
Abstract
PURPOSE:
Metal artifacts severely degrade CT image quality in clinical diagnosis, which are difficult to removed, especially for the beam hardening artifacts. The metal artifact reduction (MAR) based on prior images are the most frequently-used methods. However, there exists a lot misclassification in most prior images caused by absence of prior information such as the spectrum distribution of X-ray beam source, especially many or big metal included. The purpose of this work is to find a more accurate prior image to improve image quality.
METHODS:
The proposed method comprise of following four steps. First, the metal image is segmented by thresholding an initial image, where the metal traces are identified in the initial projection data using the forward projection of the metal image. Second, the accurate absorbent model of certain metal image is calculated according to the spectrum distribution of certain X-ray beam source and energy-dependent attenuation coefficients of metal. Then, a new metal image is reconstructed by the general analytical reconstruction algorithm such as filtered back projection (FPB). The prior image is obtained by segmenting the difference image between the initial image and the new metal image into air, tissue and bone. Finally, the initial projection data are normalized by dividing the projection data of prior image pixel to pixel, the corrected image is obtained by interpolation, denormalization and reconstruction.
RESULTS:
Some clinical images with dental fillings and knee prostheses are used to evaluate the proposed algorithm and normalized metal artifact reduction (NMAR) and linear interpolation (LI) method. The results demonstrate the artifacts can be reduced efficiently by the proposed method.
CONCLUSIONS:
The proposed method could obtain an exact prior image using the prior information about X-ray beam source and energy-dependent attenuation coefficients of metal. As a result, the better performance of reducing beam hardening artifacts can be improved, even though there were many or big implants. Moreover, the process of the proposed method is rather simple and little extra calculation burden is necessary. It has superiorities over other algorithms when include big or many implants.
Introduction
Metal artifacts, which caused by metallic implants such as surgical clips, dental fillings, heart pavement and knee prosthesis, generally appears as streaking artifacts as well as bright and dark band in reconstructed image of X-ray CT. The artifacts are mainly due to beam hardening, photonstarvation, partial volume effect and scatter [1], where beam hardening is one of primary reasons degrading image quality. It appears as beam hardening artifacts. The suppression of beam hardening artifacts is very important however rather difficult, and still a major challenge for improving CT imagingperformance.
In the past several decades, several approaches for MAR have been proposed. The approaches can be classified as sinogram inpainting methods [2–8], iterative methods [9–11] and dual energy correction methods [12, 13]. The clinical applications of iterative methods and dual energy correction methods are still limited in spite of some good preliminary results are obtained. The iterative methods need heavily calculation burden while the dual energy correction methods mean additional dose. The sinogram inpainting scheme is one of the most common technique in MAR approaches for its simple implementation. In the methods, the projection data that corrupted by metal are neglected and replaced by the interpolation data. LI, which has been proposed by Kalender et al. [2], is the simplest sinogram inpainting method. It can effectively reduce metal artifacts, however, it may lose the edge information in the metal trace and bring in secondary artifacts. In order to overcome these drawbacks, some methods based on prior image has been proposed to reduce metal artifacts while preserve the edge information in the prior image. The difference among the MAR approaches for computing prior images is mainly on how to calculate prior image. Müller et al. [14] create prior image by separating air and tissue, then normalize the original sinogram data. The corrected image is obtained by interpolating and then denormalizing. Esther Meyer et al. [15] segment the original image smoothed by Gaussian as air, soft tissue and bone. The method can effectively preserve the edge information surrounding the metallic objects. Zhang et al. [16] calculate the image mutual correlation among the original reconstructed image, LI image and their difference image to build a combined prior image, which contains fewer artifacts. Then apply the LI again to obtain the corrected image. These prior-based MAR methods build prior image by segmenting the original reconstructed images or simple pre-corrected images using k-means clustering or multithresholding. These approaches may lead to severe misclassification, which can result in residual artifacts and some tissue structures lost. The more there exist multiple metallic implants, the more severe misclassification becomes.
In order to overcome the misclassification, the prior image is built based on an accurate absorbent model in this work. First, the energy spectrum of X-ray source and absorption coefficient of certain metal are utilized to construct an absorbent model, thus to construct a prior image, which can match true beam hardening artifact image better. Then the beam hardening artifact image can be removed as more as possible from the original image. Finally, recover the image by interpolation and denormalization.
