
Abstract
BACKGROUND:
Work-related disability is caused commonly due to musculoskeletal disorders (MSD) in dentistry. Prolonged static awkward and repetitive postures cause MSD in dentists. The study was executed to confirm the development of MSD in various body regions as they have to work in a small oral cavity to perform crucial dental procedures with precision and concentration.
OBJECTIVE:
To assess the occurrence of the MSD in several body regions of dentists and to carry out postural study thereby helping them improve posture.
METHODS:
Dentists were assessed for their current working postures with various MSD symptoms and its effects. The questionnaire was devised to get musculoskeletal health data from dentists. The postural load was investigated using Rapid Upper Limb Assessment (RULA). Various risk factors contributing to MSD symptoms were identified after data were statistically analysed using IBM SPSS version 27.
RESULTS:
According to the current study neck, shoulder, lower back, upper back, wrist hand, elbow, hip, thigh, knee, and ankle were the most affected anatomical regions. Average RULA score for the current study was found to be 6.75 which indicated a need of change of posture while performing dental procedures. There is statistical correlation between gender, Body Mass Index (BMI), uncomfortable positions, stretching, use of ergonomic saddle chair, hand dominance and MSD. There is no statistical correlation between years of experience and MSD.
CONCLUSION:
Current workstation (Dental Chair) requires immediate improvements as evident from the postural load analysis, thus immediate implementation of intervention program is required.
Keywords
Introduction
Musculoskeletal disorders (MSD) refer to a range of injuries or discomfort affecting the human musculoskeletal system. This encompasses issues concerning joints, ligaments, muscles, nerves, tendons, and supportive structures in areas such as limbs, neck, and back (CDC 2019) [1]. Ergonomics is the study of designing equipment and devices that fit the human body and its cognitive abilities. It aims to improve efficiency, comfort, and safety in the workplace or any environment where people interact with tools or technology [31].
Ergonomically awkward posture refers to body positions that deviate from the optimal alignment, leading to MSD. These positions often result from poor ergonomic design of workspaces, tools, or equipment, or from prolonged static postures.
Ergonomics and proper posture should be given utmost importance to reduce the risk of MSD, where in dentistry is a profession with high risk of developing MSD. Awkward postures are adopted by the dentists while performing the dental procedures like root canal, extraction of mandibular and maxillary teeth (Refer Fig. 1). Dentists carry out various dental procedures either in seated or standing working positions. Dentists need to have a proper grip over the major instruments used, including mouth mirrors, periodontal probes, low and high speed hand pieces, explorer, forceps etc. (Refer Fig. 2).

Dentists ‘Awkward postures: a) Filling of left 2nd Molar Maxillary; b) Root Canal dressing of Mandibular right 1st Molar; c) Extraction of Left lower 2nd Molar Mandibular; d) Extraction of Right lower 2nd Molar Mandibular; e) Extraction of Right 2nd Molar Mandibular; f) Filling of left 2nd Molar Mandibular.
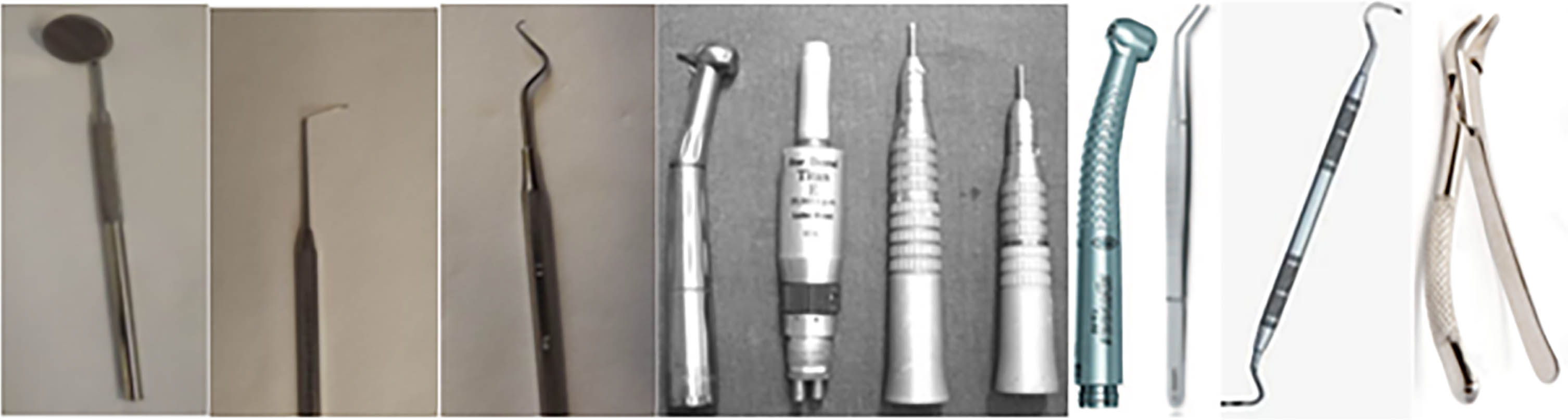
Instruments used by the dentists while performing the dental procedures.
Dentists’ working hours vary depending on dental procedures and number of patients. Those dentists who work continuously for longer period of time with improper posture significantly experience increased risk of Work-Related Musculoskeletal Disorders (WRMSD). Large number of studies have reported the occurrence of various WRMSD among dentists in India [17, 20]. Current study was carried out in Western Maharashtra (Kolhapur Region) which indicates prevalence of MSD and its impact on occupational health of dentists. There is no reported evidence of such study in this region. Considering above factors, this study was designed with identification of postural load and its relation with occurrence of WRMSD as an objective. Present study aims 1) To find dental procedures 2) To identify various postures undertaken 3) To determine the occurrence of MSD and its correlation with various factors including years of experience, Body Mass Index (BMI), stretching exercises, uncomfortable postures.
Ethical consideration: Ethical statement is not required as no experiments were carried out on participants which would cause any harm. Consent was taken from the participants before the interview/questionnaire session, during which they were informed about the current study, questions, confidentiality and right to withdraw.
