
Abstract
PURPOSE:
To explore the radiomics features of triple negative breast cancer (TNBC) and non-triple negative breast cancer (non-TNBC) based on X-ray mammography, and to differentiate the two groups of cases.
MATERIALS AND METHODS:
Preoperative mammograms of 120 patients with breast ductal carcinoma confirmed by surgical pathology were retrospectively analyzed, which include 30 TNBC and 90 non-TNBC patients. The manual segmentation of breast lesions was performed by ITK-SNAP software and 12 radiomics features were extracted by Omni-Kinetics software. The differences of these radiomics features between TNBC and non-TNBC groups were compared, and the receiver operating characteristic (ROC) curve was used to determine the optimal cutoff value of each radiomics parameter for differentiating TNBC from non-TNBC, and the corresponding area under the curve (AUC), sensitivity and specificity were obtained.
RESULTS:
There were statistically significant differences for 4 radiomics features between TNBC and non-TNBC datasets (P < 0.05). They were the roundness, concavity, gray average and skewness of breast lesions. Compared with non-TNBC, TNBC cases have following characteristics of (1) more round with the roundness of 0.621 vs. 0.413 (P < 0.001), (2) more regular with the concavity of 0.087 vs. 0.141 (P < 0.01), (3) higher density or gray average (67.261 vs. 56.842, P < 0.05), and (4) lower skewness (– 0.837 vs.– 0.671, P = 0.034). AUCs of ROC curves computed using features of the roundness and concavity were both larger than 0.70.
CONCLUSION:
Radiomics features based on X-ray mammography may be helpful to distinguish between TNBC and non-TNBC, which were associated with breast tumor histology.
Keywords
Introduction
Triple negative breast cancer (TNBC) accounts for 10% – 20% of breast cancer [1], and its biological characteristics are different from other breast cancers, which has stronger invasiveness, higher recurrence and metastasis rate, and lower survival rate of patient [2–4]. At present, immunohistochemistry methods are mainly used to judge molecular type of breast cancer, which require biopsy or surgery to obtain and analyze part of tumor tissue. However, as the spatial and temporal heterogeneity of breast tumor, this part of tumor tissue does not represent the complete features of tumor. Some scholars [5] have analyzed the X-ray features of TNBC and non-triple negative breast cancer (non-TNBC), and find that there are differences in size and morphology, indicating that mammography can distinguish between TNBC and non-TNBC, and provide valuable reference information, however this only visually indicates X-ray features of breast cancer, and the interior features of tumors cannot be detected.
Advancements in medical imaging technology and analytical methods have led to the development of radiomics -a field of study dedicated to transforming these medical images into high-dimensional, mineable data that can be used to objectively and quantitatively profile tumor phenotypes in a robust and reproducible manner [6–8]. Radiomics hypothesizes that these models hide important biological and medical data that can provide additional information for diagnosis, prognosis, and other forms of prediction in clinical practice [9, 10]. For example, Park et al. [11] demonstrated that a radiomics panel could be preoperatively, noninvasively used to predict meningioma grade. Another study reported associations between radiomics features and postoperative survival in patients with solitary hepatocellular carcinoma (HCC) patients [12].
Recently, few studies had focused on the application of radiomics in patients with breast cancer. Ma et al. [13] investigated the association between mammographic radiomic features and molecular subtypes of breast cancer, which showed that quantitative radiomic imaging features of breast tumor extracted from digital mammograms were associated with breast cancer subtypes. Moreover, Liang et al. [14] explored the application of MRI radiomics for preoperative prediction of Ki-67 status in breast cancer. However, these studies didn’t mention radiomic imaging features of TNBC, and TNBC was a very different tumor from other breast lesions. Thus, the reliability and validity of radiomics biomarkers for TNBC required further investigation. In this study, we aimed to differentiate TNBC from non-TNBC by using a radiomics method to explore the objective and quantitative radiomics parameters features of TNBC.
