
Abstract
BACKGROUND:
Long-term work with elevated arms, or overhead work, is a risk factor for musculoskeletal complaints and disorders. Upper-limb exoskeletons are a promising tool for reducing occupational workload when working with hands above shoulder level.
OBJECTIVE:
The purpose of this study was to assess the effects of upper-limb exoskeleton on muscular and physical strain and perceived exertion during dynamic work at four different shoulder joint angles. Further, we evaluated if there are any negative effects associated with the use of exoskeleton.
METHODS:
A total of 15 student participants performed dynamic work in laboratory setting with and without an exoskeleton at four different shoulder angles: 60, 90, 120 and 150 degrees. Muscle electrical activity from 8 muscles of the upper body, perceived exertion, and heart rate were measured during the work task, and grip strength, muscle stiffness, tone, and elasticity from six muscles, m. deltoideus physiological cross-sectional area and muscle fiber pennation angle, and nerve conduction velocity were measured before and after the work task.
RESULTS:
Based on the results, the use of exoskeleton significantly reduced the muscle activity of the upper limb, shoulder, and back muscles. The reduction was most significant when the arm elevation was 120°, and in m. deltoideus muscle activity. RPE was also positively affected indicating reduction in workload when using exoskeleton.
CONCLUSION:
The results suggest that the use of upper limb exoskeleton has potential to reduce physical workload during overhead work and, consequently, reduce the risk for work-related musculoskeletal disorders.
Introduction
Working with hands above shoulder level has been identified as a risk factor for pain and work-related musculoskeletal disorders (MSD) in the neck and shoulders. Recent evidence suggests that arm-hand elevation and shoulder load double the risk of specific soft tissue shoulder disorders (e.g., subacromial impingement syndrome, tendinitis of the biceps tendon, rotator cuff tears, and suprascapular nerve compression) [1–4]. Working with arm elevation causes muscle tension and increases intramuscular pressure impairing muscle blood flow in neck and shoulder region [5, 6]. Prolonged tension can further lead to accumulated fatigue [7] and possibly inflammation in the muscle tissue [8]. Also, degeneration of tendons, cartilage, and other joint structures through impairment of circulation due to static tension may occur, especially in the shoulders [9, 10]. In addition to increased load to muscles and joints, working with hands at or above heart level elevates blood pressure increasing the workload of the cardiovascular system [11]. Traditionally, potential ways to reduce MSD risk are for example improving ergonomics and proper organization of work. However, the need to reduce the physical load of work still exists.
Recently, wearable assistive devices, also called exoskeletons, have been developed for supporting movements and postures in occupational context and thereby reducing the physical strain. Upper-limb exoskeletons provide support to the upper extremities by transferring forces from the upper limbs to other parts of the body or by storing/releasing energy during movements. Exoskeletons can be classified as active or passive depending on their operating principle. Active exoskeletons operate with motors, hydraulic, or pneumatic systems. Passive exoskeletons do not have an active component but rather support the arms by storing kinetic energy to joint or spring systems [12]. The potential of upper-limb exoskeletons in reducing occupational workload has been identified. Therefore, they possess the ability to diminish the risk for work-related neck and shoulder problems and promote occupational health.
Numerous studies have found that the use of passive upper-limb exoskeleton reduces muscle activity in the neck, shoulders, and arms [13–25], and, consequently, diminishes the loading of the upper body. The magnitude of the reduction in m. deltoideus muscle activity during overhead work has ranged from 34% [20] to as great as 73% [24]. Exoskeletons also seem to reduce perceived effort and discomfort [16, 25]. Furthermore, the reduction of both heart rate (HR) and oxygen consumption when using exoskeletons for overhead work indicates that physiological strain and metabolic cost of work is decreased [15, 23]. Nevertheless, literature does not accurately report at which shoulder elevation angles the use of exoskeletons is most beneficial.