Members of Kolhapur District Dental Association participated in this study. Approximately 348 dentists work in Kolhapur district [21]. The sample size of 76 respondents is required based on confidence level of 95%, margin of error of 10% for 348 population size. Questionnaire was sent to 100 dentists with minimum of one year work experience, out of which 79 responded, among them 31 were female and 48 were male. The questionnaire covered major points including demographic data, factors affecting MSD, use of ergonomic instruments and its effects on MSD. Symptoms of MSD and its effect on dental practice, effects of awkward postures on MSD, rest breaks and its effects on MSD, importance of exercise and ergonomics training to reduce MSD and improve health, dental procedure and the tooth that caused maximum fatigue. The 5 point Likert scale was used to measure the severity of MSD in 9 anatomical regions. Moreover the working duration, number of years of experience of dentist along with their specification were taken into consideration for this study. Total of 38 questions were included in the questionnaire. Approximately 10 minutes were required to complete the questionnaire effectively. Photographs were taken to collect the real time data about the awkward postures of the dentist performing dental procedure.
All dentists were made familiar with the study and the doubts were cleared by the author. Inclusive criteria was work experience of at least 12 months of duration, dentists carrying out the tasks while standing and sitting, institutional and private practitioners, various specializations of dentists, different age, height and weight, gender. Data were collected using both direct observations and Nordic Musculoskeletal Disorder questionnaire [11]. The questionnaire was completed online by the respondents. Working postures of the dentists were evaluated through observations at the respective clinics. After describing objective of this study, consent was obtained from each dentist. Statistical data were analysed by using IBM SPSS version 27 software. Chi square test was used to determine the correlation between risk factors and severity of MSD.
Results
Sociodemographic factors which represent the gender data of the dentists include 79 subjects, out of which 48 (61%) were male and 31 (39%) were female. Demographic data of the dentists are as follows. Dentists’ age were ranging from 26 to 53 years (mean = 35.37 years; SD =±6.76 years). The average height and weight of the dentists were 163.74±24.71 cm and 70.31±11.98 kg respectively.
Job specifications of the dentists include 64% of dentists having job experience between 1–10 years, 22% of dentists having job experience between 11–20 years and 14% of dentists having job experience between 21–30 years. Their daily working hours reported were with a mean of 6.75 hours and SD±1.83 hours. Their weekly working days reported were with mean of 6.02 days and SD±0.37 days. Number of patients per day reported were with mean of 10.50 and SD±8.03. 32.9 % of the dentists worked without interruption for more than 40 minutes. Data revealed that almost 97% of the dentists reported MSD symptoms.
Out of 127 total incidences, 60 (47%) incidences reported excessive fatigue in neck and shoulder, 16(13%) reported numbness in fingers and hands, 11(9%) reported tingling, burning sensation in arms, 11(9%) reported cramping of hands, 10(8%) reported weak grip, 7(6%) reported clumsiness and dropping of objects, 6(5%) reported fatigue in upper and lower back, 2(2%) reported eye straining and 1(1%) reported finger pain.
Intensities of MSD problems in various body regions which were rated using 5 point Likert scale in percentage (Scale of 1 being least intense and 5 being the most) in nine anatomical region are shown in Fig. 3.
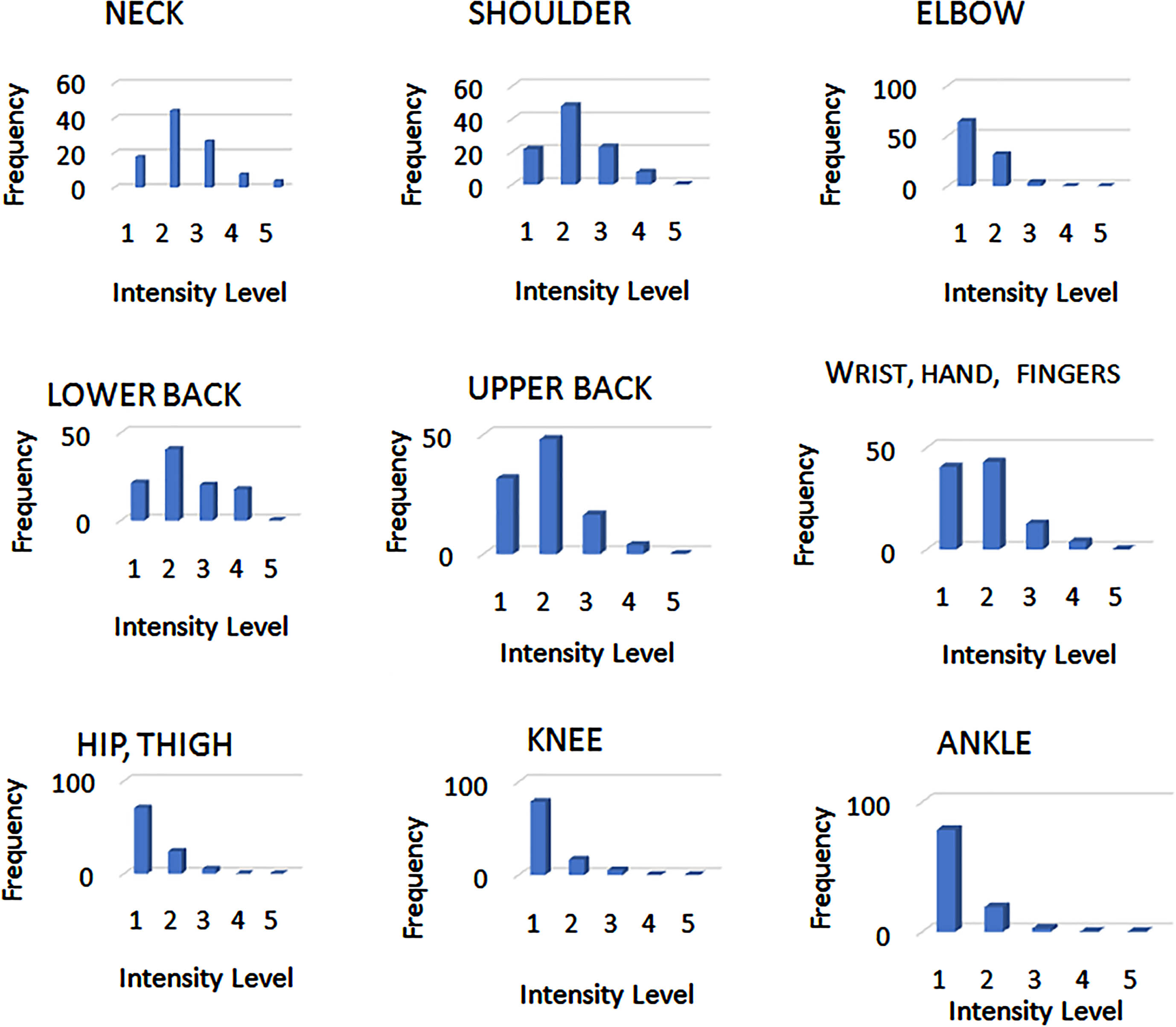
Intensity level of musculoskeletal discomfort in the body parts.
