
Abstract
Double aortic arch (DAA) is a rare congenital anomaly associated with the formation of a vascular ring. Patients with DAA commonly suffer from complications caused by intracardiac and extracardiac malformations and different degrees of airway stenosis. Multislice computed tomographic angiography (MSCTA) is an intuitive and effective medical imaging technique in clinical diagnosis of DAA. MSCTA can accurately manifest the aortic arch and the course of the descending aorta and airway stenosis in three-dimension (3D). It is important to diagnose and make an operative plan for DAA. In this paper, we present a case of DAA diagnosed by MSCTA with 3D-static images and rotated reconstruction images and performed a mini-review.
Introduction
Double aortic arch (DAA) is a type of vascular ring malformation, which occurs relatively rarely in children [1]. Its incidence is less than 1% of congenital heart diseases [2]. DAA has no known ethnic or geographic disposition. DAA’s mechanism is derived from a developmental anomaly of the original arterial arch in the embryonic period or chromosomal 22q11 microdeletion [3]. DAA is an anomaly of the aortic arch; two aortic arches form a complete vascular ring that can compress the trachea and/or esophagus [1, 4].
In accordance with its anatomic characteristics, DAA has been divided into three types [5]: large right posterior arch and small left anterior arch (right dominant aortic arch), accounting for 75%; small right rear arch and large left front arch (left dominant aortic arch), accounting for approximately 20%; and equal diameter DAA (balanced type aortic arch), accounting for 5% (Fig. 1).

Schematic diagram of the normal aortic arch and DAA: A. Normal aortic arch. B. Double aortic arch. The images show the relationship between the trachea and/or the esophagus with the aortic arch.
Treatment methods for DAA include surgical correction, conservative approach, and follow-up. Surgical correction is indicated in all patients with DAA with obstructive symptoms. A conservative approach can be reasonable when symptoms are absent. Presently, ultrasonic echocardiography (UCG), magnetic resonance imaging (MRI), digital subtraction angiography (DSA) and MSCTA are the four main clinical cardiac imaging technologies that can be applied to diagnose DAA (Table 1) [6, 7].
The advantage and disadvantage of four imaging technologies that can be applied to diagnose DAA
MSCTA can show more clearly the structure of the inner heart and the large blood vessel in the cardiovascular diseases; it is especially good in displaying the distal aortic arch, brachiocephalic artery along the approach branches, and the relationship of the arch to the trachea and bronchi [8, 9]. It not only defines the type of DAA accurately in most patients, but also clearly presents the specific location and compression condition of airway stenosis [9]. Both 3D-static images and rotated reconstruction images can be generated by CT. 3D-static images can provide detailed information of a certain site, while 3D-rotated images can be rotated from every direction and the changes in cardiovascular and pre/postoperative anatomy changes can be clearly observed [10].
In this study, we reported a case of an infant patient with DAA. 3D-rotated images and static images were generated by MSCTA to diagnose DAA. We also performed a mini-review.
A 3-month, 20-day-old female infant had been suffering from anterior fontanelle bulging for a week and eating less for 1 day; she was admitted to the Neurology Department of Children’s Hospital of Chongqing Medical University. During hospitalization, the patient’s face and lip appeared cyanotic and even appeared marble when the patient cried severely. Congenital heart disease was considered, and UCG suggested DAA, which was confirmed by MSCTA. There were surgical indications (compression of both the trachea and esophagus), and the patient was transferred to the Cardiothoracic Surgery department for an operation.
The tachypnea was mainly clinical presentation. She looked weak and pale. She was at a low weight (4 kg and 52 cm tall), with a birth weight of 3.25 kg . Her nutrition and reaction were poor, the skin was full of pigmentation, with narrow facial surface and bregmatic tonus 4 cm×4 cm in size, and had an unclosed sagittal suture. Sternum depression was observed. A few coarse rales were heard on the bilateral lung. There was no obvious systolic and diastolic murmur in heart auscultation. Laboratory examinations were unremarkable. Chest radiograph showed left lower pneumonia and an enlarged podoid. Electrocardiography indicated sinus tachycardia (Fig. 2). The patient then underwent UCG examination, which showed DAA with left aortic arch dysplasia, left patent ductus arteriosus, atrial septal defect, persistent left superior vena cava, and manipulus hydropericardium. The systolic and diastolic function of the left ventricle were normal. Laryngoscopic examination revealed mild dysplasia of the laryngeal cartilage. The compression sign of the right front esophageal was visible for X-ray barium meal examination. MSCTA (GE Medical System, light speed VCT, USA) confirmed the diagnosis of cardiovascular abnormalities, surrounding the trachea and esophagus with right arch dominance, and the diameter of the trachea was evidently small at the level of the ascending aortic arch (Fig. 3A). Patent ductus arteriosus was connected to the left aortic arch and the pulmonary artery.