Materials and methods
Patients
The present study was approved by the Institutional Review Board of my hospital and waived the requirement for informed consent due to the retrospective nature of the study. In total, 120 consecutive patients with breast cancer who had undergone preoperative X-ray mammography and had been confirmed by postoperative pathology as invasive duct carcinoma between May 2015 and October 2018 were enrolled in this study. The inclusion criteria were as follows: (a) confirmed by pathology as invasive ductal carcinoma of the breast; (b) sufficient quality of X-ray image; (c) complete medical record. The exclusion criteria were as follows: (a) received preoperative therapy; (b) less than the minimun diameter of 5 mm not to manually draw region of interest (ROI) along the margin of the tumor on the X-ray image. There were all 120 female patients with an age range of 36–75 years old (mean age, 53.1 years old), including 30 patients with TNBC with a diameter range of 0.8–5.4 cm (mean 2.7 cm) and an age range of 36–72 years old (mean 52.8 years), and 90 patients with non-TNBC with a diameter range of 0.7–6.1 cm (mean 2.9 cm) and an age range of 39–75 years old (mean 53.5 years). X-ray mammography data were obtained from the picture archiving and communications system (PACS) of our institution.
Image acquisition of mammography
The Selenia Dimensions digital mammography machine (Hologic, USA) and post-processing workstation were used to obtain the mammary craniocaudal (CC) and mediolateral obique (MLO) X-ray images through selecting Auto-Filter exposure mode.
Image interpretation
Segmentation of region of interest (ROI)
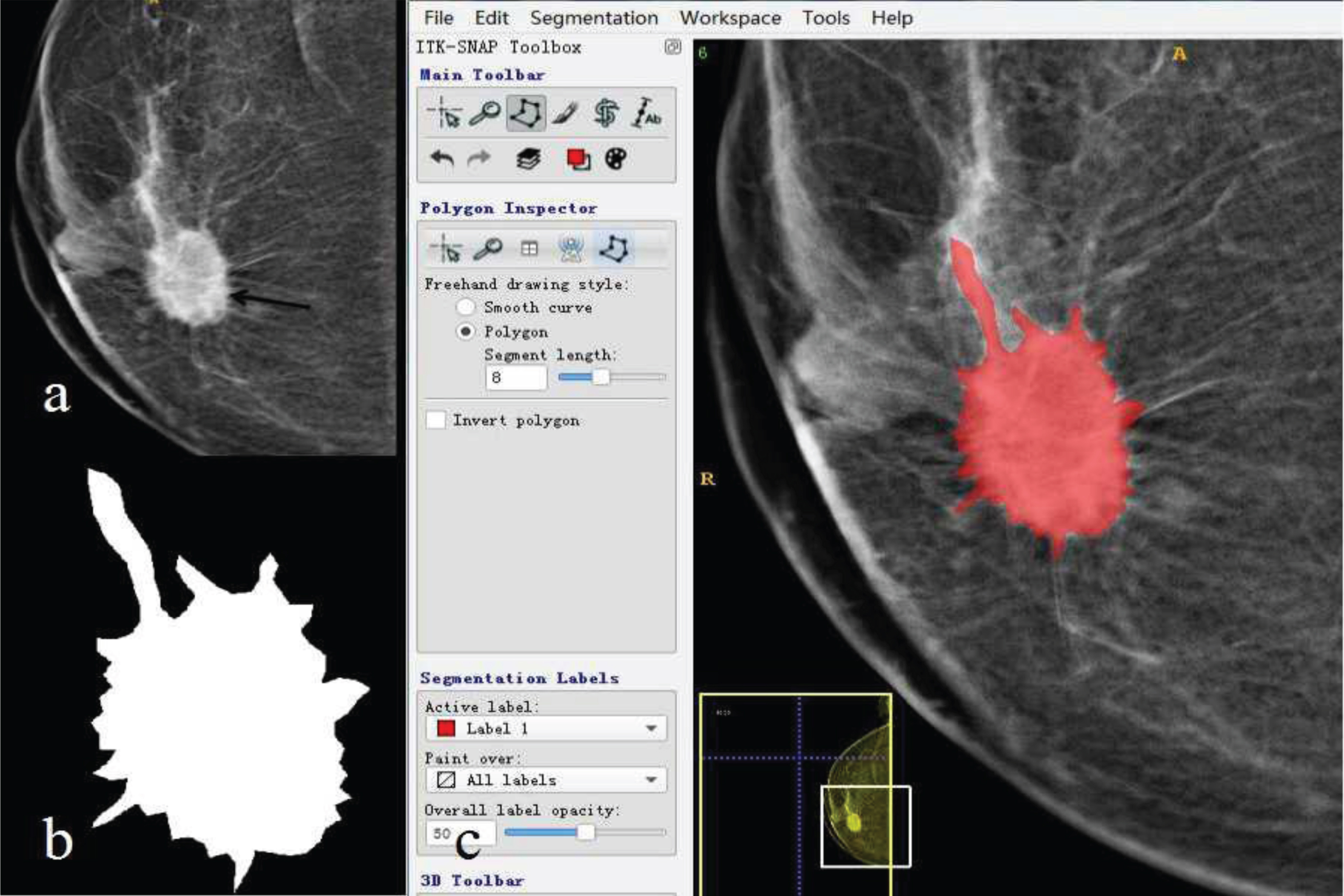
The X-ray images with the slice of the maximum diameter breast lesion were exported into ITK-SNAP software (version 2.4, USA), and tumor target regions were manually divided by a senior imaging physician along the margin of the tumor. The segmentation process were as follows: (1) introduced the breast tumor images with DICOM format into the home page by “Data” key; (2) selected “Editor” tool, and click “Apply” to the current image in “Modules” drop-down menu; (3) selected brush in the tool column from the “Draw Effect” to manually delineate region of interest (ROI) along the tumor edge; (4) clicked “File-save” to save the segmentation images into the destination folder in “img/hdr” format.