Table 1 represents RULA scores distribution. This score is one of the indicators which shows that majority of the dental chairs are ergonomically not suitable for dental procedures for long durations. As per the study, need of changing the workstation is required to avoid ergonomically awkward position thus reducing occupational risks [28].
RULA scores frequency distribution (n = 79)
This study shows that dentists work continuously for longer period of time which typically ranges from 3 to 12 hours daily. Prolonged periods of working with improper posture significantly increases the risk of work-related musculoskeletal disorders (WRMSD).
This study indicates root canal and tooth extractions are the most frequently carried out dental procedures. Root canal and tooth extractions have a RULA score of 6.75 and 6.7 respectively which indicates further need of investigation change in posture.
The outcome of this study specifies that neck pain (n = 64) and shoulder pain (n = 61) were highly prevalent among the dentists followed by lower back (n = 61), upper back (n = 53), wrist hand (n = 47), elbow (n = 27), hip thigh (n = 22), knee (n = 16) and ankle (n = 16) which was similar to a study conducted [5] (Refer Figs. 4–6).
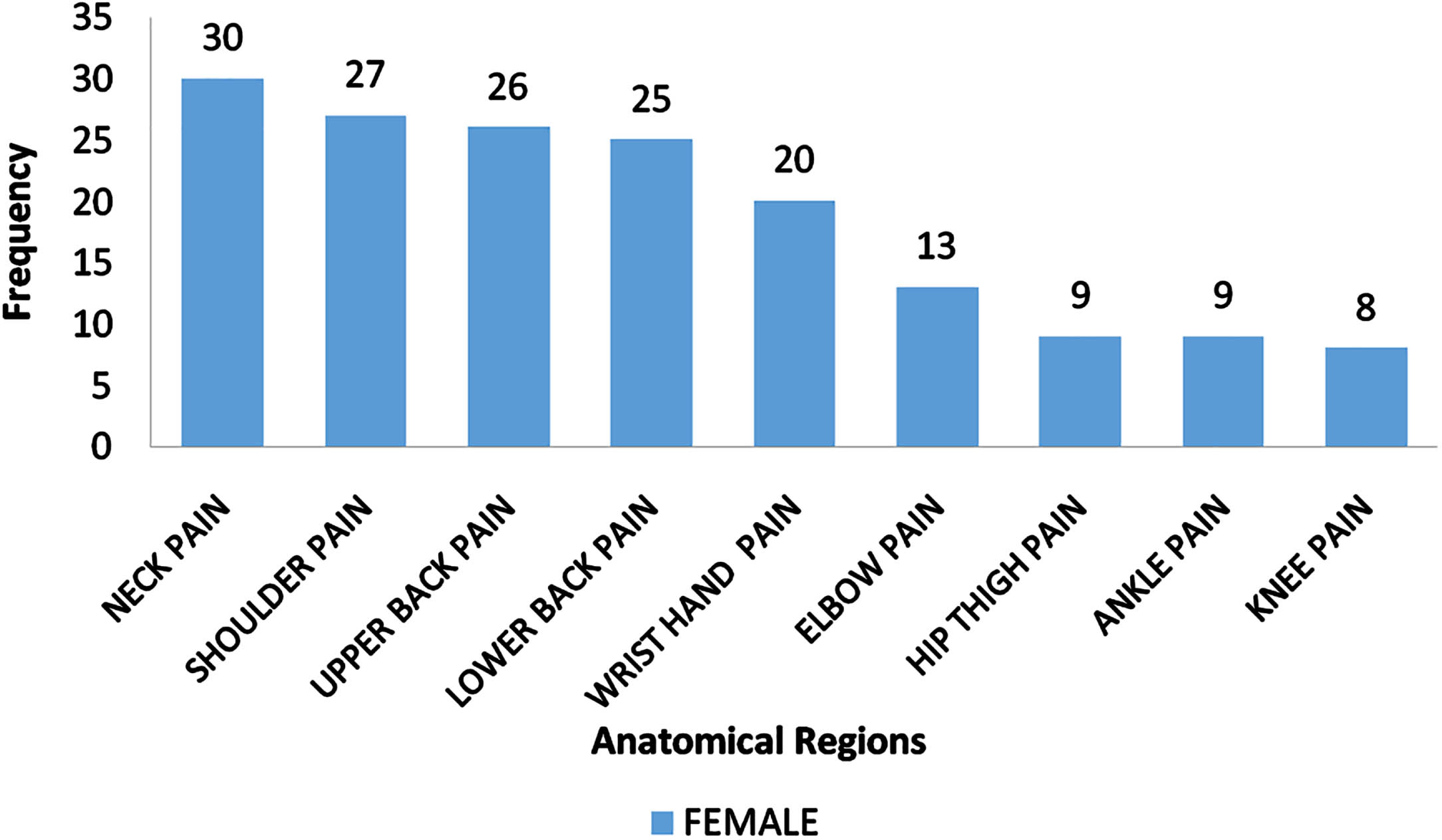
Anatomical region vs frequency of pain incidences for female dentist.
