
Abstract
BACKGROUND:
Shoulder pain affects millions of workers worldwide and is considered one of the leading causes of absenteeism and presenteeism. Therefore, using exercises in the work environment emerges as a strategy to prevent or reduce shoulder pain.
OBJECTIVE:
The objective of this study was to evaluate the effects of a workplace-based exercise program on shoulder pain and function in fruit workers.
METHODS:
This was an 8-week parallel two-arm randomized controlled trial. Forty-four fruit workers who reported chronic shoulder pain were randomized to an Experimental Group (EG) or Control Group (CG). The EG was submitted to a program of resistance and stretching exercises for eight weeks, twice a week. The CG received a booklet with muscle stretching and mobility exercises. The primary outcome was shoulder pain intensity; the secondary outcomes were Shoulder Pain and Disability Index (SPADI) and perceived global effect.
RESULTS:
Both groups showed reductions in pain intensity EG: 4.26 (95% CI 2.78–5.74) and CG: 3.74 (95% CI 1.98–5.50) points. The SPADI results showed an average reduction of 17.76 (CI 95% 3.10–32.43) for the EG and 18.39 (CI 95% 3.66–33.13) for the CG. The mean value of the perceived global effect for the CG was 3.45±2.01, and for the EG, the mean was 4.13±1.24. No differences were observed between groups in any outcome analyzed.
CONCLUSION:
Both groups showed significant changes in the analyzed outcomes. However, the workplace-based exercise program was not superior to the exercise booklet.
Keywords
Introduction
Shoulder pain affects millions of people worldwide [1–3]. In the workplace, the shoulder is one of the most affected regions by musculoskeletal disorders [4] and is considered one of the leading causes of absenteeism and presenteeism [5, 6]. In addition to the negative repercussions for workers’ health and companies’ productivity, shoulder pain generates additional costs for health services. A prospective study in Sweden estimated an average annual cost of more than 22,000 euros per patient, adding to the expenses of medical treatment, rehabilitation, and sick leave [6].
The prevalence of shoulder pain in workers increases according to occupational demand, especially in situations that require repeated execution or prolonged maintenance of overhead activities [7–9]. Activities with high physical demands, such as the manual lifting of loads, long-standing, uncomfortable postures, and repetitive movements, have been considered risk factors for developing musculoskeletal complaints [8–10]. Fruit-growing workers carry out all the previously mentioned activities in their work routine, demonstrating daily exposure to these risk factors [4, 12]. Additionally, it should be noted that these workers are almost always exposed to hot climates and high temperatures, as is the case in the São Francisco Valley region in Brazil [4].
A study performed with fruit-growing workers in Brazil demonstrates that they spend more than two-thirds of their work with overhead movements and have a prevalence of 57.8% of severe pain in the last three months for the shoulder region [4]. Furthermore, prolonged exposure to overhead tasks (≥100 minutes) and insufficiently active, overweight, and obese workers represent risk factor for shoulder pain. Therefore, using exercises in the work environment emerges as a strategy to prevent or reduce shoulder pain [13–15] and improve strength, functional capacity, workability, and absenteeism [16].
A recent systematic review with meta-analysis points to the benefits of exercising in reducing shoulder pain, precisely, in workers with pain intensity≥three on a scale of 0–10 points [14]. However, most studies compared groups undergoing exercise programs with control groups that did not perform any activity, which may have overestimated the effect of exercise programs. In addition, the training protocols performed by the studies were designed for specific complaints of the upper limbs, not considering the work demands of other body segments.
Specifically, for fruit workers, most activities are standing and walking for a long time, with simultaneous repetitive movements of hands and shoulders, often performed in uncomfortable postures [4, 17–19]. Thus, proposing an exercise protocol in this population can be beneficial since interventions with exercises have few adverse events [20], a low cost for its implementation [21], in addition, to contribute to the reduction of pain and disability in the upper limbs [13, 16]. Thus, the study aimed to evaluate the effects of a resistance exercise and stretching program on shoulder pain and functionality in fruit workers.
