
Abstract
OBJECTIVE:
Intermittent CT fluoroscopic biopsy is a new technology, but has not been studied widely. This study aims to investigate correlation between the radiation dose and fluoroscopic CT exposure factors to establish the low dose parameters for performing percutaneous lung biopsies, as well as the relationship of the mean diameter and depth of lesions with radiation dose, procedure time, success and complication rates.
MATERIALS AND METHODS:
This is a retrospective study to analyse lung biopsies performed using intermittent CT fluoroscopic technique with 18 G semi-automated coaxial gun on 256 slice scanner. A total of 50 patients were included in the study. Biopsy was done in three mAs and KVp settings (30 and 70, 10 and 120, 30 and 120, respectively). The statistical data analysis was performed using SPSS Statistics software.
RESULTS:
Pneumothorax occurred in 22 % of cases. Sampling rate was 98% but histopathological diagnosis was made in 94% cases. Mean procedure time was 30.5±11.1 minutes. Low dose protocol (30 mAs and 70 KVp) had least radiation exposure during biopsy procedure (p < 0.001) with similar success rate, complications and procedure time (p > 0.05) in comparison with high dose protocol (10 and 120, 30 and 120 mAs and KVp, respectively). Mean diameter of lesions didn’t correlate with radiation dose, success rate, complications and duration of procedure (p > 0.05) while significant association was found when depth was correlated with radiation exposure during fluoroscopic biopsy, duration of procedure and complication rates (p < 0.05) while no association was found with success rates.
CONCLUSION:
On third generation dual energy source CT scanner, reducing mAs and KVp to 30 and 70 during fluoroscopy biopsy can produce images whose complications and success rates are comparable to high dose CT. In general, intermittent CT fluoroscopy guided lung biopsy has good success rates with acceptable complications, while utilising less radiation dose and procedure time.
Introduction
Lung cancer is one of the leading causes of death in both men and women [1]. Diagnosis is of utmost importance before definite treatment can be started. CT guided lung biopsy is the procedure of choice in most cases [2]. However, CT scan can be hazardous to the patient and the operator due to ionising x-ray radiation.
Intermittent fluoroscopy is the technique where instead of continuous image acquisition, the operator takes intermittent slices in sets of three alternating with insertion, advancement and manipulation of the needle. These modern advancements can theoretically reduce the time of procedure and the radiation dose. Although low-dose CT has been extensively investigated and tested for many cancer imaging purposes including the interventional procedures [3–5], but few studies have been conducted which evaluated the outcomes of intermittent CT fluoroscopic biopsy procedures. We conducted this study to establish the ultra-low dose protocol for performance of lung biopsies and to study other parameters which have not been extensively studied.
Specifically, the objectives of this study include (1) to evaluate the radiation dose, time of procedure, success and complication rates of intermittent fluoroscopic computed tomography (CT) guided core lung biopsies; (2) to correlate the mean diameter and depth of lesions with the radiation dose, time of procedure, success and complication rates of the procedure; and (3) to evaluate the relationship between radiation dose and fluoroscopic CT exposure factors to establish the low dose CT parameters for performance of percutaneous biopsies.
Materials and methods
All patients who presented with pulmonary or mediastinal nodules or masses or any other focal lesion in the thorax, requiring histopathological confirmation underwent intermittent CT fluoroscopic guided biopsy using 18 G semi-automated coaxial gun on a Siemens Somatom Definition Flash machine (256 Slice scanner, Erlangen, Germany) using iFluoro sequence. Exclusion criteria included pregnancy, coagulation and bleeding disorders. Pre-existing diseases like severe emphysematous changes, bullous or cystic disease close to the lesion were excluded from the study. The procedure was performed by one of the three radiologists (two senior residents and one consultant) with at least two radiologists being present at the time of the procedure. Consent for the procedure was taken in all cases. Topogram of the thorax was taken followed by the plain CT of the region of interest at 120 KV with automatic tube current modulation, acquiring 5 mm thick slices and reformatted in 1 mm thick slices in lung, bone and mediastinal window, increment: 0.75 mm, pitch 1.2, rotation time: 0.5 sec. Planning was done on the console workstation on MPR view, with point of entry and depth of lesion estimated preprocedural.
