
Abstract
BACKGROUND:
Congenital hydronephrosis is often caused by aberrant renal vessel and it is difficult to be diagnosed and treated at the early stage due to lack of the significant symptoms. Although current medical diagnosis tools are widely used, the aberrant renal vessel cannot be displayed very well in the images.
OBJECTIVE:
To investigate whether applying computed tomography (CT) angiography with 3D reconstruction can improve efficacy in diagnose of this congenital hydronephrosis.
MATERIALS AND METHODS:
A male patient of 18 years old was diagnosed as hydronephrosis of left kidney. A CT angiography with 3D reconstruction was evaluated in diagnosis of the prenatal hydronephrosis compared to ultrasound (US) and intravenous urogram (IVU).
RESULTS:
US and IVU images were able to display the dilation of left pelvic and the dilated calyces, and the thinner of renal parenchyma on the left kidney (Grade II-IV), but failed to detect the causing of hydro-nephrosis. CT angiography with 3D reconstruction provided accurate images of the dilated renal pelvic, upper segment of the ureter, and an aberrant vessel bundle overcrossing at the left renal pelvic-ureter junction as well. The aberrant vessel could be revealed during surgery.
CONCLUSIONS:
A CT angiography with 3D reconstruction provides a more accurate diagnostic approach for the congenital hydronephrosis caused by aberrant renal vessel. Thus, it can offer surgeons very important information in the pre-surgery planning.
Introduction
Hydronephrosis is caused by internal and external conditions blocking normal drainage of urine from the kidney to the bladder, which leads to kidney swelling and even kidney failure. The aberrant renal vessel as an extrinsic cause of obstruction presents symptom-free but more insidious. These obstructions are usually detected incidentally during the routine clinical work-up of the primary disease process. In a general series of 3,172 autopsies of children, 2.5% were found to have urinary tract abnormalities, of which 35% were hydronephrosis or hydroureter [1]. Other than blood and urine tests, hydroneophrosis is usually diagnosed using is usually diagnosed using an ultrasound scan, intravenous urogram (IVU) or a computerized tomography (CT) scan, besides blood and urine tests.
A renal ultrasound sonogram is a primary option for the patients who have azotemia, contrast material–induced allergy, are pregnant, or are in the pediatric age group. The information of both the renal parenchyma and the collecting system can be obtained with no exposure to radiation and no contrast material–induced nephrotoxicity or anaphylaxis. However, the ultrasound sonogram cannot provide the information about renal function, whole collecting system, and exact causes of obstruction, particularly aberrant vessels outside of the ureter [2].
Within medical X-ray examinations, IVU is most commonly used for the detection of congenital defects, injury, tumors and inflammation in the urinary tract system for the patients with normal renal function. The IVU can provide both functional and anatomic details of the ureteral obstruction, displaying ureteral dilatation, tortuosity, and a standing column of contrast material in the ureter to the point of obstruction, parenchymal thinning, calyceal crescents, and a soapbubble nephrogram in the involved kidney. Although IVU provides the information on the kidney, it cannot show the obstruction caused by the vessel outside of the ureter [3]. In addition, In addition, IVU is not recommended for pregnant women or patients who are allergic to iodinated contrast material, shellfish, or asthma contrast material.
CT scans are a good alternative for patients who are allergic to contrast material or who suffer from renal function insufficiency. CT scans can also provide the information about the ureter obstruction, but it cannot exhibit the exactly image about relationship between the renal pelvi-ureteric junction (PUJ) and the aberrant vessels. As an advanced diagnostic technology, CT angiography with 3D reconstruction used special software to reconstruct 3D images of the vessels [4–9]. These models can be viewed from different angles to identify the PUJ and the aberrant vessels, also, its relationship to other anatomical structures. It provides more accurate images regarding the vascular anatomy of the kidney, which helps the pre-surgical planning and decreases complications after surgery [10]. Recently, a generalized spatio-temporal regularization technique for time-lapse tomographic reconstruction was developed in medical diagnosis [11]. In this study, we reported the diagnostic effect of CT angiography with 3D reconstruction in identification of hydronephrosis caused by the PUJ obstruction due to the adjacent abnormal vessels.