Extraction of radiomics features
The radiomics features of the segmentation images were extracted by the Omni-Kinetics software (General Electric, USA). There were 12 radiomics features parameters, including 3 morphological features, 4 gray statistical features and 5 texture features. Morphological features included the area, roundness, and concavity. The statistical feature of gray was the statistics of the gray values of the pixels, including gray average, standard deviation, kurtosis and skewness. The texture feature was the statistics of the spatial distribution pattern of the gray level of the pixel. This study adopted the texture feature parameters based on gray-level co-occurrence matrix (GLCM), including contrast, correlation, energy, entropy and homogeneity.
Statistical analysis
The Matlab 2014b software (Mathworks, Nafick, MA, USA) was used to calculate the radiomics features parameters, and the Mann-Whitney U test or t test was used to compare the differences of the age, tumor diameter, and radiomics features based on X-ray images between TNBC and non-TNBC groups, the receiver operating characteristic curve (ROC) was used to determine the optimal cutoff value of each radiomics feature parameter for differentiating TNBC from non-TNBC, and the corresponding area under the curve (AUC), sensitivity and specificity were obtained. P < 0.05 indicated that the difference was statistically significant.
Results
Clinical characteristics of patients
A total of 120 patients with invasive ductal carcinoma of the breast had been studied, including 30 patients with TNBC and 90 patients with non-TNBC, all of them were female. TNBC patients were with the age of 36–72 years old (mean 52.8 years) and with the tumor diameter range of 0.8–5.4 cm (mean 2.7 cm), non-TNBC patients were with the age of 39–75 years old (mean 53.5 years) and with the tumor diameter range of 0.7–6.1 cm (mean 2.9 cm). There were no statistically significant differences in the age and tumor diameter between two groups (P > 0.05, respectively). In 30 patients of TNBC, there were 25 cases of mass lesions, including 2 cases with calcification; 5 cases with structural distortion or asymmetrical dense lesions and without calcification. Among 90 patients of non-TNBC, there were 72 cases of mass lesions, including 8 cases with calcification; 18 cases with structural distortion or asymmetrical dense lesions, of which 6 cases with calcification.
Results of radiomics features
The lesion segmentation of TNBC and non-TNBC by drawing a ROI on the breast tumor was shown in Figs. 1 and 2 and 12 radiomics features parameters for each ROI were extracted, the statistical results were shown in Table 1. For morphological features,there were statistically significant differences in the roundness and concavity between TNBC and non-TNBC groups (P < 0.01, respectively), the corresponding AUC were 0.753 and 0.702, respectively, and the roundness of TNBC was higher than non-TNBC, but the concavity was contrary; For the statistical characteristic parameters of gray, there were statistically significant differences in the gray average and skewness between two groups (P < 0.05, respectively), and the corresponding AUC were 0.672 and 0.643, respectively. The gray average of TNBC was higher than non-TNBC, but the skewness was contrary; For the texture features, there was no statistically significant difference between two groups (P > 0.05). Among all the extracted radiomics features parameters, the best radiomics parameter was the roundness of breast tumor, the better parameter was concavity, and their optimal cutoff value, sensitivity and specificity for differentiating TNBC from non-TNBC were shown in Table 2. The corresponding ROC curve was shown in Fig. 3.