Methods
Prior image plays a crucial role in the performance of the prior-based MAR methods. In this work, a new approach is proposed to build a more exact prior image. The proposed method can be summarized by the flowchart in Fig. 1. The details of each step are described in the following subsections.
Segmentation of metals and identification of metal trace

The flowchart of the proposed method.
The metal objects are segmented by thresholding, and the fixed threshold value is employed. Where 3000 Hounsfield units (HU) is chosen as the threshold, which is proper to extract metal according to the literature [17–19]. Then the metal objects image is projected. The value above zero in the metal sinogram is viewed as metal trace.
In order to obtain a more accurate prior image, we stimulate the beam hardening artifacts, which is based on the mechanism of beam hardening described in the following, and subtract these artifacts from the original image before calculate prior image.
Beam hardening is caused by the polychromatic X-ray beam spectrum and energy dependent
attenuation coefficients. When a monoenergetic X-rays
IO,E with energy
E pass through the material, the transmitted X-ray intensity
IE,mono can be written in
the following form according to the Lambert-Beer’s law:
where μE,S is the linear
attenuation coefficient of the object at the same energy E. In fact, the
X-ray beam produced by an X-ray tube covers a board spectrum (see Fig. 2. https://www.oem-xray-components.siemens.com/x-ray-spectra-simulation). So
that the relationship between incident and transmitted X-ray intensity is expressed as:
where η (E) presents the normalized energy spectrum of X-ray beams [20]. The polychromatic projection value p poly can be obtained after a logarithm operation:
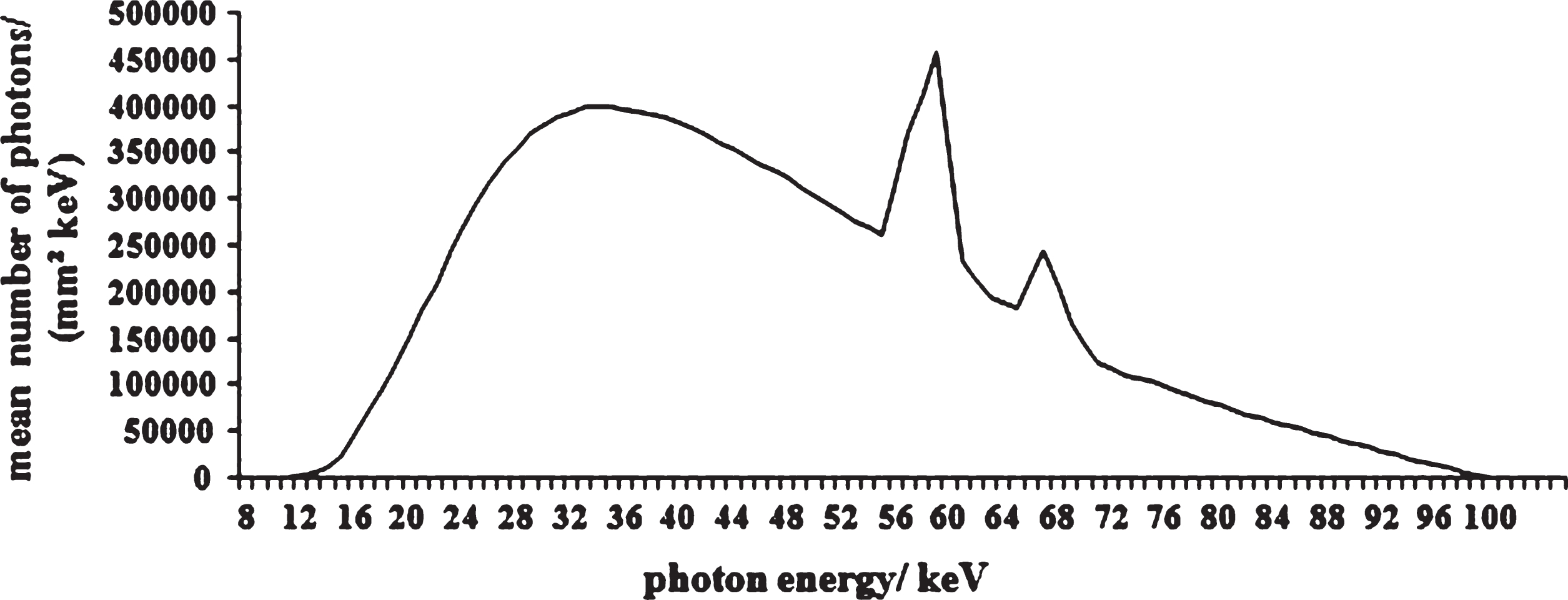
Example of an x-ray tube output energy spectrum.
