
Abstract
Lymphoepithelial carcinoma (LEC) is an uncommon malignant neoplasm. Due to the complicated anatomical structure of the human head, standard imaging modalities including ultrasound, computed tomography (CT) and magnetic resonance imaging (MRI) scan remain limited in detection of salivary tumors. We used three-dimensional computed tomography angiography (3D-CT angiography) for the assessment and pre-operative surgical planning of facial fractures of a case with LEC. The study results demonstrated that 3D-CT angiography provided an insightful approach to preoperative evaluation in the treatment of salivary tumors.
Introduction
Lymphoepithelial carcinoma (LEC) is a rare malignancy characterized by undifferentiated malignant epithelial cells with marked infiltration of lymphoid cells into the stroma [1]. LEC most frequently occurs in the nasopharynx but has also been reported arising in various organs such as salivary glands, lungs, thymus, stomach, larynx, soft palate, uterus, bladder, and skin. LEC of the salivary gland was firstly described by Hilderman et al. in 1962. It is rare and accounts for 0.3–5.9% of malignant tumors of the salivary gland [2]. Current understanding is that the tumor arises from the salivary duct epithelial cells [3]. Up to 82% of those cases occurred within the parotid gland, followed by submandibular gland. Rarely, they can be located in sublingual, lip and palate glands [4, 5]. The terminology around LEC is not standardized, having diverse nomenclature in the literature such as, lymphoepithelioma-like carcinoma, malignant lymphoepithelial lesion, undifferentiated carcinoma with lymphoid stroma, and carcinoma in lymphoepithelial lesion. It was finally defined as lymphoepithelial carcinoma by histological classification of salivary gland tumors [6]. Although the etiology of LEC is unclear, Epstein-Barr virus (EBV) might be associated with LEC in endemic regions, especially in Southeast Asia [7]. Reports demonstrated a roughly equal gender distribution and the age range from 20 to 60 years [8, 9].
The salivary glands include three major glands and several small accessory salivary glands. The major salivary glands are the parotid glands, located anterior to the ear, the sublingual glands, located under the tongue and the submandibular glands, located laterally below the mandible. Because salivary glands are radiolucent tissue, traditional imaging methods are limited in diagnosing salivary tumors. When the tumor invaded surrounding tissues symptoms include limitation of oral opening, facial paralysis and tongue numbness. Presently, there are many imaging modalities utilized for the diagnosis of salivary disease, such as plain radiography, sialography, ultrasound, MRI, CT scan, and salivary gland scintigraphy.
Three-dimensional (3D) reconstruction imaging based on CT or MRI is increasingly utilized in diagnosis and treatment of disease. The 3D reconstructed images provide more detailed information about the anatomic relationship of tumors for better preoperative planning. 3D reconstructed CT plays an important role in determining the prognosis of other malignancies like renal tumors [10]. The diagnostic value of multi-slice spiral CT in renal trauma was evaluated and kidney injury was diagnosed more accurately [11]. Compared with 2D diagnostic imaging tools, the 3D magnetic resonance urography provides more valuable information about urinary tract anatomic abnormalities for stone disease preoperative planning [12]. Furthermore, some have observed rare tumor morphology and inferior vena cava thrombus not otherwise discerned in 2D imaging [13]. Dynamic video originated from 3D reconstructed CT images can help surgeons make better preoperative assessment resulting superior therapeutic outcomes. With the aid of 3D dynamic video, a large entire adrenal carcinoma was successfully excised laparoscopically via a retroperitoneal approach [14]. A combination of 3D-static images and rotated reconstruction images generated by cone beam computed tomography (CBCT) is being utilized for diagnosis of complex malocclusion cases, aiding in improved prognosis and treatment of dental disorders [15]. 3D Micro-CT images can potentially be used in detection and quantification of root contour for orthodontists [16]. Herein, we introduce a case where 3D-CT angiography was applied for diagnosing and surgical planning of LEC.
