
Abstract
BACKGROUND:
Psychological issues and work-related violence are the main challenges faced by medical staff. The situation has become even more prevalent during the COVID-19 pandemic.
OBJECTIVE:
This research aimed to analyze the relationships among work-related violence, occupational stress and psychological distress and to further identify the direct or indirect effects of violence on psychological distress.
METHODS:
A total of 1,765 medical staff members were surveyed using the Kessler Psychological Distress Scale and Revised Occupational Stress Inventory. Work-related violence was assessed using a self-made 5-question questionnaire. STATA 14.0 and Amos 21.0 software were used for correlation analysis, variance analysis, and structural equation modeling analysis.
RESULTS:
A total of 66.1% of the medical staff suffered workplace violence, and 61.2% witnessed workplace violence. The psychological distress score (Kessler 10 Scale) of the medical staff was 22.7±7.67. The psychological strain score and physical strain score were 26.8±7.14 and 24.2±6.51, respectively. Work-related violence (suffered: β= 0.467; witnessed: β= 0.258) and occupational stress (psychological strain: β= 0.269; physical strain: β= 0.317) were predictors of psychological distress, and social support (β= –0.265) was a protective factor. Work-related violence and social support had both direct and indirect effects on psychological distress, and the intermediate factor was occupational stress. The total effects of suffered workplace violence and witnessed workplace violence were 0.181 and 0.092, respectively, and the total effect of social support was –0.262.
CONCLUSIONS:
Work-related violence may exacerbate symptoms of occupational stress and psychological distress. Reducing workplace violence and protecting medical staff from work-related violence are extremely important aspects of mental health prevention.
Introduction
Work-related violence refers to any situation in which people are abused, threatened or assaulted in professional activities. Violence in healthcare facilities is a serious threat facing medical staff worldwide [1]. In a national study in Australia, 70.6% of doctors had experienced non-physical violence, and 32.3% had experienced physical aggression [2]. In another survey conducted by two large hospital systems in Texas and North Carolina, 39% of medical staff experienced workplace violence [3]. Violence against medical staff is particularly common and severe in China. A survey of 22,213 doctors in 31 provinces across China showed that 33.5% of the doctors had experienced medical disputes in the past 12 months [4]. Another study of nurses reported that the incidence of work-related violence was 65.8%, including 11.8% physical violence [5]. A meta-analysis estimated the prevalence of violence in China was 62.4% [6]. The situation has become even more prevalent during the COVID-19 pandemic [7, 8]. The negative effect of work-related violence in healthcare facilities is serious and far-reaching. It has been reported that lifestyle, sleep disorders, and turnover intentions of medical staff are negatively affected by violence [9, 10]. Nurses who suffered workplace violence also had a high risk of headache, fatigue syndrome and sleep problems [11, 12]. In addition to physical harm and immediate health effects, the impact of violence on occupational stress and mental disorders cannot be ignored.
Occupational stress refers to the physiological and psychological strain brought about by the imbalance between objective needs and personal adaptability under specific work conditions. It is the strengthening of both mental and physical reactions to external events. It has been reported that the perceived stress of medical staff increased after exposure to violence and peaked at 1 month [13]. Yao et al. [14] also reported that practice years and violence in the workplace aggravated occupational stress. In addition, Afshari et al. [15] found that some types of workplace violence, such as physical assault and bullying/harassment, were associated with occupational stress. In addition, research has suggested that stress may be an intermediary factor in some secondary health problems. Rasool et al. [16] revealed that workplace violence negatively affects occupational stress and sustainable job performance, with stress as a mediating factor. Work-related violence negatively affects the self-reported sleep quality and subjective health status of medical staff, and stress plays a partial mediating role in the relationship between violence and sleep quality and subjective health status [17].
