substantial or excellent strength of agreement. Similarly, the Kappa coefficients for frequency, severity, and work interference ranged between 0.56–0.95, 0.56–0.97, and 0.59–0.94 for the Turkish version and 0.75, 0.77, and 0.82 for the German version [23, 24]. The values for Si-CMDQ ranged from 0.532-0.897, 0.526-0.938, and 0.563-0.967. The values for the strength of agreement assessed by the Kappa coefficient show that the Si-CMDQ is a reliable tool like the other language versions.
The Cronbach’s Alpha values for all three scales of the Si-CMDQ were high and the internal consistency was good (Table 3). Likewise, good internal consistency was observed for frequency, severity, and the work interference scale 0.88, 0.89, and 0.88 respectively in the Turkish and it was good in the German version too: 0.75, 0.77, and 0.82 [23, 24].
Further, previous studies that translated and validated the CMDQ insisted on the importance of further studies assessing the validity and reliability of further versions of the CMDQ [23–25]. Therefore, this study has contributed to adding value to the CMDQ based on validity and reliability. The Si-CMDQ will help to identify the existence of musculoskeletal pain throughout the 24 body regions (including the right and left sides, where appropriate). The severity of pain and its interference with work can also be assessed using the Si-CMDQ. This assessment tool is self-administered, precise, specific, and clear to the reader. The Si-CMDQ focuses on the neck, shoulder, upper arm, forearm, wrist, hand, upper back, lower back, hip/buttocks, thigh, knee, lower leg, ankle, and foot. As the parts are clearly mentioned and shown in the diagram the subjects will find it easy to communicate his/her pain experience through the Si-CMDQ.
This study is the first to translate and validate the CMDQ in the Sinhala language. The tool is easy to understand and easy to administer. The validation of this tool is a valuable contribution to the field of research in Sri Lanka because it will enable researchers to use the tool in the local language. Also, the tool can be used by employers and other administrators for assessment among large samples to identify WMSDs. This tool will be beneficial for the initial identification of WMSDs, as a follow-up to which further assessments and interventions can be formulated and as required interventions and strategies can be planned and implemented. This study does possess certain limitations such as, the sample of this study were security guards working at the University, they could be easily approached by the research team. Considering the type of job of the security guards, with 24 hours and 12 hours shifts, data was not collected on the same day and time. This may have influenced the nature of the information provided by the security guards. In this study, the Si-CMDQ was validated using the NRS which is also a self-administered tool. Instead, future studies can consider involving clinical reports to check the validity of the Si-CMDQ. Also, another limitation of the study is that only one job category was included for validation of the questionnaire, and the sample comprised mostly male candidates with very low female representation.
Our findings showed that Si-CMDQ has good psychometric properties. This was the first study in Sri Lanka to translate and validate the CMDQ in the Sinhala language. The cross-cultural adaptation and validation of the CMDQ in the Sinhala language have led to the availability of a valid tool to assess work-related musculoskeletal discomfort in the local language, this, in turn, will enable researchers, healthcare professionals, employers, and employees in various occupations to use the tool to identify work-related musculoskeletal discomfort. The Si-CMDQ can also be used to assess the effect of ergonomic interventions in minimizing the occurrence, severity, and interference of work-related musculoskeletal pain.
Ethics statement
This study was conducted in accordance with the principles of the Declaration of Helsinki. Ethical approval was obtained from the Ethics Review Committee of the Faculty of Allied Health Sciences, University of Peradeniya (AHS/ERC/2021/070). Informed consent was obtained from all participants included in the study.
Funding
This study received no funding or grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors do not have any competing interests to declare.
Footnotes
Acknowledgment
The authors would like to thank the participants, expert committee members and translators in this study for their contributions. They also wish to extend their gratitude to Ms. Asil Rajaratne, an Australian citizen, reading Bachelor of Animal Science & Zoology, Deakin University, Melbourne Australia for proofreading the manuscript for English language.
Si-CMDQ (Male Image) with English text
Original Cornell Musculoskeletal Discomfort Questionnaire - Sedentary Workers,Male image
© Cornell University, 1994