
Abstract
BACKGROUND:
Parents often use baby walkers (BWs) as assistive devices to improve their infants’ independent movement and motor skill acquisition. However, the literature suggests that conventional baby walkers (CBW) may cause delays in an infant’s ability to walk independently and musculoskeletal burden on parents.
OBJECTIVE:
In the current study, a baby walker (RBW) with chest support was redesigned and ergonomically assessed during an infant-walking task.
METHODS:
The anthropometric dimensions of 90 infants aged 7–11 months were measured in the city of Urmia, northwestern Iran. Following redesigning based on the results from expert panel meetings and prototyping of the RBW, 18 mothers (age: 28.33±4.27 and height: 163.75±5.32 and weight: 59.45±5.99) with their infants (9 boys and 9 girls) performed a simulated infant walking task in two experimental sessions using the CBW and RBW over a repeated measurements design. The infants’ feet track patterns, including the number of steps and step distances were assessed via the image analysis of the footprints. The mothers’ body posture and lower back spinal load were evaluated using Rapid Upper Limb Assessment (RULA) technique and 3D Static Strength Prediction Program (3DSSPP), respectively.
RESULTS:
Wilcoxon signed-rank tests showed infants walked more steps with the RBW (p = 0.002). Similarly, the distance between the infants’ left heel strike (p = 0.008) and their right and left toe-off (p = 0.03 and 0.02 respectively) was also significantly lower in the RBW use. Additionally, the body posture of mothers was improved (RULA final score from 7 for CBW to 5 for RBW). Moreover, lower back compression and shear forces were reduced significantly (p = 0.002) by the RBW use.
CONCLUSION:
According to the feet track pattern, infants took more balanced steps when the RBW was used. In addition, mothers were subjected to less pressure on the lumbar region when they placed and lifted their infant from the RBW. However, further work is necessary to investigate potential long-term effects of the RBWs use.
Introduction
Child growth is a complex physical and cognitive process [1]. Motor skill acquisition is one of the most critical processes and falls into two categories: fine motor and gross motor. Tiny gestures in the hands, wrists, fingers, feet, toes, lips, and tongue refer to fine motor skills. Gross motor skills regard muscle growth that allows babies to keep their heads up, sit, crawl, walk, run, and jump [2]. Children need to be supported by their parents to improve their skills [3], especially their mothers who often use assistive devices such as baby walkers (BWs) to improve their infants’ independent movement and motor skill acquisition [4, 5].
A BW is an assistive device that can be used by infants who cannot walk independently to move from one place to another. Studies reported that over 50% of parents of infants less than 12 months use BWs offer a BW for their infant [6–9]. Using BWs depends on parents’ social and cultural experiences [5]. Most parents use a walker because they believe it will help the infant achieve the milestone of independent walking earlier [9], and approximately 70% of the parents think the use of BW’s promotes motor skill acquisition of the child [10]. BWs usually are designed as seated or chest support walkers. Seated walkers have wheelbase frames and assist babies to move around freely [11]. Moving freely causes falls of infants from steps or allows access to dangerous areas and objects, including electrical cords, cleaning supplies, fireplaces, etc. On the other hand, chest-support walkers with straps or handheld harness are controlled by the parents, meaning that infants cannot move independently [12, 13].
Nonetheless, despite the parents’ beliefs and perceptions, using BWs may cause delays for infants to walk independently as they turn their trunks forward and put their feet in a plantar-flexed position to move around [14, 15]. A lower gait speed and a longer period of the stance and swing phases was found in BW users compared to non-users [16]. Bezgin et al. 2021, reported that using a baby walker delays motor skill acquisition by poorly affecting trunk balance [17]. Also, concerns have been raised over the last three decades about the safety of BWs [18–21]. In general, several studies warn against using BWs [22, 23]. Similarly, the American Association of Paediatrics and other studies advise against using this type of support [20, 24]. It is reported that 12–50% of infant BWs users experienced severe injuries as the BWs are allowing for infants to move around freely [25, 26]. Therefore, when parents choose a BW, they should be sure to look after their infant and be aware of its relative effects.
Another significant concern is parents’ musculoskeletal injuries during handling the infants for caring tasks. Lifting and lowering of the infants from a low height level such as BWs is known as a risk factor for musculoskeletal disorders [27–29]. For instance, [30] highlighted this risk factor by considering child’s weight, parent’s grip on the child, horizontal reach lengths, vertical lift distances, trunk rotation over 45 degrees and the combination of rotation and side bending during caring duties. Furthermore, imbalanced lifting of loads in awkward posture stretches the passive muscles of the lumbar spine and increases the risk for low back injuries.