Case presentation
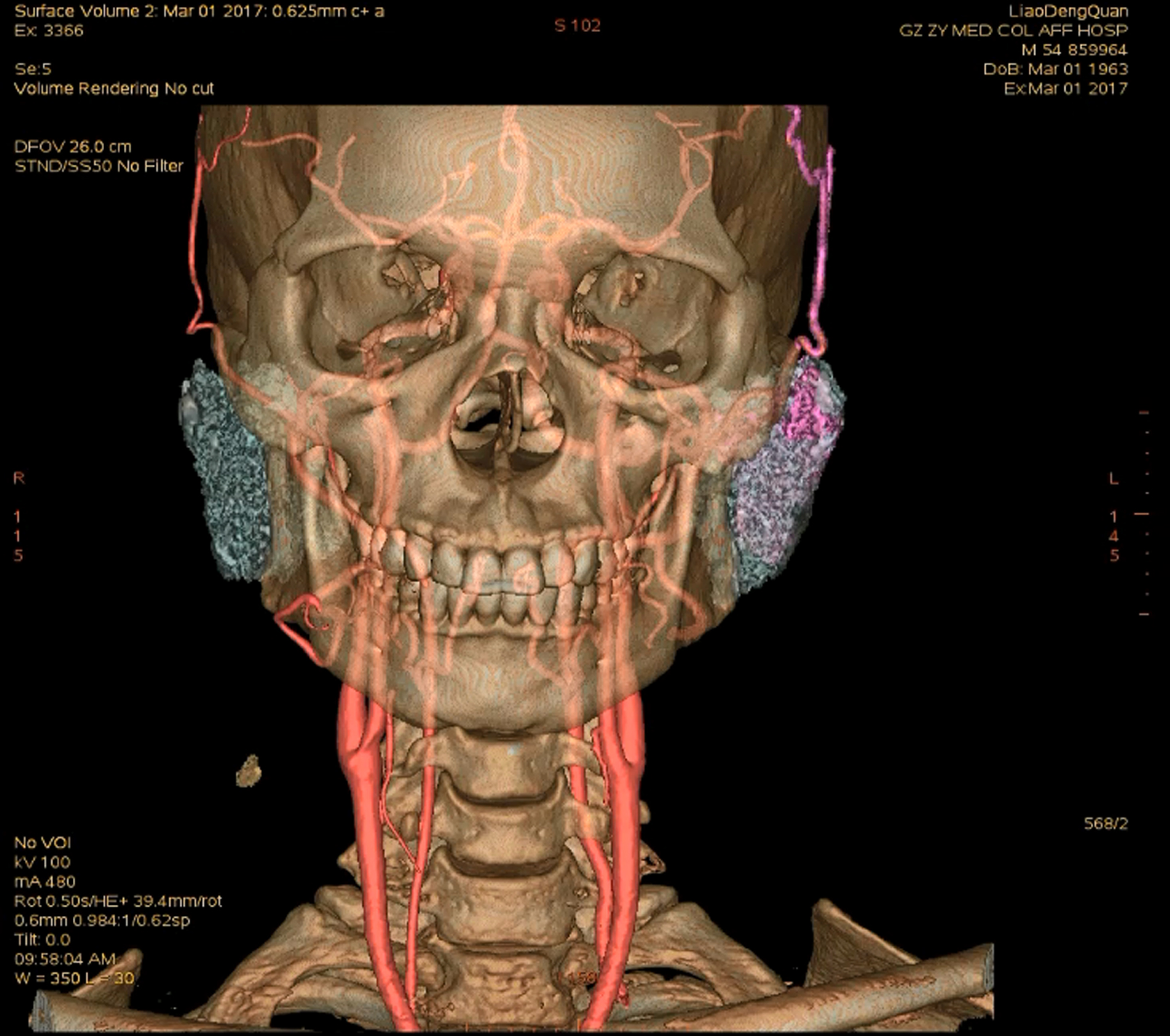
A 52-year-old man presented with a 4-month history of a painless and enlarging left parotid mass. On examination a 3-cm mass in the left preauricular area was found. The mass was firm, non-mobile, was minimally tender, adhered to the surrounding skin and tissues. Facial nerve function was intact. No cervical lymphadenopathy was noted. Chest CT revealed diffuse small nodules in the bilateral lungs. Calcified mediastinal and bilateral hilar lymphadenopathy was noted. Preoperative 3D-CT angiography demonstrated two distinct tumors located at the superior and inferior portions of parotid (Figs. 1 and 2). The bigger mass was adherent to the superficial temporal artery, which was the main source of blood supply to the tumor. Operative finding were consistent with preoperative 3D-CT (Fig. 3). He was treated with superficial parotidectomy and complete removal of both masses. Intraoperative frozen section confirmed malignancy and continued dissection was undertaken, taking care to spare the facial nerve. Due to the present lymphadenopathy intraoperatively diagnosed as metastatic carcinoma by fast frozen pathology, selective Neck Dissection (I – III levels) was performed. Facial paralysis occurred after the operation. Postoperative histopathological examination demonstrated the tumor Lymphoepithelial carcinoma (Fig. 4). Postoperatively, the patient was referred for radiation therapy, undertaken at an outside institution. The patient followed up 4 months postoperatively without evidence of recurrence.