Besides the positive effects described above, upper-limb exoskeletons may also impose adverse outcomes. While decreasing muscle load of target muscles, by design exoskeletons transfer the loading to other parts of the body, for example the lower back [26]. However, the reported adverse effects can be conflicting. For example, strain in the lumbar region has been assessed in some studies by measuring muscle activity of erector spinae. In these studies exoskeletons have not affected muscle activity or perceived effort in the muscles of the lower back [18, 22]. Still, Weston et al. [26] found an increase in compressive spinal loads of the lumbar spine but, on the contrary, Kim et al. [27] witnessed a 30% reduction in spinal loading during overhead work using an upper-limb exoskeleton.
Other concerns are related to subjective evaluations of discomfort when using exoskeletons. This is often due to the weight or improper fit of the device [28]. Also, upper-limb exoskeletons may limit or modify the range of motion or movement patterns of glenohumeral and elbow joints [20, 27]. It is also reported that the exoskeleton is cumbersome and limits shoulder mobility, which adversely affects usability of the device [16, 18].
According to available literature, exoskeletons can be considered a potential tool for reducing the workload of the upper body while working with hands at or above shoulder level. However, detailed knowledge on the effect of exoskeleton on muscle strain at different shoulder angles is missing. The purpose of this study was to assess the effects of upper-limb exoskeleton on muscular and physical strain and perceived exertion during dynamic work at four different shoulder joint angles. Further, we evaluated if there are any negative effects associated with the use of exoskeleton. To comprehensively quantify the all-round physiological effects of exoskeleton use on muscle and joint loading and cardiovascular strain, diverse measurements from several target muscles were incorporated. It is hypothesized that by using a passive upper-limb exoskeleton while working with hands elevated, muscular and physical strain, and perceived exertion are reduced with no major adverse effects.
Methods
Participants
Fifteen participants (6 females, 29.3±8.7 years, 69.3±19.2 kg, 168.5±7.4 cm and 9 males, 28.8±7.5 years, 83.1±8.5 kg, 182.8±4.9 cm, mean±standard deviation) volunteered to participate in this study. All the participants were university students. One of the participants was left-handed. Participants did not have any self-reported back or shoulder pathologies or injuries in the past six months. None of the participants had any prior experience using an exoskeleton. They gave written consent after receiving detailed information on the objectives, protocol and possible discomforts and risks. The study was conducted according to the Declaration of Helsinki of 1964 and its later amendments and had approval from the ethical committee of the Northern Ostrobothnia hospital district (EETTMK 70/2019 §215).
Experimental design and procedure
This study was a randomized cross-over study. The participants performed dynamic repetitive work tasks simulating painting work. The work task was performed with the right hand. A 2 kg dumbbell was transferred 50 cm horizontally back and forth on a marked area on a surface in front of the subject (Fig. 1). The weight was moved at the rate of 35 bpm which was set by a metronome. The task duration was the same for working without (REF) or with the exoskeleton (EXO) for each shoulder angle and the duration was determined during REF. The end of the work task was set at the time point when the perceived exertion was rated 18 (“very hard”) or above on Borg’s 6–20 rating of perceived exertion (RPE) scale [29] or at 5-minute mark. The work task was performed at four shoulder angles, 60°, 90°, 120°, and 150°, first without and then with the exoskeleton. The shoulder angle was set as the angle of humerus related to torso with a digital goniometer (Digitest Augo, Digitest Oy, Muurame, Finland). Measurement order was randomized for the shoulder angle and each of the 8 measurements (two conditions, four shoulder angles) was done on a different day with at least 48 hours between each measurement. The participants were instructed to avoid heavy exercise 48 hours before being measured.

Experimental set up and task simulating upper extremity movement pattern of painting work. The illustrated shoulder angle is 120°.