Psychological distress is a term used to describe a range of symptoms or experiences related to non-specific mental disorders that are commonly held to be troubling, confusing or out of the ordinary. It has been reported that work-related violence is positively correlated with anxiety and depression levels in nurses [18]. Posttraumatic stress disorder (PTSD) in psychiatric workers is positively linked to both workplace violence and job stress [19]. A longitudinal study also showed that PTSD, anxiety symptoms, and depression scores of medical staff were all elevated after violence [13]. At the same time, evidence has shown that work-related violence can cause a range of potential mental health issues, such as burnout, PTSD, depression and even suicide [20, 21]. A systematic review showed that compared with nurses who were not exposed to workplace violence, those who had experienced violence were more likely to report PTSD and burnout [22]. In addition to suffering workplace violence, whether witnessed workplace violence has an impact on psychological distress is one of the issues we are interested in. A survey conducted among practicing nursing students showed that those who had not witnessed violence had more positive attitudes toward the nursing profession than those who had witnessed violence [23].
However, how to prevent and reduce injuries and the series of long-term effects caused by violence in healthcare facilities is the focus of our attention. Few studies have examined the potential paths and mediating effects between workplace violence (suffered violence and witnessed violence), occupational stress, and psychological distress. Evidence has shown that many health issues are secondary to external stressors [17, 21], and social support usually acts as a negative moderator [24, 25]. Moreover, some studies have shown that violence and stress are cyclically correlated in physicians and in nurses: violence causes stress, and the distressed worker is more exposed to violence than others. Social support has a very important role [26]. Does violence in the workplace contribute to the psychological distress of medical staff through specific intermediary factors, such as occupational stress or social support? What the differences in the effect size and pathways are of suffered and witnessed workplace violence in contributing to the above health problems? The purpose of this study was to analyze whether suffered workplace violence and witnessed workplace violence in healthcare facilities increase the risk of occupational stress and psychological distress of medical staff, as well as the differences in the potential pathways and mediating effects of occupational stress and social support on psychological distress. This study aims to provide evidence for workplace violence intervention and health promotion for medical staff.
Methods
Study population
A total of 1,881 medical staff members in China were included in the cross-sectional survey. In the first stage, 15 public hospitals were selected by a convenience sampling strategy. Based on the department settings and number of medical staff in each hospital, a stratified random sampling method was adopted to select participants in the second stage (Table S1).
Inclusion criteria: participants included in this study should have worked for at least 1 year. The occupations of the participants included doctors and nurses. Exclusion criteria: medical interns and administrators of hospitals were not included in the study. The research also excluded retirees and rehires. The research team conducted the survey in collaboration with the personnel department of each hospital. The personnel department of each hospital was responsible for communication and coordination with medical staff, while the research group was responsible for providing guidance. The questionnaire was self-completed by the participants.
Data on demographic characteristics and work-related violence were collected by two self-made questionnaires. Psychological distress and occupational stress of medical staff were measured by two standard scales. A total of 1,765 medical staff were finally included in the research, and 116 were excluded for not completing all the investigations. The qualified rate of the questionnaire was 93.8%.
All participants gave informed written consent to participate voluntarily in the survey. This study was approved by the Ethics Committee of the West China School of Public Health, Sichuan University (No. Gwll2021070). We confirmed that this research was performed in accordance with the relevant guidelines and regulations of the Declaration of Helsinki.
Outcome measurements
Work-related violence, including suffered workplace violence and witnessed workplace violence in the past 12 months, was assessed using a self-made questionnaire. The questionnaire is provided in the Supplementary material (Table S2). For each question, 0 points indicated none, 1 point indicated 1 time, 2 points indicated 2 to 3 times, and 3 points indicated 4 or more times. Higher scores indicate more severe exposure to workplace violence. The internal consistency reliability coefficients of suffered workplace violence and witnessed workplace violence were 0.783 and 0.849, respectively.
Occupational stress was measured using a simplified Chinese version of the Occupational Stress Inventory-revised edition (OSI-R) [27]. The OSI-R consists of 14 dimensions in total, each dimension has 10 items, and each item is scored from 1 to 5 points. Due to the time constraints of the survey. Only three dimensions, including social support, psychological strain and physical strain, were chosen, and all the items of three dimensions were retained to ensure construct validity. The internal consistency reliability coefficients of social support, psychological strain and physical strain in this study were 0.919, 0.869 and 0.791, respectively.