To the best of the authors’ knowledge, no study has investigated the effects of the use of two different designs of baby walkers on infant walking patterns and on parents. Accordingly, driven by the research cited above about the drawbacks of using BWs and considering that they are still used widely, in the current study we aimed to (1) design a chest-support walker, (2) assess infants’ feet track pattern, and (3) ergonomically assess mothers body posture and lower back stress during CBW andRBW use.
Methods
An experimental study was carried out to compare two types of BW in a simulated infant walking task. In the first phase of the research, a walker was designed and prototyped. In the second phase, the redesigned baby walker (RBW) and conventional baby walkers (CBW) were ergonomically assessed during a simulated infant walking task. The study was approved by the Research Committee of Iran University of Medical Sciences (code IR.IUMS.REC.1398.997).
Overview of baby walker redesign
To identify factors that should be considered in the redesign of the BW with acceptable and usable characteristics, a CBW was provided following sets of initial field evaluation and benchmarking of different BW products. During the field study, interviews with salespersons and customers were done and a CBW was selected based on market popularity among customers, the quality, and the cost of existing walkers. For ethical reasons, the product’s brand and type cannot be disclosed. Next, a panel of experts was formed to identify the required characteristics for redesigning the BW. The panel members were invited by emails and/or direct phone calls based on a convenience sampling strategy.
The panel included a senior industrial design experts with 5 years of work experience in baby walker and stroller design, three ergonomics specialists with 5–8 of work experience in ergonomic design [31, 32], three mothers with caring responsibilities for children up to three years old, and two paediatric psychologists with 6–10 years of experience. Following the kick-off meeting for acquaintance and planning purposes, during a discovery meeting, the members were asked to write on sticky notes their ideas about features and characteristics of an acceptable and usable BW. Next, all notes were posted, and each comment was discussed. The panel selected six factors through voting and consensus: product and usage safety, Iranian infant’s anthropometric dimensions (age range of 7–11 months), infant motor skills acquisition, musculoskeletal burden on mothers and feasibility of fabrication. We held a third meeting to check the reliability of the selected factors and achieve convergent synthesis. All the notes were reviewed again, and we asked the members to add any new items. Subsequently, another factor, “usability” was added, leading to a list of seven factors for redesigning the baby walker.