Methods
Study design
This is a Randomized Controlled Trial (RCT) with a parallel group design. The present study was approved by the Ethical Committee in Research of the University of Pernambuco (CAAE: 17386919.6.0000.5207) and registered in the Brazilian Registry of Clinical Trials (ReBEC) under protocol number: RBR-85vqk6. Our findings are reported according to the recommendations of the Consolidated Standards of Reporting Trials (CONSORT) [22]. The reporting of interventions follows the template for intervention description and replication (TIDieR) checklist [23].
Participants
Study participants were recruited from two farms in the São Francisco Valley region (Brazil) through contact with fruit companies in the area. Participants were recruited at two times: 1) September 2020; 2) January 2021. Such a strategy was used, given many layoffs on farms due to the Covid-19 pandemic, which led to a second moment of recruitment of participants.
The eligibility criteria to participate in the study were: 1) Men and women; 2) Physically independent; 3) History of shoulder pain lasting more than three months; 4) Pain intensity≥three on the pain perception scale (0 to 10 points); 5) No history of shoulder trauma or surgery; 6) Not having a spine and knee disorders that make it impossible to perform exercises; (7) Present a positive result in the following tests: Test of resistance to external rotation, painful arc, Neer, Hawking-Kennedy and Jobe, to confirm the diagnosis of Subacromial Impingement Syndrome [24]. Exclusion criteria were: 1) Physical inability to perform the exercises included in the interventions; 2) Presence of any limiting health conditions to continue performing the interventions (Ex, osteoarticular, cardiometabolic problems, or other conditions); 3) Pregnancy.
Intervention
Participants eligible for the study were randomized into the Control Group (CG) and the Experimental Group (EG). All participants were recruited from the same company, under the same leadership, and workers had the same work and break schedule. The CG received an educational booklet with illustrations of stretching for all body segments (Supplementary Material A). The participants were instructed to perform the stretching exercises at different work times without supervision. Before starting the intervention, the booklets were personally delivered to each worker, and instruction was given for each stretch. The weekly frequency was twice a week for eight weeks. There was weekly telephone follow-up to check adherence and possible adverse events. When necessary, personal meetings were held to verify discomforts related to the stretching exercises or to encourage them not to give up on the intervention.
Regarding the EG, the supervised training program was carried out in the workplace, with strength and stretching exercises for all body segments under the supervision of a physiotherapist and a physical education teacher (Supplementary material B). All participants were requested to avoid doing physical exercise during eight weeks of interventions, and we ask indicate if they were doing shoulder rehabilitation. The training program had the same weekly frequency as the CG; each session lasted between 20 and 28 minutes. The company established session times. For some workers, it was at the end of the shift, while for others, it was in the middle. The exercise protocol was structured in three stages: 1) Stretching exercises for the most overloaded muscle groups, mobility and stationary running with two sets of 30 seconds; 2) Muscle strength and endurance exercises (external shoulder rotation, push-ups, squats, horizontal rowing, and lateral elevation). In the first two weeks, subjects performed two sets of 12 to 15 repetitions, progressing from the third to the fifth week to 10 to 12 repetitions. While from the sixth to the eighth week, the participants performed three series, varying 8 to 10 repetitions. All exercises had intervals of 30 seconds between exercises and 45 to 60 seconds between sets; 3) CORE strengthening consisted of frontal plank and pelvic elevation exercises lasting between 15 and 60 seconds, as shown in Supplementary Material B.
The exercise program was designed considering the characteristics of the studies included in the systematic review [14], making it possible to reproduce the protocol in any workplace. Training progression and load adjustment followed the recommendations of the American College of Sports Medicine [25]. The materials used to perform the exercises were: mats, elastic bands, and dumbbells.
