
Abstract
Background:
Calyceal diverticula outpouchings that occur rarely in the upper collecting system of the kidney and is often difficult to detect. In this study, we present two cases of calyceal diverticula and discuss their clinical characteristics and radiologic features.
Patients and methods:
In the presented two cases, we applied several imaging examinations, including delayed intravenous pyelography, retrograde pyelography and axial computerized tomographic (CT) scanning of the kidneys with and without contrast. Serum creatinine levels in fluid withdrawn from the diverticula were found to be significantly higher than the simultaneous serum creatinine levels. Intravenous injection of methylene blue through a ureteral catheter was also aided in the diagnosis. Calyceal diverticulum neck dilatation was performed through a percutaneous nephroscope.
Results
The two cases were diagnosed preoperatively and the operation was successful performed. The nephrostomy tube was removed seven days after surgery without complications. CT scans of the kidney after six months showed that the size of the calyceal diverticulum of two patients were considerably smaller than pre-surgery. There were no reports of pain in the lumbar region or other discomfort.
Comments:
Diagnosis of calyceal diverticulum mainly depend on a variety of imaging examinations, including the delayed intravenous pyelography, retrograde pyelography, and kidney CT plain scan plus enhanced scan. If the patient cannot be diagnosed by above methods, cyst fluid can be aspirated percutaneously to measure the preoperative creatinine level. If it is significantly higher than the serum creatinine level, the cyst fluid is considered urine, which can assist in the diagnosis of calyceal diverticulum. A ureteral catheter should also be inserted before operation namely, intravenous injection of methylene blue through a ureteral catheter is helpful for diagnosis. The choice of surgical treatment is based on the size and location of calyceal diverticulum and clinical manifestations.
Introduction
Calyceal diverticula have been defined as a congenital, non-secretory abnormality. The definition and classification of calyceal diverticula has gone through many alterations throughout the years [1]. Diverticula are characterized as transitional cell-lined cavities within the renal parenchyma, often communicating with the collecting system via a narrow channel [2], which is lined by non-secretory transitional cell epithelium and surrounded by a layer of muscularis mucosae. Calyceal diverticula have classically been divided into two types. [2, 3]: type I calyceal diverticula are the more common subtype and communicates with a minor calyx. These diverticula most commonly occur in the upper pole of the kidney [4]; type II calyceal diverticula communicate with a major calyx or the renal pelvis at the mid-pole of the kidney and tend to be larger. They are more commonly symptomatic.
Calyceal diverticula are rare condition whose incidence has not been well defined; it is reported in 0.21– 0.6 % of intravenous pyelographic investigations [3, 6] and it occurs bilaterally in nearly 3% of patients [7]. Patients are often asymptomatic until stone formation or acute infection occurs [8–10]. Calyceal diverticula occur with equal frequency in male and female patients, and there is no predilection for the left or right side. Some patients present with hematuria, pain, or sepsis, or nephrolithiasis [11]. Stones are found in more than 50% of calyceal diverticula, and they can be associated with pain, recurrent urinary tract infections, and even damage to the surrounding parenchyma [12]. Stones are thought to be a result of urinary stasis, whereby urine fills the cavity and stagnates due to the narrow neck, precipitating calculi crystals.
The diverticulum communicates with the pyelocalyceal system by a narrow infundibulum in a retrograde way. Calyceal diverticula may be diagnosed as an incidental finding or can be symptomatic owing to recurrent urinary tract infection (UTI) or stone formation within the diverticulum. Some patients concomitantly suffer from stones, tumors [13], or damage to the surrounding renal parenchyma due to compression, which may require surgical intervention [8, 15]. Clinically, simple calyceal diverticula are sometimes misdiagnosed as simple renal cysts.
Here, we present two cases. One patient was found to have a calyceal diverticulum, which had been mis-interpreted as a simple renal cyst on a number of occasions. Other patient was admitted to our hospital for two days of left renal colic. These two patients required treatment, so that we carried out percutaneous procedures to expand the calyx neck orifice. Ureteral stents were then placed to assure drainage.