Electrocardiography of pre- and postsurgery: A. The graph shows sinus tachycardia, B. The graph shows sinus rhythm.
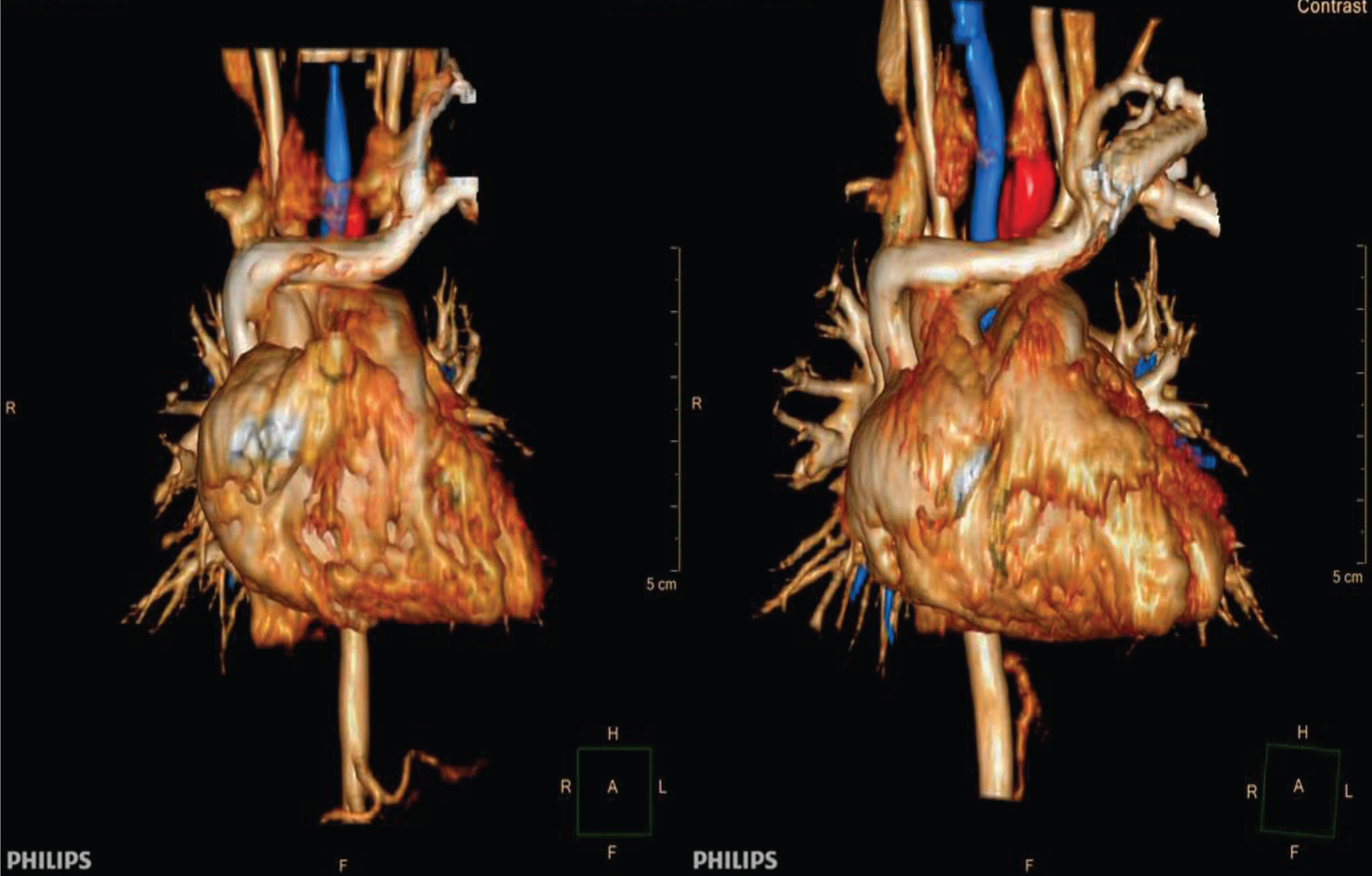
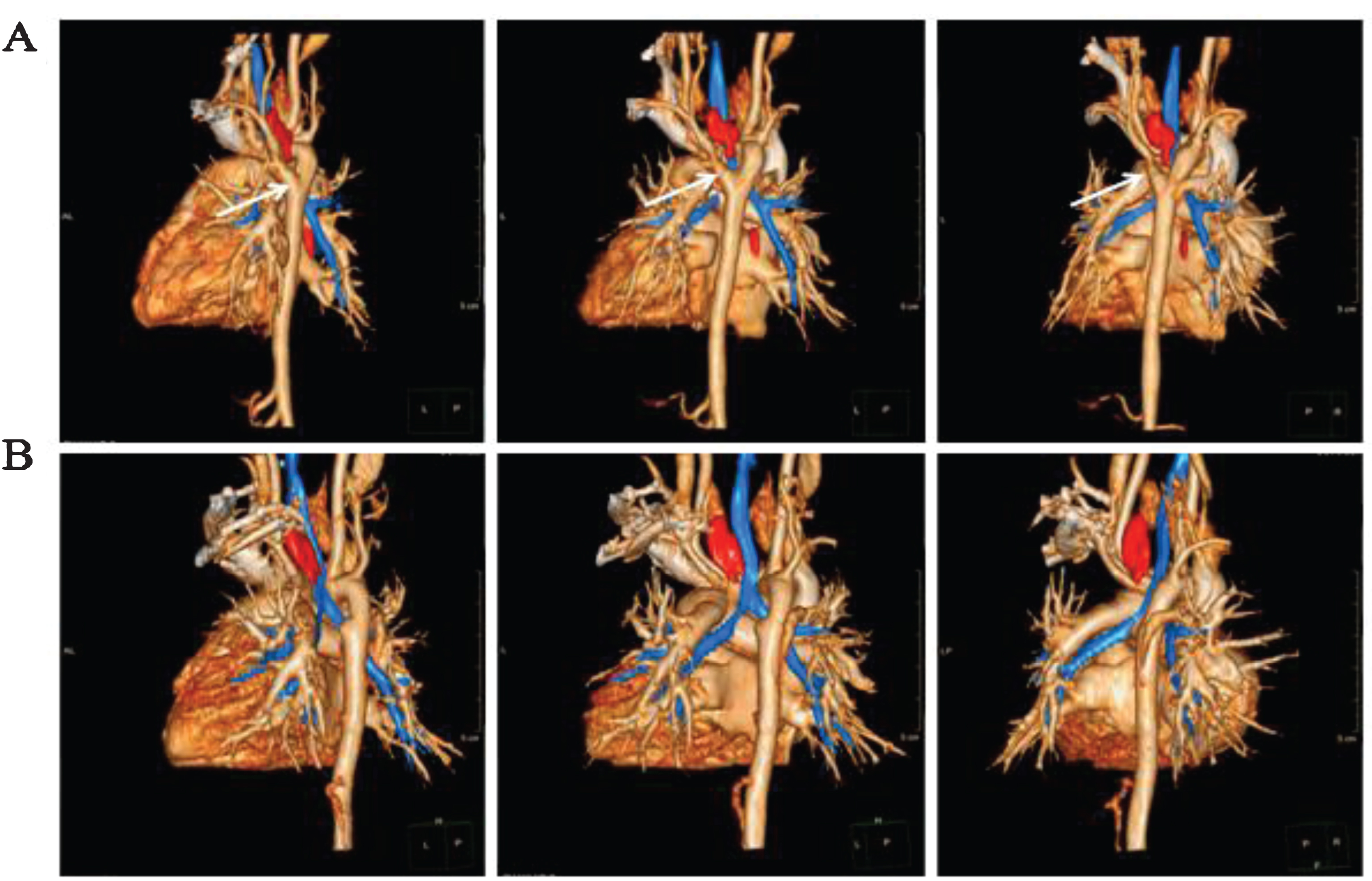
3D rotated images of pre- and postsurgery. A. 3D rotated images of presurgery; B. 3D rotated images of postsurgery.
When pulmonary inflammation was under controlled, she was underwent a correction operation of the DAA (left bow disconnection). It was approved to be DAA with surgery, which was left and right aortic arches formation vascular ring, and compression trachea and esophagus. Left aortic arch sent out two branches, left common carotid artery and left subclavian artery, and the patent ductus arteriosus was seen between the left aortic arch and the pulmonary artery. The cardiac surgeon separated the descending aorta, separated the double arch junction, performed ligation and cut off the distal end of the left bow, and performed blunt and sharp separation of the soft tissue of the trachea and esophagus.