3D-CT demonstrate two tumors (fuchsia) located in the parotid glands (Gray), the bigger tumor (pink) being located at the superior portion of the parotid, the smaller (deep pink) located at the inferior portion.
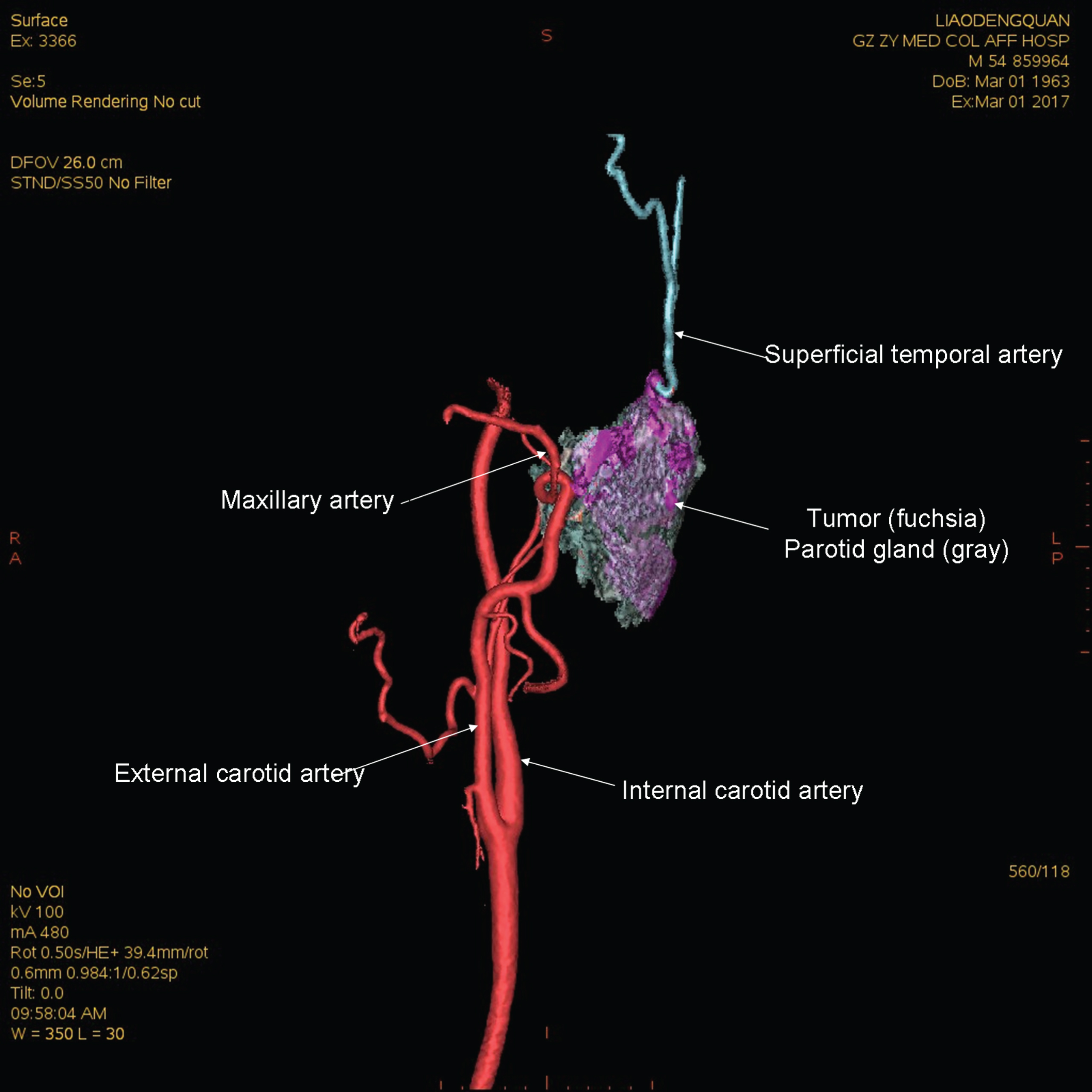
The bigger tumor adhered to the superficial temporal artery (blue).