Presentation of cases
Case 1
The first patient was a 38 year-old male. In 2000, a left renal cyst was found (size unknown) during a physical examination, without urinary frequency, urgency, odynuria, hematuria, lumbago, abdominal pain, or other clinical symptoms. The patient underwent sclerotherapy by a percutaneous puncture under ultrasonographic guidance in another hospital in 2010:280 ml of yellow cyst fluid was drained and the cyst was deflated, and, 50 ml of absolute alcohol was injected into the cyst cavity for sclerosis at the end of the operation. A review of urinary by color Doppler ultrasonography showed no significant change in the cystic space six months postoperatively. Retroperitoneal laparoscopic unroofing of the left renal cyst was performed in another hospital in 2011 (pathological results unknow); no complications such as leakage of urine occurred after operation. However, review of the kidney by color Doppler ultrasonography showed no significant change in cyst size after six months. Percutaneous puncture sclerosing treatment of the renal cyst was performed again in another hospital in 2014. After six months, new examination showed that the size of the renal cyst remained the same as the preoperative size. The patient was checked by urinary tract color ultrasonography and the size of the left renal cyst was 62×49 mm in September 2017. Intravenous pyelography showed the pelvis and calyx were constricted (Fig. 1).

Intravenous pyelography showed the pelvis and calyx were constricted.
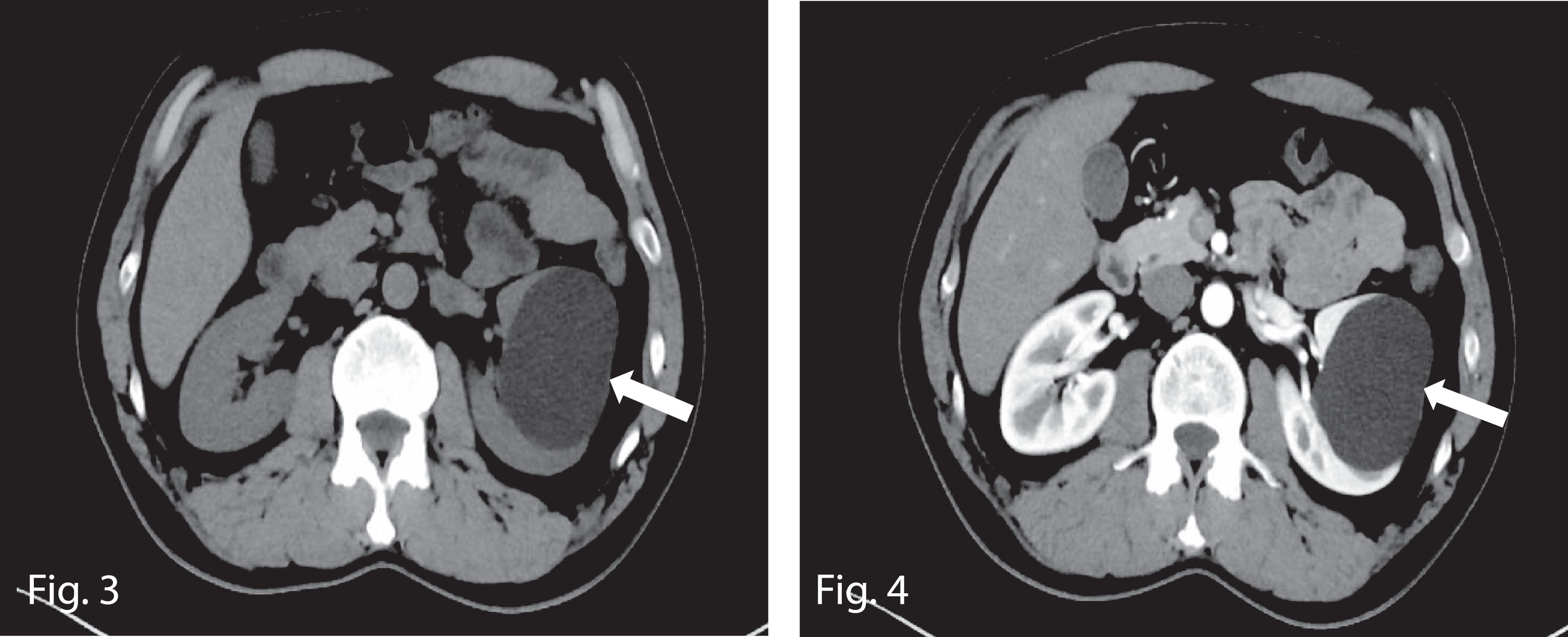
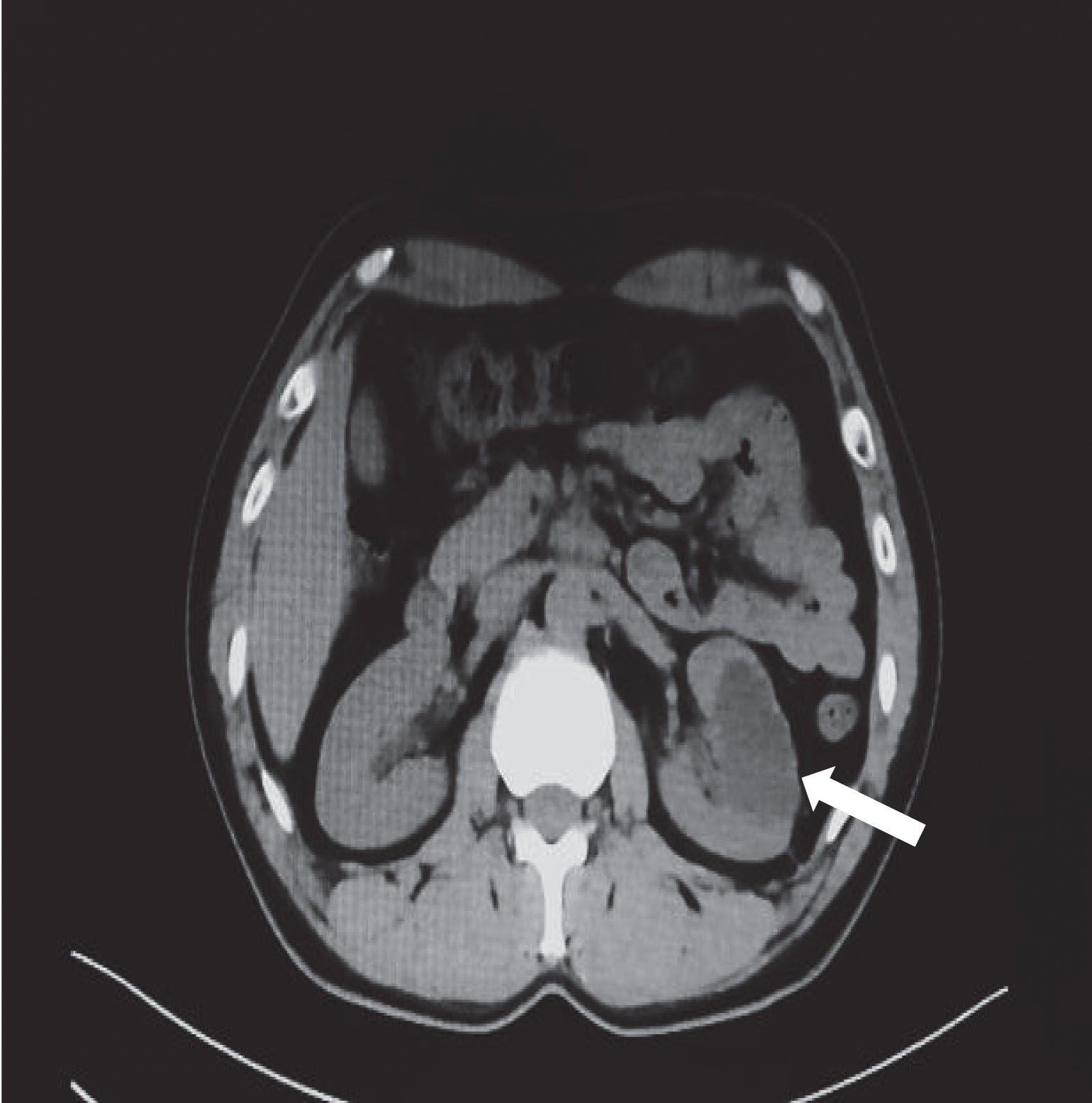