Eight months after surgery, when the child was seen for follow-up examination with MSCTA, it showed the right-sided aortic arch with right-sided descending aorta, and the left side of the aortic arch and the original patent duct artery was absent for ligation into blind end without contrast medium filling, and the tracheal stenosis was significantly alleviated (Fig. 3B). Compared with her preoperative state, the patient ate a normal diet without difficultly in swallowing, her respiratory symptoms were relieved, and her respiratory rate was reduced from 50 to 32 beats per minute.
In addition, DAA formed the vascular ring to wrap around the esophagus and trachea, which could be observed on static images generated by MSCTA (Fig. 4). MACTA clearly showed more detailed information including the relationship of the arches to the trachea and bronchi. Thus, the degree of stenosis of the trachea and esophagus can be evaluated, and the diameter of the esophagus and trachea can be measured accurately by static images before and after operation.
Static images of pre- and post-surgery were generated by MSCTA: different angles of pre- and postsurgery.
Normally, in embryonic development, the fourth left arch develops into the aortic arch, the fourth right arch develops into the innominate artery, the left dorsal aorta develops into the descending thoracic aorta, and the dorsal intersegmental arteries bilaterally develop into the subclavian arteries [8]. DAA is formed when both fourth arches and both dorsal aortas remain present around the trachea and esophagus. The right aortic arch is always larger and located higher than the left aortic arch, which might be degraded or hypoplastic [1]. In this case, both aortic arches reunite to form the descending aorta located in front of the spine, with the right aorta being larger than the left aorta.
DAA could be caused by a chromosomal abnormality. Duna Trobo [11] reported only one case of DAA with the 22q11 deletion, and the patient had extracardiac anomalies. This low percentage of chromosomal abnormalities might be due to the small number of cases or scarcity of reported data, although most of the cases with congenital heart diseases did not report any abnormal karyotyping [12].
DAA has a wide clinical manifestation; therefore, diagnosis of DAA is very difficult. The most common presenting symptoms, especially in the pediatric patients, are respiratory (stridor) and gastrointestinal (dysphagia) [13]. It is always complicated with severe respiratory distress in infants. In the present case, the girl lacked respiratory symptoms. When respiratory symptoms are minimal, DAA still cannot be diagnosed until adulthood [14]. Thus, a DAA diagnosis is not definite or easily missed. Yoon [15] et al. reported that DAA with surgical repair has a relatively good prognosis, and the operative risk in the absence of a complex heart disease is low, early diagnosis and timely surgery in symptomatic patients are paramount, while patients with mild symptoms can be managed medically with close follow-up.
An accurate and clear cardiac image is essential to diagnose DAA. However, generating a heart image is challenging because of its voluntarily rapid motion, and both temporal and spatial resolutions are key factors for the image results. High spatial resolution can generate clear and detailed images, while high temporal resolution is greatly expected to reduce the motion artifact.
MSCTA is noninvasive angiography that is in rapid development; it has a short scanning time, rapid imaging ability, high time and spatial resolution. With superior 3D CT-imaging software in the system, conducting angiography from any angle is possible. Three 3D-imaging software are commonly used in MSCTA [9]: multiplanar reconstruction (MPR), maximum intensity projection (MIP), and volume rendering (VR). MPR can obtain any-level 2-dimensional (2D) image of coronary, sagittal, shaft, and inclined surface. The image produced by MIP is intuitive and clear, with arbitrary angle rotation for the observation of vascular course and anatomic relationship. VR can display the relationship between blood vessels more clearly and accurately than MIP, retains the original 2D-image with all the information, can display spatial structure and density information, and can also be used to show the different pseudo-color variation and normal blood vessels and superimposed pictures together to provide the image with a real 3D quality. In recent years, MSCTA has become a preferred way to diagnose cardiac disease.
The advantage of MSCTA is that the pre- and post-operative images can be compared with the anatomic morphology of the vascular and the degree of the airway and esophagus compression (Fig. 5). MSCTA is an important modality used in diagnosing DAA. It accurately defines the type of anomaly and directly shows the relationship of the arch to the trachea and bronchi. The powerful postprocessing function of MSCTA allows observation of lesions from different angles.