Figure 3(b) shows a stimulated beam hardening image according to the X-ray mass attenuation coefficients [21] and the distribution of the energy spectrum of X-ray tube. The stimulated tube voltage is 100 kV (it contains 9–100 energy levels), the metal is regard as plumbum (11.3437gram/cm3). From the images, it can be seen that the stimulated beam hardening image matches the artifacts in the original image very well.
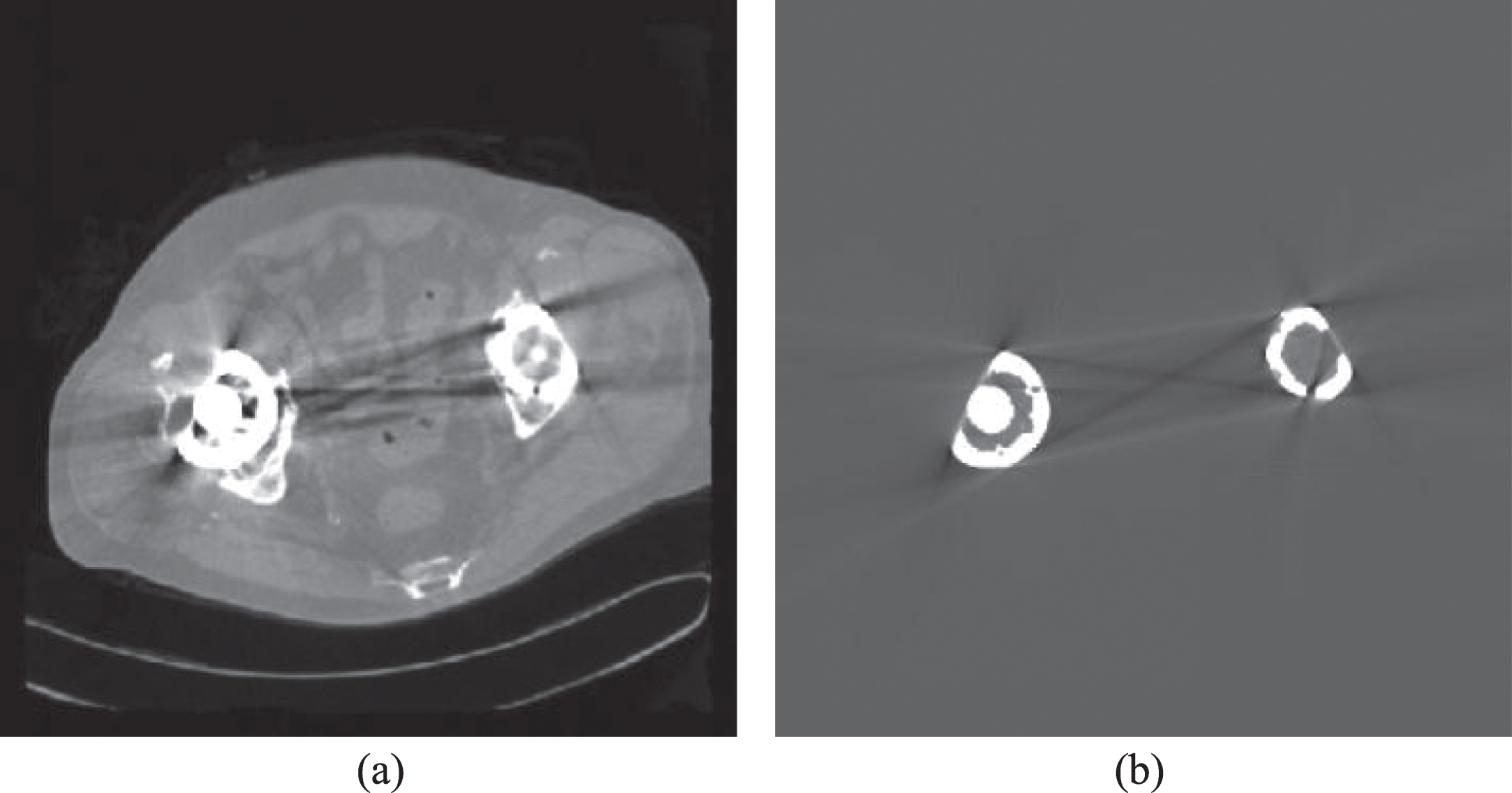
Original image and the stimulated beam hardening image. (a) the original image, (b) the stimulated beam hardening artifacts.