The Kessler Psychological Distress Scale is a well-known scale for mental health screening in population surveys [28]. The Chinese version of the 10-item Kessler Psychological Distress Scale (Kessler 10 Scale) was used to measure the psychological distress of medical staff [29]. The Chinese version of the Kessler 10 Scale measures the frequency of experiencing symptoms related to non-specific mental disorders, such as anxiety and depression, over the past four weeks. The scale has 10 items, and each item is scored from 1 to 5 points. Higher scores on all items indicate a higher risk of mental illness. The scores are divided into four grades: 10 to 15 is very low risk, 16 to 21 is low risk, 22 to 29 is high risk, and 30 to 50 is very high risk [30]. The internal consistency reliability coefficient in this study was 0.924.
Statistical analysis
STATA 14.0 and Amos 21.0 software were used for analysis. The statistical analysis methods used in this study included correlation analysis, multivariate regression, and structural equation modeling (SEM) analysis. SEM was used to analyze the potential pathways and specific effect sizes of work-related violence, occupational stress and external support on psychological distress. SEM can also be used to identify intermediate factors in a specific regression model. The fitting parameters for SEM include the ratio of chi-square degrees of freedom (χ2/df, <3), goodness-of-fit index (GFI, >0.9), normed fit index (NFI, >0.9), relative fit index (RFI, >0.9), comparative fit index (CFI, >0.9), incremental fit index (IFI, >0.9) and root mean square error of approximation (RMSEA, <0.05). The test model needs repeated fitting and correction to check whether the fitting parameters meet the requirements. If the fitting parameters meet the above criteria, the regression model is considered to be an ideal model. P < 0.05 indicated that the difference was statistically significant.
Results
Demographic characteristics of the participants
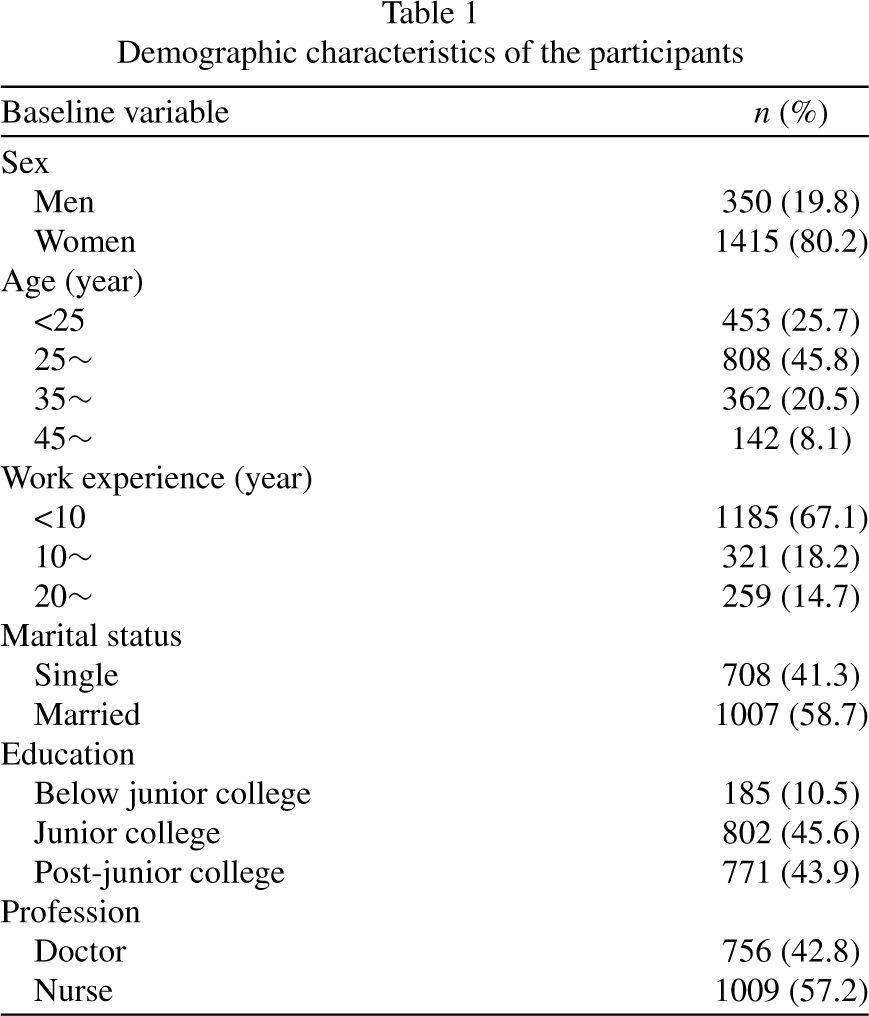
The majority of the 1,765 participants were women, and only 19.8% (350/1,765) were men (Table 1). The age of participants ranged from 18 to 64 years old. The average age was 30.9±8.34 years, and the average working life was 9.1±8.42 years. A total of 58.7% of the participants were married, and 43.9% had a post junior college degree.
