
Abstract
OBJECTIVE:
Correlation between myocardial infarction (MI) scar by cardiac magnetic resonance and the Lown’s classification of ventricular premature beats (VPBs) is poorly understood. This study aims to investigate the correlation between the MI scar characteristics by delayed-enhancement magnetic resonance imaging (DE-MRI) and the Lown’s classification of VPBs.
METHODS:
Sixty-five patients, in the convalescence stage and consolidation phase of MI, were included in this retrospective study. All patient were divided into VPBs group (n = 39) and non-VPBs group (n = 26 patients) according to the clinical diagnostic criteria of Universal Definition of MI scar. VPBs patients were assigned to Lown’s I-II group and Lown’s III-IV subgroup in accordance with the Lown classification criteria. Cardiac function parameters and MI scar characteristics were detected by cardiac magnetic resonance (CMR) and DE-MRI, respectively.
RESULTS:
Lown’s classification was negatively correlated with left ventricular ejection fraction (LVEF), peak ejection rate (PER) and peak filling rate (PFR) (–0.724, –0.628, –0.559), and positively correlated with MI area, MI integral, MI segments number and left ventricular end systolic volume (LVESV) (0.673, 0.655, 0.586, and 0.514), respectively.
CONCLUSIONS
The study indicated that MI area and MI integral were strongly associated with Lown’s classification.
Keywords
Introduction
Myocardial infarction (MI) is a dynamic pathological process which begins with acute regional myocardial ischemia and finishes with fibrotic repair. During the acute phase, ventricular arrhythmias (VA) are life threatening cardiac arrhythmias and remain the most common and much feared cause of sudden cardiac death (SCD) [1]. The presence of complex premature beats in patients with prior MI has been proved to make an independent contribution to increased risk of death [2]. In addition, there was study documented that the presence of complex forms of ventricular premature beats (VPBs) was associated with a threefold increased incidence of SCD in the 5 year period after acute MI [3]. Patients with malignant VA consistently exhibit high frequency as well as complex forms of VPBs [4]. Data reduction of VPB activity was carried out by qualitative analysis and adhered to the following Lown classification of VPBs: Grade 0, no ventricular premature beats; grade I, occasional (≤ 30/h; A,≤l/min and B,≥l/min); grade II, frequent ventricular premature beats (≥l/min or 3/h); grade III, multiform ventricular premature beats; grade IV, repetitive ventricular premature beats (A, couplets and B, salvos or ventricular tachycardia) and grade IV, early ventricular premature beats (abutting or interrupting the T wave) [5]. It was generally believed that the risk of premature ventricular was high above the third grade. It is of great clinical significance to improve the early prediction of VPBs and the prognosis of patients with coronary heart disease.
As a non-invasive, non-radiating technique, cardiac magnetic resonance (CMR) allows serial assessment of the changes in ventricular volumes, myocardial scar burden, coronary perfusion, and the ejection fraction that can be predictive of ventricular tachycardia (VT) and SCD [6, 7]. With the rapid development of CMR techniques, Delayed-Enhancement Magnetic Resonance Imaging (DE-MRI) has been considered to be a more sensitive and higher resolution imaging method for detecting the MI scars [8]. Ricciardi et al. studied periprocedural infarct by Delayed-Enhancement CMR (DE-CMR) in 14 subjects, the results showed 9 subjects with raised creatine kinase (CK-MB) had a median mass of infarcted myocardium of 2 g (assuming a myocardial specific gravity of 1.05 g/cm3) [9], while 10 g lesions could be detected by radionuclide perfusion imaging [10]. However, there are few studies focusing on the correlation between MI scar characteristics detected by CMR and the Lown’s classification of VPBs. Therefore, in our study we examined cardiac function parameters by CMR and MI scar characteristics by DE-MRI and preliminary investigate the association between MI scar characteristics and Lown’s classification of VPBs.
Methods
Patients
A total of 100 patients with coronary heart disease and MI scar were enrolled at the Department of Cardiology, the Second Affiliated Hospital of Kunming Medical University from July 2013 to 2015 December. The study was approved by the ethical committee of the Second Affiliated Hospital, Kunming Medical University and was conducted in accordance with the Helsinki Declaration of 1975. Written informed consent was obtained from all patients. Patients were excluded if they met the following criteria: (1) Patients with other heart diseases, such as dilated cardiomyopathy, hypertrophic cardiomyopathy and myocarditis, etc.; (2) Patients with right ventricular infarction; (3) Patients with a dynamic electrocardiography (ECG) recording time less than 22 hours or poor record quality, insufficient and missing records. (4) Patients with body metal implants, artificial heart materials and claustrophobia. (5) Poor CMR image quality.
