
Abstract
BACKGROUND:
Iterative reconstruction is well-established in diagnostic multidetector computed tomography (MDCT) for dose reduction and image quality enhancement. Its application to diagnostic cone beam computed tomography (CBCT) is only emerging and warrants a quantitative evaluation.
METHODS:
Several phantoms and a canine head specimen were imaged using a commercially available small-field CBCT scanner. Raw projection data were reconstructed using the Feldkamp-Davis-Kress (FDK) method with different filters, including denoising via total variation (TV) minimization (FDK-TV). Iterative reconstruction was carried out using the TV-regularized ordered subsets convex technique (OSC-TV). Signal-to-noise ratio (SNR), noise power spectrum (NPS) and spatial resolution of images were estimated. Dose levels were measured via the weighted computed tomography dose index, while low-dose image quality degradation was estimated via structural similarity (SSIM).
RESULTS:
OSC-TV and FDK-TV were shown to significantly improve image signal-to-noise ratio (SNR) compared to FDK with a standard filter, 5.8 and 4.0 times, respectively. Spatial resolution attained with different algorithms varied moderately across different experiments. For low-dose acquisitions, image quality decreased dramatically for FDK but not for FDK-TV nor OSC-TV. For low-dose canine head images acquired using about 1/5 of the dose compared to a reference image, SSIM dropped to about 0.3 for FDK, while remaining at 0.92 for FDK-TV and 0.96 for OSC-TV.
CONCLUSION:
OSC-TV was shown to improve image quality compared to FDK and FDK-TV. Moreover, this iterative approach allowed for significant dose reduction while maintaining image quality.
Introduction
Introduced towards the end of the 1990’s, diagnostic cone beam computed tomography (CBCT) [1–3] was first dedicated to dento-maxillo-facial imaging, but it is gradually becoming important in other applications such as oral, ear, paranasal sinuses and throat imaging or osteoarticular exploration of extremities [4–6]. The main advantages of these dedicated CBCT systems are high spatial resolution, with the smallest reconstructed voxel size reaching about (100×100×100) μm3, as well as reduced equipment costs and physical space required for such units. Their main disadvantages are a limited capability for truly quantitative imaging, in particular, a reduced soft-tissue contrast, and a limited field of view [3, 7]. For image reconstruction, commercial small-field CBCT systems rely almost exclusively on filtered backprojection, namely the Feldkamp-Davis-Kress (FDK) algorithm [8], with various forms of image post-processing which remain proprietary. The FDK algorithm is known for its simplicity and high computational speed. However, it performs poorly for low-dose acquisitions [9] and is prone to severe metal artifacts if no correction method is applied [10].
Ionizing radiation dose is an important concern in CT imaging [11]. For several diagnostic tasks, CBCT offers significantly lower radiation doses than multidetector CT (MDCT), without compromising diagnostic accuracy. In particular, it allowed for dose reductions for the examination of head, neck and dento-maxillofacial structures [12], sino-nasal region [13], the ankle [14] and wrist [15] regions, as well as orthognathic treatment planning and diagnostic imaging of the temporal bone [16]. However, certain state-of-the-art MDCT scanners are able to achieve lower patient dose than typical CBCT scanners, using low-dose protocols coupled to iterative reconstruction methods for dento-maxillo-facial [8, 17, 18] and extremities [19, 20] imaging.
Such observations bring an important motivation point for this paper: considering that dose levels are similar for iterative-based low-dose MDCT imaging and routine CBCT protocols, CBCT imaging coupled to iterative reconstruction may provide yet the lowest dose levels. Promising results are available with regard to iterative reconstruction for flat-panel CBCT using numerical simulation [21], prototype scanners [22], as well as clinical whole-body CBCT devices for image-guided radiation therapy [23] and C-arm CBCT scanners [24]. Our hypothesis is that iterative reconstruction also improves image quality and enables low-dose imaging in small-field CBCT. The purpose of the study is to demonstrate the potential of iterative reconstruction for dose reduction and image quality enhancement in small-field CBCT imaging by comparing conventional and iterative techniques.
Materials and methods
Test objects and acquisition parameters
Several phantoms were used in the study. A calibration phantom provided by NewTom (Verona, Italy) was used to determine denoising parameters for various reconstruction algorithms. It consists of a circular acrylic tube of an outer diameter of 150 mm. It is filled with water and contains an insert – an aluminum tube with an outer diameter of 60 mm and 2 mm thickness, placed coaxially with respect to the acrylic container. A uniform water phantom and a custom-made spatial resolution phantom were used to provide further quantitative evaluation of image characteristics, while an anthropomorphic wrist phantom and a cadaveric canine head simulated clinical uses of small-field CBCT. The uniform phantom was a water-filled plastic cylinder with a diameter of 69 mm. The spatial resolution phantom contained bars of polytetrafluoroethylene (PTFE) scanned in-air, which created a density step-function used to evaluate spatial resolution. The wrist phantom, by The Phantom Laboratory (Greenwich, NY), consisted of dried human bones embedded into a proprietary resin mimicking soft tissue and was used to investigate the potential for ionizing radiation dose reduction for extremity imaging. The canine head specimen served a dual purpose: a qualitative assessment of anatomical features and a quantitative assessment of low-dose images. All animal procedures were approved by the institutional Animal Care Committee of the Centre de recherche du Centre hospitalier de l’Université de Montréal.
For all the acquisitions, the 5G™ scanner by NewTom (Verona, Italy) was used. This device possesses a source-to-detector distance of 970 mm, a minimum source-to-skin distance of 150 mm and a flat-panel detector with an isometric pixel pitch of 127 μm [25]. The detector binning is 1×1 for scans with the “HiRes” option, and 2×2 otherwise. The tube potential is fixed at 110 kVp. The acquisition and reconstruction parameters of interest are listed in Table 1. The user can select predefined dose levels and the total exposure (mAs) is set automatically by the scanner based on scout images.
CBCT acquisition protocols and dose estimates
CBCT acquisition protocols and dose estimates
FOV = field of view, CTDIW= computed tomography dose index, weighted. The names of the options in the descriptions of the experiments are proprietary and define the number of projections and the exposure of each acquisition protocol, detailed in the respective columns.
To study low-dose acquisitions, a wrist phantom and a canine head specimen were first scanned with the CBCT protocols tuned for higher image quality and higher dose, to provide reference images. Below, the estimated doses used to obtain the reference images are compared with imaging doses reported in the literature. For the wrist phantom, the reference image was acquired using the “HiRes” option, with a total exposure of 10.53 mAs (see Table 1). This value was determined by the automatic exposure control system of the scanner. According to Koivisto et al. [15], this exposure corresponds to an effective dose of about 1.6 μSv, a dose about five times lower than for the MDCT scan, in their experiment. Dose reduction with respect to the reference image was simulated via a reduction of the number of projections, by picking projections from the original sinogram (number of projections N = 486) at regular angular intervals. The following few-view sinograms were used: 243 (N/2), 121 (∼N/4), 60 (∼N/8) and 30 (∼N/16) projections.