a: A craniocaudal (CC) X-ray image of TNBC with the tumor size of 1.5 cm×2.1cm (arrow), there were some small calcification outer the breast tumor. b: The segmentation image of the tumor from Figure a presented a round and regular tumor shape. c: The manual segmentation by drawing a ROI on the tumor in the same image as Figure a in red was extracted via ITK-SNAP software. TNBC: triple negative breast cancer, ROI: region of interest.
a: A craniocaudal (CC) X-ray image of non-TNBC with the tumor size of 2.5 cm×3.0 cm (arrow), there were some burrs and lobulated signs around the tumor. b: The segmentation image of the tumor from Figure a presented an irregular tumor shape. c: The manual segmentation by drawing a ROI on the tumor in the same image as Figure a in red was extracted via ITK-SNAP software. TNBC: triple negative breast cancer, ROI: region of interest.
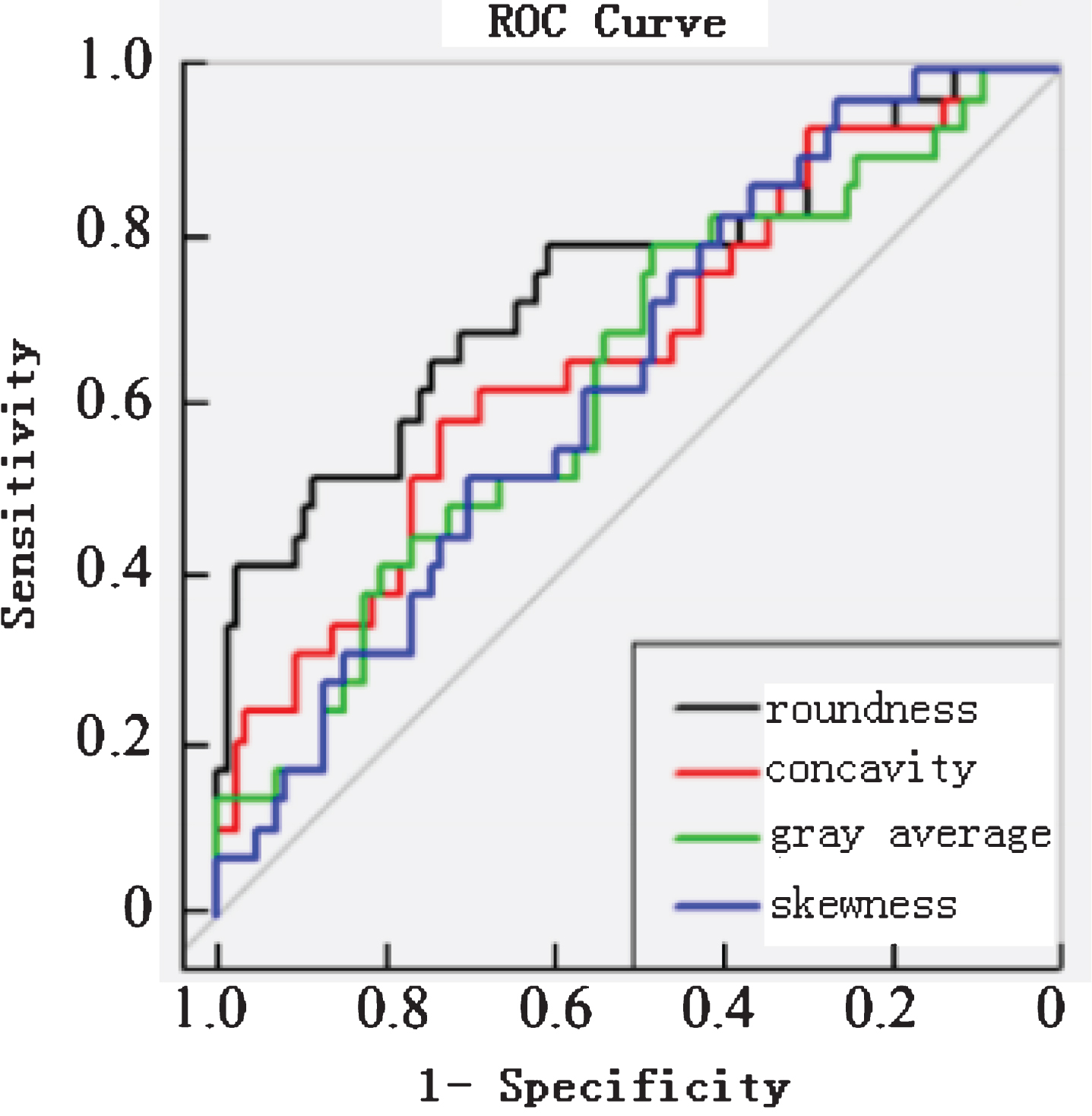
A graph showing the ROC curve for 4 radiomics features parameters with statistically significant differences. The AUCs of the roundness, concavity, gray average and skewness for differentiating TNBC from non-TNBC were 0.753, 0.702, 0.672, 0.643, respectively. ROC: receiver operating characteristic curve. AUC: area under the curve.