Adverse events
Adverse events included worsening health status or the appearance of musculoskeletal problems directly related to the intervention program. Adverse events were monitored weekly and obtained through a face-to-face interview with the EG and a call with the CG. During the interview, the volunteers were asked to report the use of medications, visits to the doctor, changes in the clinical picture, acute illnesses, or the appearance of any symptoms.
Primary outcome
The shoulder pain intensity was measured using a Numerical Pain Scale, represented in a horizontal bar, ranging from 0 to 10 points [26]. For its application, the evaluator verbally explained to the participant that zero indicated no pain, while ten represented unbearable pain [26]. Participants indicated to the evaluator which scores described the perception of shoulder pain intensity. The instrument has a Minimal Clinically Important Difference (MCID) of 2.17 points [27].
Secondary outcomes
The Shoulder Pain and Disability Index (SPADI) questionnaire, validated in Brazil [28], was used to assess shoulder pain and the inability to perform daily tasks. The questions were directed to the affected arm, composed of 13 items. The first eight questions are related to disability, and the following five are about shoulder pain. Each item has a score ranging from 0 to 10, and at the end, the result of the questionnaire has a score between 0 and 100 points, with 100 being the worst condition [28]. The instrument has an MCID of 13.2 points [29].
The Perceived Global Effect Scale was used to verify the global impression of the patient’s current recovery, comparing the onset of symptoms and the health condition at the end of the intervention. The scale is composed of 11 points, which starts at –5 (much worse) goes through 0 (did not notice changes) and ends at 5 (completely recovered) [30]. Primary and secondary outcomes were assessed at baseline and the end of the 8-week intervention.
Sample size
The sample calculation was performed using an electronic calculator [31], considering an alpha of 5% and a power of 90%. Although the study presents several outcomes, we performed the sample calculation based on shoulder pain intensity (primary outcome). We considered the mean change of 0.6 points in shoulder pain intensity for the control group and 2.2 points for the experimental group, in addition to the standard deviation of 1.5 obtained from data from the study by Jay et al. [32]. In addition, a 15% loss rate was added to get 44 subjects finally. The study by Jay et al. [32] is similar to the present study, considering: the duration of exercises, weeks of intervention, and type of intervention.
Randomization and blinding
The randomization process occurred at the end of the baseline assessments through a hidden sequence of randomly permuted blocks, which a researcher at http://www.randomizer.org independently generated. Concealed allocation was achieved using sequence codes; the volunteers were randomized to EG and CG groups with a ratio of 1:1. The evaluators did not have access to information about the randomization of the allocation codes of the participants in their respective groups, execution of the training program, data tabulation, and statistical analyses. All participants were instructed not to reveal to the evaluators which type of intervention they received.
Statistical analysis
SPSS version 22 (IBM Corp., Armonk, NY, USA) was used to perform the analyzes, and the intention-to-treat principle was applied. Descriptive statistics were based on central tendency (mean), dispersion (standard deviation), and frequency distribution (absolute or relative) and were used to characterize the participants.
Differences within and between groups and their respective confidence intervals (95% CI) were calculated using models of Generalized Estimating Equations (GEE., considering the factors group, time, and the interaction group and time). Bonferroni’s post hoc was used to perform multiple comparisons when differences were detected. The assumption of normality of the residuals was evaluated by Q-Q plot analysis.
The Mann-Whitney U test was used to compare the two groups (GC and EG) about the results of the Perception of Global Effect Scale. Mean differences and 95% confidence intervals, as well as the interpretation of the clinical significance of the results, were analyzed, adopting a significance level of 5%.
Results
The first recruitment phase was completed in September 2020, and the second phase in January 2021. The intervention period for the first phase was between October and December 2020, and for the second phase, it was between January and March 2021. Summarizing these two moments, 92 participants were recruited. However, 48 participants were not included in the study, as shown in the flowchart in Fig. 1. The 44 participants were randomized into two groups: GC (n = 22) and EG (n = 22).