In the fourth panel meeting, the walker redesign specifications were identified. To ensure the safety of the infant and prevent it from reaching hazardous material, a sliding guard was installed on the BW to limit the infants’ access (Fig. 1, part No. 4). Additionally, the industrial design group suggested using wheels with restricted mobility to prevent infants from free movement. However, due to the lack of sufficient resources, it was recommended to implement this in the final design.
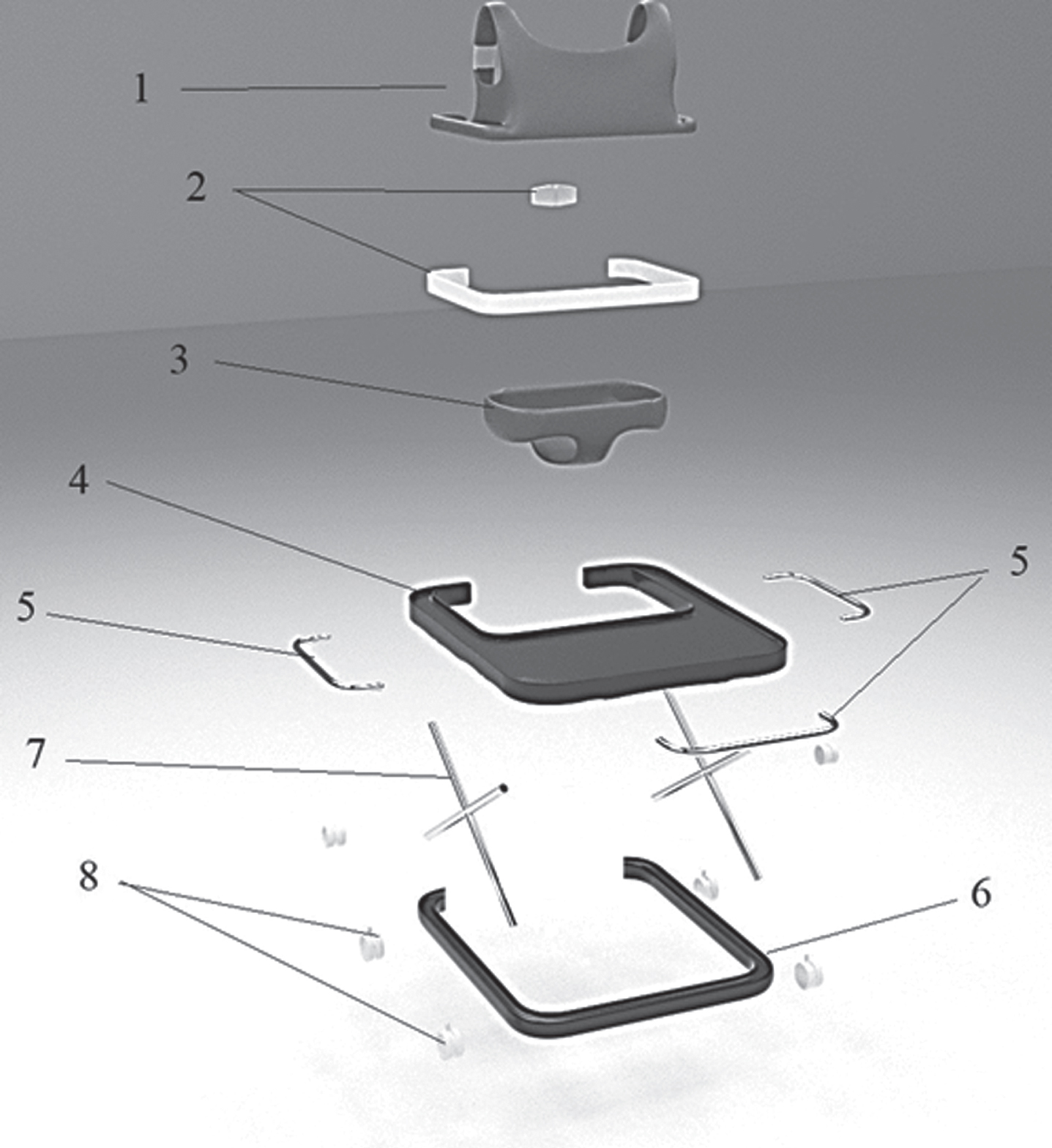
Illustration of the trimetric exploded view of the baby walker prototype, 1) chest support, 2) support clips, 3) seat, 4) upper tray, 5) guards, 6) lower tray, 7) frame, 8) wheels.
To assist infants’ motor skills, the panel suggested transferring infants’ weight supporting place from the seat part to the armpits and chest. This concept originated from the conventional way parents teach their infant to move by supporting their chest and armpit. This results in complete contact of infants’ feet with the ground while parents control the infants’ weight slightly (such as safety harness). Hence, the chest support associated with the optional baby weight support (seat of the walker) was fabricated and used in the final prototype (Fig. 1-sections 1 and 3). This part included two cotton fabric straps on the shoulder and one strap around the chest. However, a seat was still considered necessary to support infants’ weight during their resting time.
Regarding musculoskeletal risks factors, we considered a mother’s awkward posture and moment arm (i.e., the horizontal distance from the centre of the load (infant) to the mother’s waist) during handling task as risk factors for developing musculoskeletal disorders [33, 34]. With this regard, to reduce the moment arm, the back part (pillar) of the BW (Fig. 1, section 2) was removed. To ensure usability, the basic frame and the overall shape of the baby walker were kept similar to the traditional one [35]. The consideration of anthropometrics is explained in the following section.
The body dimensions of 90 infants in the city of Urmia, northwestern Iran, in the age group of 7 to 11 months were measured based on cluster random sampling. After preparing a complete list of all local health departments affiliated with Urmia Medical University, nine clusters were created to cover all respective districts and 10 infants were selected from each cluster.
The anthropometric data (Table 1) were measured by two ergonomics specialists in Local Health Departments using a tape measure and digital scale (LAIGA model PS3001, Italy) according to the following standard protocol to determine the hand reaching distance, chest support dimensions and height [36] as follows: Stature: infant’s natural height from the top of his/her head to the bottom of one of his/her heels. Grip reach: the distance from the infant’s shoulder axis to the palm. Chest circumference: measured horizontally around the upper body (chest) of an infant at the nipple line. Axillary height: infant’s natural height from the centre of his/her armpit to the bottom of one of his/her heels.