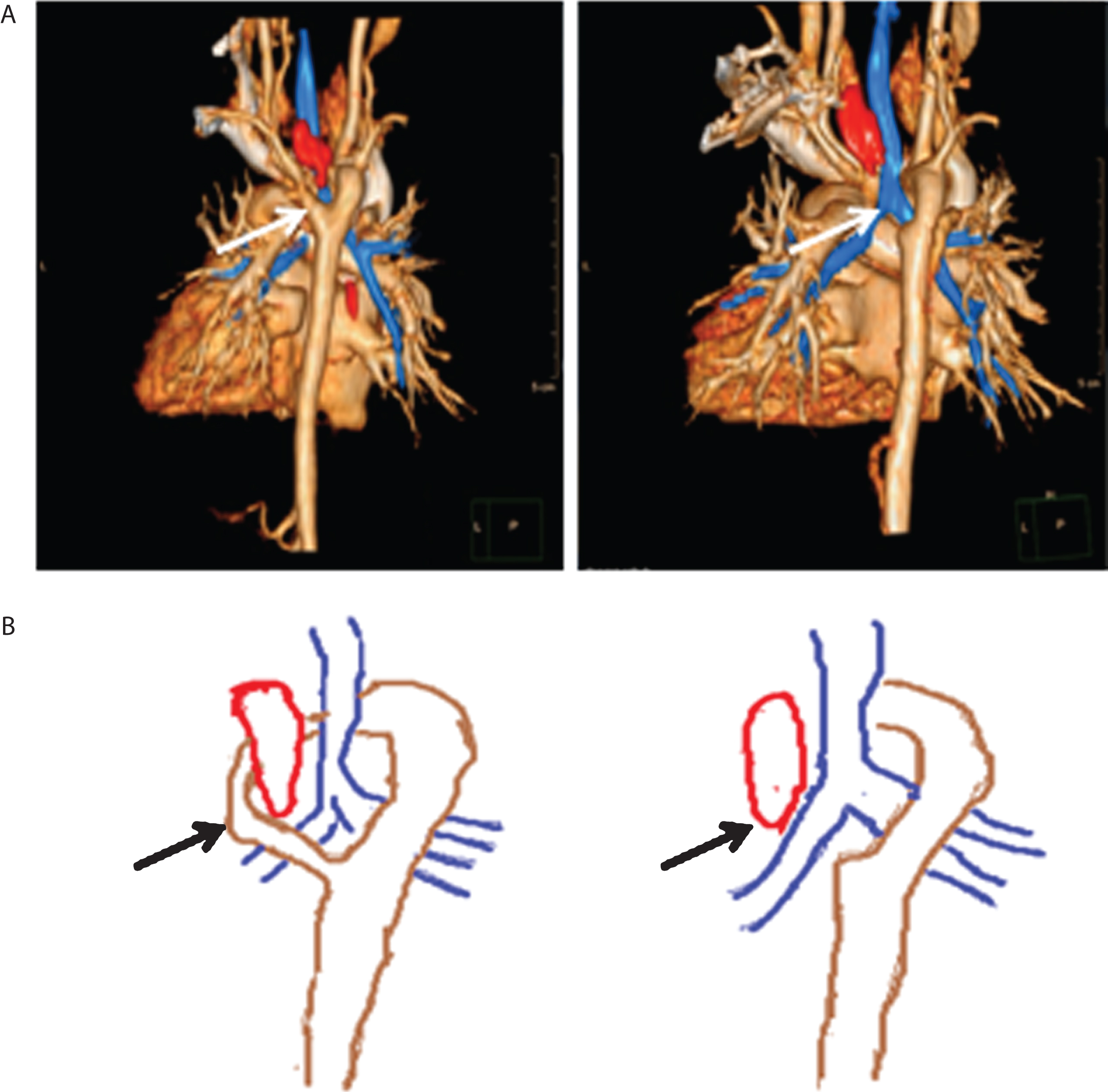
Static images and Schematic diagram of DAA after pre- and postsurgery: A shows static images generated by MSCTA, the white arrow displays the small right rear arch and large left front arch (left dominant aortic arch) on the left figure, while the right one presents that the small right rear arch was ablated. B shows Schematic diagram of the figure A (as shown by the black arrow).
Because of radiation, the application of MSCTA is limited and cannot be used in critically ill children. It is also expensive. Young children should be deeply sedated and even anesthetized, and clinical follow-up is not convenient. However, wearing lead eyeglasses, scarves, and aprons can minimize the exposure of patients without influencing the diagnosis.
Cardiovascular MSCTA can provide a definitive diagnosis of DAA, especially for the location of the aortic arch and assessment the degree of compression of the airways and the esophagus. This case illustrates the important role of MSCTA with invasive aortography in diagnosing a rare DAA anatomic variant [16].
This case report demonstrates the application value of MSCTA equipped with 3D-rotated images and static images in clinical practice. MSCTA is a reliable and feasible modality to diagnosis and follow-up patients with DAA because of its clear and intuitive 3D-imaging.
Footnotes
Acknowledgments
The work was supported by National Natural Science Foundation of China (Grant Nos 81301300); Chongqing Science and Technology Commission (cstc2016shmszx 130009).