Demographic characteristics of the participants
Demographic characteristics of the participants
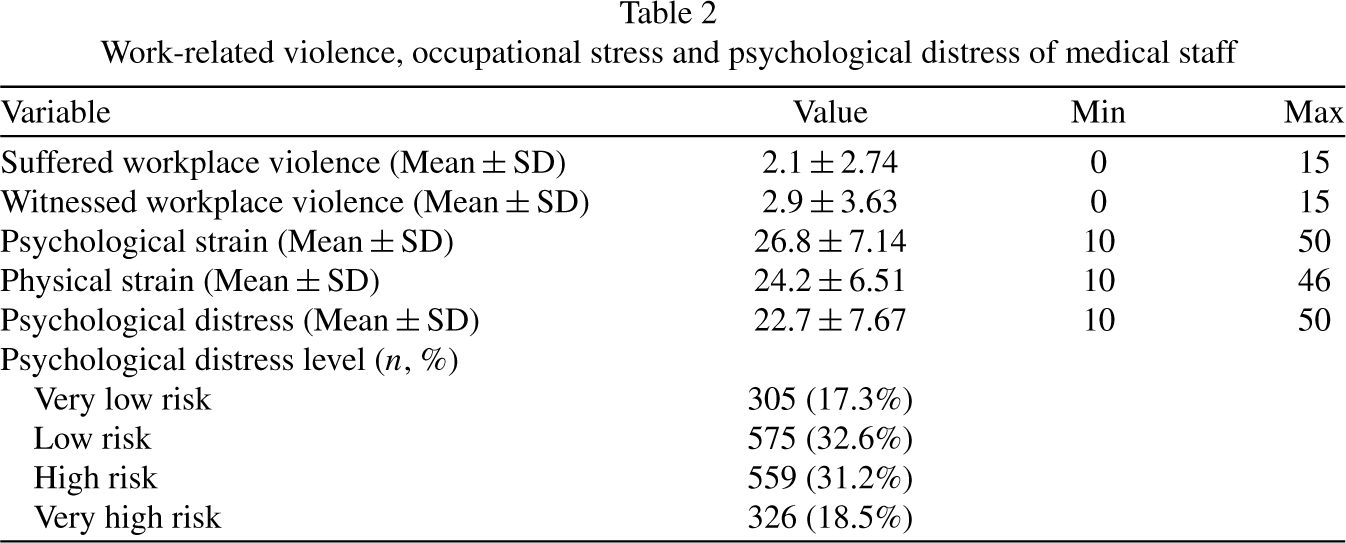
The suffered workplace violence score of medical staff was 2.1±2.74, and the witnessed workplace violence score was 2.9±3.63. The psychological strain score and physical strain score were 26.8±7.14 and 24.2±6.51, respectively. The psychological distress score of the medical staff was 22.7±7.67. A total of 49.7% of the medical staff were classified as having a high risk or very high risk of psychological distress. The characteristics of work-related violence, occupational stress and psychological distress are shown in Table 2.
