
Abstract
PURPOSE:
To investigate associations between the clinicopathologic features and CT perfusion parameters of triple-negative breast cancer (TNBC) and non-TNBC using low-dose computed tomography perfusion imaging (LDCTPI), and to find potential clinical applications in the prognosis assessment of TNBC.
MATERIALS AND METHODS:
A total of 60 patients with breast cancer confirmed by pathological examination were studied prospectively using LDCTPI on a 64-slice spiral CT scanner. The acquired volume data were used for calculations, mapping, and analysis by using a tumor perfusion protocol in the CT perfusion software package to measure 2 parameters namely, blood flow (BF), and permeability surface (PS) area product. Patients were grouped into TNBC (n = 27) and non-TNBC (n = 33) subtypes. Associations between these two subtypes and clinicopathologic characteristics were evaluated by both univariate and multivariate logistic regression. CT perfusion parameters values were compared for clinicopathologic characteristics using independent 2-sample t test.
RESULTS:
TNBC displayed higher CT perfusion parameters values (BF: 57.56±10.94 vs 52.70±7.79 mL/100 g/min, p = 0.006; PS: 38.98±9.46 vs 33.39±8.07 mL/100 g/min, p = 0.001) than non-TNBC. In addition, breast cancer with poorly histologic grade or positive Ki-67 expression showed higher BF and PS values than those with well and moderately histologic grade or negative Ki-67 expression (p < 0.05). TNBC had poorer histologic grade (P = 0.032) and higher Ki-67 expression (P = 0.013) than non-TNBC.
CONCLUSION:
LDCTPI is a functional imaging technology from the perspective of hemodynamics with potential of clinical applications. The BF and PS values were higher in TNBC patient group than non-TNBC group. TNBC patients also have poorer clinicopathologic outcome.
Keywords
Introduction
Breast cancer (BC) is the most common female cancer and represents the leading cause of cancer death in women aged 20–59 years [1]. At present, breast cancer is recognized as a group of highly heterogeneous diseases and is further categorized into two major subtypes based on immunohistochemical expression of receptors, namely triple-negative breast cancer (TNBC)[estrogen receptor (ER) negative, progesterone receptor (PR) negative, and human epidermal growth factor receptor 2 (HER2) negative], and non-TNBC (ER or PR or HER2 positive) [2]. Because of this mixed spectrum of gene expression, each subtype displays different clinical behaviors, responses to treatment, and prognosis [3]. In particular, triple-negative breast cancer (TNBC) lacks expression of all three receptors (ER, PR, and HER2) and is known to have a more aggressive clinical course and poorer outcomes [4–6]. Accordingly, early distinction of TNBC from other subtypes with a non-invasive imaging modality (LDCTPI) would allow clinicians to establish ideal treatment management before final pathologic confirmation [7].
Previous studies have described MRI features of TNBC as a intra-tumoral heterogeneity on dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) and higher apparent diffusion coefficient (ADC) on diffusion-weighted image (DWI) [8, 9]. However, these studies only measured ADC values from a single slice of ADC maps, which could have resulted in observer bias and insufficient information regarding heterogeneity of the tumor. At the same time MRI has some other weaknesses, such as the high cost, complexity of interpretation, lengthy inspection times, and contraindications (claustrophobia, implanted devices, or renal insufficiency), and these issues limit its use in breast screening. In order to overcome such limitations, we adopted a hemodynamics analysis of the breast tumor by CT perfusion imaging. A similar study by Miho et al. [10] demonstrated that MRI perfusion parameters correlated with prognostic factors and subtypes of invasive ductal carcinoma (IDC) of the breast.
CTPI is a novel functional examination technology that was developed recently. In 1991, Miles et al. [11] first proposed the concept of CT perfusion imaging (CTPI). Currently, CTPI is widely used in research of the head [12], lung [13], liver [14], stomach [15], and other organs. However, CTPI produces large amounts of radiation, so we apply low dose (namely low tuber current of 50–80 mA and tube voltage of 80–100 kV) CT perfusion scans method to give rise to less radiation than regular CT perfusion imaging scans (tuber current of 200 mA and tube voltage of 120 kV). The research on LDCTPI of breast cancer is still in the exploratory stage and few studies have been published [16]. This study aimed to investigate associations between TNBC and non-TNBC with regard to clinicopathologic features and CT perfusion parameters.