RPE, electromyography (EMG) from eight muscles, and HR were measured continuously during the work task. Maximal grip strength, m. deltoideus muscle physiological cross-sectional area (PCSA) and muscle fiber pennation angle (PA), muscle stiffness, tone, and elasticity from six muscles and n. axillaris nerve conduction velocity were measured before and after each work task. All measurements were made from the right side of the body. Tasks and measurements were performed under constant temperature and relative humidity conditions (20±1°C and 40±5%, respectively).
The exoskeleton used in this study was a commercially available passive exoskeleton Skelex 360 (Fig. 2, Skelex, Rotterdam, the Netherlands), which is designed for repetitive and static work with arms at or above shoulder level. The upper limb effort is reduced by means of two carbon fiber springs. The exoskeleton is worn by the user like a backpack with distal extremities of the mechanical arms attached to user’s upper arms with elastic straps. Skelex 360 weighs 2.7 kg and was individually adjusted to suit the user with assisting force (0.5–3.5 kg) set proportional to user’s body weight. According to the user manual, the adjustment setting 1 was used for users weighing over 50 kg, setting 2 for users over 65 kg, setting 3 for users over 80 kg and setting 4 for users over 95 kg. All the other adjustments of the exoskeleton were made according to anthropometric measures as instructed in the user manual [30].
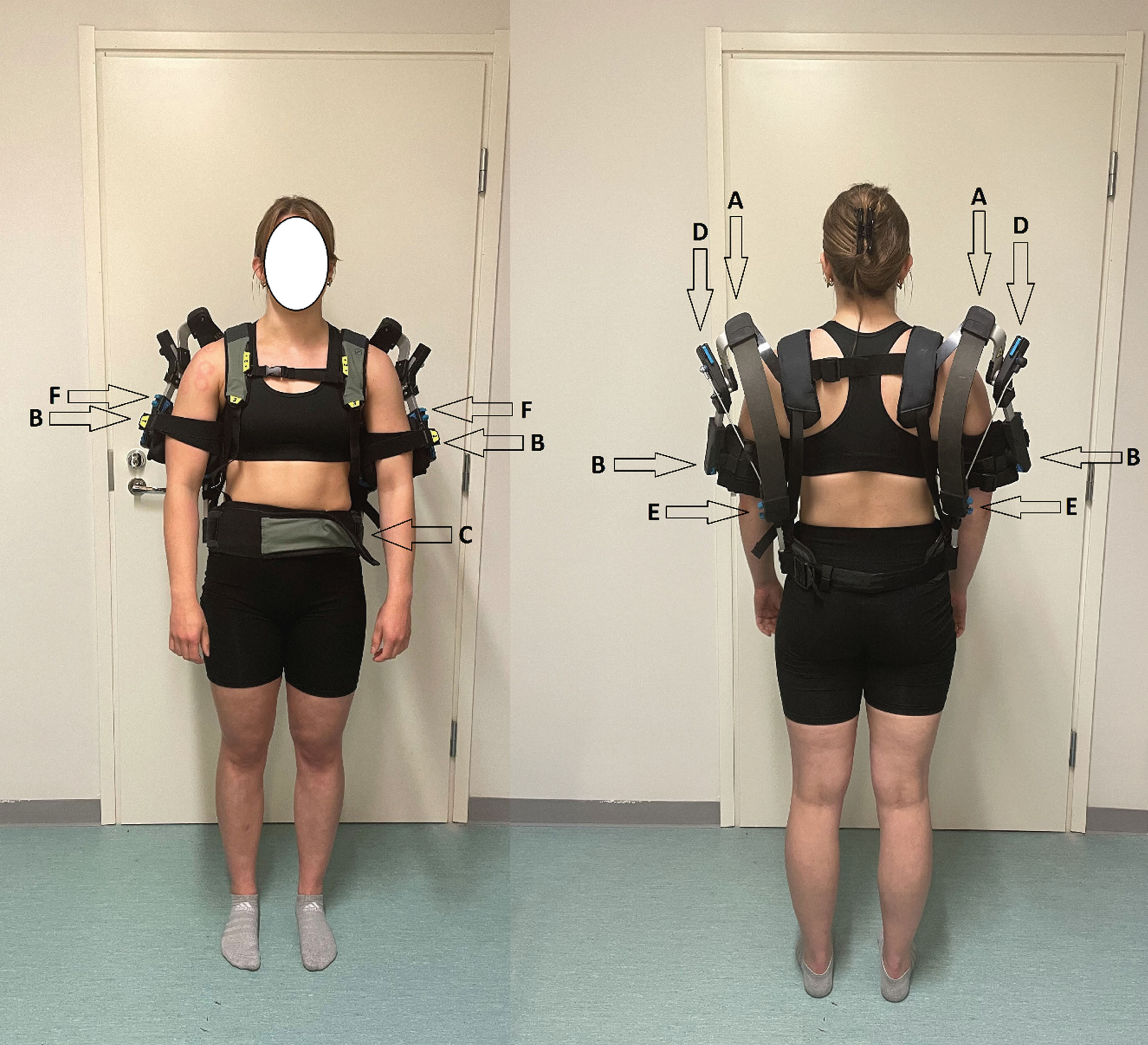
Skelex 360 exoskeleton. A: carbon fiber springs, B: arm cup and elastic arm strap, C: adjustable belt, D: force adjustment, E: spring height adjustment, F: arm length adjustment.
Electromyography
EMG was recorded with ME6000 (Bittium Wireless Oy, Kajaani, Finland) from eight muscles: m. extensor carpi radialis longus (wrist extensor, WE), m. flexor carpi radialis (wrist flexor, WF), m. triceps brachii (TB), m. deltoideus pars acromialis (medial deltoid, MD), m. deltoideus pars clavicularis (anterior deltoid, AD), m. trapezius pars descendens (upper trapezius, UT), m. trapezius