Work-related violence, occupational stress and psychological distress of medical staff
Work-related violence, occupational stress and psychological distress of medical staff
The correlation analysis showed that there were statistically significant correlations between work-related violence, occupational stress, social support and psychological distress. The correlation coefficients between work-related violence and psychological distress were 0.303 (suffered workplace violence) and 0.287 (witnessed workplace violence), respectively. The full correlation analysis results are shown in Table S3.
Multivariate linear regression of psychological distress
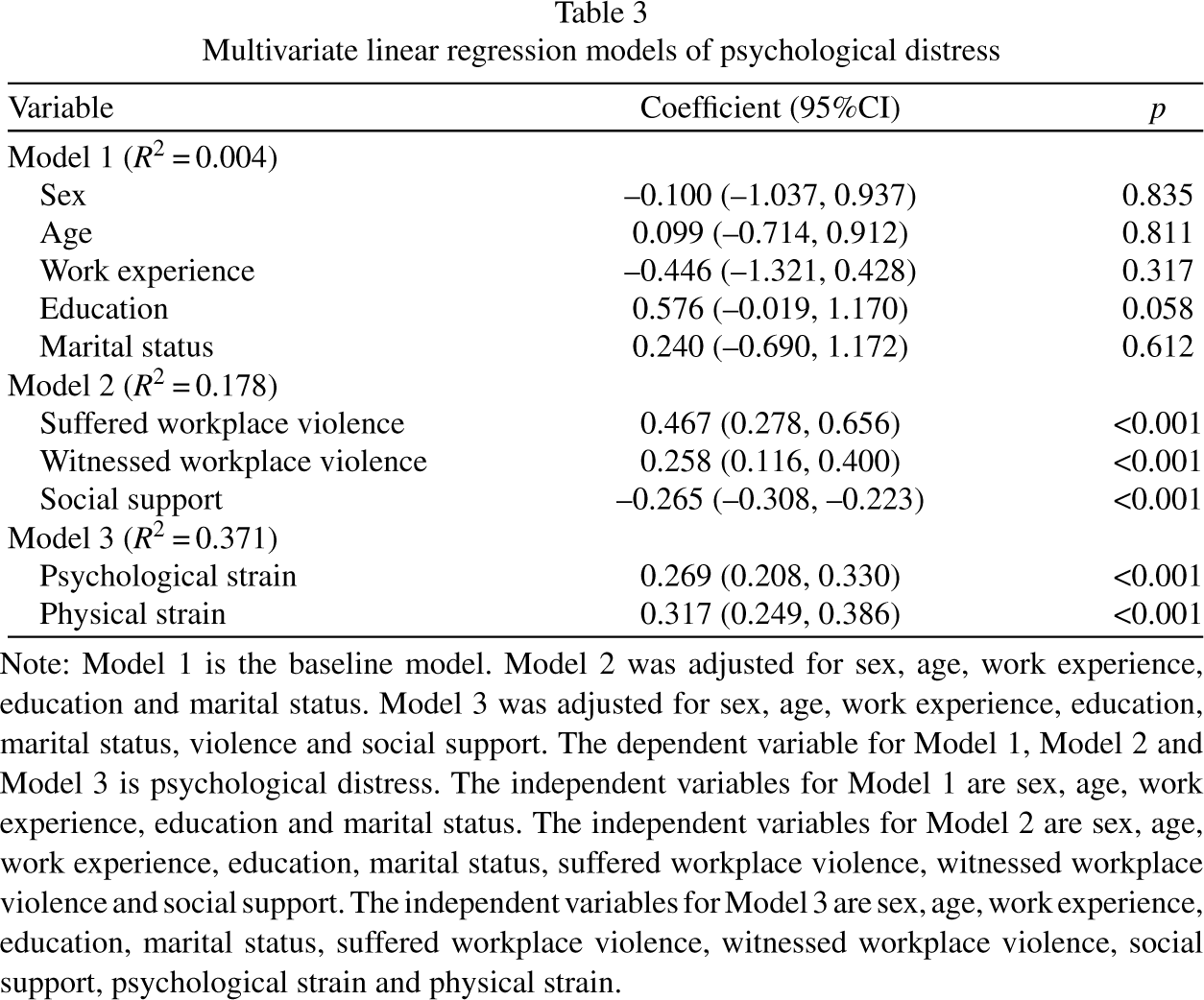
The results of the multivariate linear regression analysis are shown in Table 3. Sex, age, work experience, education, and marital status were not statistically significant in the baseline model (Model 1, R2 = 0.004). Work-related violence and social support were statistically significant in Model 2 (Model 2, R2 = 0.178) after adjusting for demographic characteristic variables. Both psychological strain and physical strain were statistically significant in Model 3 (Model 3, R2 = 0.371) after adjusting for all the variables in Model 1 and Model 2.