For the canine head, a reference acquisition with a higher dose (CTDIW of 1.58 mGy) and two test acquisitions with lower doses (0.48 mGy and 0.31 mGy) were acquired, as reported in Table 1. These values may be cautiously compared to doses in clinical settings. A similar type of acquisition, with respect to anatomy size and structure, would be a pediatric head CT. It should be noted that the volumetric CTDIVOL is used for MDCT acquisitions, mostly done in helical mode to account for the scanner pitch. For a typical CBCT scanner, the CTDIW and CTDIVOL are equivalent, since the scan is acquired in a single revolution. According to a survey of the American College of Radiology, the mean CTDIVOL for a pediatric head scan in U.S. children’s hospitals is of 22.3 mGy [26], about 14 times the dose imparted by the reference canine CBCT scan in our study.
The classical FDK filtered backprojection algorithm [27] from the OpenRTK library v.1.1.0 [28] was used as a reference reconstruction method. As the choice of filter influences image properties, two filters were considered. The first is a ramp function multiplied by a Hamming window similar to a standard filter. The corresponding reconstructions were labelled FDK-Hamming. The second one is a ramp multiplied by a Cosine window similar to a bone CT filter, with the label FDK-Cosine.
The iterative reconstruction technique used in this study was the OSC-TV method by Matenine et al. [9] It combines two algorithms, each now considered classic in iterative reconstruction. The OSC algorithm [29] is a model-based technique which supposes Poisson-distributed photon counts at the detector, well-suited for low-dose acquisitions. Geometrical modelling of the CBCT acquisition process is done via ray-tracing. The TV denoising technique is applied to the 3D image estimate in an alternating fashion with OSC. OSC-TV was shown to be of interest using simulations and a small set of experimental CBCT data [9], but a thorough evaluation in a realistic CBCT context is not available at this time, which in part motivates the current study.
To consider the recent introduction of advanced denoising techniques into clinical practice, another method was evaluated: FDK-Hamming images regularized using the TV denoising identical to the TV step of the OSC-TV algorithm [30], further denoted FDK-TV. A similar technique was proposed by Mao et al. [31]. In our work, OSC-TV and TV filtering for FDK-TV were performed using an in-house GPU-based implementation of these techniques. The parallel code was run on a single NVIDIA (Santa Clara, CA) GTX Titan GPU (GK110 microarchitecture).
Selection of denoising parameters
Iterative algorithms are known to be sensitive to the choice of free parameters, especially ones regulating denoising properties [23, 24]. Before proceeding with case studies, the influence of free parameters on the noise-resolution trade-off was studied on the calibration phantom. Data was retrieved in a slice 10.5 mm off the imaging isocenter. The image SNR was assessed in water, in a circular region-of-interest (ROI) with a diameter of 37.5 mm in the center of the slice. The SNR formula was SNR = E/σ, where E denotes the mean density value in the ROI and σ denotes the standard deviation therein. The spatial resolution was assessed using the modulation transfer function (MTF) derived from the step-function profiles created by the water-aluminium interface, as described by Cunningham and Fenster [32]. The step-function was oversampled using the small-angle approach by Fujita et al. [33] The edge profiles were sampled in the radial and tangential directions, at a distance of about 30 mm from the rotation axis (measured in-slice). MTF50 values, defined as the spatial frequency at which the MTF reaches 50% contrast, were interpolated from the MTF curves.
Several reconstructions of the same sinogram were performed. For the FDK methods, the relative cut-off frequency of the filter window varied from factor 0.5 to 1.0 of the Nyquist frequency. For OSC-TV, several values of the regularization strength parameter c, described in detail by Matenine et al. [9], were tested. The initialization image was uniform with an attenuation of 0.5 cm–1. The number of iterations was constant at 12, as suggested by Matenine et al. [9], and the initial number of subsets was set to 1/8 of the number of projection views, since larger numbers of subsets led to numerical instability. For FDK-TV, the cut-off frequency of the FDK filter window was set to 1.0 and the regularization strength c was set to several values. In OSC-TV, OSC and TV steps are alternated. It should be noted that FDK-TV considers the extreme case where FDK is a single iteration of an iterative algorithm and is followed by a single TV step. In consequence, it is expected that the values of c may be very different between OSC-TV and FDK-TV for similar image properties.
Image quality metrics
The image SNR was assessed in the central slice of the water phantom, using a circular region-of-interest (ROI) with a diameter of 60 mm, which amounts to 75.6% of the total surface of the water phantom in an axial slice, therefore covering the center and the periphery of the phantom. To check the variability of the SNR estimates, a ROI of the same size and in-slice position was sampled elsewhere in the volume: 15 mm below and 15 mm above the central slice, in the axial direction. The root-mean-square (RMS) difference between the center and the off-center SNR was computed. Further, the 3D noise power spectrum (3D NPS) was assessed on the same phantom, using the technique proposed by Boone et al. [34], using 16 cubic ROIs placed along a concentric circle in the central axial plane. For the dedicated resolution phantom, the edge profiles were sampled at about 40 mm from the scanner isocenter, in the radial and tangential directions and analysed using the method described above for the calibration phantom. A relative metric was used to assess image degradation for lower imaging dose levels and fewer X-ray projections. Even if exact density values are not known in a specimen, images of the specimen acquired at different dose levels can be compared quantitatively using the mean structural similarity index (SSIM) [35]. It compares images in terms of luminance, contrast and structure to provide a quality index similar to the evaluation by a human observer. It varies from 1.0 for identical images to –1.0 for full contrast inversion.
Since each reconstruction algorithm yields unique image characteristics, none is selected as a gold standard of image quality, but image degradation is assessed for each algorithm separately. Quantitative evaluation was performed using in-house plugins for the ImageJ/FIJI [36] software and Python scripts for final analysis and graph generation. Images were also subject to qualitative evaluation by a radiologist specialized in dento-maxillo-facial imaging with 20 years of experience. For the wrist phantom, the delineation of compact bone and trabecular bone was visually compared between algorithms. For the canine head, soft tissue delineation was compared; severity of the streaking artifact was assessed for both phantoms.