The patient was hospitalized in our hospital in April 2018, because he demanded treatment of the left renal cyst. The color Doppler ultrasound, IVP, kidney computed tomography (CT) plain scan, and contrast-enhanced scan all indicated the presence of a renal cyst, with a size of 66×50 mm (Figs. 3 and 4). The patient had a history of multiple treatments and rapid recurrence in a short time, so we considered the possibility of calyceal diverticulum with hydrocele. After preoperative puncture of the hydronephrotic kidney under the guidance of ultrasound, the creatinine (CR) level of puncture fluid was 2529μmol/l (serum CR levels men < 97μmol/l, women < 73μmol/l), confirming the puncture fluid was urine, so we made the diagnosis of calyceal diverticulum. We treated the calyceal diverticulum through percutaneous nephroscopy with holmium laser and dilatation of the calyceal stenosis.

Two 6 Fr double-J stents were placed from the diverticulum to the bladder.
A 23-year-old female patient was admitted to our hospital due to left renal colic with nausea vomiting and fever (her maximum temperature was 39.2°). She had a medical history of kidney cysts. A color Doppler ultrasonography check of the urinary system had indicated renal cystic lesions of the left kidney in another hospital. We made a kidney CT plain scan and a contrast-enhanced scan, which indicated renal cystic lesions (size 65×52 mm) and renal stones (Fig. 5). We carried out percutaneous nephrostomy and drained abscess fluid. The CR level of puncture fluid was 1626μmol/l. We performed fistula angiography after puncture and drainage (Fig. 6),and we diagnosed the patient with calyceal diverticulum pre-operatively. We performed percutaneous nephroscopy one week after drainage.

Kidney CT contrast-enhanced scan indicated renal cystic lesions and stones.

Fistula angiography show passage between the diverticulum and the calyces.