Anthropometric estimates for Urmia infant population aged 7–11 months (N = 90)
Anthropometric estimates for Urmia infant population aged 7–11 months (N = 90)
The design specifications derived from the expert panel were shared with the industrial design team. A primary 3D design was created based on the sample dimensions of the CBW and the infants’ anthropometric data (Table 1). The 3ds MAX Software Version 2020 was used for sketching and 3D modeling [37]. Figure 1 shows the exploded view of the initial sketch, and Fig. 2 shows the 3D renders of the new BW. By considering the components of the CBW, a prototype weighing 3700 g with adjustable height Y: 44.8–60.2 cm was fabricated. Figure 3-part B shows the prototype of the RBW that was used in all ergonomic assessments.
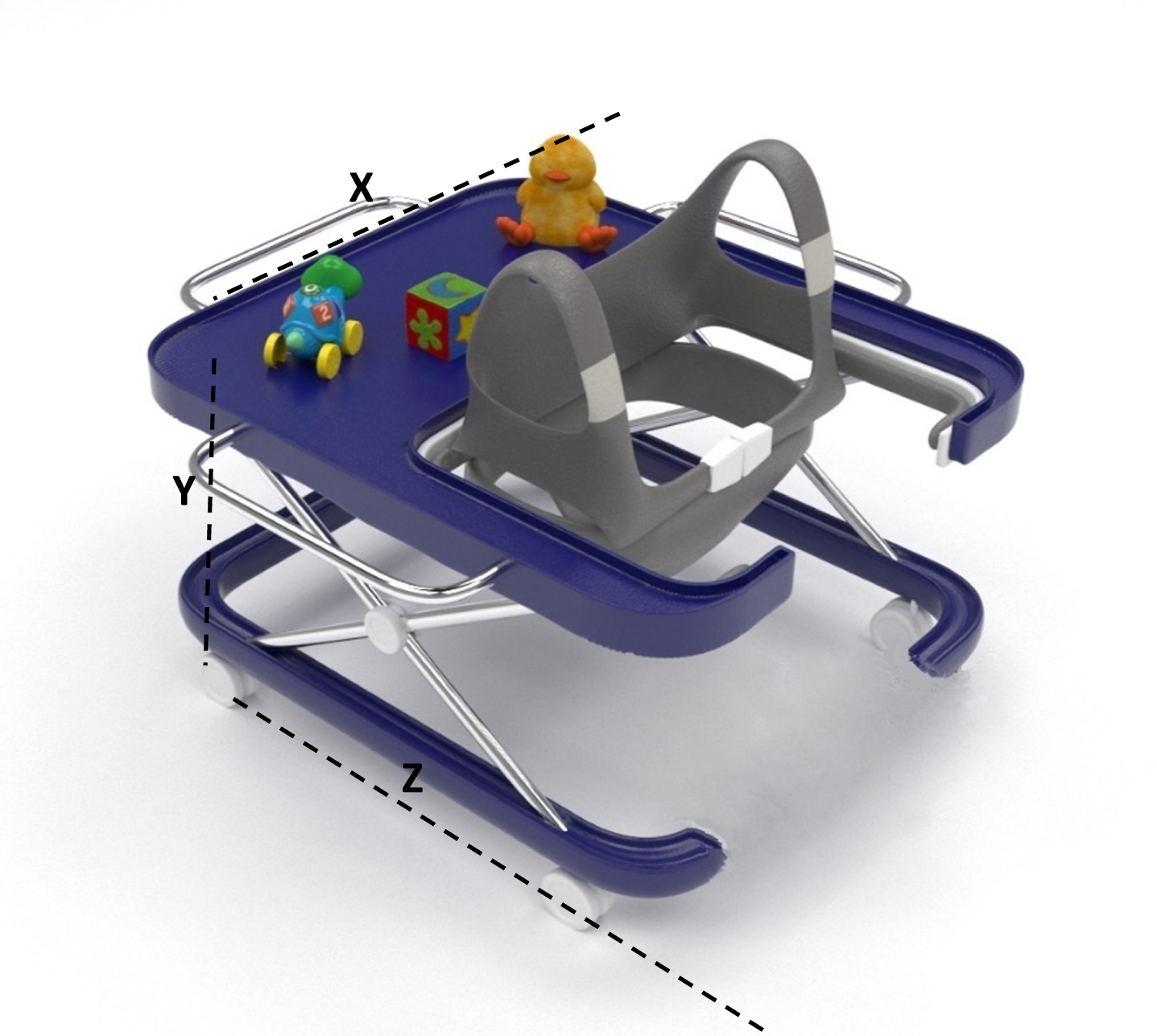
Three-dimensional view of the BW, drawn in 3ds MAX Software. (Y: 44.8–60.2 cm, X: 60 cm, Z: 70 cm).