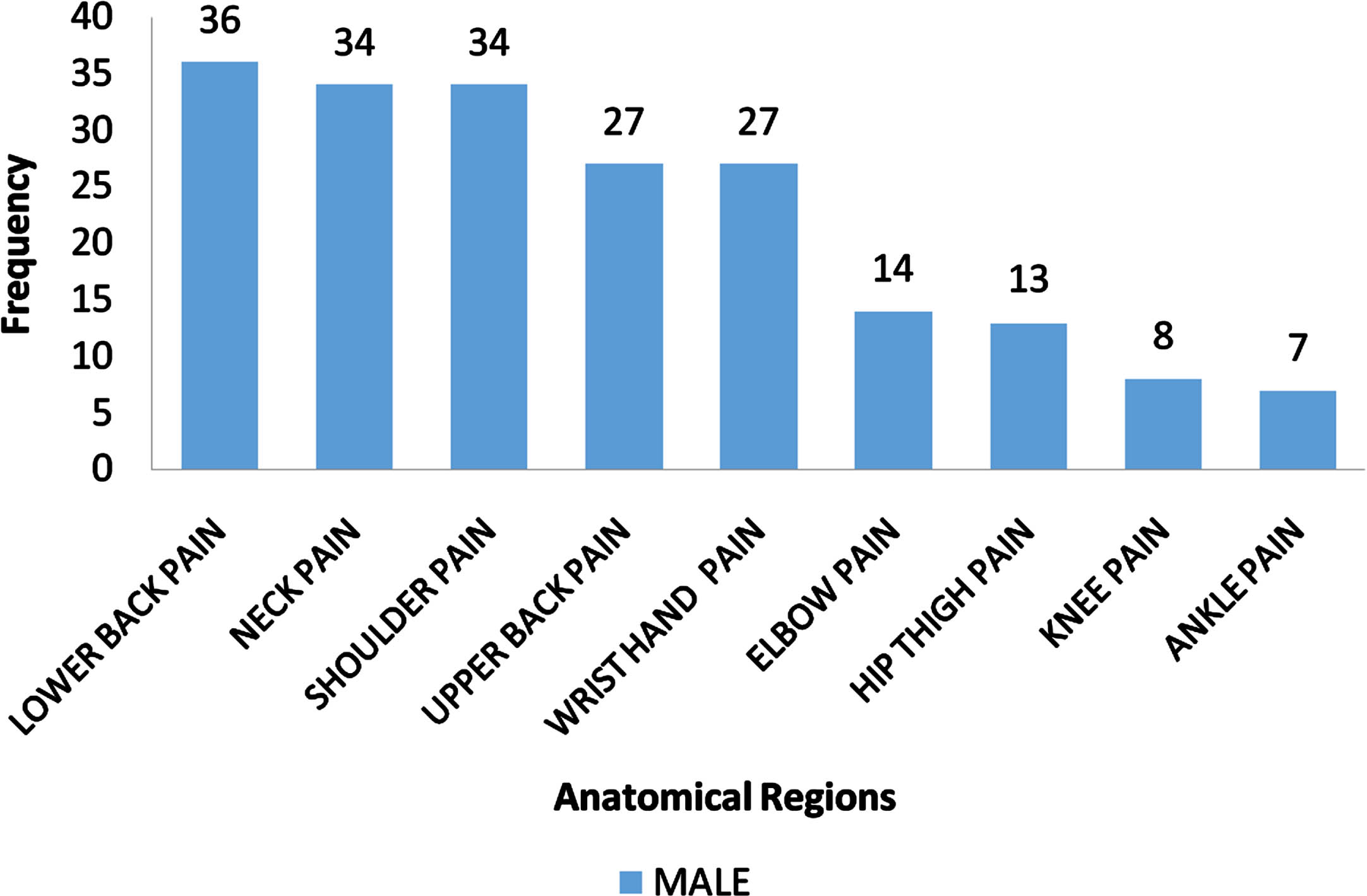
Anatomical region vs frequency of pain incidences for male dentist.