The site was prepared and local anaesthesia infiltrated up to the pleura. Biopsy was done at 70KV and 30 mAs (in most of the cases) and section thickness was 5 mm. The CT fluoroscopy tool (iFluoro) generated three contiguous images, one at the desired site, and one each at head and foot sides. The window setting which was used was midway between soft tissue and lung window settings so that if lesions were closer to any vessel, the vessel could also be visualized. Also, the window setting could also be changed from the console by the technicians whenever required. The images were acquired on pressing the foot paddle by the operator. The coaxial needle (17 G) was introduced through the point of entry up to the required depth using intermittent presses of the footswitch. The needle was held by needle holder to avoid radiation exposure to the hand of the radiologist. When foot switch was pressed, 3 axial sections appeared on the screen which helped in guiding the needle.
After the coaxial needle reached the required depth, typically the peripheral portion of the desired lesion, the trocar was taken out and biopsy gun (18 G, 20 mm throw, COOKS Medical, Bloomington IN) introduced through the cannula and multiple samples, at least 4 cores, were taken. For lesions smaller than 1 cm in size, 18 G gun with 10 mm throw was used. Length of biopsy gun was 15 cm in either situation. Patient stayed on table for 5 minutes and then pneumothorax was screened by taking a single section at the same level. Post procedure, patients were shifted to recovery room. All patients went for Chest X-ray after an hour and those who had pneumothorax were reviewed in 30–60 minutes for stability or progression. Those who were asymptomatic with small stable pneumothorax didn’t require further follow up. Patients who developed moderate pneumothorax underwent aspiration with 50cc syringe attached to a three-way stopcock and connecting tube. Patients with severe pneumothorax underwent placement of 12F chest tube using standard techniques.
Results
Out of 53 cases received for biopsy, one with extensive mediastinal disease died in the CT suite before starting procedure, and two more could not comply because of dyspnea. Thus a total of 50 patients (22 females and 28 males; mean age 54.1±15.59 years) were included in the study. Mean diameter of biopsied lesion was 3.64±2.32 cm in size. Mean depth of the lesion was 4.89±1.86 cm from skin surface. Mean dose length product (DLP) including topogram, plain CT of the region of interest and fluoroscopic biopsy calculated was 232.76±113.14 mGy-cm, while mean DLP during fluoroscopic biopsy measured 21.468±25.95 mGy-cm.