pars tranversa (tranverse trapezius; upper back, TT), and m. longissimus dorsi (lower back, LB). Two single-use surface electrodes (BlueSensor M-00-S, Ambu A/S, Ballerup, Denmark) were placed on shaved, alcohol cleaned skin on the muscle belly of the measured muscles. EMG signals were recorded at 1000 Hz, amplified (x2000), filtered with Butterworth filter (8/500 Hz), and averaged with 100 ms overlapping (30 ms) time window. EMG data were analyzed with MegaWin software (Bittium Biosignals Oy, Kuopio, Finland) and windowed to include EMG data from the entire work task.
Before the first work task, maximal isometric voluntary contractions were performed separately for each muscle. The maximal amplitude value (μV) during the maximal isometric voluntary contraction was used to calculate muscle electrical activity in relation to maximum (% MEMG) for each measured muscle. % MEMG was calculated as an average from the whole duration of the work task for each muscle as well as an average from all 8 muscles.
Perceived exertion
RPE was assessed using the Borg 6–20 RPE scale [29] every 30 seconds during and at the end of each work task in all experimental conditions. The slope of the increase in RPE over the work task was calculated, and REF and EXO were compared based on the slope of the regression line.
Heart rate
Beat-to-beat HR was measured with Firstbeat Bodyguard2 (Firstbeat Technologies Oy, Jyväskylä, Finland). The device was attached to participant’s chest with two single-use ECG electrodes (BlueSensor VL-00-S, Ambu A/S, Ballerup, Denmark): one electrode was attached under the clavicle on the right side and another on rib cage on the left side. If needed, the skin was shaved from excess body hair prior to attaching the electrodes. The results for HR were calculated as an average from the whole duration of the work task.
Data collected before and after the work task
Grip strength
Maximal grip strength was measured with the forearm supported at 90° elbow angle using a strain gauge sensor device (Newtest Grip Strength, Newtest Oy, Oulu, Finland). Higher value of two efforts was selected.