We successfully treated the two cases through percutaneous nephrolithotomy (PCNL) by holmium laser and dilatation of calyceal stenosis. We followed the procedure previously reported by Shah [16]. Briefly, the patient underwent combined epidural and spinal anesthesia. The patient was placed in a semi-supine combined lithotomy position. The leg on the side of the operation is nearly fully extended with a slight abduction of the hip joint. The other leg is bent, allowing for simultaneous reverse operation throughout the process. First, a 6/7.8 Fr Wolf rigid ureteroscope (Richard Wolf, Germany) is used to check the ureter under the guidance of the guide wire (Boston Scientific). Next, the guidewire is placed into the renal pelvis, and a 6 Fr open-ended ureteral stent is placed by the ureteroscopy and directed through the guidewire. A 16 G coaxial needle is used to initially puncture into the dominant calyx under ultrasound guidance (BK Ultrasound System, Denmark).
The cyst fluid is discharged through the puncture needle tube, proving the puncture was successful. The guidewire is then passed through the needle sheath into the target calyx. The next step is to use the dilated sheath sequentially from 10 Fr, 14 Fr, and 18 Fr to expand muscle and fascial layers. An F16 outer sheath is used to place into the target calyx directed by the guidewire. Rigid ureteroscopy was performed along the guidewire, using a peristaltic pump to continuously rinse with saline to keep the vision clear. However, we could not identify the calyx neck orifice after entering the target calyx, so methylene blue solution was injected through the ureteral catheter. The calyceal opening was detected where methylene blue flowed out, but we were unsuccessful to pass the guide wire due to the obvious stenosis of the calyx neck orifice in the first patient, so we used a holmium laser to open the calyx neck and pass the guide wire through the calyceal opening.