Multivariate linear regression models of psychological distress
Multivariate linear regression models of psychological distress
Note: Model 1 is the baseline model. Model 2 was adjusted for sex, age, work experience, education and marital status. Model 3 was adjusted for sex, age, work experience, education, marital status, violence and social support. The dependent variable for Model 1, Model 2 and Model 3 is psychological distress. The independent variables for Model 1 are sex, age, work experience, education and marital status. The independent variables for Model 2 are sex, age, work experience, education, marital status, suffered workplace violence, witnessed workplace violence and social support. The independent variables for Model 3 are sex, age, work experience, education, marital status, suffered workplace violence, witnessed workplace violence, social support, psychological strain and physical strain.
SEM was used to analyze the potential pathways and specific effect sizes of violence, stress and social support on psychological distress. The final fitting model met the criteria after repeated fittings and corrections (χ2/df = 0.894, RMSEA <0.001, GFI = 0.999, NFI = 0.999, RFI = 0.998, CFI = 1.000, and IFI = 0.999). The final fitting model is shown in Fig. 1.
The results (Table 4 and Table S4) showed that suffered workplace violence and social support had both direct and indirect effects on psychological distress, and the intermediate factor was occupational stress. Witnessed workplace violence only had indirect effects on psychological distress. The total effects of suffered workplace violence and witnessed workplace violence were 0.181 (direct effects and indirect effects) and 0.092 (only indirect effects), respectively, and the total effect of social support was –0.262 (direct effects and indirect effects).
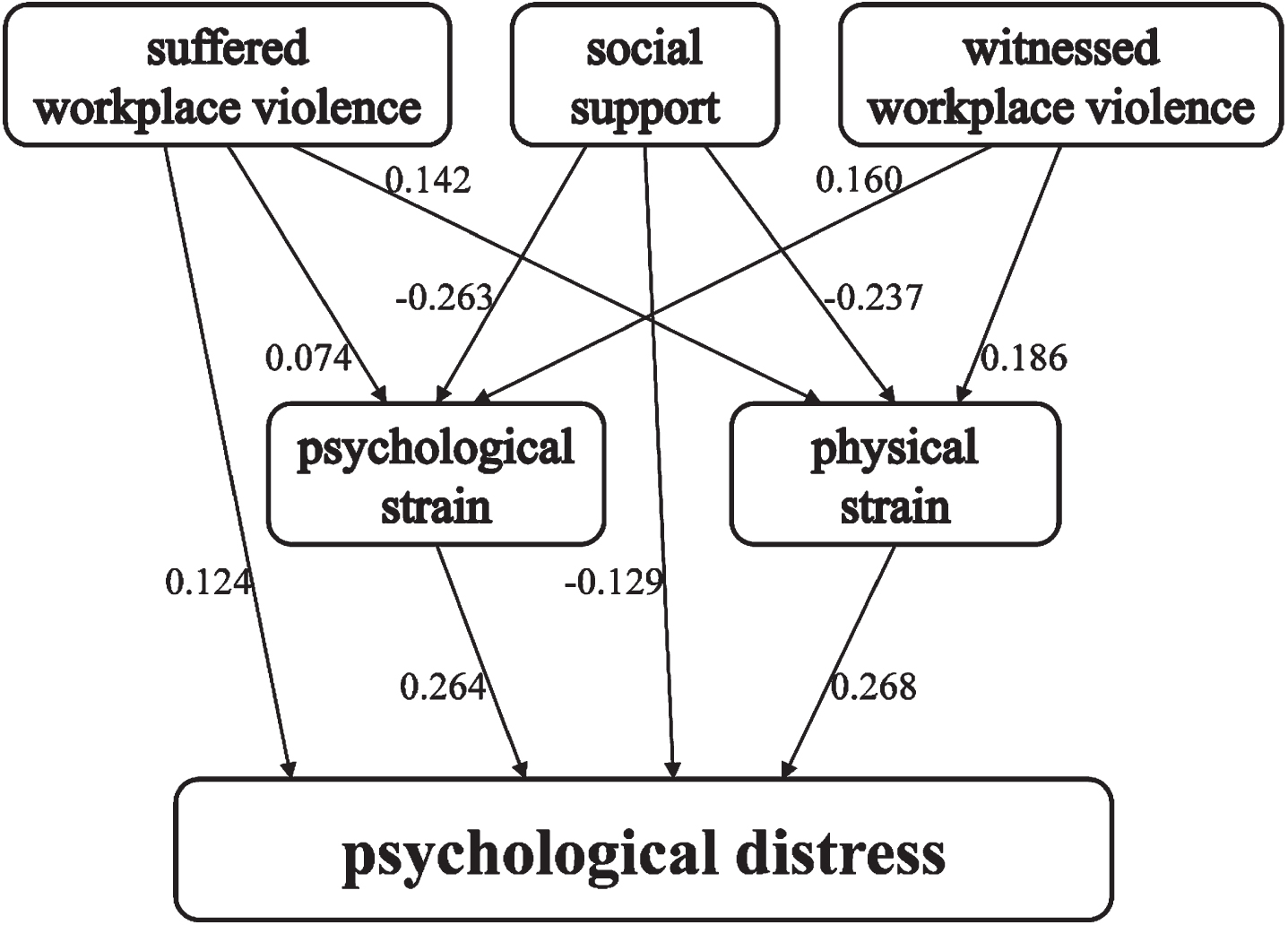