A dynamic video based on 3D reconstruction of CT images and cerebral angiography.
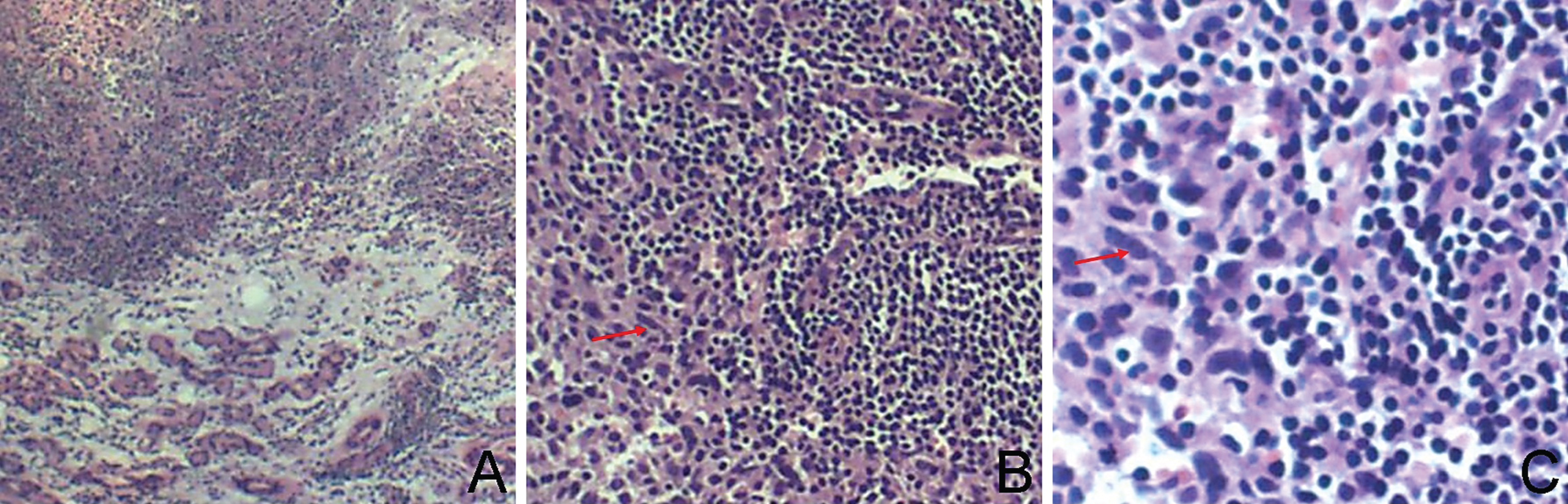
Histopathological characteristics of the LEC of the parotid gland. A. Intratumoral lymphocytes invasion, ×40. B. lymphoid cells, ×100. C lymphoid cells (Red arrowheads), ×200.
3D imaging angiography has been utilized in clinical examination, particularly in the diagnosis of vascular disease. It can assess the course and shape of blood vessels in order to guide treatment. 3D angiography is also utilized in cardiothoracic surgery during lung operations. It can map the course of blood vessel or aberrant vessel to improve the operative safety to reduce the risk of severe bleeding intraoperatively. In the minimally invasive surgical specialties, a careful preoperative evaluation by 3D-CT angiography enables surgeons to operate more safely and with fewer complications [17].