After the stimulation of beam hardening artifacts image, a beam hardening artifacts-removed image is constructed by subtracting the beam hardening artifact image from the original image. Then the prior image is calculated by segmenting the combined image into air, tissue and bone region. In this way, a prior image that matches the real tissue structure better can be produced.
Sinogram completion
Firstly, the prior image is projected to produce a prior sinogram. Then the original sinogram is normalized by dividing the prior sinogram according to literature [8, 14, 15]. In this step, the information of the edge can be remained in the prior projection data. Thirdly, LI of metal trace is applied on the normalized sinogram. Subsequently, the corrected sinogram is obtained by denormalized the interpolated normalized sonogram. So that the structure information preserved in the prior image can be brought back to the corrected image. In addition, the step ensures that there is no offset between original and corrected data. After reconstruction, the metal is inserted back into the corrected image.
Results
The proposed method is evaluated by several stimulated and clinical images. In the following cases, the images are reconstructed by FBP.
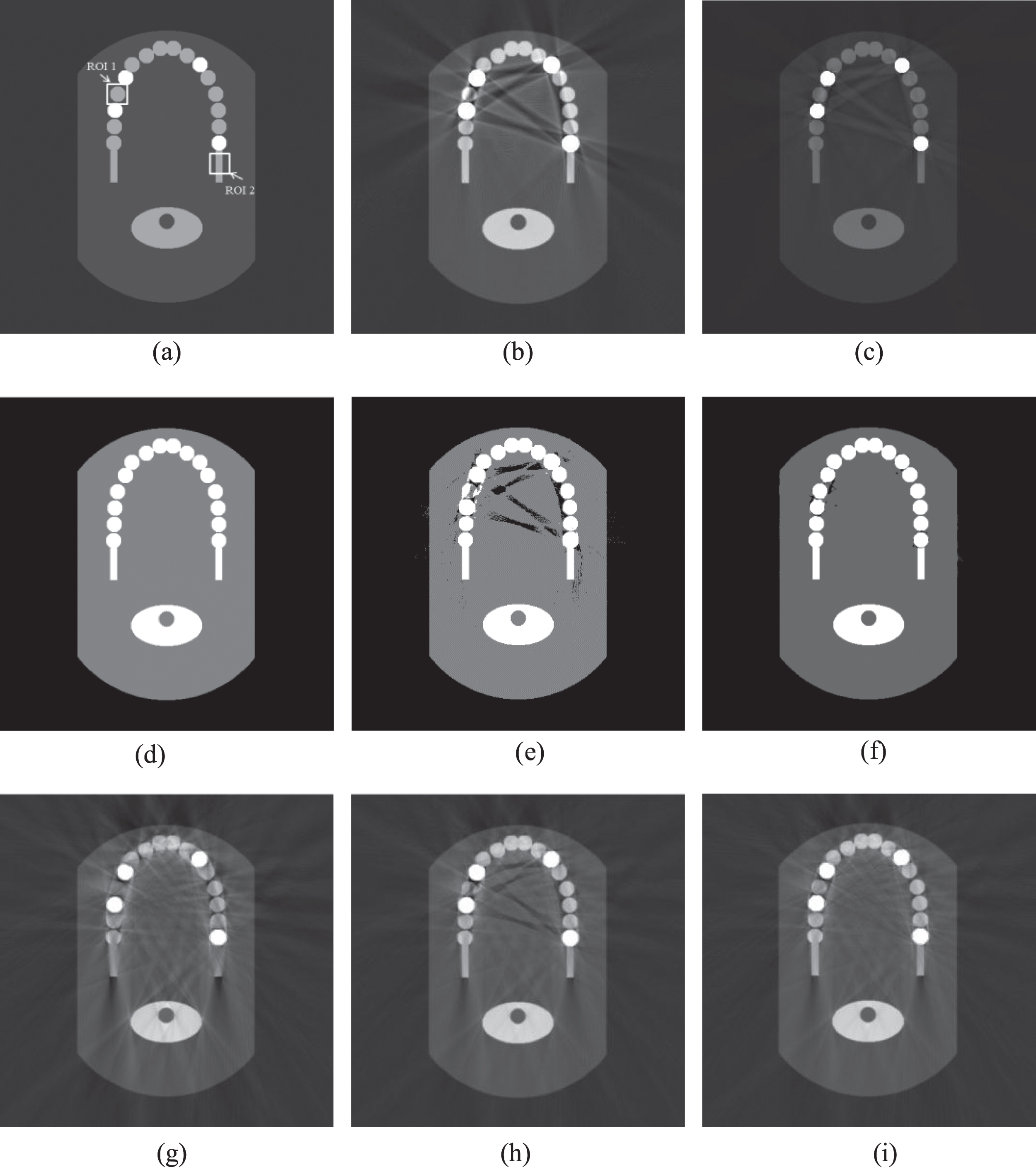