Structural equation model of violence, occupational stress and psychological distress. Note: Work-related violence and social support had both direct and indirect effects on psychological distress, and the intermediate factor was occupational stress (psychological strain and physical strain). Suffered workplace violence had both direct and indirect negative effects on psychological distress, while witnessed workplace violence only had indirect effects on psychological distress. Social support had both direct and indirect protective effects by relieving occupational stress on psychological distress.
Direct and indirect effects of work-related violence on psychological distress

This study revealed the potential links and pathways of work-related violence, social support, occupational stress, and psychological distress. Work-related violence was related to psychological distress through occupational stress among medical staff. Occupational stress was the intermediate factor, and social support played a negative regulatory role in the model. It should be noted that although both those who suffered workplace violence and those who witnessed workplace violence entered the final model, they worked differently. Suffered workplace violence had both direct and indirect associations with psychological distress, but witnessed workplace violence only had indirect associations. Witnessed workplace violence was not directly associated with psychological distress but increased risk through psychological strain and physical strain.
Our research showed that suffering workplace violence was positively correlated with occupational stress. Itzhaki et al. reported a similar correlation between physical and verbal violence and occupational stress in nurses [31]. Another survey conducted in Germany also showed that nearly one-third of employees felt high levels of stress as a result of workplace violence [32]. In fact, work-related violence was identified as a key risk factor and predictor of stress and possible mental disorders in medical staff working in high-risk environments [9]. However, none of the above studies reported the relationship between witnessed workplace violence and occupational stress. In addition to suffered violence, our study also found that witnessed violence in the workplace was statistically correlated with psychological strain and physical strain; that is, suffered and witnessed violence were both powerful external stressors.