Muscle stiffness, tone, and elasticity and muscle architecture
Muscle stiffness, tone, and elasticity were measured with a myotonometer (Myoton-3, Myoton AS, Tallinn, Estonia). The method is based on measuring the attenuation of vibration applied to a tissue. The myotonometer delivers five consecutive, constant (0.5 N) impacts to the surface of the skin. Based on the rate and magnitude of attenuation, the device calculates the stiffness, tone, and elasticity of muscle tissue as an average from five impacts. Measurements were made from WE, WF, MD, UT, TT, and LB. A longitudinal and transverse image of m. deltoideus was taken with ultrasound (Logiq-5, General Electric, Boston, USA) and average PCSA of the muscle and muscle fiber PA were analyzed.
Nerve conduction velocity
Nerve conduction velocity was measured from n. axillaris with an EMG device (Sierra II Wedge, Cadwell, Kennewick, USA). The stimulus to n. axillaris was applied at the crook of the arm and the motor nerve response (M-wave) was measured from m. deltoideus. Required stimulus current amplitude was determined during the first measurement by increasing the stimulus amplitude until clear nerve response was detected. The average stimulus intensity was 26.0±3.8 mA. Motor nerve response delay time (M-wave latency) and response size (M-wave amplitude) were analyzed as an average of five measurements.
Statistical analyses
The data were statistically analyzed using SPSS Statistics 27 (IBM Corp., Armonk, NY, USA). The data were tested for normal distribution with Kolmogorov-Smirnov-test, homogeneity of variance with Levene’s test, and sphericity with Maulchly’s test. Differences in % MEMG, RPE, and HR between REF and EXO as well as changes in variables measured before and after each work task were compared with a paired samples t-test. Differences between work durations at different shoulder angles were tested with one-way analysis of variance (ANOVA) and Bonferroni correction. The level of statistical significance was set at p < 0.05. All results are presented as mean±standard error of mean. The sample size was sufficient based on power calculations with alpha-value of 0.05 and a power of 80 percent.
Results
Work duration
The duration of the performed work was longest at 60° (3.1±0.3 min). The work duration at 60° differed from 90° (2.4±0.3 min, p < 0.001) and 120° (2.5±0.2 min, p < 0.01) but not from 150° (2.5±0.2 min).
Electromyography
In AD and MD, % MEMG was lower in EXO at all shoulder angles (Fig. 3). In addition, % MEMG was reduced in TB at 60°, 120° and 150°, in TT at 90° and 120°, and in WF at 60° and 150°. There were no statistically significant differences in % MEMG between REF and EXO in WE, UT or LB at any shoulder angle. The greatest reductions in % MEMG were recorded from MD at 60° (38.7±7.8%) and AD at 90° (38.2±5.3%). The average reduction (all 8 muscles) in % MEMG in EXO was greatest at 120° (25.4±4.1%, p < 0.001). Corresponding reductions were 21.5±3.0% at 60° (p < 0.001), 23.6±4.5% at 90° (p < 0.001), and 19.3±5.6% at 150° (p < 0.01).