Lastly, Sixty-five patients in the convalescence stage and consolidation phase of MI diagnosed by CMR were included in this study. Patients were divided into VPBs group (39 patients, 59.46±13.30 years) and non-VPBs group (26 patients, 52.31±12.10 years) according to the clinical diagnostic criteria of Universal Definition of MI scar, which defined by expert consensus document 2007 European Society of Cardiology (ESC) and the American Heart Association (AHA) jointly. Patients in VPBs group were further assigned to Lown’s I-II and Lown’s III-IV in accordance with the Lown classification criteria.
DE-MRI
MRI examinations were performed using Achieva 3.0T scanner (Philips Medical Systems, Best, Netherlands), with the gradient field strength at 40mT/m and gradient switching rate at 200mT/m. Breath-hold CMR was used and 25 images were captured in a cardiac cycle. Scanning parameters were as follows, TR = 39.76 ms, TE = 1.22 ms, slice thickness = 8 mm and FOV = 276 mm×340 mm. DE-MRI scanned 3 layers 4-chamber level long-axis, 3 layers 2-chamber long-axis and, 8–10 layers left ventricular short-axis gradually covering the entirety of the left ventricle from the base to the apex.
After scanning, first-pass perfusion image acquisition synchronized with contrast agent injection. A total dose of 0.05 mmol/kg gadolinium-diethylenetriamine pentaacetic acid (GD-DTPA) with a flow rate at 5 ml/s was administered intravenously through the vein by automatic pressure syringe. After first injection, 0.1 mmol/kg GD-DTPA with a flow rate at 2 ml/s was injected again. Following a 5–30 min delay time, the image was obtained by cardiac electrical gating technique in the front of chest. The scanning sequence was Breath-hold phase sensitive inversion recovery tuibo field echo (PSIR_TFE_BH) with the following imaging parameters: mode = M2D, single-shot; TFE = 19; shim = default; TR/TE = 6.1/3.0 ms; flip angle = 25°; thickness = 10 mm; FOV = 320 mm×320 mm and bandwidth = 130 Hz.
Image analysis
MR images were analyzed by EWS software packages. Cardiac function and MI scar parameters of were traced by the combination of automatic delineation and manual modification on Argus software, and then the global and segmental function of left ventricle was calculated by post-processing system. Left ventricular function parameters including left ventricular ejection fraction (LVEF), left ventricular end-diastolic volume (LVEDV), left ventricular end systolic volume (LVESV), myocardial mass (MM), stroke volume (SV), cardiac output (CO), cardiac index (CI), Peak ejection rate (PER), peak filling rate (PFR), ventricular aneurysm and wall motion were calculated by CMR. In addition, left ventricle was divided into 17 segments in accordance with the American Heart Association standards [11]. The transmural extent of MI in each segment was graded from 0 to IV: 0, normal; I, <25% transmural extent, scored 1; II, 26–50%, scored 2; III, 51–75%, scored 3; IV, 76–100%, scored 4. The MI integral was the sum of transmural extent from 17 segments. These tests were blindly carried out and consensus was achieved by two radiologists.
Statistical analysis
All statistical analyses were performed using the SPSS17.0 software package for Windows (SPSS Inc., Chicago, IL, USA). Measurement data was expressed as means±SD. The association between the variables was tested using the chi-square test. Univariate analysis and logistic regression analysis were used to analyze variables. Correlation was performed by Spearman rank correlation analysis. The level of statistical significance was set at 0.05.
Results
Clinical characteristics, cardiac function indexes and MI scar characteristics of 65 MI scar patients
65 patients in the convalescence stage and consolidation phase of MI were assigned to VPBs group (including 30 men and 9 women), and non-VPBs group (including 17 men and 9 women). Further, 39 patients with VPBs were graded to Lown’s III-IV group (n = 22) and Lown’s I-II group (n = 17). As shown in Table 1, patients with VPBs had significant differences in LVEF, LVESV, MM, SV, PER, PFR, VA, MI area ratio, MI integral, MI segments number and transmural segments compared with patients without VPBs.