Materials and methods
Patients
Ethical approval: all procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee. Informed consent was obtained from all individual participants included in the study. Inclusion criterion: (1) The result of each patient should be pathologically confirmed as breast ductal carcinoma; (2) CT perfusion images of each patient should be clear, and the breast tumor should be displayed well. Exclusion criterion: (1) Subjects were allergic to contrast agent; and (2) the artifacts of CT perfusion images were enough serious to limit the quality of images. A total of 60 consecutive patients with BC confirmed by means of puncture biopsy were prospectively recruited, including 27 TNBC with an age range of 26–74 years old (mean age, 54.35 years old), and 33 non-TNBC with an age range of 29–79 years old (mean age, 55.52 years old). The histologic size of 60 tumors ranged from 1.6–6.7 cm (mean tumor size, 3.21±1.30 cm). The mean sizes of TNBC and non-TNBC subtype were 3.07±1.16 cm and 3.29±1.37 cm, respectively. Well or moderate histologic grade was found in 32 (53.33%) patients, and poor histologic grade was found in 28(46.67%). In addition, 34 (56.67%) patients had negative axillary nodal status, and 26 (43.33%) patients had positive axillary nodal status. Of the total, 31(51.67%) patients displayed positive Ki-67 expression, while 29(48.37%) displayed negative Ki-67 expression.
All patients were performed preoperative breast CT perfusion and post-operative pathology examination. Pathologic types of 60 breast cancer patients consisting of 27 TNBC and 33 non-TNBC subtypes were all ductal carcinoma. In 33 non-TNBC subtypes, 8 cases were ER positive, 5 cases were PR positive, 5 cases were HER2 positive, and 15 cases were more than one positive.
Perfusion CT study protocol
First, All breasts were conventionally plain-scanned on a 64-slice spiral CT scanner (Siemens Sensation 64, Germany) with the following parameters: a slice thickness and spacing of 5 mm, tube voltage of 80–100 kV, tuber current of 50–80 mA, a matrix of 512×512 pixels, and pitch of 0.984:1. Then, based on the plain CT image, LDCTPI was performed, the slice containing the largest breast tumor area was selected as the center slice, and a total of 6 nearby slices including the center slice were selected every 3 cm on the Z-axis. These slices were scanned with a small field of view (SFOV) at a 5 mm slice thickness. 50 mL bolus of iopamidol (Iopamiro; Bracco; Shanghai, China) containing 300 mg of iodine per mL was injected using a power injector (MEORAO-Stellant, MEO-RAO Company, Germany) via an antecubital vein at a rate of 5 mL/s through an 18-gauge intravenous cannula. Scanning commenced 5 s after contrast agent injection and the scan duration was 30 s. Participants were instructed in breathing exercises to hold breath during the LDCTPI examination.
Image interpretation
Data from the dynamic perfusion scan were transmitted to a advantage workstation (ADW 4.0, Siemens company) system. A tumor perfusion protocol in the body CT perfusion 3.0 software (deconvolution method) was then used for data processing. The chest aorta was selected as the input artery and pseudo-color (pcolor) perfusion images including BF and PS images were obtained through workstation processing. The red or yellow sections in the pseudo-color images denoted high blood perfusion. On the contrary, the blue or purple sections in the pseudo-color images denoted low blood perfusion. The region of interest (ROI) which should avoid the necrotic area of the target lesions was drawn on the breast tumor. The corresponding blood flow (BF) and permeability surface (PS) were measured. Measurements of all perfusion parameters were repeated 3 times by a radiologist who engaged in breast imaging, and the averages of the 3 measurements were shown.
Clinicopathologic data analysis
The clinician who didn’t participate in image analysis collected clinical and histopathologic data and pathological reports, including patient age, tumor type, size, histological grade, Ki-67 index, presence of axillary lymph node metastasis. Tumor size was measured as the maximum diameter of the surgically resected specimen.
On the basis of receptor expression status, tumors were grouped as TNBC or non-TNBC subtype. Histopathological assessment was completed by a pathologist with 15 years of experience. ER and PR positivity were defined as more than 1% staining of nuclei in cancer cells on an entire stained slide. The intensity of HER2 expression was semi-quantitatively scored as 0, 1+, 2+, or 3+, such that 3+ score was classified as HER2 positive, and 0, 1+ or 2+ score was considered HER2 negative.We defined Ki-67 index >20% as positive expression.