Illustration of the baby walkers and test setting. A: CBW, B: RBW.
Participants
Eighteen children, nine girls and nine boys randomly selected from the anthropometrics measurement sample (section 2.1.1) with their mothers (age: 28.33±4.27 years; height: 163.75±5.32 cm, weight: 59.45±5.99 kg) participated in the study. Inclusion criteria for infants werethey were breastfeeding, not standing or walking independently, having the ability to sit independently, and no congenital or past medical disorders, including musculoskeletal disorders, disabilities, movement disorders and severe ailment experiences. Inclusion criteria for the mothers was that they were not older than 35 years and had one child. In this study, mothers were selected since in the studied population they are mainly responsible for taking care of infants.
Infant walking tasks
To control the study conditions and analyse mothers’ posture while handling the infants in a BW, the infant walking task was broken down into four subtasks (Table 2) performed using the CBW or RBW per walking task (Fig. 3, A and B).
Infant walking subtasks
Infant walking subtasks
Initially, the mothers were asked to read and sign the informed consent form on behalf of both parents and the infant. Before the test, the mothers were given the study protocol and practiced the infant walking task in each of the BWs. Next, the mothers were asked to perform the baby walking task on a simulated pathway in a private lab. Earlier, a CBW or RBW was randomly placed on the pathway. The pathway was covered by a one-meter whiteboard card. Therefore, under a repeated measurements design, each mother performed the walking task twice, once with CBW and once with RBW, in a random order. Participants were free to perform the walking tasks at their own peace, and between the sessions a 15-min rest time was provided.
Before the test, the seat of the BWs was adjusted to the infant’s stature. To record infants’ walking patterns, the sole of infants’ feet was covered with powder colour [38]. We used green and red colours for identifying feet track patterns in the RBW and CBW, respectively. During the infant’s walking task, the mothers’ posture was videotaped to derive data for the evaluation and simulation through software, and, after each record, the whiteboard card was changed.
Feet track patterns
The feet track patterns on the whiteboards were first photographed at the same distance (2-meter) using a Canon SLR D 600. Then, we measured the number of steps and step distances [Heel Strike (HS), Toe-Off (TO), in both right and left foot, separately] using Matlab image processing toolbox, MATLAB software version R2014a (8.1.0.6.4) [39]. To calibrate the image size, camera catalogue information was used (i.e., an area of one square millimetre per image equal to 5.4×10∨10 pixels) to determine the distances between steps. Since infants’ feet track pattern images was colour mixing, we converted all images to grey scale images (the black and white images). As the particular software is capable of generating a range of image contrast, the borderline of white area and black/ grey area for length measurement was considered as onset and offset of the infant feet borderline (Pixel Based Technique).
Posture evaluation using RULA
Ergonomic risk factors for mothers were assessed through direct observation based on the Rapid Upper Limb Assessment (RULA) technique, which is a observational and sufficiently reliable tool [40, 41]. RULA gives a combined “score A” for the Upper Arm and Lower Arm, a combined “score B” for Wrist, Neck, Trunk and Leg and a “Final Score”. Depending on the combined scores, actions for awkward postures fall in four levels: 1) acceptable posture, 2) further investigation is needed, and changes may be required, 3) investigation and changes are required as soon as possible, and 4) investigation and changes are required immediately. The RULA technique was selected because it comprehensively covers hand grip status and upper body conditions. The main criteria for the worst posture selection in subtasks No 2 and 4 were the awkward posture of the body as determined by the RULA sheet [40].
Two ergonomic specialists carried out the posture assessments, and the worst cases were determined and captured through direct observations of the postural deviations during the experiment. Moreover, two Canon SLR 600D digital cameras were used simultaneously to capture the mothers’ body postures in lateral and front views. The cameras were fixed on the tripods with a 2-meter distance away from the target. The captured postures were used to verify the worst postures determined by the direct observations. The worst posture per walking task was considered the highest limb extension, flexion, and trunkbending.
Lumbar spine forces
To estimate the lumbar spine intervertebral compression/shear force, the worst mothers’ postures according to the RULA worksheets while performing subtasks No 2 and 4 were simulated in the 3DSSPP software version 7.0.6 [42, 43]. The specific software was developed by the University of Michigan to evaluate shear and compressive forces on the lumbar spine according to body posture during manual handling tasks. Biometric data of the mothers were entered into the anthropometric section of the software (sex, weight, and height) and the infants’ weights were considered as the external load the mothers lift with both hands.