Patient information and materials
A young male at 18 years old occasionally felt dull pain in the upper left side of his abdomen for one years. The pain was unpredictable, lasted for a few hours, and then subsided spontaneously. Otherwise, the patient had no special complaints and nothing abnormal was found in his physical examination.
Laboratory test
A routine urine screening proved to be normal. Serum creatinine and blood urea nitrogen for renal function tests were within normal limits. Ultrasonography showed hydronephrosis with a severe dilation of collecting system on the left kidney.
Intravenous urogram (IVU)
IVU indicated a dilation of the left pelvic and a dilation of the entire calyces to three times than its normal size, and diminished parenchyma thickness (50%–75%) (Grade III-IV) and delayed image of the left ureter. Otherwise, no abnormality was detected in the right urinary tract system.
CT angiography with 3D reconstruction
A 64-slice CT and 3D-CT angiography clearly showed the anatomy of the kidney pelvic and its vasculatures. Gamma camera nephrography (5 m-Ci 99m-Tc MAG-3) with frusemide (20 mg i.v.) and fluid overload (NaCl 0.9% 2,000 ml) showed a dilated non-obstructed washout pattern with normal split renal function on the left side.

Plain CT scan indicated a dilated left pelvic (Grade III-IV) and an aberrant vessel to the inferior pole of left kidney. The arterial phase of contrast-enhanced CT scan demonstrates the signs of left hydronephrosis and stricture of ureteropelvic junction, also, two renal arteries originating from the aorta. An inferior aberrant artery (as the white arrow indicated) is crossing over the ureteropelvic junction.