Clinical characteristics, cardiac function indexes and MI characteristics of 65 myocardial infarction scar patients
Clinical characteristics, cardiac function indexes and MI characteristics of 65 myocardial infarction scar patients
MI, Myocardial infarction.
*P < 0.05,
**P < 0.01.
The significant cardiac function indexes and MI characteristics from Table 1 were further analyzed by logistic regression analysis. The result suggested that MI integral, CI, LVEF and wall motion abnormality might markedly contribute to VPB (Table 2). And MI integral was the predominant index.
Logistic regression analysis of significant cardiac function indexes and myocardial infarction scar characteristics
Logistic regression analysis of significant cardiac function indexes and myocardial infarction scar characteristics
Clinical characteristics including age, gender, obesity, hypertension, diabetes, smoking, drinking and dyslipidemia were not statistically significant different between Lown’s III-IV patients and Lown’s I-II patients (P > 0.05, Table 3). Obvious differences in cardiac function parameters (LVEF, LVESV, LVEDV, PER, PFR) and MI characteristics (VA, MI area ratio, MI integral and transmural segments) were found between these two groups. LVEF, LVESV, LVEDV, PER, PFR was significantly decreased in Lown’s III-IV patients when compared to patients in Lown’s I-II group (P < 0.05), and LVESV, LVEDV was significantly increased in Lown’s III-IV patients when compared to patients in Lown’s I-II group (P < 0.05), while DE-MRI-detected MI area ratio and MI integral were much higher than those in Lown’s I-II group (P < 0.05, Table 3).
Clinical characteristics, cardiac function indexes and myocardial infarction scar characteristics of Lown’s III-IV patients and Lown’s I-II patients
Clinical characteristics, cardiac function indexes and myocardial infarction scar characteristics of Lown’s III-IV patients and Lown’s I-II patients
*P < 0.05,
**P < 0.01.
The correlation of MI area, MI integral, MI segments number, LVEF, PFR and Lown classification from 39 patients with VPBs were shown in Table 4. Spearman rank correlation analysis revealed that there was a negative correlation between LVEF, PFR and the Lown classification (P < 0.01). At the same time, Lown classification had a positive correlation with DE-MRI-detected MI area, MI integral and MI segments number (P < 0.01).
The correlation of MI area, MI integral, MI segments number, LVEF, PER, PFR, ESV and Lown classification from 39 patients with VPBs
The correlation of MI area, MI integral, MI segments number, LVEF, PER, PFR, ESV and Lown classification from 39 patients with VPBs