Additional necessary 3DSSPP inputs (i.e., body segment angles in horizontal and vertical axes, including Limb Angles, Trunk Angles, and Head Angles) were calculated using images of the worst mother’s body posture in the Digimizer software version 5.3.5 2019. Digimizer image analysis software package allows precise manual measurements of target dimensions and angles [44]. For image size calibration, the 50 cm ruler (earlier installed in the testing background) was used as a reference in the Digimizer software. Next, through visual inspection and body landmarks, angles of trunk, knee, arm, upper arm, hand and neck were measured. The measured inputs were entered into the 3DSSPP software, and the compression and shear force were calculated at the L4/L5-L5/S1 lumbar spine levels [42]. Figure 4 demonstrates a simulated mother body posture while performing the infant handling task.
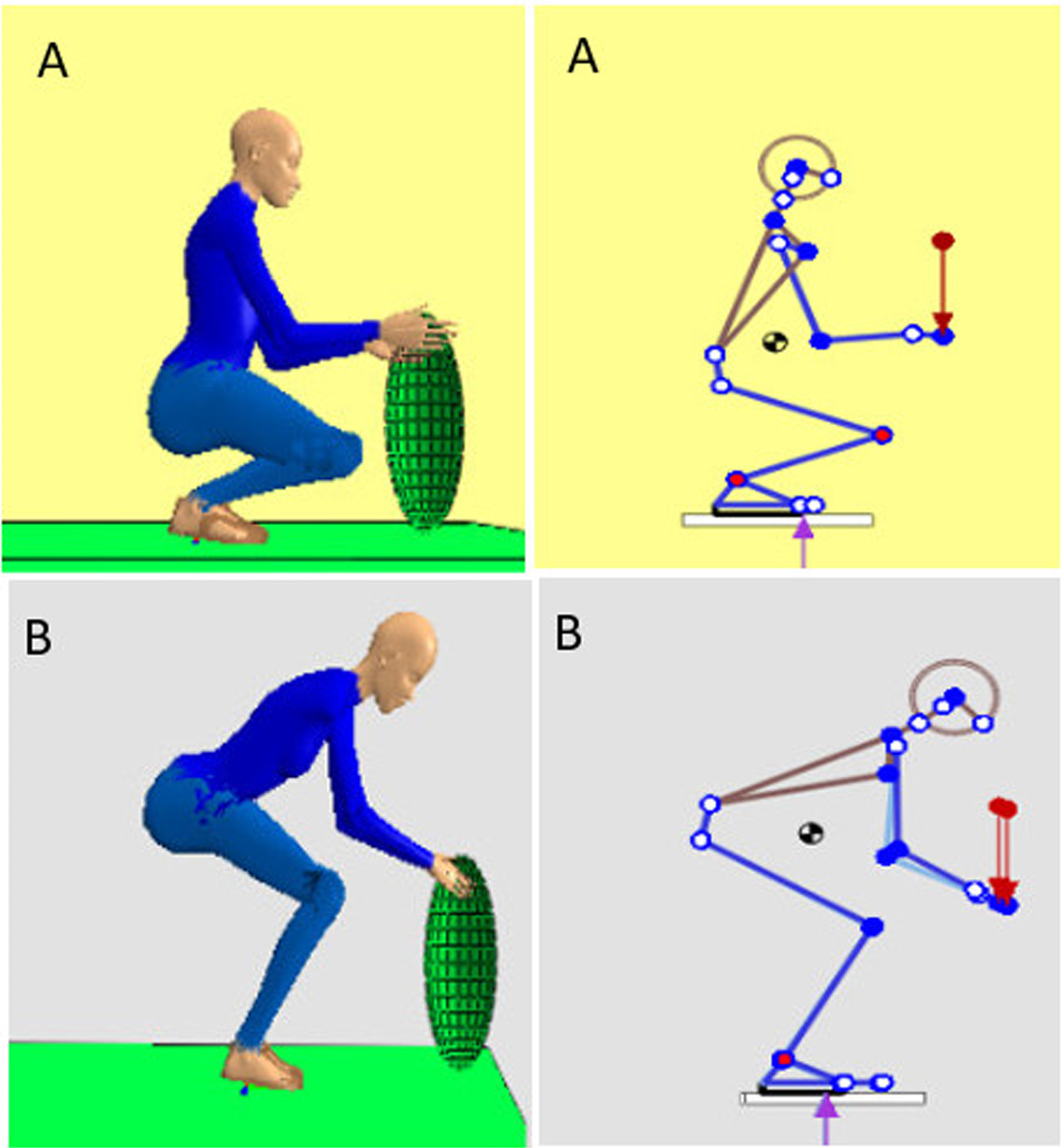
Simulated mother body posture while performing the infant walking task (obtained from participant no. six, subtask no. 4). A: RBW, B: CBW. Inputs in the 3DSSPP software: infant weight 9.7 kg, vertical lifting distance 46 cm, trunk flexion angle 75 and 32 degrees for posture A and B, respectively.