The complication rate of the study was 22 % (11 patients) with 5 cases required intervention (10%). Six patients had mild asymptomatic pneumothorax, four patients had moderate pneumothorax and underwent manual syringe aspiration, and one patient had gross pneumothorax who underwent on table chest tube insertion. Six patients complained of streak hemoptysis which started next morning, and subsided with conservative management on an average of 3.5 days.
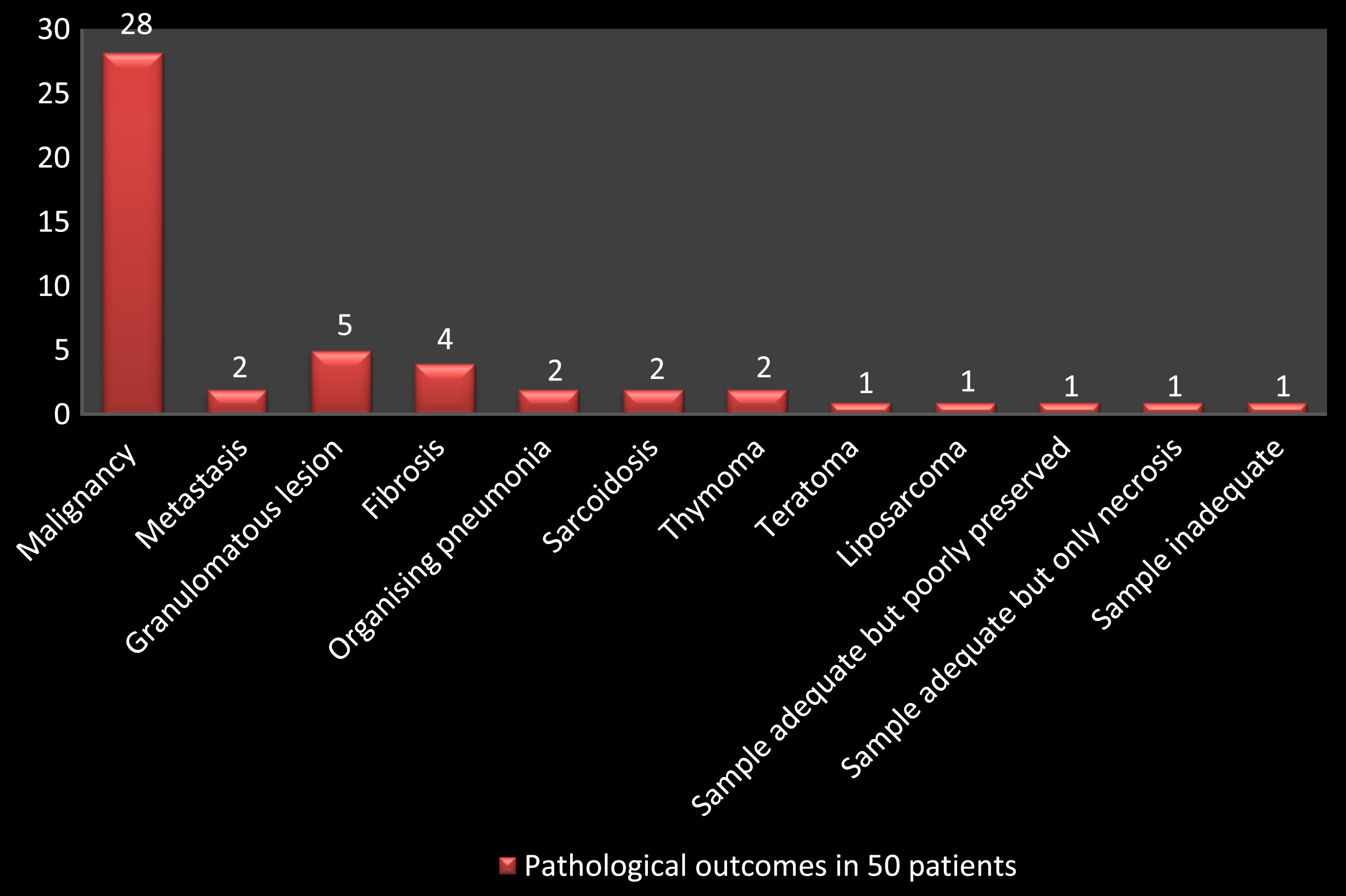
Mean procedure time was approximately 30.5±11.12 minutes. Sampling rate was 98%. However, tissue diagnosis was not obtained in 3 cases (6%). Results are summarised in Table 1.
Pathological outcomes in 50 patients
Pathological outcomes in 50 patients
Statistical significance was assumed at P < 0.05. All calculations were done with SPSS Statistics software (Version 22). Three size groups were formed with mean diameters of ≤15 mm, 16–30 mm and >30 mm each (Table 2). Each group was correlated with radiation exposure (DLP), complication rate, success rate and time of procedure. Using One way ANOVA test, the three mean diameter groups when compared to fluoroscopic DLP, total DLP and time of procedure, difference was found to be statistically insignificant (p > 0.05). Hence, even when the lesion size was small, time taken and radiation exposure remained the same. Comparing the three diameter groups with the complication and success rates using Fisher exact test, no significant difference was found. Hence, the chances of early pneumothorax and positive histopathological report did not correlate with mean lesion diameter in our study.
Patient distribution in three groups based on mean diameter of lesions
Pearson correlation test was used to measure the relationship of the mean depth of lesions (4.89±1.86 cm) with the fluoroscopic DLP (21.47±25.95 mGy-cm) and time of procedure (30.5 + 11.12 min) and the test were found to be significant (p value 0.003 and 0.001 respectively). (Table 3) Independent T test was used to correlate the depth of lesions with success and complication rates. There is significant correlation between the depth of lesions and chance of pneumothorax (p < 0.05), but not when depth was compared to biopsy success rates (p > 0.05) (as shown in Table 4).