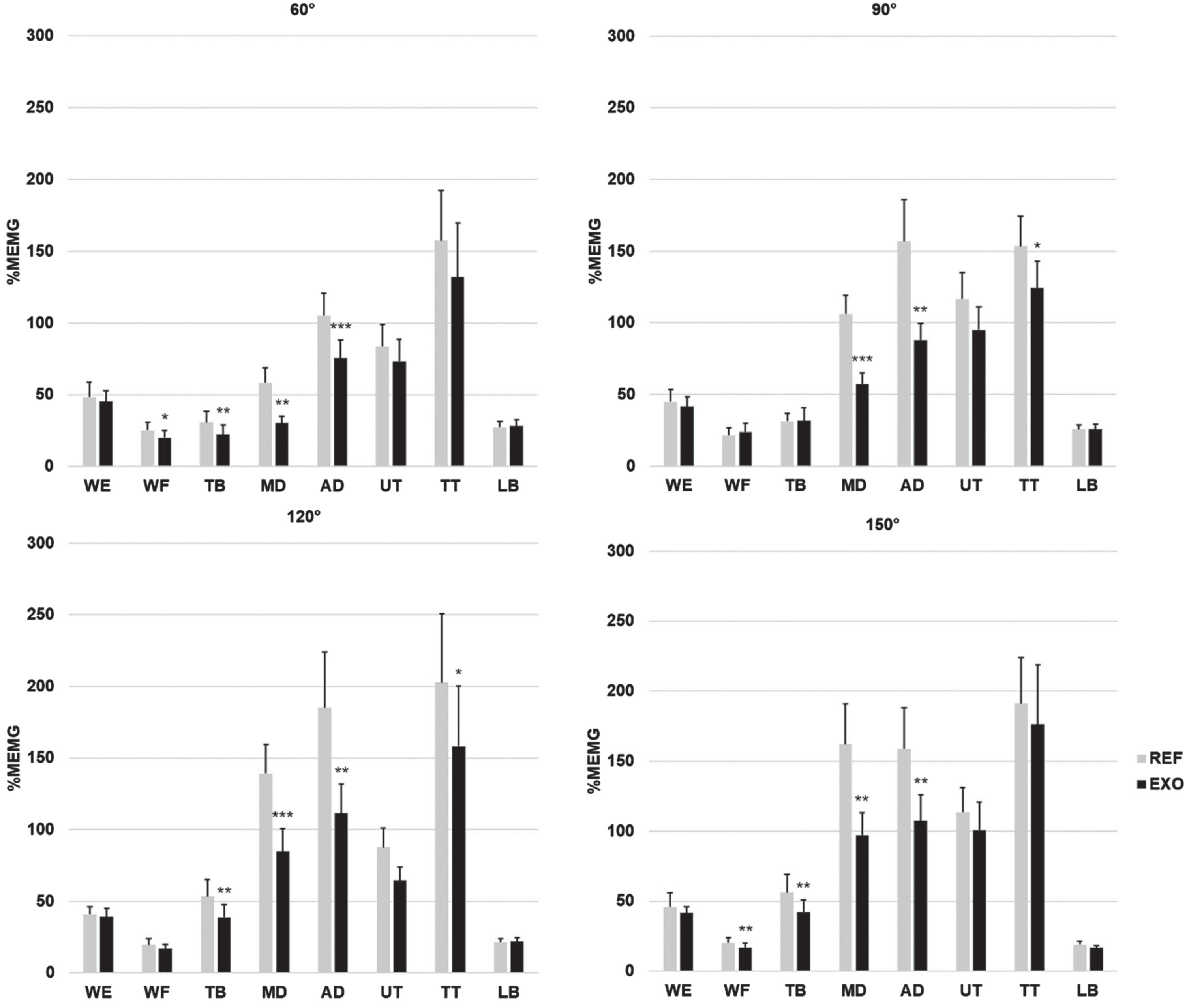
Muscle electical activity in eight muscles during dynamic work at four shoulder angles. % MEMG = muscle electrical activity in relation to maximum; WE = wrist extensor; WF = wrist flexor; TB = triceps brachii; MD = medial deltoid; AD = anterior deltoid; UT = upper trapezius; TT = transverse trapezius (upper back); LB = lower back; REF = reference condition; EXO = exoskeleton condition. *Statistically significant difference between REF and EXO *p < 0.05, **p < 0.01, ***p < 0.001.
RPE was significantly lower while using the exoskeleton at all shoulder angles (Fig. 4) and the difference between the conditions was largest at 120°.

Rating of perceived exertion (RPE) during dynamic work at four shoulder angles. REF = reference condition; EXO = exoskeleton condition. *Statistically significant difference in the linear slope between REF and EXO *p < 0.05, **p < 0.01, ***p < 0.001.
HR was significantly lower in EXO at 60°, 120°, and 150° shoulder angles. Average working HRs at four shoulder angles are presented in Table 1.