In this study, walker type (CBW/RBW) was considered as an independent variable and indicators of infant feet pattern, RULA score and compression and shear force in lumbosacral level were the dependent variables. The Shapiro-Wilk test was used to evaluate the normality of the collected data. Due to non-parametric distributions of the data, Wilcoxon signed-rank tests were used to evaluate the differences of dependent variables in both study conditions. The statistical significance value was set to α= 0.05, and the analysis was performed with SPSSsoftware V21.
Results
The results from the infants’ feet track patterns analysis (Table 3), suggest there were significant differences between the CBW and RBW conditions. The infants significantly took more steps when the RBW was used (p = 0.002). Also, the distance between the left foot heal strikes was significantly (p = 0.008) higher when using the CBW, with the right foot heal strikes also being higher for the CBW but marginally statistically significant (p = 0.05). Furthermore, the Wilcoxon test results revealed significant differences between left (p = 0.023) and right (p = 0.034) feet distance.
Median values and results from Wilcoxon signed-rank test of feet track pattern
Median values and results from Wilcoxon signed-rank test of feet track pattern
Table 4 shows the RULA score for mothers with the worst posture while performing the baby-walking task. Out of 36 accomplished RULA worksheets, the median value of the worst posture in which CBW/RBW was determined. When performing the baby-walking task using CBW, the final score and action level were 7 and 4, respectively. The RULA final score and action level for the RBW were calculated 5 and 3, respectively.
The results of mothers body posture considering the worst posture while performing infant walking task
Table 5 presents the mean amplitudes and standard deviations for the mothers’ lumbar spine compression and shear force in the L4/L5, and L5/S1 levels while using the conventional and redesigned walkers. The highest overall peak compression (3520 N) and shear (343 N) forces occurred at the L4/L5 level during the lifting of the infants from the CBW. Wilcoxon test results showed that the mean compression and shear force in both L4/L5, and L5/S1 levels were significantly reduced when using the RBW(p = 0.002).
The results of Wilcoxon signed-rank test for mother’s lumbar spine compression and shear mean (SD)\\ force (Newton) in the Lumbosacral levels (N = 18)
In this study, it was observed that when using the RBW, infants took steps with shorter distances when compared to CBW, which can help them maintain balance [45]. On the other hand, when using the conventional BW, we recorded higher distances of heal strikes for the right and left foot, higher distances between the left and right feet and a lower number of steps. Hence, the assessment results suggest the RBW could ameliorate the effects reported by [5] who found adverse impacts on infants’ walking pattern when using conventional BWs before independent walking. Also, using the RBW could reduce the implications on motor skill acquisition of infants and misbalancing of the trunk region reported by [46] for seat-support walkers as in our newly designed RBW there was additional support in the chest area to offer better control of the trunk.
The results related to mothers’ body posture showed a higher RULA final score (worse posture) for mothers when using the baby walking task with the CBW. Performing the walking task with the RBW led to decreasing the median value of the RULA final score by two units from 7 to 5 and the action level by one unit from 4 (investigation and changes are required as soon as possible) to 3 (investigation and changes are required immediately). Admittedly, although these findings suggest improvements with RBW over CBW, there is still room for further supporting parents and reducing further their postural load. Nevertheless, the relatively high score when also using the RBW could be attributed to the common tasks performed (e.g., lifting, placing and removing the infant from the baby walker).
Indeed, [47] reported that the majority of mothers (64%) who lift their infants (9–14 Kg) in a manual way suffered from low back pain, and mothers bear stress on their low back during performing lifting and lowering tasks [48]. Other studies found that lifting the infants was a prominent biomechanical musculoskeletal discomfort risk factor, also associated with parents’ awkward posture during similar tasks (onto a changing table or toilet, into and out of a pushcart or crib), bending (to feed, play, wash hands, or clean the room) and stooping [45, 50]. However, using a correct lifting technique could decrease the impact of this risk factor for mothers [51, 52], without excluding possible future versions of the RBW with appropriate mechanical support.