The relation of depth of lesions with that of radiation dose during fluoroscopic biopsy and time of procedure
The relation of mean depth of lesions with the risk of pneumothorax and success rates
Based upon mAs and KVp settings during fluoroscopic guided biopsy, three groups were made (Table 5). The three groups were then compared with the exposure rates during biopsy procedure, success rates, complication rates and time of procedure. The difference was not found to be statistically significant when comparison was done with complication rate (Fisher Exact test-2.258, p > 0.05), success rates (Fisher Exact test-2.181, p > 0.05) and time of procedure (One way ANOVA test, p > 0.05). However, difference was statistically significant when comparison was done with DLP during the biopsy procedure (One way ANOVA test, p < 0.001) (Table 6). Hence, when mAs and KVp were kept minimum (30 and 70 respectively), radiation exposure during the biopsy procedure when both doctor and patient are inside the CT room, was significantly reduced, the background noise was increased but didn’t affect the biopsy technique, with comparable success rates, complication rates and time of procedure as comparable to high dose CT parameters (as shown in Figs. 1, 2 and 3).
Three groups divided based on the mAs and KVp settings during intermittent fluoroscopic biopsy
The relationship between fluoroscopic DLP values between different groups
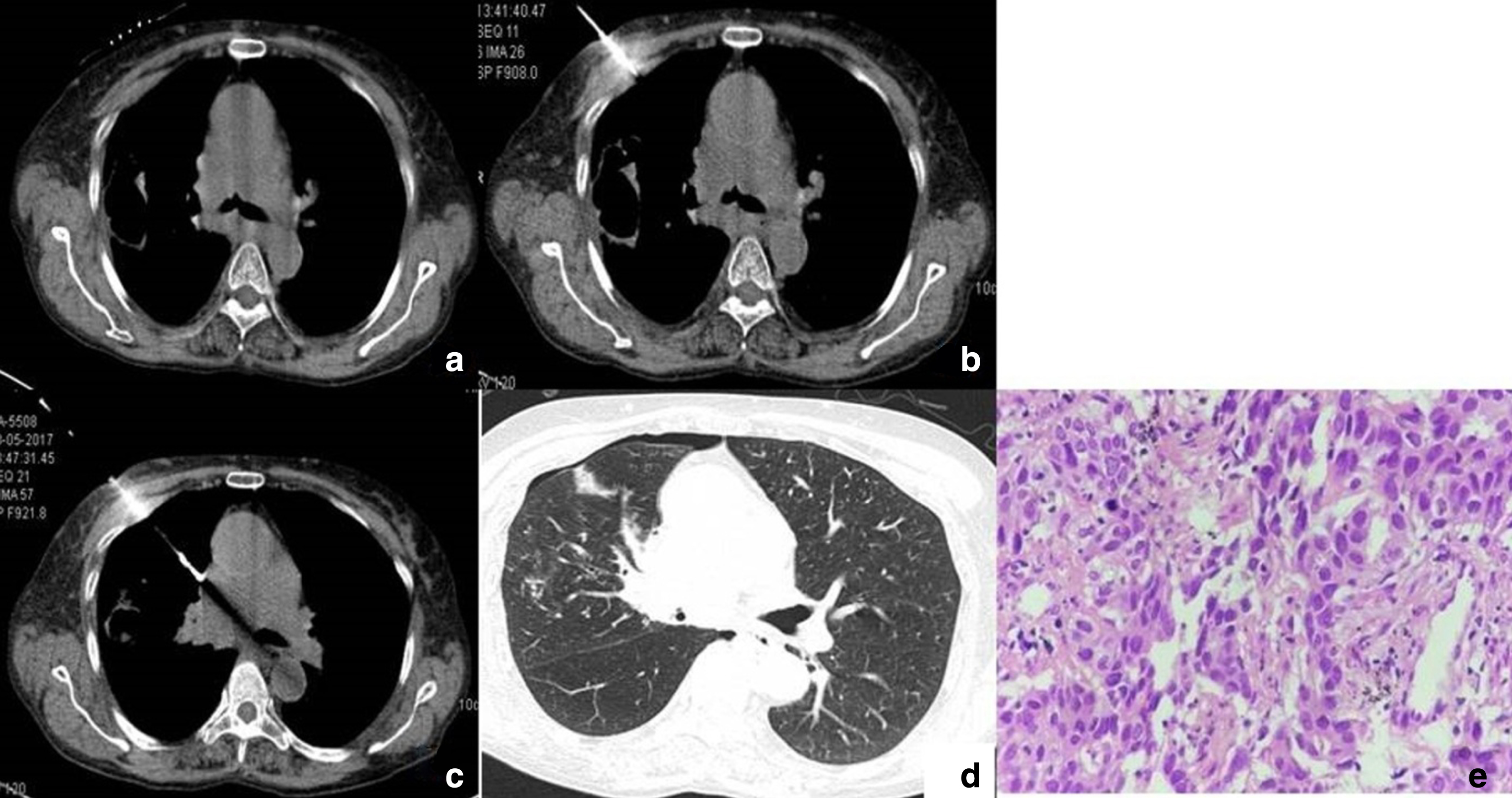
Squamous cell carcinoma: Biopsy done at 120 KVp and 30 mAs setting. 1(a) Needle marker placed on the skin. (b, c) Needle was advanced upto the surface of lesion at right lung hila. (d) Post procedure, thin strip of pneumothorax and needle tract haemorrhage was seen. Aspiration was not done. (e) Microphotograph (H & E; 400X) showing malignant squamous cells arranged in sheets and around blood vessels.