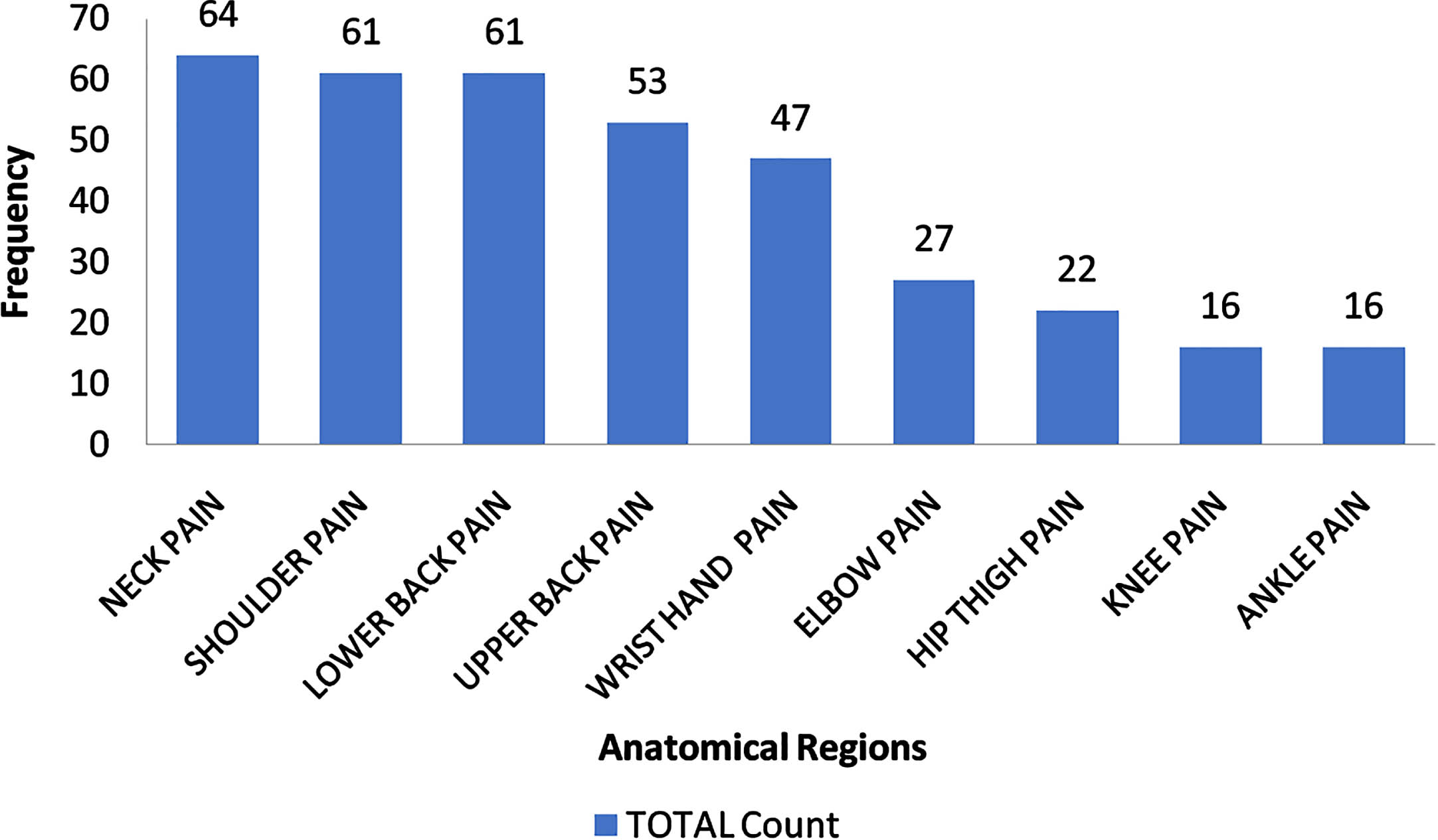
Anatomical region vs frequency of pain incidences for overall population of dentist.
Table 2. Summarises the severity of musculoskeletal symptoms across nine anatomical regions among male and female dentists. Statistically, there is significant correlation between gender vs neck pain (Chi square value = 7.572 and p = 0.006 (<0.05)) and gender vs upper back pain (Chi square value = 5.989 and p = 0.014 (<0.05)). Significantly more number of females have been affected for neck pain and upper back pain than males. There is no correlation between gender vs shoulder pain (Chi square value = 2.386 and p = 0.122 (>0.05)), elbow pain (Chi square value = 1.218 and p = 0.27 (>0.05)), lower back (Chi square value = 0.18 and p = 0.672 (>0.05)), wrist hand fingers pain (Chi square value = 0.39 and p = 0.532 (>0.05)), hips and thighs pain (Chi square value = 0.017 and p = 0.895 (>0.05)), knee pain (Chi square value = 0.884 and p = 0.347 (>0.05)) and ankle pain (Chi square value = 2.29 and p = 0.13 (>0.05)).
Severity of musculoskeletal indications informed by dentists (n = 79)
Statistically, there is no correlation between years of experience and neck pain (Chi square = 0.757, p = 0.629 > 0.05), Shoulder Pain (Chi square = 1.828, p = 0.381 > 0.05), Elbow (Chi square = 2.688, p = 0.255 > 0.05), Upper back (Chi square = 1.657, p = 0.436 > 0.05), Lower back (Chi square = 2.503, p = 0.314 > 0.05), wrist and hand (Chi square = 4.767, p = 0.111 > 0.05), Hips and thighs (Chi square = 2.002, p = 0.410 > 0.05), knees (Chi square = 0.472, p = 0.844 > 0.05) and ankles (Chi square = 1.997, p = 0.387 > 0.05)(Refer Table 3). Dentists having 0–10 years of experience reported the neck (41) as most impacted anatomical region followed by shoulder (40), lower back (39), upper back (35), wrist hand (25), elbow (14), hip thigh (13), knee (10) and ankle (9) in descending order. Dentists having 11–20 years of experience reported the neck (15) as most impacted anatomical region followed by wrist (14), shoulder (12), lower back (12), elbow (9), hip thighs (5), knees (3) and ankle (3). Dentists having 21–30 years of experience reported the lower back (10) as most impacted anatomical region followed by shoulders (9), neck (8), upper back (8), wrist hand (8), hip thighs (5), elbow (4), ankle (4) and knees (3). (Refer Fig. 7).