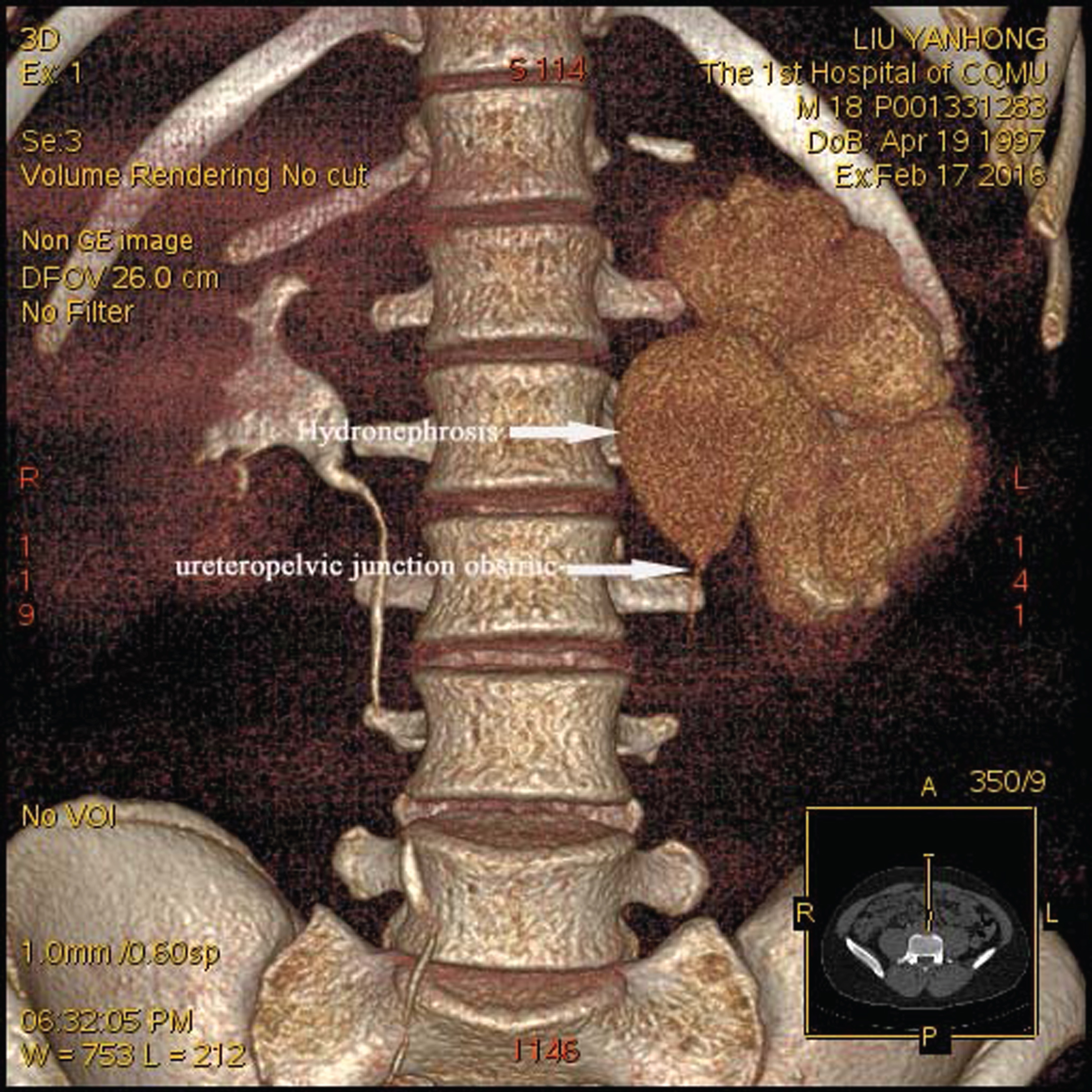
Extrinsic blacking (arrow) at the left ureteropelvic junction with severe hydronephrosis. Left ureter were significantly distended and narrowed down at the inferior renal pole at the third lumbar level with faint images (as the white arrow indicated).
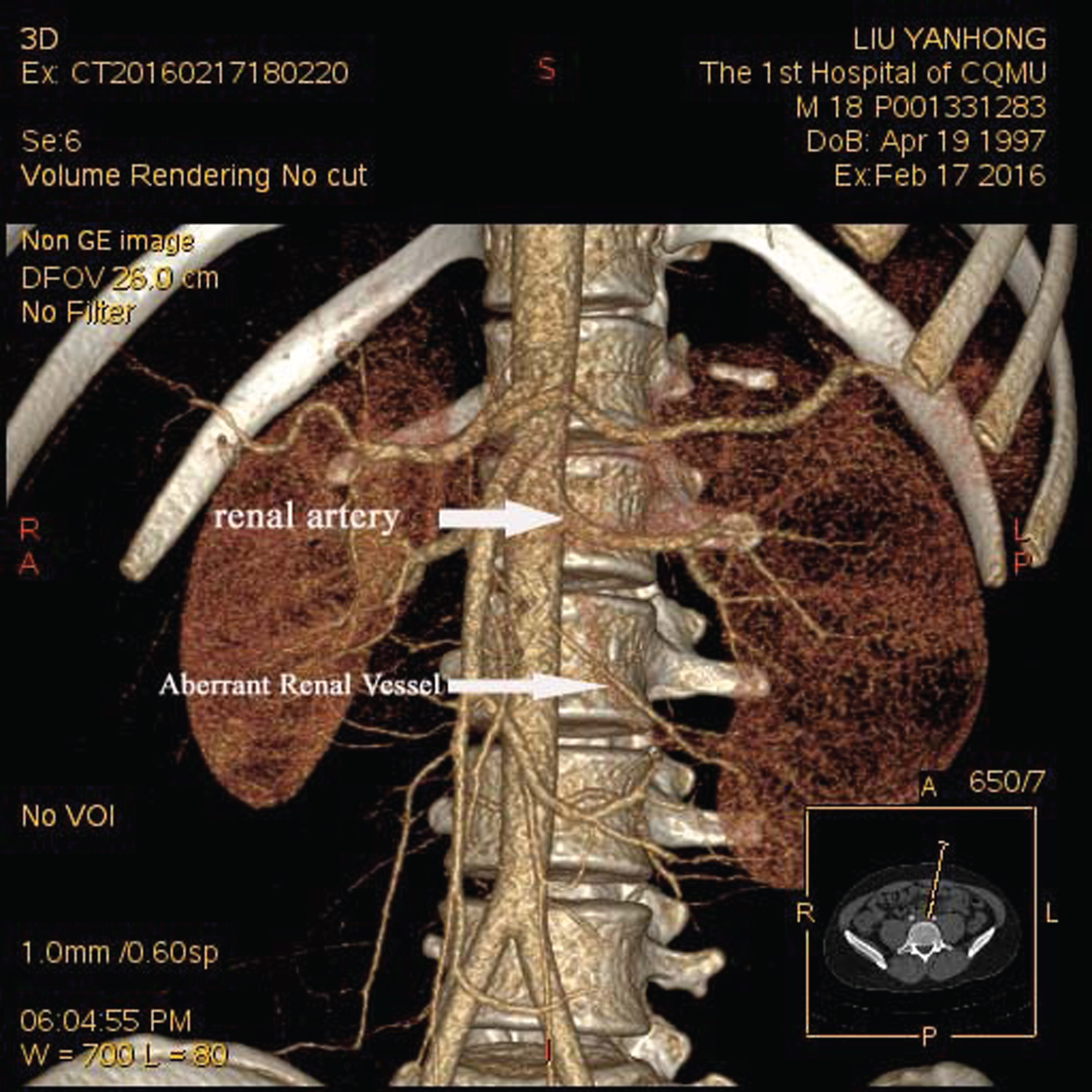
The 3D CT artery phase displayed the kidney artery, the branches and aberrant artery route. The left aberrant artery was directly derived from the abdominal aorta and descended alone the left kidney (a short and thick arrow) at the third lumbar level (a long and thin arrow).
The CT arterial phase showed clearly the relationship of the dilated pelvic and artery. While, 3D CT arterial phase indicated the whole kidney with dilated pelvic and the artery supplying the kidney. 3D CT arterial phase can be viewed from different angles to identify the dilated pelvic and the aberrant vessels, also, its relationship to other anatomical structures.
The aberrant vascular on the left kidney as shown by CT angiography with 3D reconstruction (Fig. 4) was confirmed during surgery. The patient underwent Anderson-Hynes surgery (Fig. 5), which was to obliquely dismember the renal pelvis and the aberrant vessels in the posterior of pelvis and ureter.

The aberrant renal vessel cross the upper segment of the left ureter was observed during the operation, leading the hydronephrosis of the left kidney.