Stimulation images and prior images. (a) the original image, (b) the image reconstructed by FBP, (c) the beam hardening artifacts-removed image. (d) and (e) are the DPI, (f) the PPI. (g), (h) and (i) are the images reconstructed by LI, NMAR and the proposed method, respectively (WW/WL = 100HU/1500HU).
The normalized root mean square difference (NRMSD) is employed as criteria in accessing the
correction performance. The NRMSD in certain region between the reconstructed and reference
image (the original image) is computed according to the following formula,
where N is the pixel number in the region selected, x max and x min are the maximum and minimum intensities in the region of reference image, respectively; xr,i and xc,i are the intensities of the corresponding pixels in the reconstructed and reference images, respectively. The results of the global image and ROI1 are shown in Table 1.
The quantitative comparison of correction performance among FBP, LI, NMAR and the proposed method using NRMSD
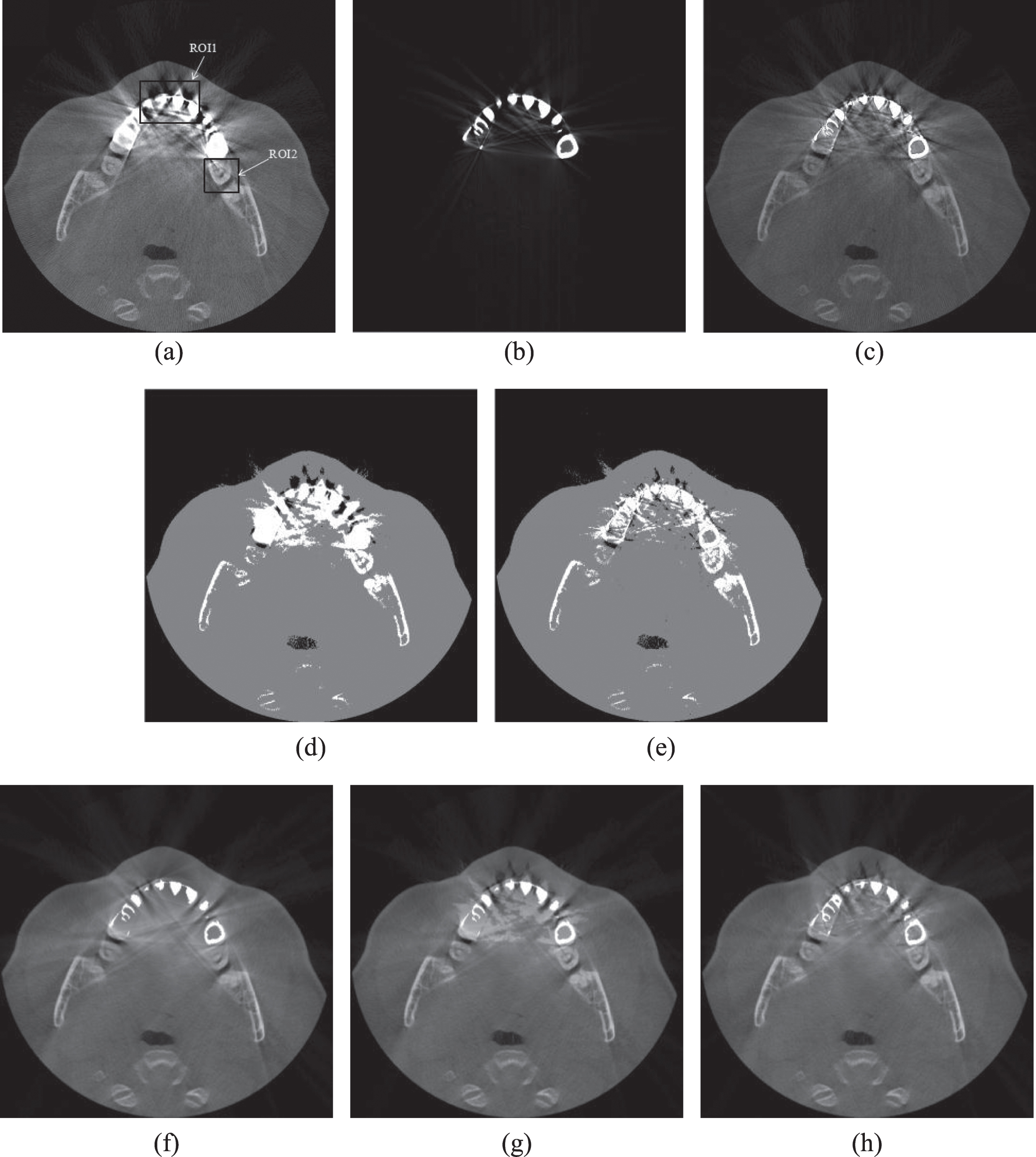
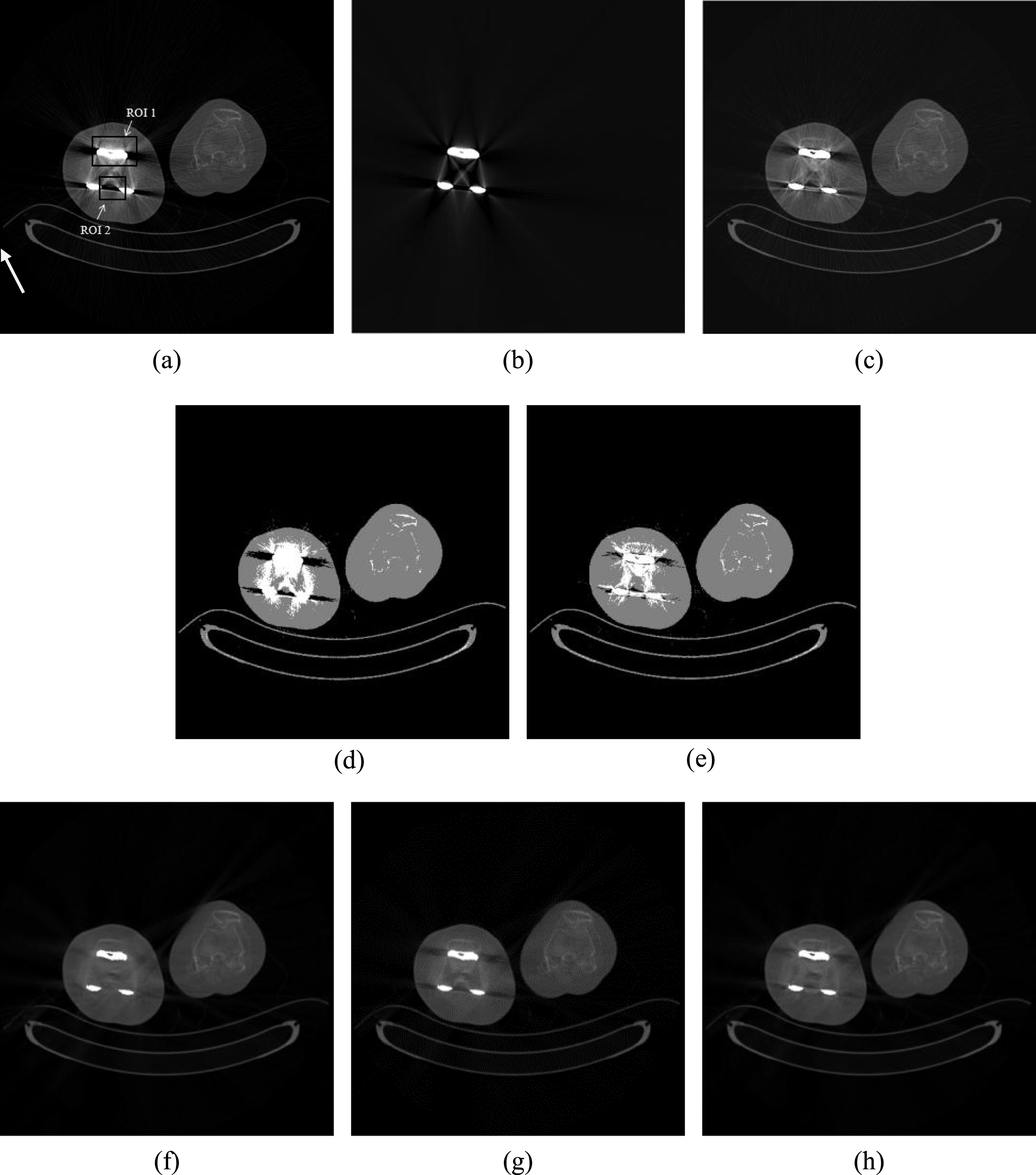
The reconstructed dental images using different approaches. (a) the original image, (b) the simulated beam hardening artifacts image. (c) the beam hardening artifacts-removed image. (d) and (e) are the DPI and PPI, respectively. (f), (g) and (h) are the corrected images using LI, NMAR and the proposed method, respectively (WW/WL = 1500HU/1500HU).