Musculoskeletal indications compared to years of experience
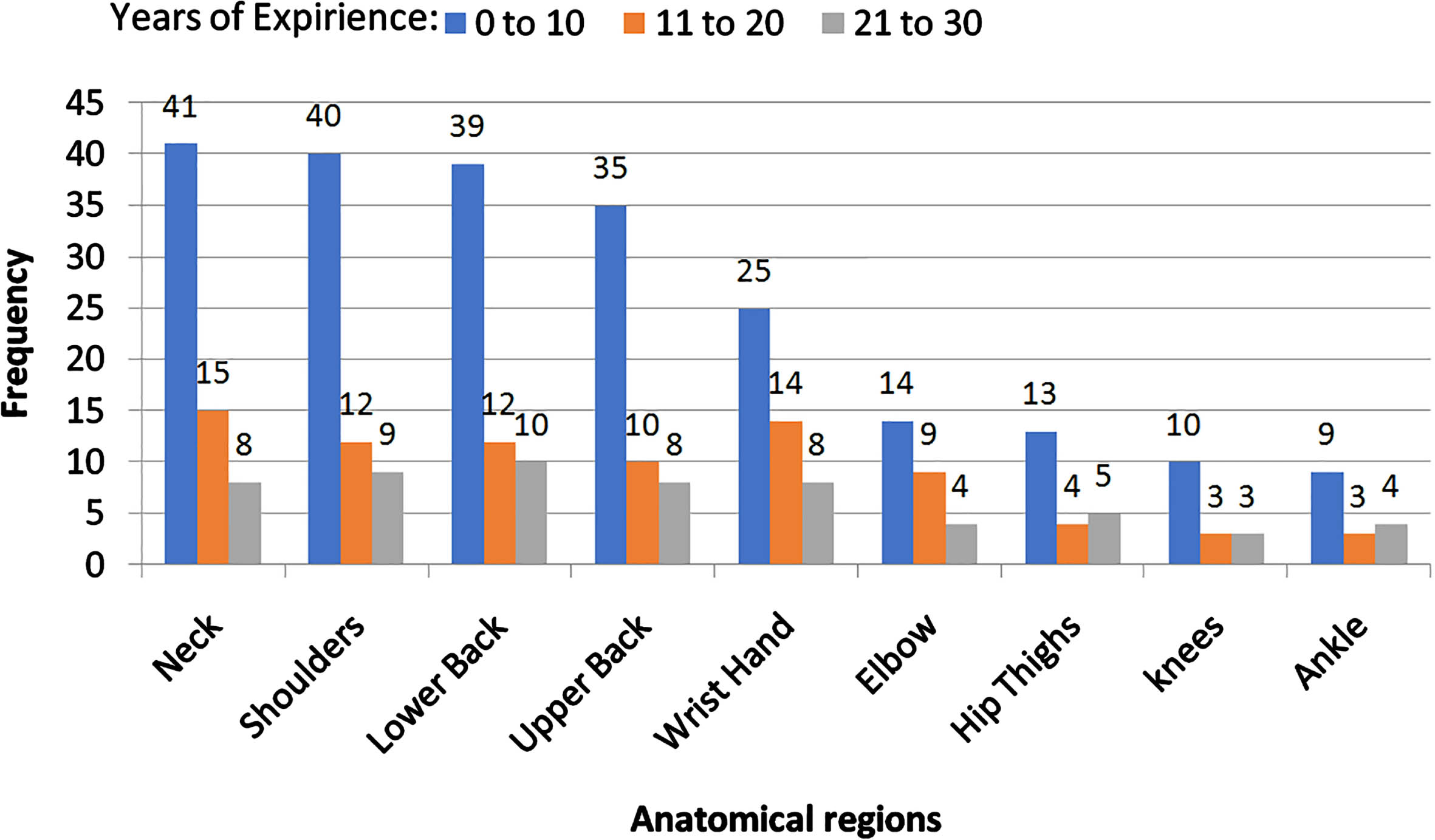
Years of experience vs MSD in anatomical region for overall population of dentist.
Statistically, there is significant relation between BMI vs upper back (Chi square value = 8.62 and p = 0.013 (<0.05)) and BMI vs lower back (Chi square value = 8.62 and p = 0.013 (<0.05)). Significantly more number of respondents with higher BMI have been affected by upper back (n = 35) and lower back (n = 35) pain than the respondent with normal BMI for upper back (n = 21) and lower back (n = 22) pain.
Table 4 shows correlation between musculoskeletal disorders in nine anatomical regions and BMI. Statistically there is no correlation between BMI vs neck (Chi square value = 1.164 and p = 0.567 (>0.05)), shoulder (Chi square value = 0.964 and p = 0.624 (>0.05)), elbow (Chi square value = 2.255 and p = 0.103 (>0.05)), wrist (Chi square value = 3.319 and p = 0.194 (>0.05)), thighs (Chi square value = 0.748 and p = 0.270(>0.05)), knees (Chi square value = 0.457 and p = 0.346 (>0.05)) and ankles (Chi square value = 1.014 and p = 0.234 (>0.05)). Another study shows that there is correlation of age, BMI, and years of experience with the musculoskeletal pain which are partially consistent with this study [4]. Excess body weight puts increased stress on the joints, leading to a higher risk of developing musculoskeletal issues [26].
Musculoskeletal symptoms compared to BMI
Table 5 highlights the effect of uncomfortable positions especially on upper and lower back. There is significant correlation between dentists sitting position (flexed or twisted torso), lower back (Chi square = 17.884 and p = 0.001 < 0.05) and dentists sitting position (flexed or twisted torso), upper back (Chi square = 23.45 and p = 0.004 < 0.05).
Effect of uncomfortable positions on upper and lower back
Table 6 shows the effect of stretching on the nine anatomical regions. Statistically, there is significant correlation between stretching exercises vs neck (Chi square value = 13.393 and p = 0.001(<0.05)), shoulders (Chi square value = 6.791 and p = .032(<0.05)) elbow (Chi square value = 9.176 and p = 0.02(<0.05)), upper back (Chi square value = 8.174 and p = 0.015(<0.05)), lower back (Chi square value = 5.615 and p = 0.05(<0.05)) wrist and hand (Chi square value = 11.265 and p = 0.03(<0.05)).
Effect of stretching on the nine anatomical regions
Table 7 shows effect of use of ergonomic saddle chair on nine anatomical regions. There is significant correlation between use of ergonomic saddle chair and pain in lower back (Chi square = 8.326, P = 0.018 < 0.05). Statistically there is no correlation between use of ergonomic saddle and pain in neck (Chi square = 1.96, P = 0.415 > 0.05), shoulder (Chi square = 1.482, P = 0.519 > 0.05), elbow (Chi square = 3.625, P = 0.057 > 0.05), upper back (Chi square = 4.634, P = 0.170 > 0.05), wrist (Chi square = 3.184, P = 0.128 > 0.05), thigh (Chi square = 1.479, P = 0.172 > 0.05), knee (Chi square = 1.592, P = 0.234 > 0.05), ankle (Chi square = 1.592, P = 0.415 > 0.05) (refer Table 7).