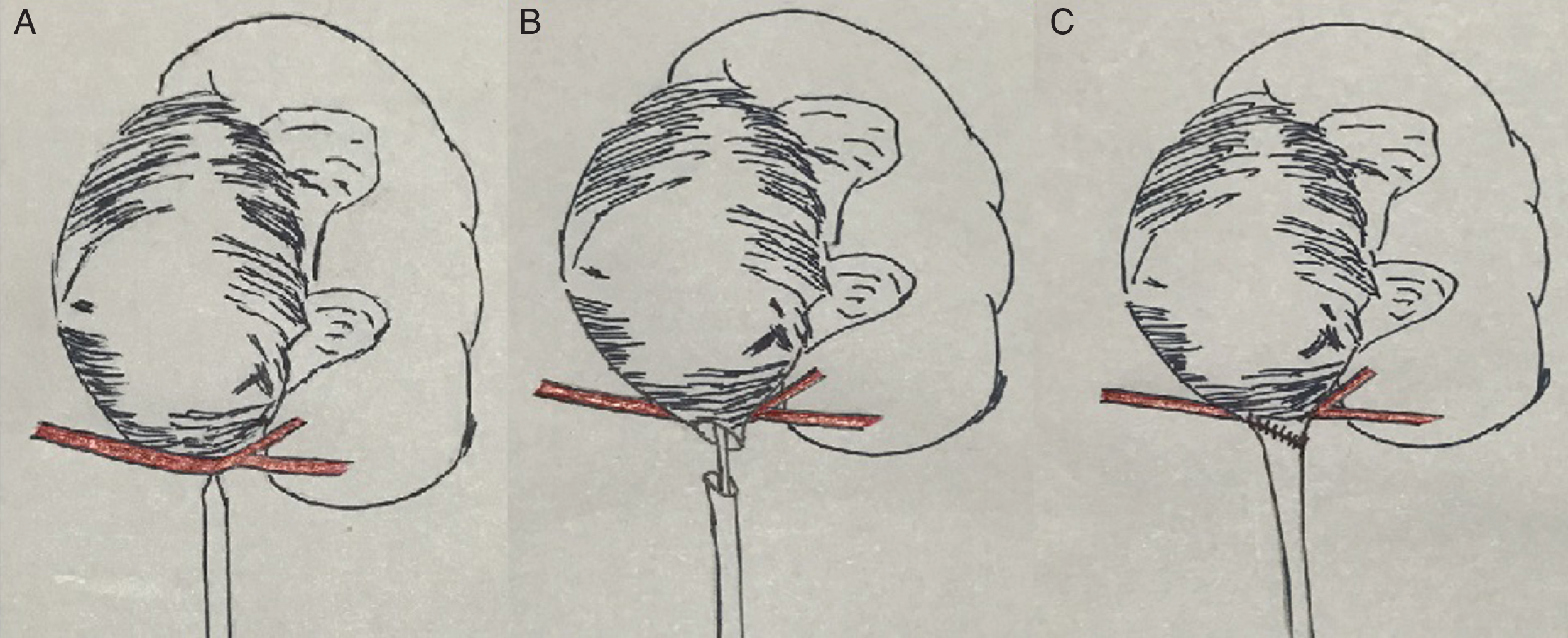
Anderson-Hynes Surgery Procedure in this case. A). An aberrant vascular bundle (red) crosses over the renal pelvi-ureteric junction at the left ureter, causing hydronephrosis. B), The dilated pelvic and upper ureter were separated and the narrow segment were removed, the pelvic and upper ureter were shaped to a 60 degree parallel bevel. A double J stent were implanted into the ureter and pelvic. C), An oblique anastomosis were made between the pelvic and upper ureter in front of the aberrant vascular.
Hydronephrosis is generally defined as dilatation of the renal pelvis and calyces resulting from obstruction to the flow of urine [12]. The causes of hydroureter and hydronephrosis are classically divided into three types: extraureteral lesions (such as postperitoneal fibrosis), compression by aberrant vessels or fibrous band outside of ureter, and structural abnormalities in ureteral wall (such as stone, scaring tissue or inflammatory) [13–16]. Radiographic studies are of decisive significance in the diagnosis and surgical management of hydronephosis [17, 18]. The CTA and MRA image were used to diagnose the hydronephosis caused by aberrant vascular. However, to the best of our knowledge CT angiography with 3D reconstruction was rarely used in the diagnosis of this disease [19]. In this case, the patient was a young male adult who presented no clinical symptoms and had no positive findings in laboratory examination. Preoperative ultrasound and IVU suggested left hydronephrosis. Finally, CT angiography with 3D reconstruction provided an accurate diagnosis for the cause of hydronephrosis.
In detection of the hydronephrosis, both artery and discharge phases of 3D-CT reconstruction with angiography played significant roles in the diagnosis of the disease. The 3D-CT clearly displayed the distended collection system of the left kidney as well as a sharp narrow sign at the inferior renal pole in both phases, indicating a PUJ obstruction caused by aberrant renal vessel.
Although the 3D-CT angiography cannot provide the information about the renal function and the renal pelvic structures, it offers accurate images renal vascular anatomy and the obstructive site of ureter [20, 21]. A published study showed that in 52 cases with hydonephrosis, 3D-CT angiography showed PUJ obstruction caused by aberrant vessels of the kidney in 14 cases, including accessory renal arteries in 10 patients, ovarian artery originating from left renal artery in one, right accessory renal artery in one and gonad veins in two cases. CT angiography with 3D reconstruction findings corresponded to operations in all these 14 cases. The sensitivity and specificity of CT angiography in evaluating UPJ obstruction was 100%, respectively [22, 23].
In conclusion, 3D-CT angiography is the first option in the diagnosis of renal vascular abnormality, such as aberrant renal vessel causing PUJ obstruction for pre-surgical planning.