Average heart rates (bpm) during dynamic work at four shoulder angles. p-value represents statistical differences between reference (REF) and exoskeleton (EXO) conditions
Average heart rates (bpm) during dynamic work at four shoulder angles. p-value represents statistical differences between reference (REF) and exoskeleton (EXO) conditions
ns = statistically nonsignificant difference between REF and EXO.
The results for maximal grip strength, muscle stiffness, tone and elasticity, m. deltoideus PCSA and muscle fiber PA, and M-wave latency time and amplitude were mostly insignificant between REF and EXO. However, the stiffness of the upper back (m. trapezius) increased from 354.2±17.9 N/m to 365.6±20.9 N/m in EXO, compared to a decrease from 341.3±13.2 N/m to 339.9±17.9 N/m in REF at 60° shoulder angle. In addition, muscle tone of TT increased from 17.5±0.7 Hz to 18.1±0.7 Hz in EXO, whereas muscle tone remained constant at 17.4±0.6 in REF before and after the work task at 60° shoulder angle. These changes were statistically significant between the conditions (p < 0.05).
Discussion
The results demonstrated a significant reduction in muscle activity as well as HR when using the exoskeleton. The main finding of this study included reduced muscle activity up to 38% with exoskeleton compared to not using one during dynamic work performed in laboratory. Subjective evaluation of perceived exertion provided similar information on reduction of workload when using the exoskeleton.
Our results showed significant reductions of EMG activity during overhead work while wearing the passive exoskeleton. Due to the use of exoskeleton, no significant increase in muscle activity was observed in any of the muscles studied. The decrease in muscle activity was on average 22.5% when all the shoulder angles were combined. These data are in accordance with for example de Vries et al. [16] who also reported reduced muscle activity when using a similar exoskeleton for tasks involving overhead work (plastering). Also, a recent overall pooled analysis in a systematic review and meta-analysis by Bär et al. [31] showed statistically significant reduction in muscle activity of the shoulder elevators and rotators when using upper-limb-supporting exoskeletons.
The standard laboratory setting permits evaluation of the effectiveness of exoskeleton also at different fixed shoulder joint angles in simulated dynamic painting work. Overall, the reductions in % MEMG were greatest at and above shoulder level, but the exoskeleton also reduced muscle activity in dynamic work at 60° shoulder angle. On average, using the exoskeleton was most beneficial when the task was performed at 120° shoulder joint angle, where muscle activity was reduced by 25.4% on average. The corresponding reductions in average muscle activity at other shoulder angles were 21.5%, 23.6%, and 19.3% at 60°, 90°, and 150°, respectively. According to the manufacturer, Skelex 360 is designed for repetitive and static manual work at shoulder level and above. The results of the present study are in accordance with the recommendations and suggest the use of exoskeleton in overhead work tasks at elevation angles above 90° shoulder angle. In the case of 60° shoulder angle, the risks for MSDs are initially lower and, therefore, the need for exoskeleton should be evaluated on a case-by-case basis.
In dynamic work with exoskeleton, we witnessed a significant reduction in the activity of two out of eight measured muscles (i.e., m. deltoideus pars clavicularis and pars acromialis) at all the shoulder angles studied, compared to not using exoskeleton. The reduction in EMG activity was most evident in these shoulder muscles ranging from 27.5 to 38.2% for m. deltoideus pars clavicularis and from 34.1 to 38.7% for pars acromialis. The upper limb, particularly the shoulder joint, is especially susceptible to MSDs caused by repetitive [4, 32] and overhead work [33]. Shoulder disorders have a considerable impact on sickness absence [34, 35], premature withdrawal from the working life and productivity loss [36, 37]. Therefore, due to substantial reduction observed in physical workload on shoulder joint, it can be argued that the use of a passive upper limb exoskeleton has the potential to prevent shoulder complaints and, further, reduce the risk of upper extremity MSDs. Additional follow-up field studies are, however, needed to examine long-term benefits of passive exoskeletons in reducing the risks of work-related MSDs and occurrence of sickness absence.