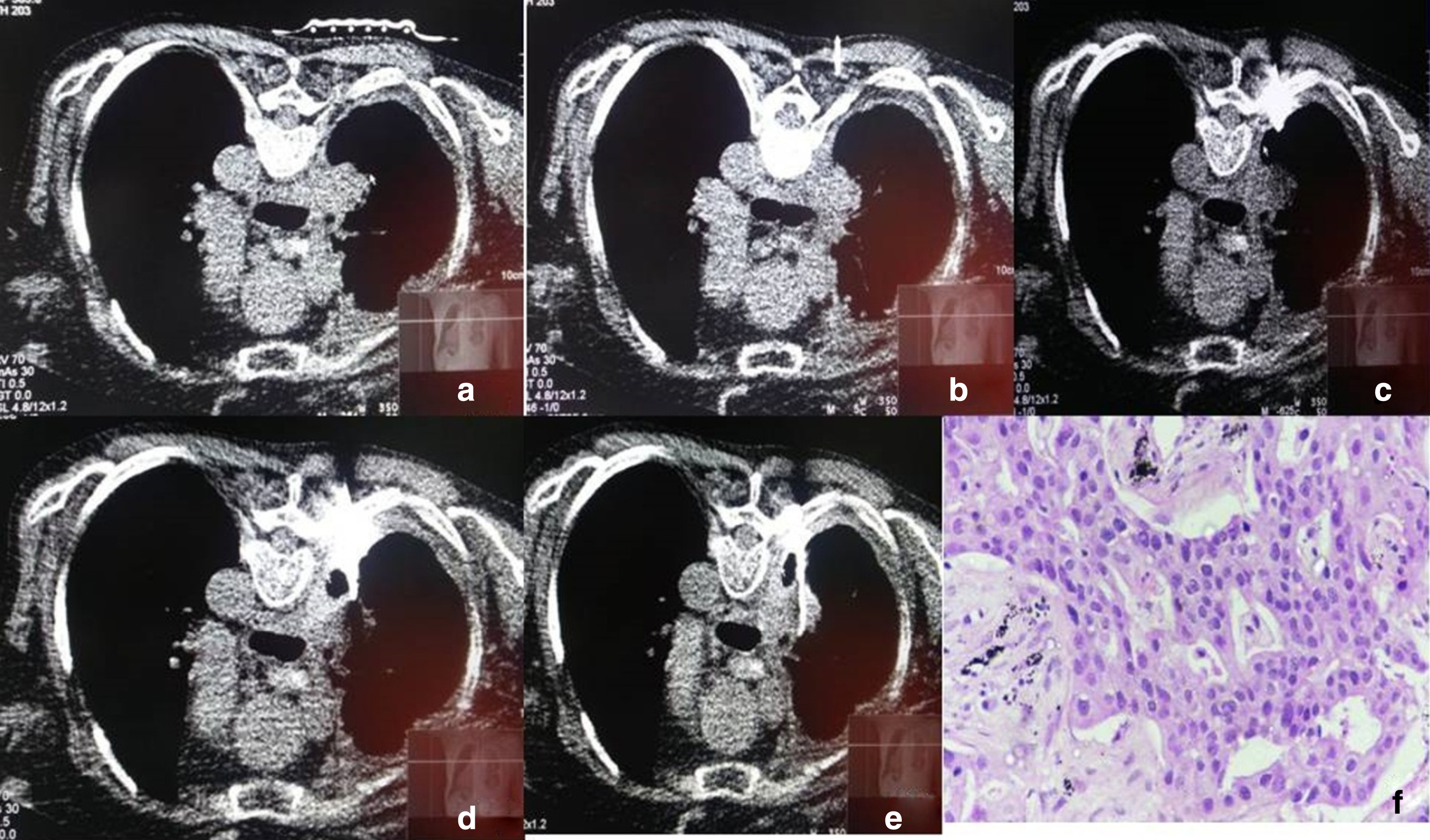
Adenocarcinoma: Biopsy was done at 70 KVp and 30 mAs setting. There is increase in background noise. 2(a) Needle marker was placed on the skin. (b, c, d) Needle was advanced upto the surface of lesion at right lung hila. (e) Sample core was taken with the help of semi-automated gun with 20 mm throw. (e) Microphotograph (H & E; 400X) showing malignant cells arranged in acinar pattern along with presence of carbon particles in background.