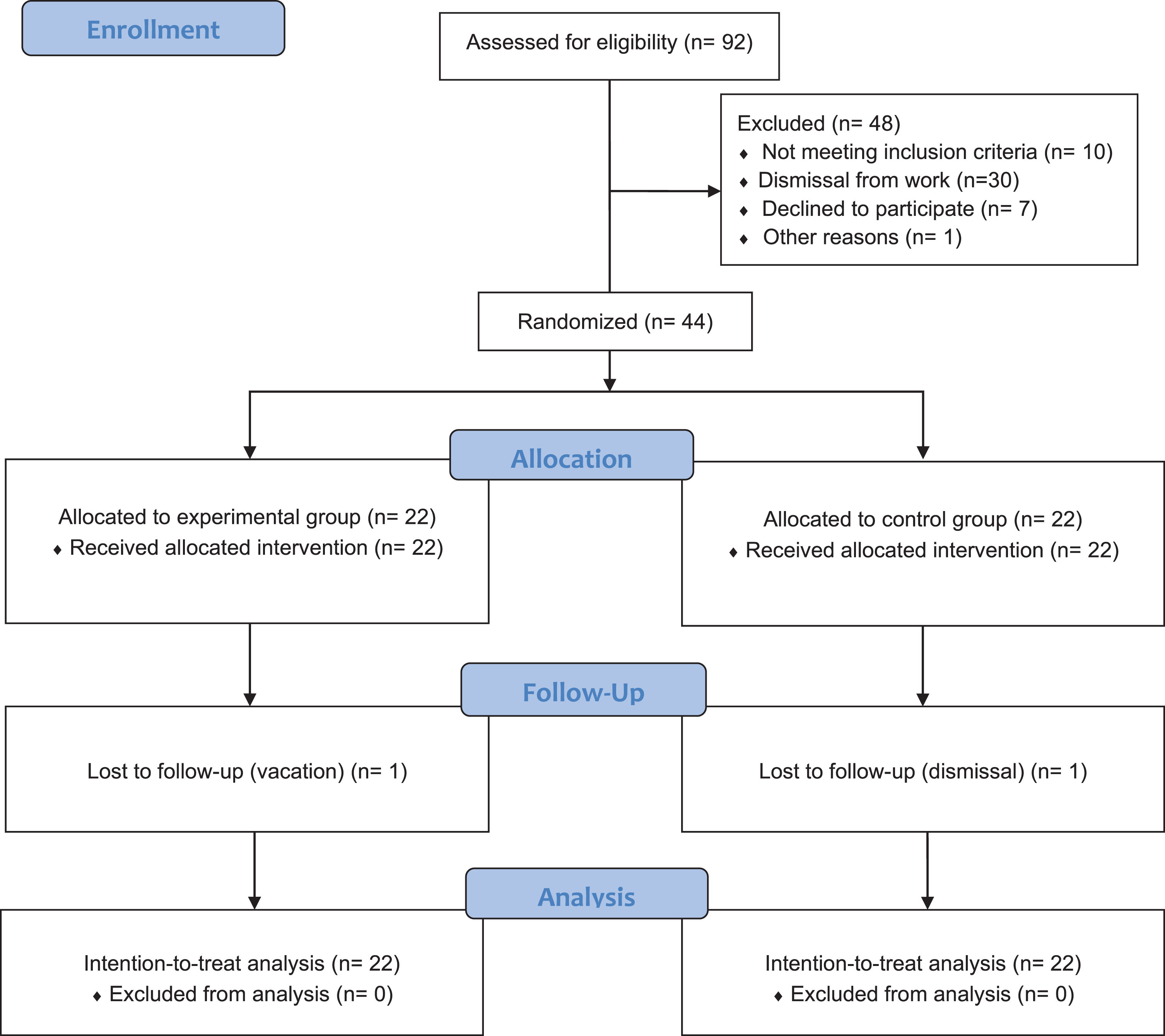
Flowchart of the study process based on CONSORT guidelines.