Due to the additional mass of exoskeleton (2.7 kg), a potential increase of 1–3% in metabolic strain was expected based on Taylor et al. [38]. The present results show, on the contrary, that HR decreased up to 7.1% when using exoskeleton compared to not using one. This is consistent with previous studies by De Bock et al. [15], Maurice et al. [22] and Schmalz et al. [23] indicating statistically significant reduction in HR and oxygen consumption during short-term dynamic work tasks when the exoskeleton is used for overhead tasks. Working with hands at or above the heart level increases physiological strain causing temporal hypertension [11]. High blood pressure is one of the main risk factors for cardiovascular disease. Therefore, despite its weigh, by reducing cardiovascular load in short-term near-maximal workloads, exoskeletons may contribute to reducing work-related risk of cardiovascular disease.
To examine the effect of exoskeleton use on biomechanical and viscoelastic properties of muscle tissue, muscle stiffness, tone and elasticity were measured using a myotonometer. To our knowledge, this study is the first to also evaluate mechanical muscle properties during standardized movements with upper-limb-supporting exoskeleton. Based on our results, m. trapezius pars transversa (upper back) muscle stiffness and tone increased in dynamic work at 60° shoulder angle. The exoskeleton used in this study is worn like a backpack and, thus, the weight of the device is concentrated on the shoulder and upper back area. According to Hadid et al. [39], load bearing and carrying heavy loads on the back may increase stiffness in shoulder region. Besides the upper back muscle stiffness and tone, no other adverse physiological effects were associated with the use of exoskeleton. No differences were observed in maximal grip strength, nerve conduction velocity, nor m. deltoideus muscle PSCA or muscle fiber PA when using exoskeleton compared to working without exoskeleton.
A key strength of the present study is the wide range of different parameters measured in standardized laboratory conditions. Furthermore, different working heights and shoulder angles were used in order to better evaluate the efficacy of the exoskeleton in varying working positions. There are also some limitations in this study that should be noted. First, although HR obtained by Bodyguard2 system reaches the required level of reliability, one of the limitations of the protocol is that HR is dependent on multiple external factors, such as caffeine intake, smoking, or regular exercise habit, which may have an impact on resting, mean and peak HR during occupational physical activity. Second, since only one physically quite demanding simulated task was done in a short period of time, it remains unclear if the observed results might change for a longer-term performance. For example, the impact of movement assistance on postural control, neuromuscular coordination and joints kinematics could outweigh the benefits. Third, these results apply only to the one exoskeleton studied (Skelex 360) and the extent to which these results generalize to other passive upper limb exoskeletons is unknown.
Conclusions
We conclude that passive upper limb exoskeleton type Skelex 360 significantly reduces muscle activity, perceived exertion, and cardiovascular demand during dynamic work tasks in standardized laboratory conditions. In particular, the reduction in muscle activity was distinct in m. deltoideus and when the arm elevation was 120°. Still, we observed beneficial effects of the exoskeleton at all the measured shoulder elevation angles. Therefore, the use of an exoskeleton potentially decreases the risk for harmful effects imposed by overhead work on the shoulder area. No significant negative effects were observed, besides a minor increase in muscle stiffness in the upper back, when working with exoskeleton. Overall, these results suggest that the use of upper limb exoskeleton has the potential to reduce workload during overhead work and, further, the risks for work-related MSDs. However, more in-field research is needed to give practical recommendations on the use of exoskeletons in real working conditions.
Ethical approval
The study was conducted according to the Declaration of Helsinki of 1964 and its later amendments. Approval was obtained from the ethical committee of the Northern Ostrobothnia hospital district (EETTMK 70/2019 §215).
Informed consent
All involved subjects provided written informed consent prior to study inclusion.
Conflict of interest
The authors declare no conflicts of interest.
Footnotes
Acknowledgments
Not applicable.
Funding
This work was supported by the Finnish Work Environment Fund (grant no. 190358). The funder had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.