Early LEC’s of salivary gland present with a painless, hard mass and intact facial nerve function. The mobility of the mass decreases with increased propensity to affix to adjacent tissue. Facial nerve involvement often causes facial paralysis and carotid lymphadenectomy. Facial paralysis occurs in 20% of patients and 40% of the cases were found to have cervical lymph node metastasis [18]. Pathologically, tumor cells were arranged in irregular nests with lightly stained cytoplasm with acidophilic, vacuoles and scattered prominent nucleoli. Occasionally, the above pathology is accompanied with abnormal mitoses and interstitial lymphocytic infiltration to form a lymphoid follicle [1, 19]. Immunohistochemistry demonstrates strong staining for cytokeratin in the epithelial component and CD45 among the lymphoplasmacytic infiltration. Treatment of LEC is generally radical parotidectomy. At present, surgical excision followed by postoperative radiation therapy is considered the treatment of choice for LEC. 2, 5 and 10-year survival rates are reported to be 91%, 66%, and 29%, respectively [1]. Clinically, pleomorphic adenoma, mucoepidermoid carcinoma, and adenoid cystic carcinoma as the most common salivary gland tumors and need to be differentiated from LEC (Table 1).
A comparison of common tumors and LEC within salivary glands
A comparison of common tumors and LEC within salivary glands
Abbreviations: PA- pleomorphic adenoma; ACC- adenoid cystic carcinoma; MEC- mucoepidermoid carcinoma; LEC- Lymphoepithelial carcinoma. Notes: *Incident rate in all patients with salivary gland tumors.
Plain radiography is an inexpensive and simple way of studying sialolithiasis in the salivary gland. But only one-fifth of ductal sialoithiasis are radiopaque. Furthermore, phlebolithiasis or calcified lymph nodes may mimic sialolithiasis on plain radiography. Because of the limitations of radiography for soft tissue, it is limited to diagnose salivary tumors.
Sialography
By injecting contrast agents into the duct, the salivary ductal system can be efficiently imaged with conventional X-ray or CT. These sialography techniques have some benefits for imaging ducts, ductules and parenchyma of the salivary gland. They are useful for diagnosis of ductal stenosis. Irregular pooling of contrast agent and ductal obstruction without the presence of sialolithiasis may be indirect signs of malignancy. Sialography for the diagnosis of parotid tumor is limited. Potential complications associated with sialography include rupture of the ductal system, activation of clinically dormant infection and adverse reactions to the contrast agent used. The examination is contraindicated in acute sialoadenitis and in cases of former allergic reaction to iodine-containing contrast agents. Clinically, sialography has a higher failure rate because ionizing radiation exposure depends on the operator’s technical skills. Additionally, quick cannulation of the ductal system increases the risk of radiation injuries to the operator.
Ultrasound
Ultrasound (US) is in many cases the initial imaging modality for assessment of the salivary glands [20]. Using high frequency (7–15 MHz) probes, US has a high accuracy for delineating benign and malignant lesions, especially when superficial [21]. US has been evaluated in both benign and malignant conditions. It is widely available in clinic, can be used for guiding biopsies, and can be performed in the emergency setting at bedside [22]. US is limited in evaluating structures behind bone, such as the parts of the parotid gland that lay deep to the mandible.
In acute inflammation, US is utilized to detect sialolithiasis or abscesses. It has a high sensitivity for detecting sialolithiasis, and has replaced standard sialography. In a study by Gritzmann, 94% of sialolithiasis was detected with US in a cohort of 174 patients [20]. The sensitivity for sialolithiasis was only 77 % in general, but increased to 94% when looking at sialolithiasis larger than 3 mm [23, 24]. In acute viral infection, such as with mumps, symptoms are usually bilateral and the glands are enlarged and more hypo-echoic due to edema. Increased visualization is possible using color Doppler. US was a useful diagnostic tool but it has poor accuracy for detecting tumor boundaries, often differences are seen intraoperatively.
MRI
Magnetic resonance imaging (MRI) is important in evaluation of major salivary gland disease, especially neoplastic disease. If there is a strong suspicion of malignancy, MRI is the method of choice [25]. If the tumor is large (>3 cm) or located in the deep lobe of the parotid gland, US is limited and MRI should be performed. MRI provides a large variety of soft tissue signal differences and is helpful in delineating the extent of tumor. Skull base invasion is clear on MRI [26]. In the case of a large malignant tumor with cranialnerve deficit, MRI should be performed to evaluate the locate extent of the lesion, to detect perineural tumor spread and intracranial invasion [20, 27]. MRI has been applied to sialography similarly to magnetic resonance cholangio-pancreatography for the biliary duct [28]. This is where the patient’s own saliva is used as contrast agent. Magnetic resonance sialography has poor spatial resolution compared to conventional sialography but may be an alternative if x-ray sialography cannot be performed, especially due to acute inflammation [29]. The advantages of MRI are no ionizing radiation and the non-invasive nature. However, the cost of MRI is expensive.