During the follow-up, there was a loss for each of the groups. In the EG, a participant went on vacation, and it was not possible to be reassessed, and in the CG, one of the participants was fired, affecting his reassessment. However, the follow-up data of these two participants were imputed for the analyses.
Descriptive information on participants at baseline is shown in Table 1. The sample consisted of 44 participants, 31 women (70.50%) and 13 men (29.50%), with a mean age of 38.97±9.18 years old and a BMI of 26.34±5.09 kg/m2. Mean shoulder pain intensity was 7±2 points, with pain duration of 31.95±40.49 months and a mean SPADI total score of 33.91±24.91 points.
Descriptive characteristics of participants
Note: SPADI - Shoulder Pain and Disability Index; BMI - Body Mass Index; The results are % or averages (standard deviation).
The results of the interaction between groups and time are presented in Table 2. No significant difference was observed between the groups for shoulder pain intensity in the post-intervention moment, with a mean reduction of 0.19 (95% CI –2.64; 2.26). However, both groups showed significant decreases at the end of eight weeks of training, with an average shoulder pain intensity for the CG of 3.74 (CI 95% 1.98;5.50) and 4.26 (CI 95% 2.78;5.74) for the EG.
Mean (SE) of the variables analyzed in the participants’ assessments, mean (SE) difference within groups, and mean difference between groups (95% CI)
Note: The results are mean (standard error) and difference mean (95% CI) within and between groups.
Regarding the SPADI results, no significant difference was observed between the groups after the intervention 1.23 (CI 95% –13.54;16.00). However, significant differences were verified within the groups, with an average reduction of 18.39 (CI 95% 3.66;33.13) for the CG and 17.76 (CI 95% 3.10;32.43) for GE.
The Global Effect Perception Scale does not show a significant difference between the groups, with a positive effect of 3.45±2.01 and 4.13±1.24 for the CG and EG, respectively. Regarding the participants’ adherence, the CG showed an adherence of 95.43% ±10.39, while the EG was 61.51% ±37.17. Throughout the study, no adverse events were reported for either group.
This study hypothesized that carrying out an eight-week workplace-based exercise program would have superior effects in improving shoulder pain and disability compared to an educative intervention with minimal physical activity and without supervision. The results did not show significant differences between the groups, rejecting the initial hypothesis. However, both interventions presented changes in the analyzed outcomes. If their magnitudes are considered, it is possible to verify that these changes, in addition to being statistically significant, proved clinically meaningful.
EG participants who performed the resistance exercise program (dynamic and isometric) and static stretching showed an average reduction of 4.26 points in pain intensity and 17.76 points in SPADI. In both outcomes, statistically significant differences and magnitude of reductions were verified that exceeded the values described in the literature as clinically important, 2.17 for pain and 13.2 for SPADI. These findings corroborate recent systematic reviews, which found that resistance exercise programs can effectively improve pain and disability in people with subacromial symptoms [33–35]. Specifically for workers with upper limb conditions, Hoosain et al. [16] found that resistance training contributed to improving pain-related aspects, such as strength, functional capacity, workability, and absenteeism. More recently, Picón et al. [14] demonstrated a substantial degree of recommendation for using resistance exercises to reduce shoulder pain in workers with pain≥3 points, resulting in clinical changes.
Notably, the workers in the present study have occupational characteristics of overhead activities, which may contribute to shoulder injuries. A study published by Batista et al. [4] showed that fruit workers spent an average of 357 minutes of occupational time with overhead movements. Workers who perform≥100 minutes of work time in overhead activities have a chance of increasing shoulder pain by 1% each minute during overhead activity. Likewise, Leong et al. [10] reported that working with the shoulder above 90° was associated with an increased risk of rotator cuff tendinopathy among the working population (OR 2.41, 95% CI 1.31–4.45). In this sense, using resistance exercise strategies can help this population with work demands; Pieters [33] highlights that there is evidence, from moderate to high, to recommend the practice of strengthening and stretching exercises of the scapular and shoulder muscles to improve functionality and reduction of pain, in the short and long term.