Statistical analysis
The data were expressed as mean±standard deviation (mean±SD) or frequency (percentage, %). Then, statistical software (SPSS, version 17.0) was applied for the statistical analysis. The reference range includes 95% confidence intervals (95% CI). A total of 60 TNBC or non-TNBC patients with preoperative CT perfusion parameters were divided into two groups according to histologic grade (well or moderate vs. poor), axillary nodal status (negative vs. positive), Ki-67 index (negative vs. positive). Associations between the two subtypes (TNBC vs. non-TNBC) for clinic-pathologic characteristics were evaluated by both univariate and multivariate logistic regression. CT perfusion parameters values were compared for pathologic characteristics using independent 2-sample t test. Differences were considered to be statistically significant at p < 0.05.
Results
In 60 cases, all CT perfusion series were usable for the analysis because breast tumor was recognizable in each patient, and no significant respiration artifacts were detected. LDCTPI produced radiation of 2 mSv. The radiologist made 3 measurements in each case and the average number was used. The range of BF value of 60 cases was 46.18–67.69 mL/100 g/min, the range of PS value of 60 cases was 25.85–51.33 mL/100 g/min. There were no statistically significant difference among 3 measurements in BF and PS values (p > 0.05).
Associations of clinicopathologic features between two subtypes
Table 1 showed the results of univariate and multivariate logistic regression analyses comparing the clinicopathologic features associated with TNBC and non-TNBC subtypes. Histologic grade and Ki-67 value were significant factors in both univariate and multivariate analyses. Poorer histologic grade of tumor was significantly associated with TNBC subtype (74.07% (20/27) in TNBC vs. 24.24% (8/33) in non-TNBC, p = 0.032). Higher Ki-67 was significantly associated with TNBC subtype (Ki-67 > 20% in 88.89% (24/27) of TNBC vs. 21.21% (7/33) of non-TNBC, p = 0.013). No significant difference was found in axillary nodal status or lesion size or age between the two subtypes.
Clinicopathologic associations between TNBC and non-TNBC subtypes (N (%) or mean±SD)
Clinicopathologic associations between TNBC and non-TNBC subtypes (N (%) or mean±SD)
Values are number (percentage) for categorical variables and mean±SD for numerical variables. TNBC: Triple-negative breast cancers, OR: odds ratio, CI: confidence interval. Associations between the two subtypes for clinicopathologic characteristics were evaluated by both univariate and multivariate logistic regression.
Table 2 showed the results of independent 2-sample t test comparing CT perfusion parameters BF and PS values for pathologic features. Higher BF and PS values were significantly associated with TNBC subtype, poor histologic grade, positive Ki-67 expression (p < 0.05, respectively); but There were no significant differences in BF and PS values between positive axillary nodal group and negative group (p > 0.05, respectively). Figure 1 presented that the tumor area was shown in yellow in the BF and PS images of a patient with non-TNBC, Fig. 2 presented that the tumor area was shown in yellow in the BF image and in red in the PS image of a patient with TNBC, demonstrating that there was a higher blood flow perfusion in TNBC than non-TNBC.
Comparisons of CT perfusion parameters for pathologic characteristics in 60 breast cancers (mean±SD)
Comparisons of CT perfusion parameters for pathologic characteristics in 60 breast cancers (mean±SD)
BF: blood flow, PS: permeability surface, TNBC: Triple-negative breast cancers. CT perfusion parameters values were compared for pathologic characteristics using independent 2-sample t test.