Dosimetry
A number of recent dosimetric studies reported the effective dose for particular scanning protocols and sites, for the NewTom 5G scanner used for this paper [12, 14–16]. In particular, Koivisto et al. estimated the effective dose to the wrist via experimental measurements using multiple MOSFET dosimeters embedded in a multi-sectional anthropomorphic wrist phantom [15]; Nardi et al. reported several effective dose values for head and neck imaging [12]. Effective dose measurements are out of the scope of this paper; instead, the weighted computed tomography dose index (CTDIw) was measured experimentally according to the procedure described in AAPM Task Group 111 report [37] for the 12×8 and 15×12 fields. The main motivation here is to independently quantify the imaging dose and its reduction in a repeatable manner and enable dose comparisons, using a state-of-the art dosimetric protocol. An acrylic phantom of 16 cm in diameter and a length of 28 cm was used to generate sufficient scattered radiation. Dose measurements were acquired with a small volume ion chamber (10X6-0.6CT, Radcal Corporation, Monrovia, CA).
Results
Selection of denoising parameters
Noise-resolution curves obtained from the calibration phantom reconstructions are presented in Fig. 1. FDK-Hamming and FDK-Cosine demonstrate a wide variation of spatial resolution when the cut-off frequency is varied, while the SNR variation is limited. FDK-TV also demonstrates a wide variation of spatial resolution, with higher resolution attained for the lowest regularization strength. Peak SNR is reached at c = 0.02, while the spatial resolution is at a medium value. OSC-TV, for its part, offers an almost constant spatial resolution over a wide range of regularisation strength values, but the SNR varies greatly, with the highest SNR values achieved at c = 0.1.
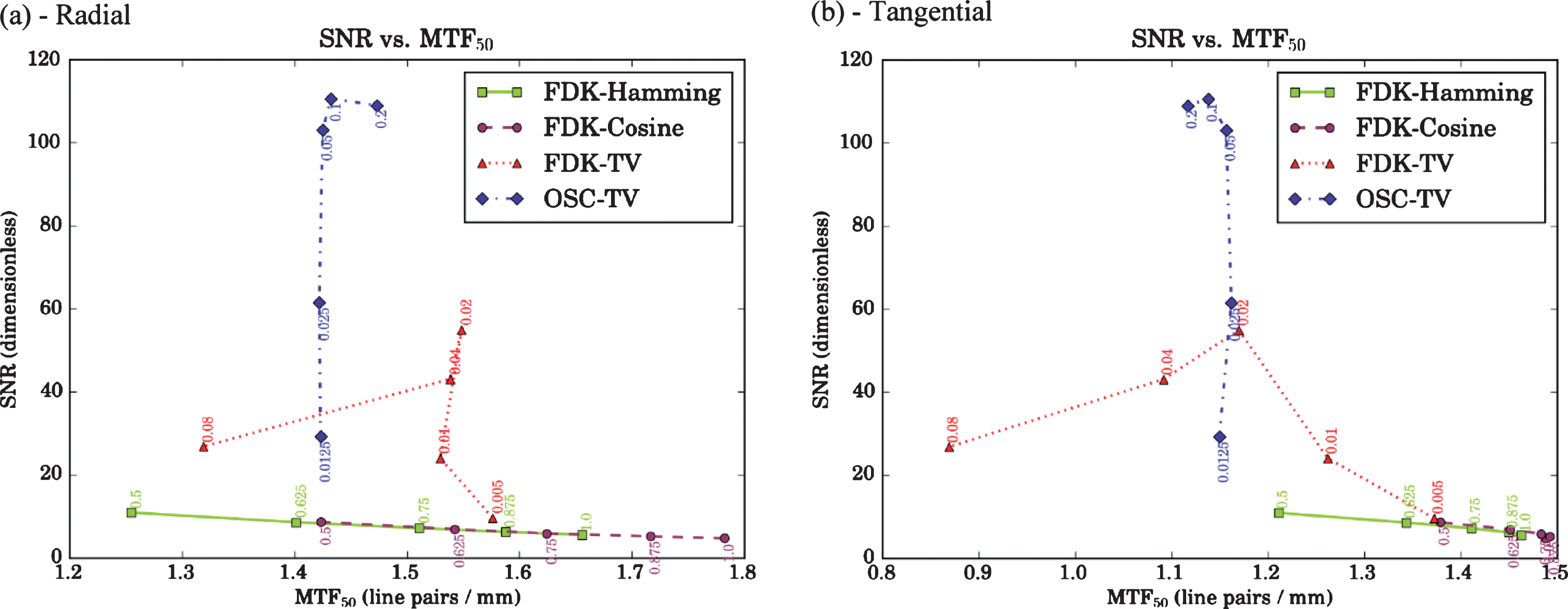
(a, b) Noise-resolution properties for a range of denoising settings, for resolution measured (a) radially and (b) tangentially in the calibration phantom. For FDK-Hamming and FDK-Cosine, relative cut-off frequencies are used as point labels. For FDK-TV and OSC-TV, values of regularization strength c are used as point labels. OSC-TV offers an almost constant spatial resolution, while the SNR varies greatly. FDK-TV reaches a peak SNR at c = 0.02, while spatial resolution varies greatly. FDK-Hamming and FDK-Cosine demonstrate high resolution variation with a low SNR variation.
The algorithms behave quite differently, with OSC-TV offering a radial resolution roughly equivalent to FDK-Cosine at a relative cut-off frequency of 0.5 and a tangential resolution about 6% below the lowest resolution attained via classical approaches. Therefore, we reason that the choice of the free parameters relies on the best an algorithm has to offer (either better SNR or better resolution), since it would be difficult to match both SNR and resolution for all algorithms. Based on this reasoning, for FDK-Hamming and FDK-Cosine, a relative cut-off frequency of 1.0 is retained, since it yields the best spatial resolution while the SNR does not diminish dramatically. For FDK-TV, the choice is obvious, thanks to the SNR peak at c = 0.02. For OSC-TV, since the spatial resolution is almost constant, the SNR peak also guides the choice of regularization strength (c = 0.1). These values are therefore retained for the experiments that follow, and the major difference in the behaviour of algorithms should be considered in further analysis.
The reconstructions of the central slice of the water phantom are shown in Fig. 2 along with central line profiles. Profiles of unregularized FDK methods (Fig. 2, top row) are quite noisy, with FDK-Cosine presenting more noise, consistent with a bone filter. Regularized FDK-TV and OSC-TV yield more uniform profiles, with OSC-TV surpassing FDK-TV. SNR values obtained in the relevant ROI were the following: 11.3±0.7 for FDK-Hamming, 5.2±0.4 for FDK-Cosine, 45±2 for FDK-TV and 65±2 for OSC-TV. The variation indicated is the RMS difference between the central slice SNR estimate and the SNR in off-center slices. Compared to FDK-Hamming (soft tissue filter), OSC-TV and FDK-TV provided an SNR gain of 5.8 times and 4.0 times, respectively. Multiplanar views of the 3D NPS are shown in Fig. 3. All these profiles have a roughly toroidal shape typical for CT imaging. FDK-Cosine shows the highest spectral spread as well as the highest dynamic range of noise power. FDK-Hamming shows similar profiles with lower spectral spread and dynamic range. FDK-TV and OSC-TV show noise concentrated at much lower frequencies and a lower dynamic range, consistent with effective reduction of the high-frequency noise components by the TV algorithm.