Comparisons of 12 radiomics features between TNBC and non-TNBC
Note: athere were statistically significant differences for 4 radiomics features parameters between TNBC and non-TNBC datasets (P < 0.05). TNBC: triple negative breast cancer.
Results of ROCs of 12 radiomics features parameters for differentiating TNBC from non-TNBC
Note: TNBC: triple negative breast cancer, ROC: receiver operating characteristic curve, AUC: area under the curve.
At present, breast cancer is recognized as a group of highly heterogeneous diseases and is further categorized into two major subtypes based on immunohistochemical expression of receptors, namely triple-negative breast cancer (TNBC) [estrogen receptor (ER) negative, progesterone receptor (PR) negative, and human epidermal growth factor receptor 2 (HER2) negative], and non-TNBC (ER or PR or HER2 positive) [15]. Because of this mixed spectrum of gene expression, each subtype displays different clinical behaviors, responses to treatment, and prognosis [16]. In particular, TNBC lacks expression of all three receptors (ER, PR, and HER2) and is known to have a more aggressive clinical course and poorer outcomes [17–19]. Accordingly, early distinction of TNBC from other subtypes with a non-invasive imaging modality would allow clinicians to establish ideal treatment management before final pathologic confirmation [20]. The radiomics method may play the role on differentiating breast tumors and monitoring their development and treatment response, and it can provide a reliable solution to the spatial and heterogeneous problems of breast tumors. In this study, the morphological, gray statistics and texture features in the radiomics method were used to objectively and quantitatively analyze the breast tumors on the X-ray images, and there were statistically significant differences in the morphological and gray statistics features between TNBC and non-TNBC groups (P < 0.05); but there wasn’t a statistically significant difference in the texture feature between the two groups (P > 0.05).
In this study, we compared 12 radiomics features between TNBC and non-TNBC, the results showed that there were statistically significant differences in 2 morphological features (roundness and concavity) and 2 gray features (gray average and skewness). Compared non-TNBC, TNBC was more round and more regular, which was consistent with the literature [21]. The concavity reflected the regularity degree of the shape of breast tumor, the smaller the value of the concavity was, the more regular the shape of the tumor became. The gray feature results showed that TNBC had a higher gray average, demonstrating that TNBC had higher brightness than non-TNBC on X-ray images. Skewness referred to the bending state of asymmetric distribution. In this study, most of the skewness of breast lesion was smaller than 0, presenting negative skewness, and the skewness of non-TNBC was bigger than TNBC. For the ability to distinguish between TNBC and non-TNBC, the AUCs of the roundness and concavity of breast tumors were both more than 0.70, but the sensitivity of the concavity was only 0.586; Among them the sensitivity of the skewness was the highest (0.966); while the specificity of concavity was the highest (0.825). Therefore, the above radiomics features parameters should be considered as potential markers, which could be applied to distinguish between TNBC and non-TNBC in the future.
For the size of breast tumor, the results of this study showed that there wasn’t a statistically significant difference between TNBC and non-TNBC, which was consistent with the literature [21]. However, the results of Youk et al. [22] showed that TNBC was larger than non-TNBC on MRI, this may be because that X-ray image was a two-dimensional image, while MRI could display three-dimensional lesions, and there was a deviation for the actual size of breast tumor between on X-ray image and on MRI; For the texture features, there were not any statistically significant differences between two groups in this study, but the previous studies [22] showed that TNBC was more uneven on dynamic contrast-enhanced MRI, this was possibly related to the different imaging modes, and it may also have an effect on the texture features results due to the small sample in this study.
Our study also had several limitations. First, as there was no obvious boundary between breast lesion and normal breast tissue, and there was no suitable algorithm to achieve the automatic segmentation of breast lesions, the data used in this study was all manually divided by a senior imaging physician, and this would inevitably cause errors to the real boundary of lesions; Second, the sample amount in this study was less, and it needed a large number of multi-center patient data to validate the accuracy.
In conclusion, the radiomics features of breast cancer based on X-ray images, namely the roundness, concavity, gray average and skewness, could be helpful to differentiate TNBC from non-TNBC, which have potential value on clinical treatment options.