Additionally to the observations above, the compression forces at the level L4/L5 when using the CBW were over the NIOSH recommended standard threshold level (3400 N) for manual material handling tasks [53]. On the other hand, these forces were more than half lower when using the RBW, with the median value within the NIOSH limits. Although this improvement was not further investigated and is not fully reflected on the RULA scores, it could be attributed to some change in the lifting technique [54]. In the RBW, by removing the rear parts of the CBW (Fig. 1-part No. 2), we provided more space for the mothers during the infant walking task by shortening the horizontal distance from the infant to the mother’s waist. Besides, for lifting and lowering of infants in the RBW, the mothers have to take a seated posture without extending her upper arms (near reaching distance) and this lifting technique strongly affect the intervertebral compression/shear force.
Indeed, as deacreasing intervertebral compression force is an ergonomic improvement to reduce mothers low back strain, it could be concluded that using the RBW may change the infant lifting technique and result in a lower impact on the mother’s lumbar region. Still, although the RBW may help mothers reduce the frequency of the awkward postures and lumbosacral strain, proper ways of lifting and placing infants into the walker must be considered [49, 55–58] while efforts for more supportive walkers continue.
We found no study that evaluates mothers’ spinal load during the infant walking task. Nevertheless, Vincent & Hocking 2002, in an observational study, found that child weight, gripe type, horizontal reach and vertical lift distance were among the most frequent risk factors for mothers’ musculoskeletal disorders [47]. Other child factors in the developmental and behavioural level may influence the severity of parents musculoskeletal disorders [52, 57]. For instance, [59] reported a high prevalence of spinal column musculoskeletal disorders in caregivers of children with cerebral palsy. The estimated shear force in the lumbosacral level for both study conditions with CBW and RBW fell into the normal range according to the NIOSH standard level [53]. However, the reduction in shear force was statistically significant when using the RBW, suggesting that the new design possibly led to improvements regarding the shear force.
Despite the significance findings discussed above, this study has some limitations. First, we considered the north-west population of Iranian infants for anthropometry measurements to redesign the BW. For more representative and generalisable results, infant population anthropometric data in the other regions are necessary. The second limitation of the study was the lack of objective techniques such as foot scan and pressure matt to evaluate infants walking pattern. As infants were not able to provide informed consent, using objective techniques was rejected by the Local Ethics Committee. Third, the assessments were done once and we did not assess long-term effects, which could be the goal of a future study.
The last limitation regards the safety features or effects of using the RBW. Although the latter includes some adjustments, such as a sliding guard to limit the infants’ access to their environment and increase safety (Fig. 1, part No. 4), it was outside the scope of our research to evaluate safety characteristics. BWs safety is the most common issue raised by several studies. About 12% –40% of infants who use walkers may sustain some kind of walker-associated injuries [9, 60–62]. Also, the risk of accidents and injuries is higher when using improperly designed baby walkers [9, 63].
Conclusion
During this study, we redesigned and ergonomically assessed a BW with chest support to reduce the adverse consequences on infants and parents when using conventional BW. The assessment results showed significant improvements when the redesigned RBW was used, including shorter baby steps and heal strikes and improved postural load and reduced intervertebral compression forces for the mothers. These results suggest that using the RBW could help infants gain more control over their walking and delay and/or reduce the development of musculoskeletal disorders in mothers by altering the lifting/lowering techniques of infant from walker. However, the long-term effects of RBW on infants’ motor skill acquisition and safety are recommended to be assessed in future longitudinal studies with more representative populations. Finally, it is recommended for parents who use a walker for their infants to simultaneously look after of their infant and be aware of the relevant effects of BWs.
Ethical approval
The study was approved by the Research Committee of Iran University of Medical Sciences (No. IR.IUMS.REC.1398.997).
Informed consent
In this study, the mothers were asked to read and sign the informed consent form on behalf of both parents and the infant. The informed consent was approved by the Ethics Committee of Iran University of Medical Sciences.
Conflict of interest
None to report.
Footnotes
Acknowledgments
The authors thank all participants for their kind cooperation and the expert panel members for their participation. They also thank Sajad Saleh for 3D modelling of the RBW and Peter A. Howlett for English proofreading of the manuscript.
Funding
Not applicable.