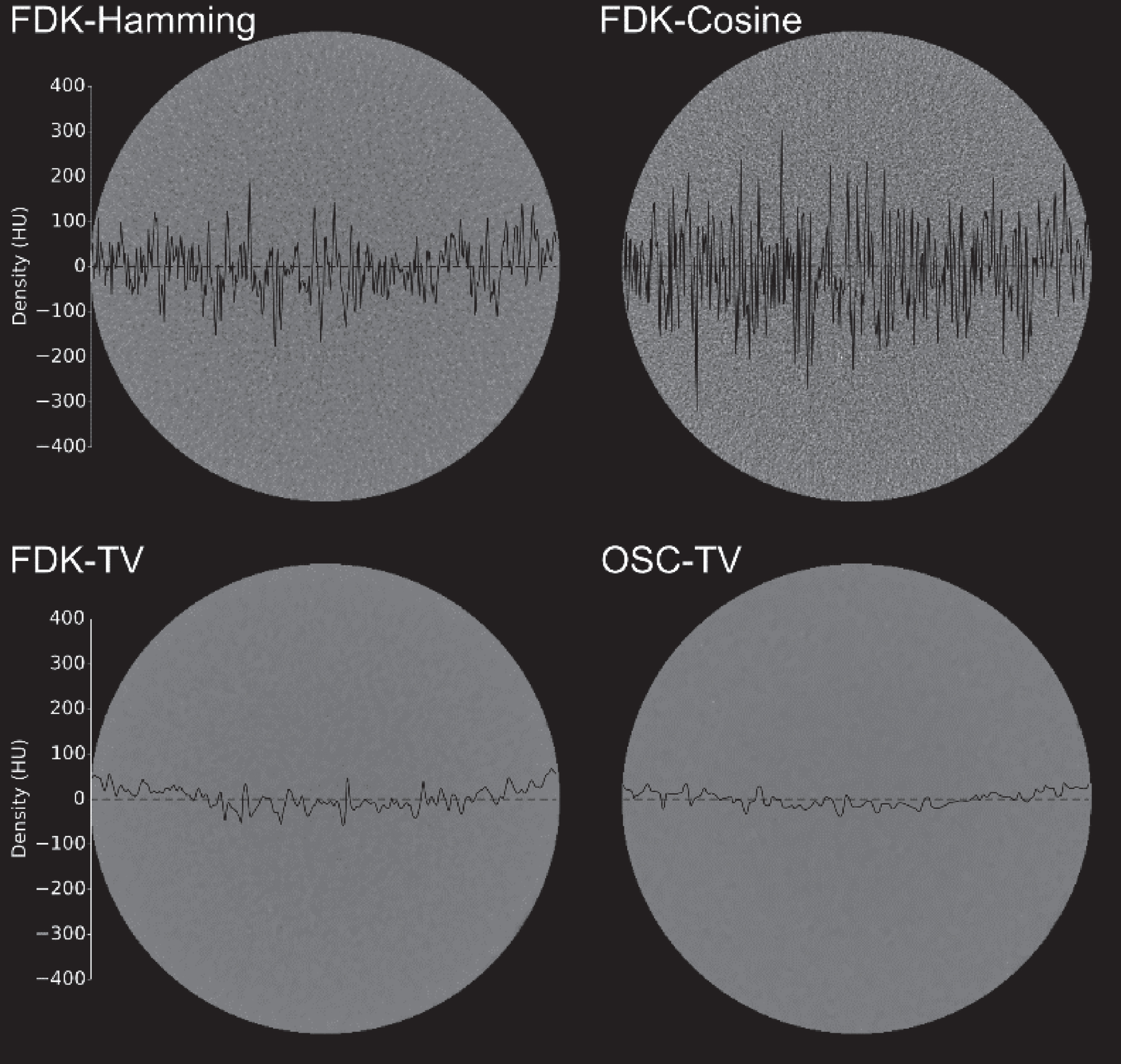
Reconstructions of a water phantom. A density profile is plotted over the corresponding area. Note effective denoising when using TV-regularized methods, with OSC-TV assuring maximum denoising.
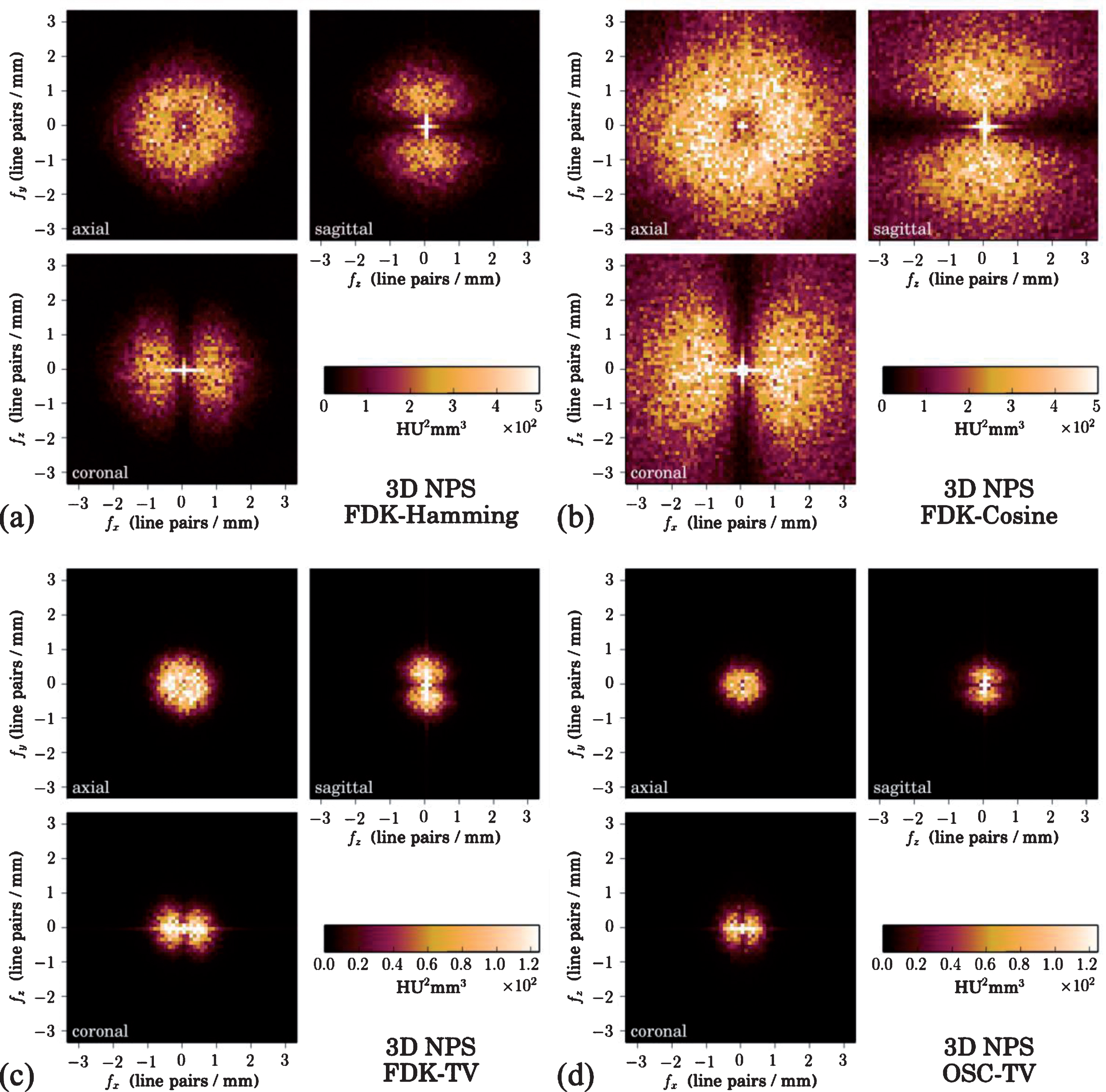
Noise power spectra (NPS) for the different reconstruction algorithms. Orthogonal multiplanar views aligned with the origin are shown, f denotes spatial frequency. Note the different NPS scales used in (a,b) vs. (c,d). TV regularization reduces high-frequency noise as expected, with the model-based OSC-TV providing the least noisy images. Data was collected in the water phantom.
The MTF plots obtained using the spatial resolution phantom are shown in Fig. 4 along with the corresponding MTF50 values and reconstructed edge ROIs. Compared to FDK-Hamming, OSC-TV allowed for a 12% increase in the radial MTF50 and a 14% increase in the tangential MTF50. FDK-Cosine offered an increase of 4.3% and 2.3%, respectively. In contrast, FDK-TV demonstrated reduced spatial resolution: –10% and –8.0% respectively. The overall result shows that the radial resolution is about 30% higher than the tangential one. This effect is true for all tested algorithms and appears