The next step was to use the dilated sheath sequentially from 10 Fr, 14 Fr, and 18 Fr to expand the calyx neck. Two 6 Fr double-J stents were placed anterogradely and passed through the calyx neck, directed by two guide wires. Ureteroscopy was performed to confirm that the lower end of the double-J stent was in the bladder. The operation was completed after the 14 Fr renal stent was placed optimally in the collecting system thought the PCNL channel and properly fixed. The stent was removed on the 7th post-operative day; no complications such as urinary leakage occurring. After three months, a follow-up visit was required. Two double-J stents were removed by cystoscopy after appropriate KUB imaging (Fig. 2). So far, the follow-up period has been more than six months. CT scans of the kidney after six months shows that the size of the calyceal diverticulum of the first patient is 36×32 mm (Fig. 7) and that of the second patient is 37×33 mm, which is smaller than before surgery. There have been no reports of pain in the lumbar region or other discomfort remains by the patients. The two patients are still being followed without further complications.
The CT scans of the kidney after operation showed the size calyceal diverticulum was 38×35 mm.
The etiology of calyceal diverticulum formations remains controversial and appears to be multi-factorial. The most widely accepted hypothesis is that diverticulum development is congenital in origin, resulting from the failure of regression of the third or fourth divisions of the ureteric buds of the Wolffian duct [2, 8]. Alternatively, some proposed that calyceal diverticula are an acquired condition, secondary to the sequelae of obstruction, infections, or tumor [17], which lead to inflammatory or mechanical stenosis of the calyceal or cervical sphincter, and which cause local reflux disorder and increased intracalyx pressure. Finally, the calyx is passively dilated over time to form a diverticulum. Calyceal diverticulum calculi or calcium milk formation is due to a combination of urinary stasis and recurrent infection within the diverticulum.
Regarding the diagnosis and differential diagnosis of calyceal diverticulum, several observations deserve to be emphasized. Firstly, there is a limited allantoic space in the renal parenchyma, which is lined by non-secretory transitional cell epithelium and surrounded by a layer of muscularis mucosae. Secondly, there is an interchange channel between the cyst and the renal collecting system. Several imaging studies have been used in the diagnosis of calyceal diverticulum (Table 1). Ultrasound is a non-invasive simple examination with low intensity, high frequency, low price, and no damage to the human body, and a simple operation procedure. The main disadvantage is that it is difficult to distinguish calyceal diverticulum from a simple renal cyst. Assimos described that measurement of the volume change of the calyceal anechoic area before and after urination could assist in the diagnosis of calyceal diverticulum [18]. Calyceal diverticula and its narrow tubes can be clearly seen by retrograde pyelography, but retrograde intubation is an invasive procedure that can easily induce retrograde infection. IVP has a high detection rate [19]; moving from adjacent calyces to the channel between the cyst and the renal collecting system and then to the diverticulum, the density of contrast medium increases gradually. If the tube between the diverticulum and the collecting system is very narrow and the calyceal diverticulum cannot be found by IVP, the chances of misdiagnosis are high. Multi-directional and multi-angle photography, dynamic observation, or delay tracking radiography under fluoroscopy could improve the detection rate of calyceal diverticulum [20]. The images of calyceal diverticulum on renal CT scans are very similar to those of a renal cyst, and furthermore, the CT scan can accurately localize the diverticulum and estimate the amount of overlying renal parenchyma and its relation to surrounding structures [21]. In contrast-enhanced CT scans of the kidney, the narrow channel between the diverticulum and the collecting system obstructs the excretion of contrast agent, which gradually accumulates in the diverticulum. The density of the focus increases continuously for a long time during the delayed scan, which is a typical characteristic of calyceal diverticula. Another characteristic of calyceal diverticula is the presence of liquid stratification in the diverticulum. If the intrapelvic contrast agent cannot enter the diverticulum, the delayed scanning of the diverticulum without the contrast agent can easily lead to the misdiagnosis of renal cyst.