Effect of use of ergonomic saddle chair on nine anatomical regions
Table 8 represents effect of hand dominance on nine anatomical regions. There is a significant correlation between hand dominance and occurrence of MSD in neck (Chi square = 11.65, p = 0.015 < 0.05), upper back (Chi square = 11.75, p = 0.012 < 0.05), lower back (Chi square = 10.43, p = 0.026 < 0.05) and wrist (Chi square = 11.49, p = 0.015 < 0.05). Statistically there is no correlation between hand dominance and occurrence of MSD in shoulder (Chi square = 0.296, p = 1 > 0.05), elbow (Chi square = 3.038, p = 0.117 > 0.05), thighs (Chi square = 0.021, p = 0.685 > 0.05), knees (Chi square = 0.052, p = 0.609 > 0.05), ankle (Chi square = 0.052, p = 0. 609 > 0.05) (Refer Table 8).
Effect of hand dominance on nine anatomical regions
The current study revealed that the awkward static repetitive postures of the dentist while performing the dental procedures were ergonomically not suitable thus inducing MSD in various anatomical regions majorly in neck, shoulder followed by upper back, lower back, thighs, knees, ankles. Musculoskeletal disorders can limit work capacity, requiring expensive medical treatment. In some cases, full recovery is not possible, leading to early retirement [2].
Most of the common symptoms reported were excessive fatigue in shoulder, neck, upper back, lower back and numbness in finger and hands. This study revealed that the pain affected the routine of the dentist leading to reduced working hours, increased number of breaks. The number of parameters like prolonged static awkward postures, no stretching exercises performed between two successive treatments and obesity were associated with musculoskeletal symptoms in some body regions [4, 7].
Musculoskeletal disorders include disc problem, Spondylitis, Sciatica, Carpel tunnel syndrome, Tennis Elbow. Muscle disorders in areas of head and neck are caused due to frontal flexion of the head and elevated limbs. Musculoskeletal disorders are mainly located in neck and shoulders [27]. Prolonged sitting is a critical factor which causes lower back pain. Conventional sitting has numerous adverse effects including a flattened lumbar curve, a pelvis tilted posteriorly and increased lower back compressive load. Muscle fatigue and pain are caused due to upright sitting. Spinal loading is increased in slumped sitting, which is further exaggerated by excessive contractions of spinal muscles. Slumped sitting posture leads to greater head and neck flexion. Prevalence of musculoskeletal symptoms were further transformed to alarming musculoskeletal disorders which would cause difficulties in activities for the body regions [30]. High RULA score while performing the dental procedures with the dental chair suggests immediate or near future investigation. Thus the analysis of dentists’ posture and position of the dental chair is required to be prioritised. The postures adopted by dentists scored between 3–7, therefore none of the posture was acceptable according to RULA Method [20].
A study conducted among Egyptian dentists revealed that MSDs has affected the dentists in their work performance, reduction in daily activities, taking analgesic, hospitalization and surgical interference [3] Further neck and shoulder area were the most prevalent region of pain, while the second highest region of pain was the lower back which was similar to the this study [13]. Another study highlighted that dentists commonly report significant discomfort in their neck, along with discomfort in the lower back, hand, and wrist leading to MSD [27]. The author found that highest frequency of MSD among dentist irrespective of their specialisation, the neck was the most commonly affected region [14] which is similar to this study. The most common anatomical regions reported were the neck, shoulder and lower back [15, 17]. Females reported more musculoskeletal problems than males [16]. Neck pain was most prevalent in women than men [17]. A study indicates a substantial association between MSD and the female gender [22]. The consensus among female participants was that they experienced pain significantly more often [23].
This study further analysed the effects of lack of awareness of ergonomics during the early years of their practice on MSD which was in continuation with the study [7]. This shows that knowledge about ergonomics and workplace modifications can reduce the occurrence of MSD. Furthermore another study explained that ergonomic training improved the working postures in dentistry [8].
Prolonged static postures without break has been shown to be associated with neck problems among the dentists. Another study shows that, pain in more than two anatomical regions were reported in dentists who examine more than eight patients as compared those who examine less than 8 patients daily [9]. This study shows that inappropriate working posture is one of the contributing factors for development of musculoskeletal symptoms.
A study shows that young and less experienced dentists are more prone to high rates of MSD due to lack of professional experience and improper postures during work which does not match the current results [12]. A lower percentage of musculoskeletal disorders (MSD) was found in dentists of a higher age group [6]. The neck and the upper back were the common areas that were involved in occurrence of MSD [18]. Study shows that age or years of experience were not significantly related to MSD [19] which is exactly similar to this study.
Implementation of training and awareness program is essential for reducing the prevalence of MSD among dentists and prolong their dental practicing careers [8]. Another study shows that 67% of dentist don’t perform stretching exercises between two successive treatments and thus are prone to musculoskeletal disorders. Furthermore it was evident that consistent work rest patterns contribute positively to musculoskeletal health in dental practice [13]. The another study found that dental professionals who practiced yoga or stretching as physical activities showed a lower prevalence of work-related musculoskeletal disorders (WMSD) at 77%, in contrast to those who engaged in other physical activities, where the prevalence of WMSD was higher at 84% [25].
It was found in this study that majority of the dentists face difficulty while treating Maxillary teeth as compared to mandibular. Furthermore posture wise maxillary premolars are the most difficult teeth to be treated (Refer Fig. 8).