related to the imaging system. Radial resolution depends mostly on the source and detector properties, while tangential resolution depends mostly on the angular sampling rate, which was rather modest at 486 views per (the single) revolution, compared to approximately 1000 views per revolution in MDCT.
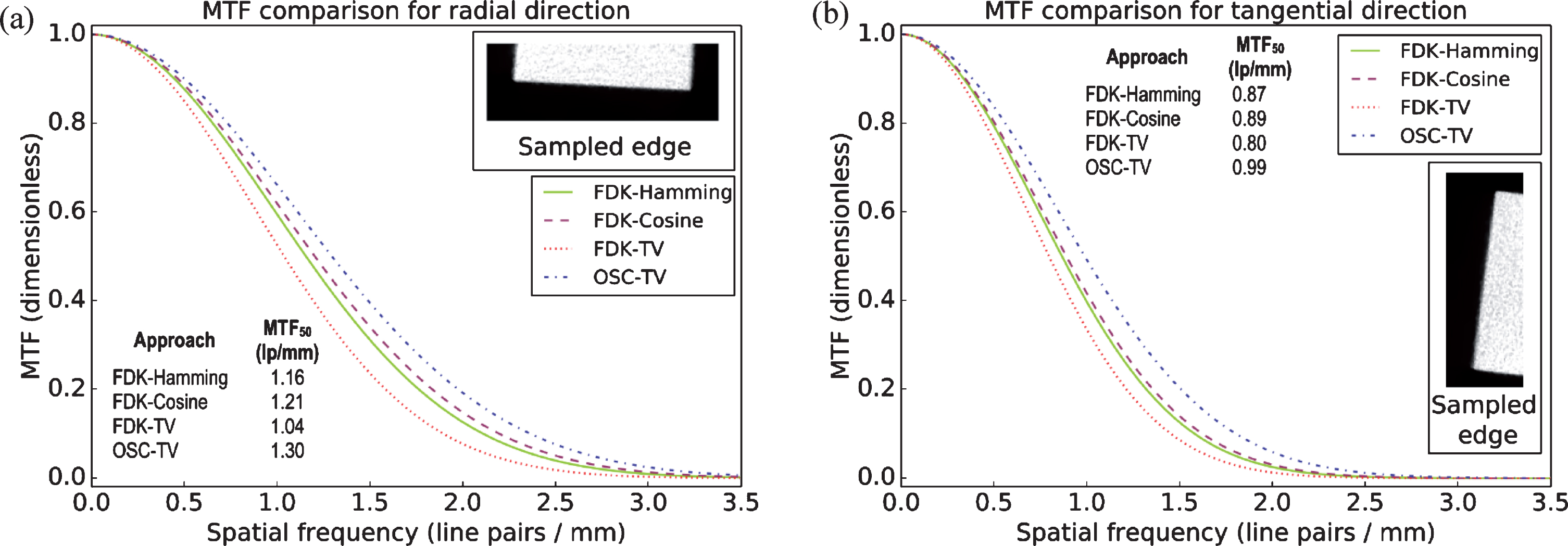
(a, b) Modulation transfer function (MTF) profiles of the edge phantom in the (a) radial and (b) tangential directions. OSC-TV reconstruction of the edge region of interest shown in the inserts. OSC-TV yields the highest MTF values, followed by FDK-Cosine, FDK-Hamming and FDK-TV.
Reconstructions of the wrist phantom and the corresponding SSIM indices are shown in Fig. 5. Visually, FDK-based approaches offer satisfactory results at N (N = 486) and N/2 projections, then image quality degrades rapidly with severe streaking artifacts. OSC-TV is mostly streak-free down to N/4, beyond which streaking appears, but less prominently than for FDK-based methods. Image degradation for the latter is confirmed using the SSIM index, which drops steeply to reach 0.08–0.09 for N/16, see SSIM labels at bottom row of Fig. 5. For OSC-TV, SSIM decreased gradually, reaching 0.57 for N/16 (same image row).