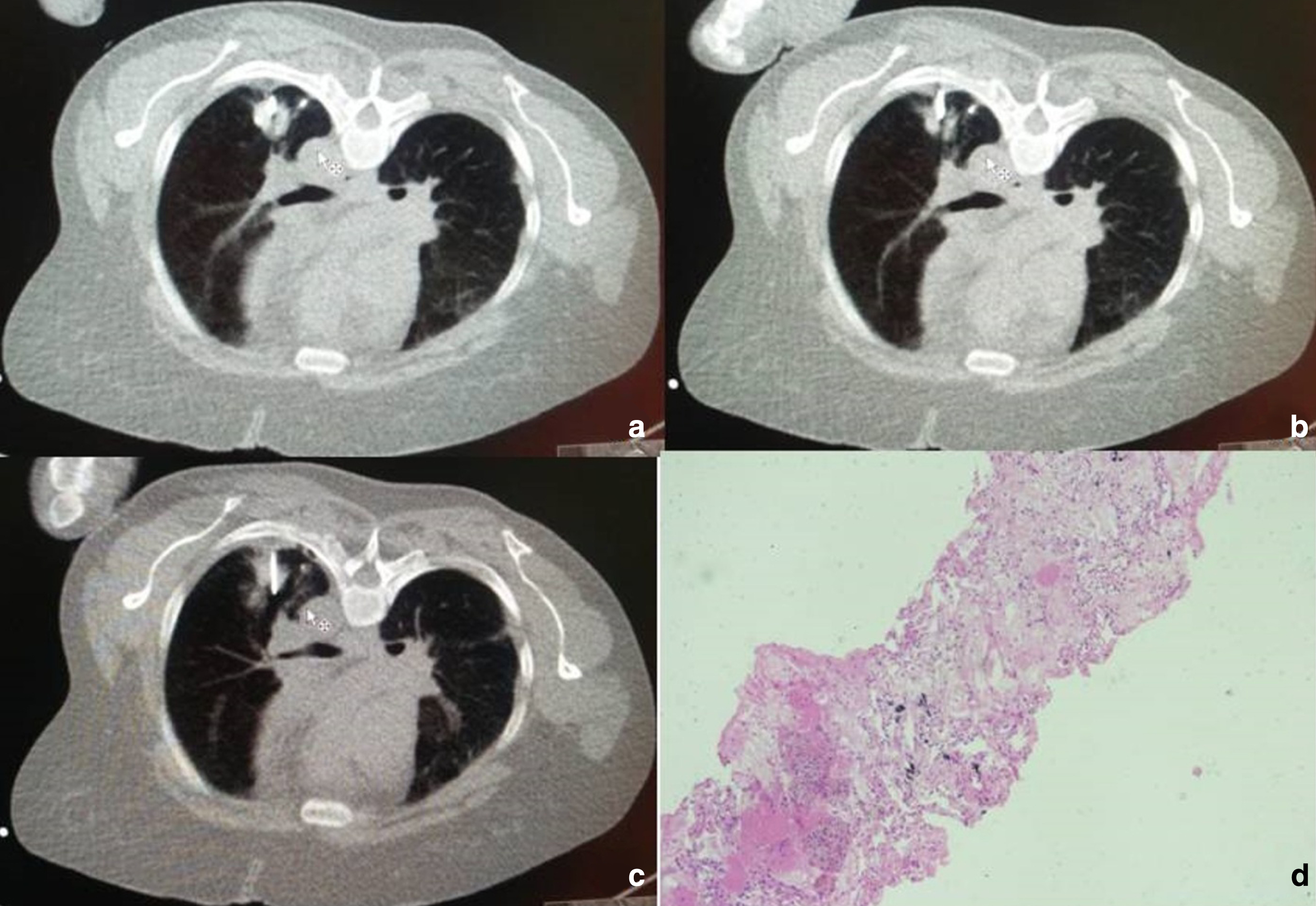
Fibrosis: Biopsy was done at 70 KVp and 30 mAs setting. No significant noise was seen as procedure was done in window setting between soft tissue and lung window. 3 (a, b, c) Multiple cores were taken from a small nodule in superior segment of right lower lobe. Minimal needle tract haemorrhage was seen. (d) Microphotograph (H & E; 100X) showing fibrocollagenous tissue admixed with mixed inflammatory cells and carbon particles.