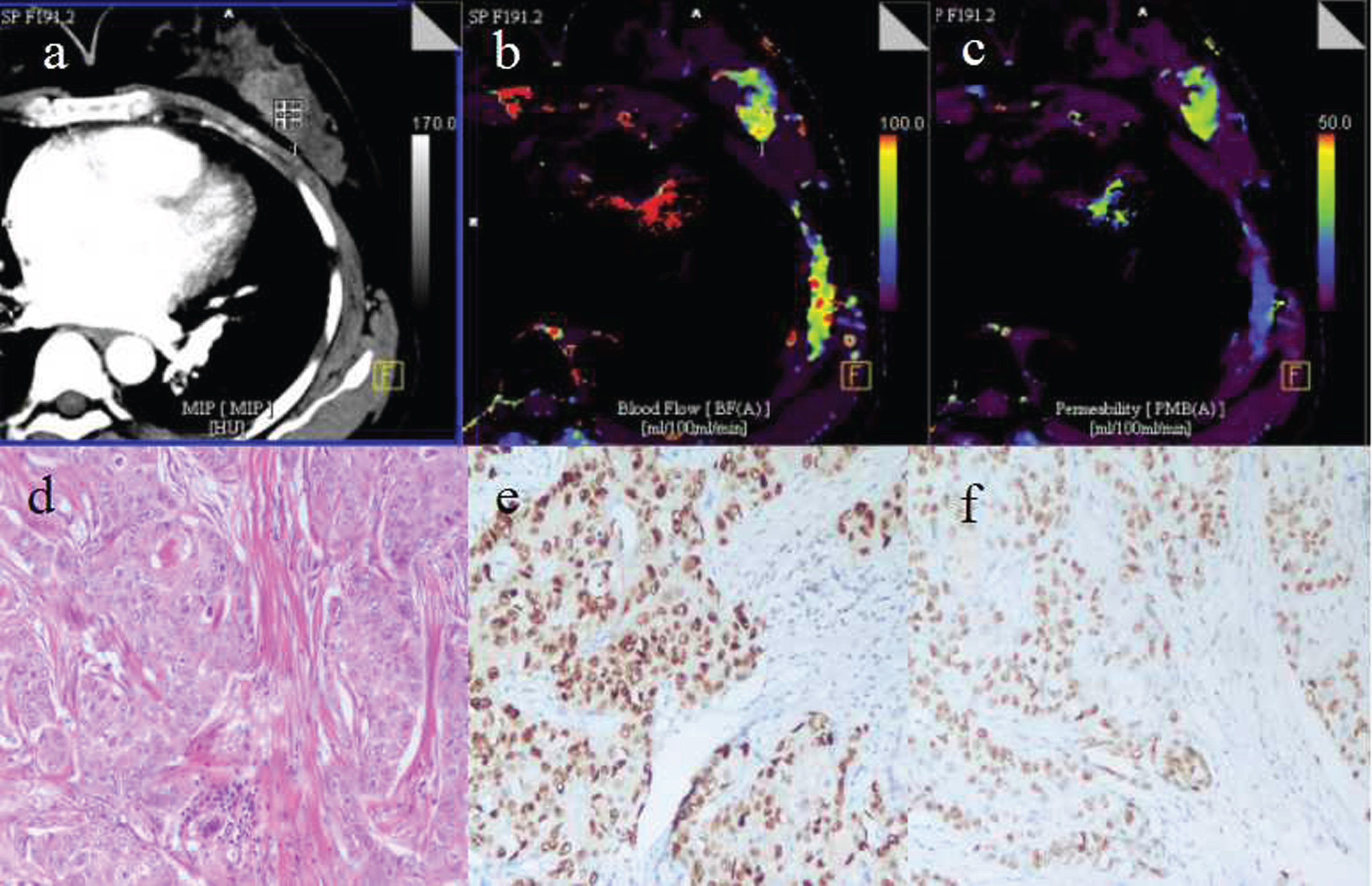
A 45-year-old woman with non-TNBC in the left breast. a: An original CT image showed a irregular mass with obvious enhancement (ROI), the diameter of the mass was about 4 cm. b–c: CT perfusion pcolor images for BF and PS, respectively. In the BF and PS images, the tumor area was shown in yellow, demonstrating that there was a higher blood flow perfusion in the mass area. d: A pathological image (HE staining,100×) showed the moderately differentiated cancer cells with a certain degree of pleomorphism and cord-like or small nest-like arrangement. e: Strong nuclear positivity was shown in brown for ER immunostaining. f: Strong nuclear positivity was shown in brown for PR immunostaining. BF: blood flow, PS: permeability surface, TNBC: triple-negative breast cancers, HE: hematoxylin eosin, ER: estrogen, PR: progesterone receptor.