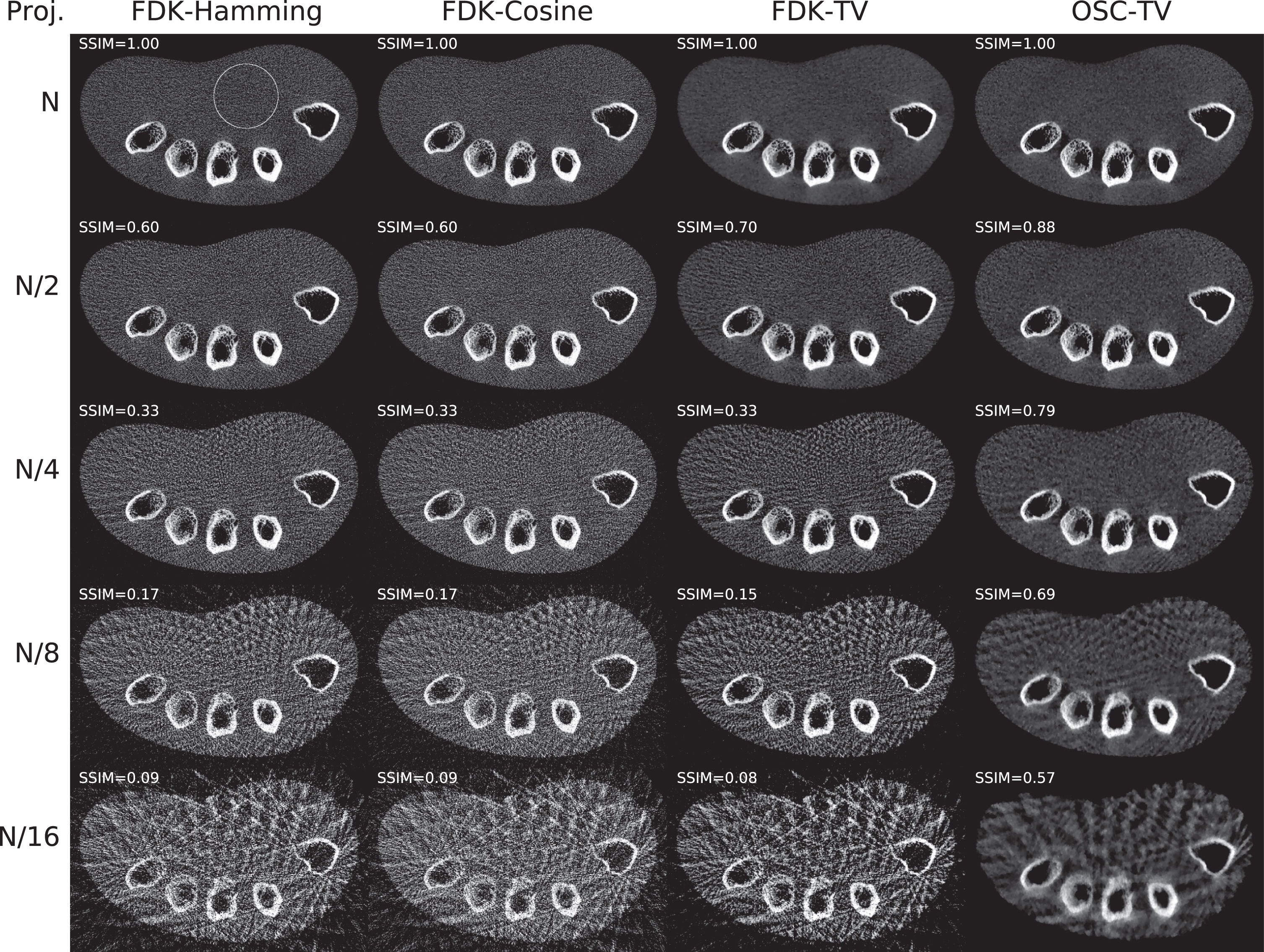
Axial plane reconstructions of a wrist phantom, using different numbers of projections and reconstruction algorithms. The number of projection views in the original dataset was N = 486. The structural similarity index (SSIM) was used to evaluate image quality degradation for few-view reconstructions, separately for each algorithm. Each top-row image is the ground truth for its column. Using fewer projections, the SSIM drops sharply for FDK-based methods, which is not the case for OSC-TV. The top-left reconstruction shows the circular ROI used to evaluate the SNR, see Fig. 6.
Qualitatively, OSC-TV preserved visualisation of trabecular bone down to N/4, while it was already affected for FDK-based methods. At N/8 and N/16, only the edges of the compact bone were well preserved using OSC-TV, while these edges were affected by streaking with FDK-based methods. SNR measurements in a uniform region (see Fig. 5, top-left image) were made, yielding the chart in Fig. 6. SNR values are low for unregularized FDK methods; FDK-TV is equivalent to OSC-TV for the complete sinogram, but its SNR drops dramatically for reduced datasets, while OSC-TV systematically exhibits higher values.