Lung biopsy is the most important technique to retrieve samples for histopathological confirmation of lung nodules. Traditionally, it is being done by conventional CT guided biopsy procedure and it has been studied extensively. Under fluoroscopic guidance, either intermittent or continuous mode can be used for real time imaging and retrieval of tissue specimen [6]. In this study, we have made following observations in different aspects.
Radiation dose
Intermittent technique helps in reduction of effective dose because of limited scan range [7]. The factors that influence the radiation dose directly are x-ray beam energy (kilovolt peak), tube current (in mill amperes), rotation or exposure time, section thickness, object thickness, pitch, dose reduction techniques such as tube current modulation, and distance from the x-ray tube to isocenter [8]. The radiation dose is linear with the milliampere-seconds value when all other factors are held constant. However, this reduction will increase image noise by 1/√ (mAs). (Figs. 2 and 3) Reduction in beam energy results in reduced radiation dose when all other factors are held constant. However, radiation dose gradient decreases from periphery to centre at lower KVp settings. This leads to increased relative skin dose for patients at low KVp [8].
We performed lung biopsies using intermittent fluoroscopic technique by keeping different mAs and KVp settings (30 and 70, 10 and 120, 30 and 120 respectively). Hence, three groups were made based upon these parameters during the biopsy procedure. Mean DLP calculated during fluoroscopy biopsy was significantly reduced when 30 and 70 (mAs and KVp) setting was used compared to other groups keeping success rate, complication rate and duration of procedure more or less similar in three groups. Frisch et al compared the ultralow dose CT (80KVp and 20 mAs) with standard dose CT (120KVp with automatic mAs modulation) in performing lung biopsies using 256 slice scanner and concluded that complication rates were similar in both groups and there was significant reduction in the cumulative radiation dose, from 412 mGy-cm to 34 mGy-cm, with no reduction in the accuracy of needle placement [9]. Smith et al performed lung biopsies on 16 slice scanner and compared ultralow dose (100KVp, 7.5 mAs) with standard dose protocol. They described >95% reduction in radiation dose with similar complication and success rates in two groups [10]. Yoshikazu et al compared the different scan parameters with image quality and radiation dose using 4 detector row CT scanner. Acceptable image quality was achieved in 94% of patients with radiation dose of 1.18 mGy/sec when 120 kV, 10 mA parameters were used and in 100% of patients at 135 kV, 10 mA parameters, however radiation dose was greater than 1.48 mGy/sec. The authors didn’t recommend lung intervention below 80 KVp as it increased the skin dose [11].
In our study, mean calculated DLP during fluoroscopic biopsy was significantly lower measuring 7.32 mGy-cm (30mAs, 70KVp) as compared to 24.38 mGy-cm (10mAs, 120KVp) and 51.75 mGy-cm (30mAs, 120 KVp) in other groups. Multiplying with k factor of chest (0.014), gives radiation dose in milli seiverts (0.10, 0.34, 0.72 respectively). Hence modern day third generation dual energy CT scanner generates much less radiation even if KVp is reduced to below 80. However, a limitation of the study was that standard dose protocol was followed while taking topogram and plain CT sections before the start of biopsy procedure. Further reduction in radiation dose can be done if low dose protocol is followed in them as well.