CT
Computed tomography (CT) of the salivary glands is easy, rapid and cheap compared to MRI. However, patients are exposed to ionizing radiation this increasing the risk of ionizing radiation injury. Non-contrast enhanced CT can demonstrate sialolithiasis, tissue calcification, and bony erosion caused by malignant lesions, or infection. Contrast enhanced CT can increase the visualization of boundary between tumor and surrounding tissue.
Salivary gland scintigraphy
Börner first introduced 99mTc pertechnetate for salivary gland scintigraphy in 1965. It has been used to examine the extent of disease in Sjgren’s syndrome (SS). Salivary gland scintigraphy is a functional examination, which is helpful for prediction of salivary gland function following radiation therapy [30]. Scintigraphy cannot be used to differentiate between benign and malignant tumors, nor can it predict the outcome of a surgical procedure.
Different types of salivary disease have different preferred imaging modalities. Which method is preferred depends on the location and manifestation of disease. Sometimes we need to utilize multiple examinations. US is the initial modality both for assessing superficial parotid and submandibular gland lesions, salolithiasis and in guidance for biopsies. Sialography is used to assess the salivary ductal system. MRI, CT and US are preferred for obstruction of ducts or salivary gland tumors. Scintigraphy is preferred for examination for parenchymal damage and glandular function, in particularly SS [31] (Table 2).
Recommendation for imaging detection approaches in diagnosis of the salivary diseases
Recommendation for imaging detection approaches in diagnosis of the salivary diseases
Abbreviations: SS- Söjgren Syndrome; US- Ultrasound; CT- Computed tomography; MRI- Magnetic resonance imaging; 3D-CT- Three dimension computed tomography.
Preoperative planning of malignant masses must define the boundaries of the lesion. At present, CT or MRI are used to assess the tumor boundaries. But traditional imaging modalities are static 2D or 3D images. In this report, we used a dynamic 3D-CT technique to observe the relationship between the tumor and surrounding tissues, especially blood vessel and bone, showed in the video (Fig. 3). It enabled the surgeon to perform a safer and more efficient operation.
Because of the complicated anatomical structures in the facial region and lack the specific clinical manifestation of LEC, it is a challenge to examine mass features among the adjacent organs and tissues by routine x-ray imaging. The final diagnosis needs histopathological examination for further confirmation.
The dynamic 3D-CT angiography reconstruction provides an excellent tool to communicate with patient and family members before surgery. It could improve understanding for disease and break down communication barriers caused by different cognitive levels. In addition, 3D-CT angiography offers a useful teaching method for medical students and residents with better comprehension of tumor shape. The dynamic video based on 3D reconstruction of CT images can provide more visual characteristics of the tumor for young doctors and nurses in the preoperative discussion, resulting in patients getting more effective governance during the perioperative period. The dynamic 3D-CT also provides teaching material for clinicians.
However, 3D-CT angiography has some disadvantages and limitations, such as expensiveness, poor imaging for small branches of vasculature. When the blood supply of tumor is poor, the boarders between the tumor and adjacent tissues are hard to discern. In this situation, we can assess with dynamic 3D-MRI based on 3D reconstructing of MRI images, but the cost of examination would be great.
Base on this case report, the dynamic 3D-CT angiography is highly recommended for use to assess the tumor, especially deep lesions or diseases that have a close relationship with blood vessels, such as hemangioma or vascular malformation. It will also provide better clinical images for preoperative physician-patient communication, planning and medical education.
Footnotes
Acknowledgments
This study has been supported by Science and Technology Fund of Guizhou Province (LKZ [2013] 36) and Start-up Fund for Master of Zunyi Medical University (F-618), Key Clinical Specialist Construction Programs of Guizhou Province (KY2017-07).