The knee prosthesis’s reconstructed images using different approaches. (a) the original image, (b) the stimulated beam hardening artifacts image. (c) the beam hardening artifacts-removed image. (d) and (e) are the DPI and PPI, respectively. (f), (g) and (h) are the corrected images using LI, NMAR and the proposed method, respectively (WW/WL = 2000HU/2200HU).
Real tissue structure information can be used to optimize MAR methods. The result of an improved prior image will result in an improvement of the whole prior-based MAR.
It has been shown that the quality of prior image is clearly improved by subtracting the stimulation beam hardening artifacts image from original image before calculating it. In Fig. 5, we can see that the PPI, compared with DPI, has less wrong tissue classification and better preserved tissue information which can significantly reduce residual artifacts. However, there are several limitations of the proposed method. First, the shape and size of implant metal gained by simple thresholding may be inaccurate, and this may introduce some secondary artifacts. Second, the values of the stimulated beam-hardening image are very small, so they are multiplied by a constant. The purpose of the stimulated beam-hardening image is to decrease the value of artifacts in the original image, so the existence of small errors is allowed. Finally, which is also a main limitation, due to the complicated reasons for metal artifacts, when there is extremely serious photon starvation, the result would be not satisfactory (see Fig. 6).
Conclusion
In this work, a novel method aimed to reduce beam hardening artifacts is proposed. In the proposed method, the stimulation and removal of beam hardening artifacts make sure the exactness of the prior image. The good prior image ensured the edge information in the corrected image. As the results of examples, the quality of images corrected by the proposed method is superior to that corrected by LI and NMAR, because the prior image calculated by the proposed method can decrease wrong tissue classification. However, for the complication of metal artifact, we cannot obtain a perfect prior image by the proposed method, so there are residual artifacts in the corrected image. Future work is needed to deal with the situation.
Footnotes
Acknowledgement
This work has been supported by National Natural Science Foundation of China (NSFC) under Grant No. 60972156, Beijing Natural Science Foundation under Grant No. 7142022 and Scientific Research Common Program of Beijing Municipal Commission of Education No. KM201410025011.