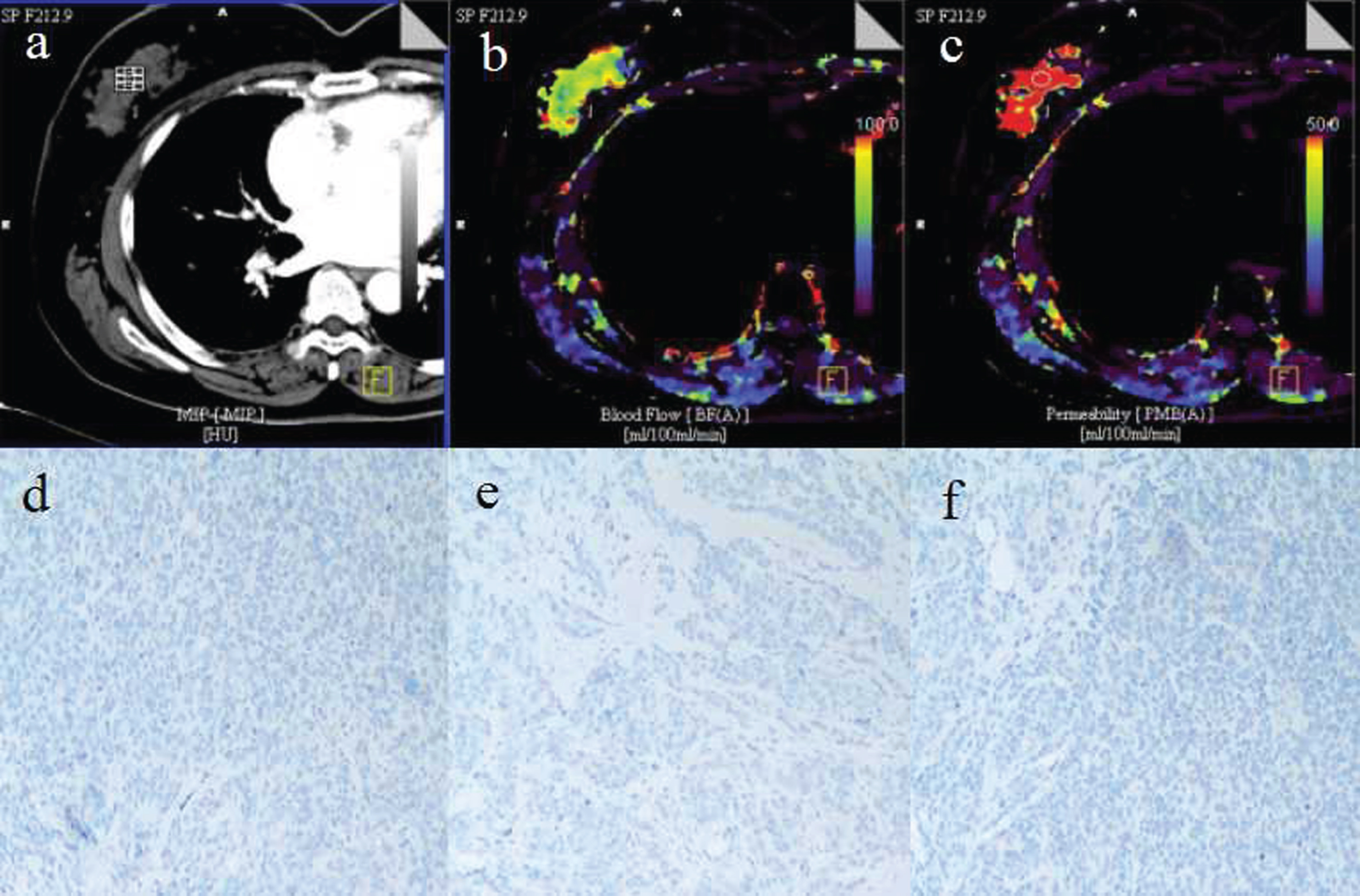
A 70-year-old woman with TNBC in the right breast. a: An original CT image showed a irregular mass with obvious enhancement (ROI), the diameter of the mass was about 6 cm. b–c: CT perfusion pcolor images for BF and PS, respectively. In the BF image, the tumor area was shown in yellow; in the PS image, the tumor area was shown in red, demonstrating that there was a very high blood flow perfusion in the mass area. d: A pathological image showed negative immunostaining in blue for ER. e: Negative PR immunostaining. f: Negative HER2 immunostaining. BF: blood flow, PS: permeability surface, TNBC: triple-negative breast cancers, ER: estrogen, PR: progesterone receptor, HER2: human epidermal growth factor receptor 2.