Our research showed that both suffered and witnessed workplace violence were both positively associated with the psychological distress of medical staff. It has been reported that there are significant differences in the rates of psychological problems and anxiety among medical staff who experience workplace violence [33]. A survey among medical staff revealed that 71.3% of the participants who suffered work-related violence reported depressive symptoms [34]. Another study also found that compared with the control group, medical staff who experienced violence were more likely to experience symptoms of depression and anxiety [35]. According to a survey conducted in Pakistan, 1 in 6 doctors who experienced verbal abuse were positive for PTSD, and 2 in 5 doctors were screened for anxiety and depression; PTSD and psychological problems are significant comorbidities [36]. Compared with those that have suffered workplace violence, few studies have focused on the impact of witnessed violence on the psychological distress of medical staff. According to a series of relevant studies on witnessed domestic violence and community violence and its subsequent behavior and health effects in adolescents, witnessed workplace violence may also have long-term effects that cannot be ignored [37–39]. In this study, witnessed violence also positively predicted the level of psychological distress.
In addition, the results of this study also showed that violence was related to psychological distress through direct and indirect paths among medical staff, in which stress was an intermediate factor and social support played a negative regulatory role. However, the comorbidity of occupational stress and mental disorders has been reported in many studies. For example, Lee et al. [40] revealed that abuse, threat, or humiliation were linked to greater stress and poorer mental health in nurses at the same time. Whether there is a mediating effect is worth noting. Kobayashi et al. [41] suggested that work-related violence may be a persistent and/or cumulative source of stress, rather than a short-term experience, and may cause potential changes at the psychological level. It has been reported that occupational stress moderates the relationship between work-related violence and self-reported health status [21]. Furthermore, social support moderates turnover intention and mental health problems caused by work-related violence [42]. Family support and psychological capital also playe an intermediary role between violence and depressive symptoms among medical staff after suffering violence [25, 43]. In contrast, Shahrour et al. [44] suggested that violence and social support predict stress in psychiatric nurses, but social support is not an intermediate factor. However, few studies have reported the intermediating factors or mediating effects between witnessed violence and psychological distress. According to our study, witnessed violence had only indirect effects on psychological distress, in which both psychological strain and physical strain were the intermediate factors and social support was the moderating factor.
Limitations of the study: 1) The research data came from a cross-sectional survey, which may have uncertain information bias. In addition, the conclusion lacked further support from longitudinal data also prevents the exclusion of reverse causality. 2) The outcome of this research was measured using the self-reported 10-item Kessler scale rather than specific clinical diagnostic guidelines. However, clinical diagnostic such as depression or autism as the outcome variable may provide more convincing evidence. 3) Due to the difficulty of implementation, this study adopted convenient sampling strategy, which may lead to selection bias. Participants included in this study may not fully represent the total population studied.
Conclusion
This study revealed that work-related violence is associated with psychological distress, while occupational stress is the mediating role. There were differences in the pathway and effect characteristics between suffered workplace violence and witnessed workplace violence among medical staff. The results suggest that it is urgent and necessary to intervene in work-related violence in healthcare facilities. It should be noted that when formulating intervention measures, the differences between suffered workplace violence and witnessed workplace violence should also be taken into account.
Data availability
The data are not available for the privacy of the participants and the corresponding author can be contacted upon reasonable request.
Ethical approval
This study was approved by the Ethics Committee of the West China School of Public Health, Sichuan University (No. Gwll2021070).
Informed consent
All participants gave informed written consent to participate voluntarily in the survey.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
This study was supported by the Sichuan Science and Technology Program (No. 2022YFS0422 & No. 2023NSFSC1736).
Supplementary Material
Footnotes
Acknowledgments
The authors would like to thank all the participants in this study and all those who provided help with this study.
Table S1. Sampling strategy of the cross-sectional survey. Table S2. The questionnaire of workplace-related violence survey. Table S3. Correlation between violence, occupational stress and psychological distress. Table S4. Structural equation model of psychological distress.