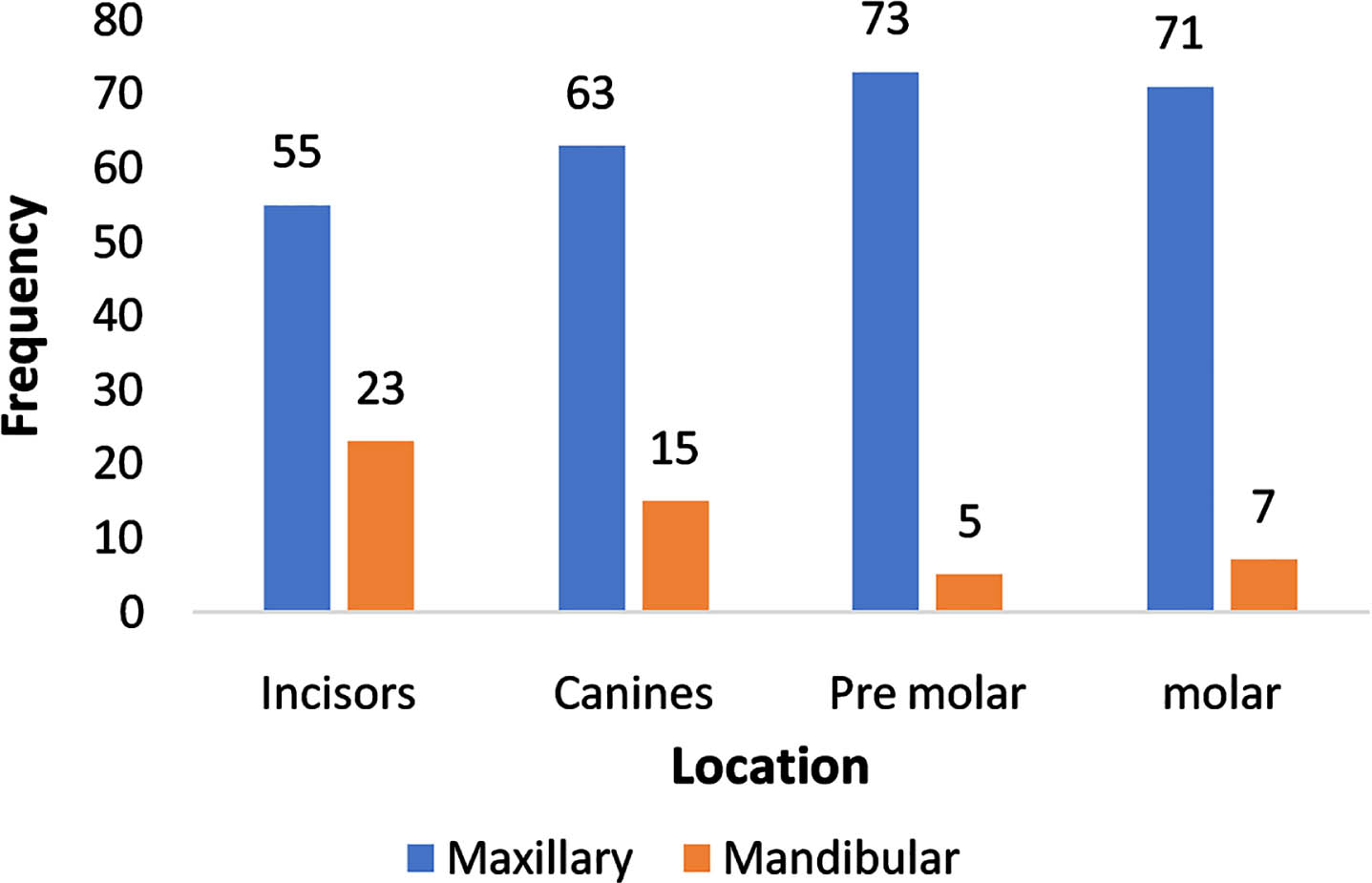
Number of dentists perceiving difficulties for dental procedures at maxillary vs mandibular location of incisors, canines, premolars and molars.
This study shows that the dentistry is the origin of the WMSDs of the dentists and there is immediate need of ergonomic intervention for improvement of dentists’ occupational health. As mentioned by the author due to lack of availability of proper anthropometric data and limited infrastructure support to ergonomic activities and intervention in developing countries, a simple low cost ergonomic solution should be implemented to improve working conditions [10]. Thus, it is necessary to provide cost effective ergonomic equipment (dental chair) which will contribute in maintaining occupational health of the dentist. Research findings emphasize the crucial role of dental health care providers recognizing and implementing appropriate ergonomic postures early in their careers to mitigate work-related MSD [24]. Emphasizing awareness, training, and hazard reduction is crucial for the effectiveness of MSD prevention practices [29].
This study shows that only 5% of the dentists used both standing and sitting postures. Sitting is the most common position used by both institutionalized and private practitioners. Recent dental chairs have a lot of modifications available as per requirements but it was observed that none of the dentists used any adjustment to keep his/her posture normal.
According to the study conducted there is a correlation between BMI and MSD. The dentists with higher BMI are prone to MSD. This study revealed that there is significant correlation between stretching and anatomical regions including neck, shoulder, upper back, lower back, wrist and hand respectively. Stretching excercises thus reduces the occurrences of MSD prominently in neck and shoulders. There is significant correlation between twisted torso and pain in lower and upper back. There is no correlation between years of experience and MSD. There is significant correlation between gender vs neck and upper back pain. More number of females are affected for neck pain and upper back than male. This study shows that pain in anatomical regions due to MSD reduced working hours and increased number of breaks.
This study shows that dentists having less experience found the task of performing dental procedures to be strenuous. The real time observations and discussion with dentists revealed that the root canal and the tooth extractions were the most frequently performed procedures. The activities to be carried out in coordination with these procedures were monotonous and repetitive in nature. Maxillary premolar teeth are the most difficult to treat.
Considering the above findings and as evident from the postural load analysis, it is required to implement improvement in current workstation (Dental Chair) design. Immediate need of implementation of intervention program is required.
Ethical approval
Not applicable.
Informed consent
Consent was taken from the participants before the interview/questionnaire session, during which they were informed about the current study, questions, confidentiality and right to withdraw.
Conflict of interest
The authors declare no conflict of interest.
Footnotes
Acknowledgments
The authors express their gratitude to the participants of the study who gave us an unconditional support. We are thankful to the chairman of Indian Dental association Kolhapur for their valuable guidance.
Funding
This study has not been funded by any organisation.