Triple-negative breast cancers (TNBC) account for less than 20% of all breast cancers, but treatment is limited by the lack of effective targeted therapies and by their aggressive clinical behavior, which is typically characterized by earlier relapses and worse outcomes [3]. The clinical characteristics of the TNBC population in this study are similar to those previously reported, which are higher Ki67 counts and poorer histologic grade of tumor in comparison to non-TNBC subtype. In this study, poorer histologic grade and higher Ki-67 expression of breast cancer were both significantly associated with TNBC subtype. This finding was consistent with a previous study by Urru et al. [17], which found that a higher pathologic grade of TNBC, and two other studies [18, 19] showing higher Ki-67 expression as an independent predictor of TNBC.TNBC was known to manifest as larger lesions than other subtypes [20], but we saw no significant size difference between TNBC and non-TNBC subtypes in this study.
MRI features of TNBC have been studied widely [21, 22] as early non-invasive detection prior to treatment. However, CT perfusion features of TNBC have been studied very little. This study addressed CT perfusion features of TNBC and compared them to those of non-TNBC subtype. These findings displayed higher BF and PS values were significantly associated with TNBC subtype, poor histologic grade, positive Ki-67 expression (p < 0.05, respectively). This finding was consistent with a previous study by Li et al. [23], which found that TNBC possess characteristic features on MRI imaging, with higher blood flow (BF) and higher contrast agent wash-out rate (higher vascular permeability, namely PS).On the contrary, the previous study by Young-Sil An et al. [24] found that lower Ktrans and lower Ve were significantly associated TNBC, and TNBC showed higher metabolic-perfusion ratios compared to non-TNBC. However any conditions influencing blood perfusion including patient factors such as cardiac output and hypertension may potentially confound measurements of perfusion parameters.
We found there were no statistically significant difference between regular dose CTPI and LDCTPI used in this study in distinguishing between TNBC and non-TNBC, but regular dose CTPI produced large amounts of radiation (about 6 mSv) which had an effect on human health, while LDCTPI produced radiation of 2 mSv. We recognized that although multiple statistical comparisons were performed in this analysis, and this was an exploratory study designed to be hypothesis generating. However further validation in a larger patient population was warranted. To our knowledge, findings using fully quantitative methods of LDCTPI have not been widely reported in the literature.
CT perfusion imaging (CTPI) offers valuable imaging parameters, since it is non-invasive, and is quantitative and repeatable. The serious problem is large amounts of radiation and low resolution produced by CTPI. So we perform low-dose CTPI scanning with low tuber current of 50–80 mA and tube voltage of 80–100kv combined with small field of view (SFOV), in order to produce little radiation and high spatial resolution. Sun et al. [25] reported the application of low-dose CTPI in gastric cancer with tuber current of 50 mA, and thought that the parameters BF and BV values may play a valuable role in the diagnosis and assessment of gastric cancer. BF reflected microvascular density (MVD) of tumors, which was considered to reflect the angiogenic activity generated by tumor cells and supportive stroma. PS was the unidirectional transfer rate of contrast agent from the endothelium of the capillaries into the intercellular space, which reflected wall permeability, integrity, and other characteristics of vascular endothelial cells within tumor tissue. Miho et al. [10] investigated the feasibility of perfusion imaging using an arterial spin labeling (ASL) technique for breast cancer, which was appropriate for cerebral brain perfusion; however a limitation of their breast ASL perfusion study was some artifacts, and their study thought that tumor lesions that often show high perfusion rates can be detected in the normal breast tissues. Results from Boruah et al. [26] showed that all microvessel parameters had a positive correlation with breast tumor grades, the mean of the microvessel parameters were the least for the benign and the largest for the grade 3 tumors of breast cancer.
Our study had several limitations. Firstly, small tumors less than 1 cm were excluded due to limited quality of reconstructed image from CTPI and difficulty in manual selection of region of interest (ROI). Secondly, the artifact due to respiration was minimized but not avoided, which may limit the quality of images and interfere with the results. Thirdly, the radiation due to CTPI was minimized but not avoided, which may limit the promotion and application of CTPI in the breast. But these problems may be resolved when the speed of CT scanning was very fast with advanced CT machines.
In conclusion, TNBC displayed poorer clinicopathologic outcomes than non-TNBC. LDCTPI analysis showed perfusion parameters BF and PS were higher in TNBC than non-TNBC subtype, indicating that they may be a useful index for differentiating TNBC from other breast cancer subtypes.
Footnotes
Acknowledgments
We would like to acknowledge Professor Hu chunhong for his technical help. Zong-Qiong Sun has received research grants from the science foundation of Wuxi Health and Family Planning Commission in China (MS201643).