**P < 0.01.
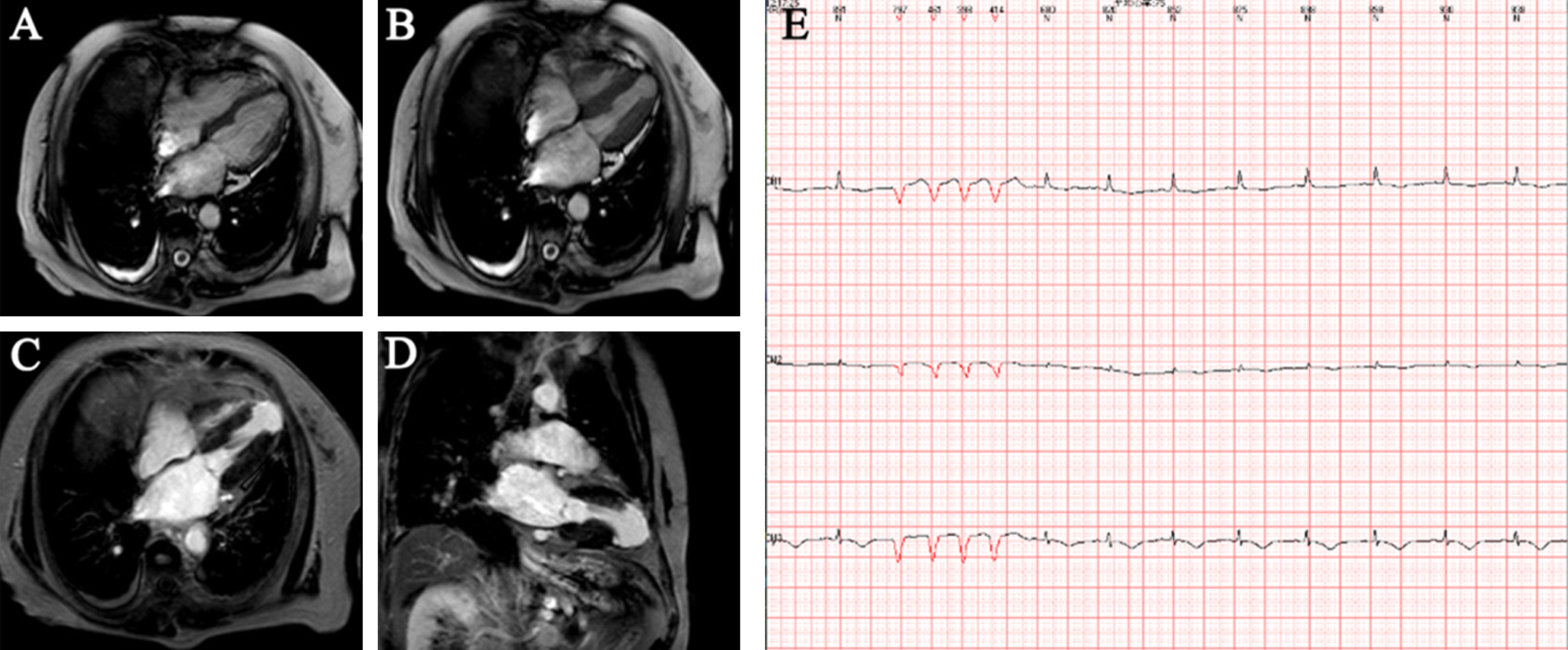
As Fig. 1A-B shown, MR images of a patient without VPB showed systolic and diastolic of MR functional cardiac imaging in left ventricular four-chamber, and MR cardiac Explorer postprocessing software showed that cardiac function was 34.5%. The middle part of anteroseptal MI was found by DE-MRI (Fig. 1C-D), with a transmural extent of 25–50%, MI integral score of 2 and MI area of 3.5%. ECG showed sinus rhythm without VPB (Fig. 1E).

A forty-six year old patient (male). (A-B), systolic and diastolic of MR functional cardiac imaging in left ventricular four-chamber. (C-D), left ventricular apical, middle and basal short-axis detected by DE-MRI; (E) 24 hours 12 lead electrocardiogram. DE-MRI, delayed enhanced-magnetic resonance imaging.
MR images from a patient with Lown’s IV B VPB were shown in Fig. 2. Apical VA was observed in Fig. 2A-B, and cardiac function was recorded as 55.7%. Apical and apical 13, 14, 15, 16 and 17 transmural segments MI with a 100% transmural extent, approximately 30.6% MI area and 20 MI integral score were detected by DE-MRI (Fig. 2C-D).
A fifty-nine year old patient (female). (A-B), systolic and diastolic cardiac MR images of left ventricular four-chamber; (C-D), left ventricular four-chamber level and two-chamber level detected by DE-MRI; (E) 24 hours 12 lead electrocardiogram. DE-MRI, delayed enhanced-magnetic resonance imaging.
MI scar formation is commonly accepted as a leading cause of ventricular remodeling which has been generally considered as a determinant of ventricular arrhythmias. Ventricular arrhythmias are an important cause of morbidity and associated with an increased risk of sudden death in patients with heart disease. Therefore, assessment of viable myocardium is great importance for the guidance of treatment and the judgment of prognosis. MRI is the imaging method with the highest resolution of soft tissue contrast. It can directly calculate the volume of the heart cavity without depending on geometric shape assumption. Its accuracy is not affected by the shape and size of the heart cavity. It has the advantages of small artificial error, accurate measurement and good repeatability. At present, it is the “gold standard” for measuring cardiac volume and ejection fraction [12]. Therefore, MRI has absolute superiority in detecting scar features and analyzing cardiac function of MI. Furthermore, clinical researches have shown a correlation between MI scar detected by CMR and histopathology [13, 14]. Therefore, the ability of CMR to accurate identify the characteristics of MI scar provides a potential diagnostic method for patients with MI.