Advantages and disadvantages of diagnostic methods for calyceal diverticula
The first patient underwent delayed IVP and CT scans without deposition of contrast media in the diverticulum. Due to the narrow passage between the diverticulum and the calyces, or the poor secretory function of transitional epithelial cells in the diverticulum wall, the patient had no deposition of contrast media in the diverticulum. Combining with the patient’s medical history, it was preoperatively highly suspected we were dealing with a calyceal diverticulum. However, IVP, urinary color Doppler ultrasonography, and renal CT scan plus enhancement all indicated the presence of a renal cyst (Figs. 1, 3, and 4). In order to make the diagnosis of calyceal diverticulum, a cystic fluid puncture was performed by bedside ultrasonography before surgery, and the fluid CR level was measured; a CR level of 2529μmol/l was found, which was significantly higher than the serum level (serum CR in males < 97μmol/l). When we injected methylene blue through the ureteral catheter during operation, we found the calyceal opening where methylene blue flowed out, confirming communication between the cyst and the renal collecting system.
Calyceal diverticula should be differentiated from simple renal cysts (Table 2), cystic renal cell carcinoma (CRCC), renal tuberculosis, hydronephrosis and renal tumors. The images findings of simple calyceal diverticula and renal cysts are highly similar, hence misdiagnosis rate is relatively high. CT images of simple renal cysts have the following characteristics. Firstly, the boundary of the cyst is clear, thin and smooth. Secondly, the fluid in the cyst is homogeneous and of low density (fluid of high density is more common in cystic fluid with high protein levels or cystic hemorrhage). Thirdly, no enhancement of the cystic wall is observed on enhanced CT scans. CT scans of cystic renal cell carcinomas showed a low-density lesion similar to a cyst, with one or more cysts [22, 23]. The cystic wall or septal nodule, and irregular enhancement of the nodule can be seen on enhanced scans. Renal tuberculosis cavities can be multiple and irregular in shape, and erosion-like changes of calyx nephrons can be found, where progressive enlargement usually occurs. The patients generally have a history of tuberculosis and present with tuberculosis such as low fever and night sweats. Furthermore, purulent cells or tuberculosis acid-fast bacilli can be found in urine. The key points to distinguish hydronephrosis from calyceal diverticulum are the following. IVP shows (i) that the diverticulum is located around the calyx with compression and deformity of the pelvis and calyx, (ii) hydronephrosis with urinary tract obstruction such as bluntness or disappearance of the calyceal angle, and (iii) dilatation of the pelvis and calyx. The images of renal tumors show compression deformation, and a filling defect of the pelvis and calyx was observed in IVP [24, 25]. The tumors were markedly enhanced and the blood flow signal was visible on contrast-enhanced CT scans; the diagnostic accuracy of CT scans for renal tumors can be as high as 97.7% [13].
Differential diagnosis and treatment between renal cysts and calyceal diverticula
Calyceal diverticula are usually asymptomatic and requires no treatment, but it may cause symptoms such as lumbago, hematuria or urinary tract infections, so that intervention may be necessary. Calyceal diverticular calculus patients are at risk of progression, and many patients need active management. The main principles of surgical management of calyceal diverticulum are the following: firstly, closing the calyceal neck; and secondly, preventing urine reflux and enlargement of the calyceal neck, strengthening the drainage of urine. The size and location of calyceal diverticulum can influence complications such as infection and stones, which determine the choice of treatment options [26, 27].
Patient selection, the characteristics of the diverticulum, and the surgeon expertise will play a role in the decision-making process. Multiple treatment options, such as open surgery, extracorporeal shock wave lithotripsy (ESWL) [10, 28], retrograde endoscopic [29, 30] percutaneous nephrolithotomy (PCNL) [18], and laparoscopy [31] have been described for the management of this uncommon urological condition. No two treatments have the same success rate and complication rate. The goal in all of these surgical procedures is enlargement of the diverticular neck (or diverticulum ablation without dilation of the infundibulum) to avoid recurrence [6, 32] and treatment of stones at the same time.