Regarding the mechanisms to explain the responses observed after the interventions, resistance exercises could reduce the perception of pain, considering that they contribute to the activation of central pain inhibition and modulation mechanisms, which may include an increase in the concentration of β-endorphins and catecholamines, change in sensitivity to painful stimuli, among other aspects [36, 37]. In addition, performing static stretching exercises could decrease the viscosity and rigidity of the musculotendinous unit in the most contracted musculatures, and change the sensory perception of pain or discomfort, thus increasing the range of motion [38].
These possible mechanisms related to muscle stretching exercises may help explain the significant CG changes. Even if performed without supervision, workers allocated to the CG showed clinically important reductions in pain intensity (3.74 points) and disability (18.39 points in SPADI) outcomes. A study with a training protocol similar to our control group proved effective in reducing pain and improving shoulder range of motion in office workers [39]. These findings are similar to the results of other studies, which point to the benefits of stretching exercises for pain and shoulder functionality in workers [40, 41].
We observed clinically meaningful improvements in the evaluated outcomes in both groups, with no differences after an eight-week protocol. Thus, our findings reinforce the indication of physical exercise, regardless of modality, as an essential resource for pain management and improving shoulder function in workers. The dynamic characteristic of both interventions affects the analyzed results positively. Our results corroborate the study by Gram et al. [42]. The authors found that 20 weeks of exercise, with minimal supervision, significantly reduced shoulder/neck pain in office workers. Even if an unsupervised intervention has a lower cost for the company, we highlight the need for a physiotherapy professional to verify the workers’ work demands and musculoskeletal complaints to prescribe the appropriate exercises. Still, another aspect that should be highlighted is greater adherence and engagement by the CG group compared to the EG. This fact may have provided the CG with a higher “intervention dose,” which may have influenced the results obtained by this group. However, these findings must be considered with caution, considering the method’s limitations for this type of analysis.
In this RCT, there are several strengths: 1) Conducting an RCT with fruit workers, considering the scarcity of published studies in this population; 2) Low sample loss, considering that the workers who left the study were caused not related to the interventions; 3) Interventions are simple and inexpensive, making it possible to implement this type of protocol according to the availability of resources and company preference; 4) The evaluators were blind about the analyzed outcomes. However, the study also has limitations, including 1) The use of instruments with subjective measures, which can generate bias in the responses, especially in subjects with a low level of education; 2) A short intervention period; 3) We did not assess aspects related to productivity and work absenteeism. In this sense, we suggest that future studies use objective measurements, such as a pressure algometer, and that interventions be carried out over a more extended period.
Conclusion
The results of this study suggest that there is no difference between a stretching and resistance exercises supervised program performed at the workplace and a stretching program performed at home without supervision on the outcomes of pain and disability in fruit workers. However, it is essential to highlight that both programs provided clinically meaningful improvements in the analyzed outcomes. These findings expand the possibilities of intervention in this population, and it is up to companies to define the most appropriate option according to their financial and logistical reality.
Ethical approval
This study was approved by the Ethics and Research Committee of the University of Pernambuco (CAAE: 17386919.6.0000.5207).
Informed consent
All individuals were informed about the objectives of the study and signed a Free and Informed Consent Form, according to the rules of Resolution 466/12 of the National Health Council and the Declaration of Helsinki.
Conflict of interest
None of the authors have any conflicts of interest, including specific financial interests, relationships, and affiliations relevant to the subject matter or materials included in this manuscript.
Footnotes
Acknowledgments
We are grateful for the collaboration of the participants and the employers’, making it possible to perform the data collection. We thank the support of the scholarship given by the Coordination for the Improvement of Higher Education Personnel (CAPES) for two students of Ph.D. degrees: Sol Patricia Beltrán and Gabriel de Amorim Batista. This research has been funded by Dirección General de Investigaciones of Universidad Santiago de Cali under call No. 02-2023.
Funding
The authors report no funding.