Pneumothorax
Pneumothorax is the most common complication of CT guided lung biopsies. In the guidelines given by British thoracic society 2003, they adviced the cut off percentages of complications like pneumothorax (20.5% of biopsies), pneumothorax requiring a chest drain (3.1%), haemoptysis (5.3%), and death (0.15%) [12]. In this study, we observed that occurrence of pneumothorax did not correlate with the size of lesion (P 0.434) but it correlated well with the mean depth of lesions (p < 0.05). Pneumothorax occurred in 11 patients (22%) with mean depth of 6.2 cm, manual aspiration was done in 4 patients (8%) and chest tube insertion was done in 1 patient (2%), latter occurred due to small bulla adjacent to the lesion which was not seen prior to procedure but opened up after inserting needle into the lesion. Some studies suggest increased rate of pneumothorax when lesion size is <2 cm while other studies showed no such difference in complications whether lesion size is < />2 cm [13–16]. M Mills et al showed increased chances of pneumothorax with longer transparenchymal distance [14]. Khan et al proposed that an intrapulmonary needle path >4 cm is associated with increased chances of pneumothorax [16]. Increased depth from skin is an independent risk factor for pneumothorax when univariate analysis was done but not with multivariate analysis [13]. Other factors which increase the rate of pneumothorax is increased number of needle punctures, experience of radiologist, presence or absence of emphysema, needle size, history of previous surgery, location of lesion and position of patient [13, 17].
Success rate
When mean diameter and depth of lesion was correlated with success rates (positive histopathology report), no significant difference was found. Hence, success rates were similar for smaller and deeper lesions. Out of three lesions in which diagnosis was not made (6%), one lesion had adequate sampling but only necrosis was seen (mean diameter was 4.5 cm) and another lesion also had adequate sampling but poorly preserved (mean diameter was 2.2 cm). Yeow et al suggested lesions measuring >5 cm in size have decreased diagnostic accuracy due to presence of necrosis [18]. Decreased lesion size (<10–20 mm) are associated with decreased success rates [19]. Gelbman et al suggested reduced experience of radiologist, solitary nodule and occurrence of pneumothorax during the procedure can lead to false negative results [20]. A retrospective analysis done by Hiraki T et al evaluated diagnostic outcomes in 1000 pulmonary lesions under intermittent CT fluoroscopy technique using 20 G coaxiale cutting needle suggested lesion ≤1 cm and ≥3 cm lead to higher failure rates [21]. However, in our study only 5 (10%) lesions were ≤15 mm in diameter, all of them showed positive sampling and histopathological diagnosis.
Time of procedure
In our study, depth of lesion from skin surface correlated well with duration of procedure (P 0.001). But no significant association was noted when size was correlated with time of procedure (p > 0.05). Mean time of procedure was approximately 30.5±11.12 minutes (which included the time, patient was on CT table as well as the management of pneumothorax).
The mean time required for each biopsy procedure under real time fluoroscopy in 138 nodules was 25.6±10.1 minutes [22]. Compared to conventional CT guided procedures, fluoroscopic technique helps in rapid completion of procedure, reduced number of punctures and hence reduced chances of complications [23]. When procedure time was compared in two groups (continuous fluoroscopy and conventional CT guided) methods, there was increase in success rates and reduced mean procedure times (27.56 min) in continuous CT fluoroscopic group [24]. We didn’t do real time tracking but during intermittent fluoroscopic technique, as there was no need to move into or out of the room plus every time, three images were acquired by pressing the foot plate, it saved time and we did not feel the need of real time tracking.
Limitation
This study also has a number of limitations. First, we did not have a control group with which we could compare intermittent fluoroscopic technique with conventional CT guided lung biopsies. Second, while calculating radiation dose, separate skin dose was not calculated. Third, we did not do the follow up of patients and considered positive histopathological report as diagnostic success rate in our study. Fourth, while studying the depth of lesions, we did not take the depth of lesions from pleura but took it from skin surface. Last, our sample size was also quite small for lesions with mean diameter <15 mm. Hence, correlating this group with radiation dose, success and complication rates needs further validation from future study with a larger and more diverse dataset.
Conclusion
This study demonstrated when using the third generation dual energy source CT scanner, reducing radiation dose to 30mAs and 70KVp during fluoroscopy biopsy can produce images whose complications and success rates are comparable to using high dose CT. Increase in depth of lesions increase the DLP during fluoroscopic biopsy, time of procedure and complication rates. Size of the lesions does not directly correlate with radiation dose, time of procedure, success and complication rates in our study. In summary, intermittent CT fluoroscopy guided lung biopsy has good success rates with acceptable complications, while utilising less radiation dose and procedure time.