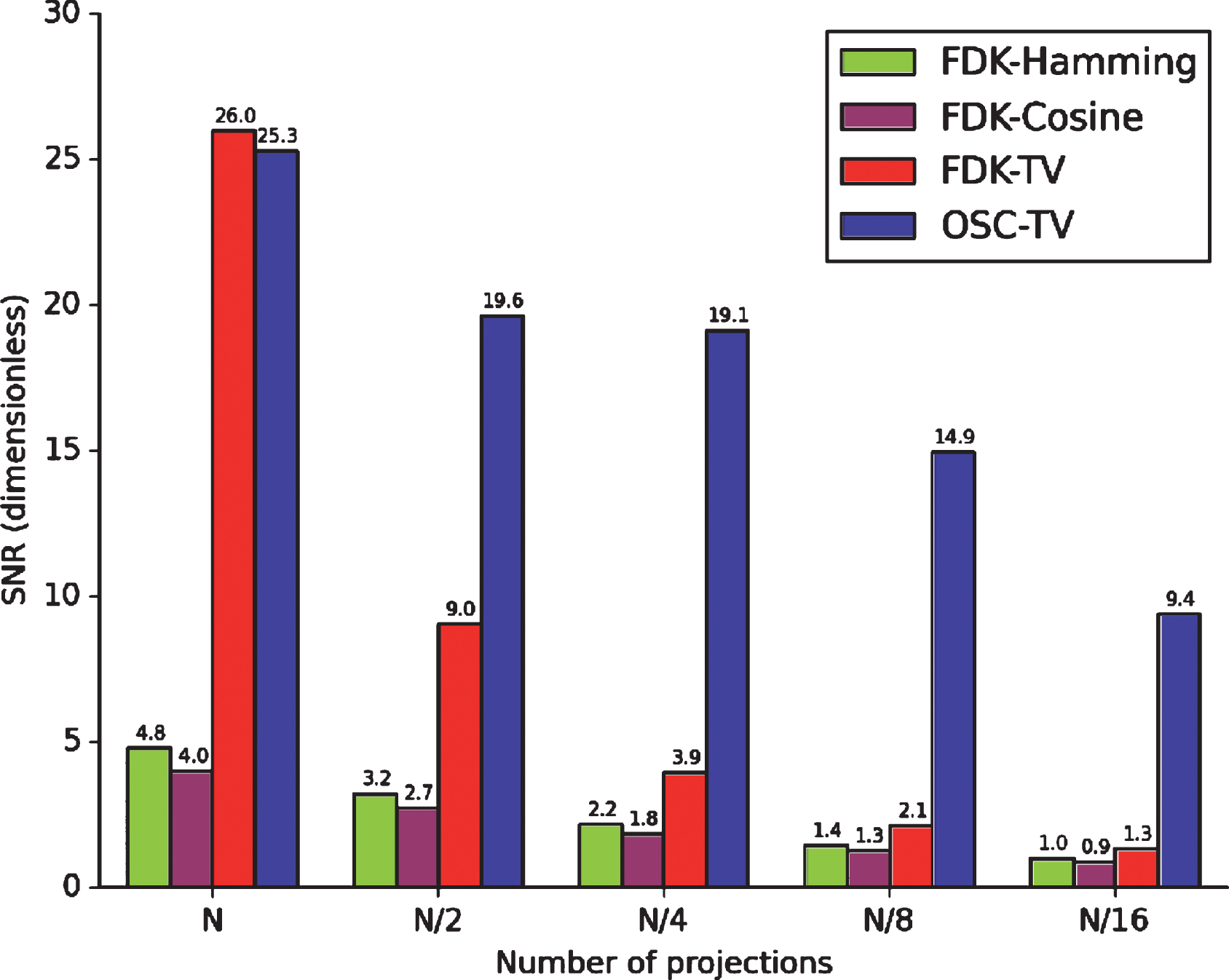
SNR measurements in a circular ROI of the wrist phantom shown in Fig. 5, for different numbers of projections and reconstruction algorithms. The number of projection views in the original dataset was N = 486. SNR values are low for unregularized FDK methods. FDK-TV performs well for a complete dataset, but the SNR drops steeply for few-view datasets. OSC-TV demonstrates the highest SNR values for few-view reconstructions.
Reconstructions of the canine head are shown in Fig. 7. Reference reconstructions obtained from 13.05 mAs datasets are already quite different, with unregularized FDK approaches affected by minor streaking. At 3.97 mAs, noise and streaking already hinder soft-tissue visualisation around the oral cavity and at the level of the subcutaneous fat. At 2.57 mAs, FDK-TV also reveals streaking, while OSC-TV is mostly consistent with higher-dose images. SSIM measurements (see data inserts in Fig. 7) for lower doses quantitatively confirm severe image degradation for unregularized FDK methods and close image correspondence for FDK-TV and OSC-TV.
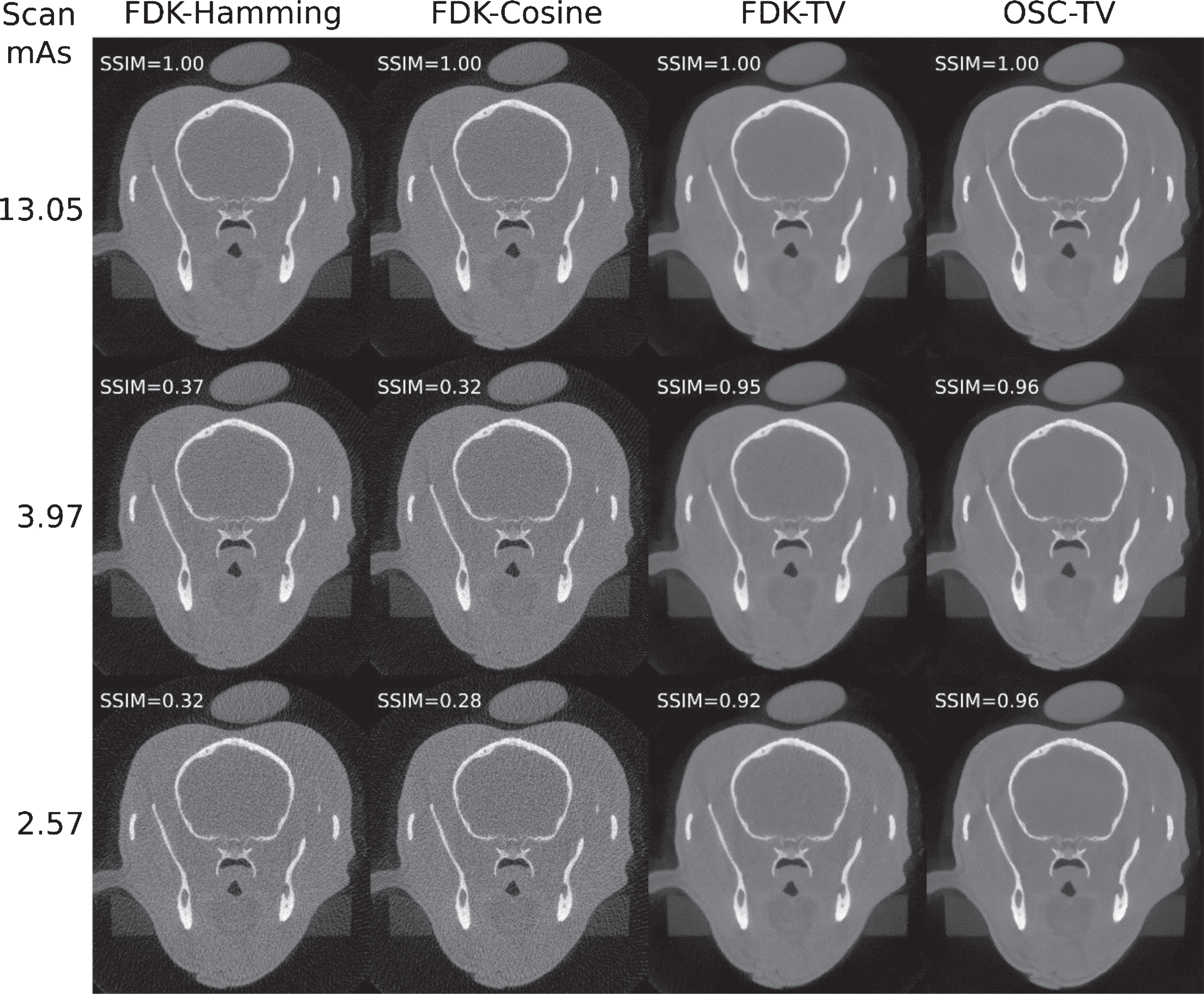
Reconstructions of a cadaveric canine head, using different acquisition protocols and reconstruction algorithms. The axial slice depicts the cranium and mandible. The topmost separate object is a water container for calibration of Hounsfield units. The structural similarity index (SSIM) was used to evaluate image quality degradation for low-dose images, separately for each algorithm. Each top-row image is the ground truth for its column. The SSIM drops sharply for unregularized FDK, while it drops moderately for FDK-TV and even less so for OSC-TV.