DE-MRI takes advantages of the microscopic remodeling of the ventricle, and accurately detection of the infarction core, the infarction area and the myocardial hypertrophy. Selvanayagam [15] suggested that preoperative DE-MRI could accurately predict myocardial viability after surgical revascularization and a strong correlation between the transmural extent of hyperenhancement and the recovery in regional function at 6 months was found, providing an important role for this technique in clinical viability assessment. In a prospectively study, 30 patients were evaluated for arrhythmogenic right ventricular dysplasia/cardiomyopathy (ARVD/C) by DE-MRI, indicating that noninvasive detection of right ventricle myocardial fibro-fatty changes in ARVD/C was possible by DE-MRI instead of endomyocardial biopsy [16]. Adabag [17] also demonstrated that it was much more susceptive to ventricular tachyarrhythmias for patients with hypertrophic cardiomyopathy identified by contrast-enhanced CMR. In the present study, the characteristics of MI scar, including DE-MRI-detected MI area ratio, number of MI segments and transmural segments, and MI integral were found to be risk factors for VPBs.
Previous animal studies had suggested that the transmural extent of acute MI detected by contrast-enhanced MRI was associated with early restoration of flow and future improvements in contractile function [18]. Further clinical research found a decrease in the transmural extent of infarction was related to greater long-term improvement in contractile function within dysfunctional regions [19]. Raymond J et al. [20] found that blood supply reconstruction is inversely proportional to the transmural extent of MI; in segments with >50% transmural extent of infarction, the cardiac function was unlikely to be completely recovered. Therefore, the assessment of the transmural extent of MI in myocardial segments by DE-MRI may be a potential option in Lown classification of VPBs. In this study, DE-MRI-detected transmural segments in Lown’s III-IV group were much higher than those in Lown’s I-II group. A positive correlation was observed between Lown classification and DE-MRI-detected MI area, MI integral and MI segments number. Therefore, patients with high Lown’s grade could be further evaluated MI scar characteristics and cardiac function by CMR. If the patient’s MI score was low, the ECG could be followed regularly. If the MI score was high, we need to monitor the ECG for a long time. Especially for Lown’s III-IV grade patients with high-frequency VPBs, interventional therapy was require, with, and CMR could contribute to preoperative localization of radiofrequency ablation.
LVEF had been the main indication applied to select patients for implantable cardioverter defibrillator (ICD) therapy. In this study, however, there was a low correlation coefficient between Lown classification and LVEF, and the difference between Lown ‘s 3–5 group and Lown’ s 1–2 group was not statistically significant (P > 0.05), indicating that LVEF was of little significance in predicting the risk of VBPs. Although EF was an excellent predictor for prognosis of heart failure and heart failure death, previous study had revealed a limitation of LVEF in accurate prediction of sudden death [21]. Buxton et al. [22] also showed higher mortality and a higher risk of sudden death in patients with EF >30% and other risk factors than patients with EF≤30%. Thus, risk of sudden death in patients with coronary disease depends on multiple variables in addition to EF. Therefore, for the prediction of the risk of VBPs, CMR detection of MI area and MI integral are likely to be more meaningful.
This study also has limitation. It showed the correlation between MI scar characteristics by cardiac MR and the Lown’s classification of VPBs in 65 patients involved in the present study. The small sample size used in this study remains as a limitation towards conducting further analysis. Thus, this study can only be regarded as a pilot study and further clinical research with larger sample size is warranted.
Conclusions
In conclusion, CMR can accurately and fully evaluate the heart function and MI characteristics of patients with MI. These help to assess the risk of VPBs and the Lown risk profile of VPBs, which contributes to early decrease in the malignant arrhythmia and cardiac sudden death, and increase in post-infarction survival rate.
Conflict of interest
The authors declare no conflict of interest.
Footnotes
Acknowledgments
This work was supported by the National Natural Science Foundation of China (Grant No. 81260213); the Young and Middle-aged Technical Academic Leaders Training Project in Yunnan province (Grant No. 2015HB068); the Yunnan Province Medical Subject Leaders Training Project (Grant No. D-201646); the Medical subject leaders Training Project in Yunnan Province (Grant No. D-201646); and the Applied Basic Research on Projects in Yunnan Province (Grant No. 2017FE468-178).