Based on experimental measurements, the CTDIw dose-to-exposure ratio was found to be (0.108±0.004) mGy/mAs for the 12×8 field. For the 15×12 field, it was of (0.121±0.005) mGy/mAs, consistent with higher scatter levels. With these coefficients, the CTDIw was estimated and reported in Table 1. For simulated few-view wrist phantom reconstructions, the CTDIw was assumed to scale with the number of projections: (1.14±0.05) mGy for N = 486 projections, (0.28±0.01) mGy for N/4 projections and (0.070±0.003) mGy for N/16 projections. Regarding the dose measurement error, the main uncertainty was the calibration tolerance of 4% of the ionization chamber, as reported by its manufacturer. The random errors arising from repeated measurements accounted for less than 0.2%.
Discussion
With respect to image enhancement, regularized and model-based reconstructions increased SNR values several times compared to FDK as indicated by the calibration phantom study and the water phantom study. NPS analysis was consistent, with a reduction in high-frequency noise and overall magnitude when using TV-regularized methods, especially OSC-TV. Spatial resolution measurements yielded variable results: for the calibration phantom, using an aluminium-water interface, OSC-TV demonstrated a reduced spatial resolution compared to FDK-based approaches. For the PTFE-in-air edge phantom, despite a high regularization strength used for reconstruction, the spatial resolution was slightly higher than for classic reconstructions and FDK-TV, in both radial and tangential directions.
Reconstructions of few-view sinograms, down to N/16 projections, were intended to test the limits of their usability depending on the reconstruction algorithm. FDK-based approaches suffered severe image quality loss starting at N/4 and below, which is expected for analytical methods. OSC-TV offered interesting results down to N/4 projections and limited streaking down to N/16 projections. Such few-view protocols may be appropriate for follow-up imaging, where repeated scans assess the same anatomical site, and radiation dose becomes a concern. A loss of tangential spatial resolution is expected in few-view scans and a dedicated study of this effect is desirable. Among current applications of CBCT, traumatology [38–40], including low-dose protocols [41], is prominent, and follow-up assisted by OSC-TV would be of interest in this field. Another area of interest is diagnostic imaging of rheumatic disorders, such as osteoarthritis. These diseases are often characterised by macroscopic changes in bone, a high-density structure readily observable using CBCT, for example, in the temporomandibular joint [42, 43]. These degenerative pathologies require long-term follow-up, and low-dose imaging is therefore desirable too.
Canine head reconstructions using OSC-TV demonstrated well-preserved boundaries of soft tissues in low-dose images, with CTDIw as low as (0.31±0.01) mGy, compared to FDK-based methods. In terms of size and structure densities, the canine head represents well a pediatric head or an adult neck, the latter two being of interest for future algorithm evaluation. Another potential application is 3D imaging of canine models in preclinical studies, where CBCT may bridge the gap between micro-CT and MDCT in terms of FOV and spatial resolution. OSC-TV would enable low-dose imaging for studies where radiation exposure is to be minimized. Moreover, in veterinary medicine, CBCT is already adopted as a cost-effective diagnostic modality for full-body imaging of small animals [44]. Iterative reconstruction could therefore be extended to diagnostic imaging and low-dose follow-up of many animal species, as well as imaging of osteoarticular pathologies in large animals.
From a general point of view, the study is in agreement with relevant literature [17, 21, 22], which demonstrates that iterative and especially model-based reconstruction is a promising image enhancement and dose reduction strategy. This study extends the existing knowledge to small-field CBCT. For OSC-TV specifically, SNR enhancement and positive response to few-view datasets corroborate the results of a previous numerical and large-field study [9]. NPS analysis, spatial resolution and SSIM measurements based on experimental acquisitions provide new evidence of the potential of OSC-TV in small-field CBCT.
Some limitations of this initial experimental study are to mention. With respect to radiation physics modelling, OSC-TV does not directly address such issues as beam hardening or scattered radiation. Nevertheless, these effects are important to consider in future research on small field CBCT reconstruction, since beam hardening due to metallic restorations and scatter due to wide beam collimation are non-negligible. Recent advances in these areas include augmented likelihood image reconstruction for beam hardening correction [45], as well as a fast algorithm for scatter correction based on photon transport modelling [46, 47], which would be useful for small-field CBCT applications. The limits of the study with respect to clinical applications are the following: first, no reconstructions of clinical cases and no evaluations by several expert observers were performed. Second, this study has not covered the response of the algorithms to metal artifacts and low-contrast lesions, the former being quite common in dental applications.
Conclusions
In this study, the FDK filtered backprojection algorithm routinely used in CBCT systems was compared to an iteratively regularized filtered backprojection method (FDK-TV), and a model-based regularized iterative algorithm (OSC-TV), using experimental data acquired with a diagnostic CBCT scanner employed in clinical practice.
Using a uniform phantom, it was shown that OSC-TV and FDK-TV improve the SNR 5.8 and 4.0 times, respectively, compared to FDK with a Hamming window. 3D NPS profiles showed a lower magnitude and spectral spread for OSC-TV and FDK-TV. The spatial resolution estimates varied moderately across the different experiments. For few-view sinograms of an anthropomorphic wrist phantom, it was shown that OSC-TV was able to prevent streaking artifacts for a sinogram of as few as 121 projections, while the streaking was apparent for the other algorithms in this case. For canine head specimen acquisitions, OSC-TV was able to preserve image quality at about 1/5 of the dose compared to a reference image, yielding an SSIM of 0.96. FDK-TV yielded an SSIM of 0.92, while FDK yielded values close to 0.3.
In summary, iterative reconstruction was shown to improve image quality compared to analytical approaches and allowed for significant dose reduction while maintaining image quality, offering new avenues for diagnostic CBCT imaging.
Disclosure of conflicts of interest
Dmitri Matenine is a part-time employee of Useful Progress Services Inc. (Montreal, QC).
Footnotes
Acknowledgments
This work was partly financially supported by MITACS through the MITACS Accelerate program and by Canada Research Chairs. The authors also would like to thank Useful Progress Services Inc. (Montreal, QC) and its founder Francis Siguenza for financially supporting the MITACS Program.