Open surgery is less often employed in the clinic, but it is still used for the cases that are difficult to deal with by minimally invasive surgery. ESWL in the treatment of stone-bearing calyceal diverticula has the advantages of small trauma and high acceptance of patients, but it has the disadvantages that stone discharge is difficult, so it provides stone-free rates below 20% at short-term follow-up [32]. This method is unable to fix the underlying stenosis of the calyceal diverticulum, so it has a high recurrence rate of symptoms and stones compared with other techniques.
Percutaneous nephroscopy is an effective method for the treatment of calyceal diverticulum, especially with a concomitant large stone burden [29]. This method is commonly used for the treatment of diverticula in posterior renal calyces, and it provides high stone-free rates (87.5– 100%) and obliteration rates of the diverticular cavity (73– 100%) [5, 26]. Rates of complications such as bleeding may increase if the puncture in the treatment of anterior diverticula travels a long distance and transverses through the renal parenchyma. Percutaneous nephroscopy can be used in the treatment of upper and middle calyx diverticula. Generally, retrograde endoscopy is technically feasible in 70– 95% of stone bearing calyceal diverticula [33, 34].
Flexible ureterorenoscopy is a reasonable minimally invasive treatment option for patients with locations in the upper or middle calyceal diverticula with calculi of diameter less than 1.5 cm and when the diverticular neck is accessible. It is more effective than ESWL monotherapy and less traumatic than PCNL or laparoscopic. It cannot be used in the patients who has a lower pole diverticulum or a very narrow calyx neck orifice that cannot be dilated at the same time, leading to a relatively high recurrence rate. Other disadvantages of flexible ureteroscopic surgery include difficulties in identifying the orifice and a low clearance rate.
Laparoscopy is a more useful approach for anterior, large diverticula and for cases with a history of unsuccessful endourologic management of diverticula. The advantage of laparoscopic surgery is that it can deal with diverticula and stones simultaneously and cure the pathological mechanisms behind diverticulum formation. However, it is not suitable for patients with a thick diverticulum wall or a previous history of kidney surgery or trauma. Some symptomatic calyceal diverticula can be effectively treated by using a minimally invasive robotic approach in some hospitals with robotic surgical system [35]. Akca et al. [36] reported their experience with a single center case series on robotic partial nephrectomy for calyceal diverticula. This surgical procedure is used for cases where the management by endourologic or ESWL treatment was unsuccessful.
Some cases of calyceal diverticulum are misdiagnosed as simple renal cyst, which occur occasionally in the clinic. The lining of the cyst is fibrocollagenous tissue or is comprised of pavement epithelium cells in the cases of a renal cyst. Calyceal diverticula are lined with transitional epithelium and communicate with the collecting system through an infundibulum. Some patients are misdiagnosed and laparoscopic unroofing of the renal cyst is carried out, which has led to some complications such as urinary leakage post-operatively. Not only does this increase patients’ suffering but it also increases treatment costs. Our first patient was diagnosed with a simple renal cyst and underwent laparoscopic de-roofing of renal cyst, percutaneous aspiration and alcohol injection. However, there was no urinary leakage after surgery, because the channel between the collecting system and the diverticulum was very small. The calyx neck orifice of the patient was very narrow, so the guide wire could not pass through it at first. It is not excluded that this is related to the sclerosis of the renal cyst puncture by other hospitals in the past.
In the first patient, the delayed contrast enhanced CT scans of the kidney failed to detect a significant concentration of contrast medium in the diverticulum preoperatively, and the opening of the diverticulum could not be found during the operation. After injecting methylene blue into the diverticulum through the ureteral catheter, the diverticulum opening could still not be found under the guidance of the guide wire. All the above preoperative examinations and intraoperative findings suggested that the channels between the diverticulum and the collecting system were extremely narrow.
A calyceal diverticulum is similar to renal cysts in imaging (Table 3). The clinical incidence of renal cysts is high, while the incidence of calyceal diverticula is significantly lower than that of a simple renal cyst. It is important for both the uroradiologist as well as the radiologist to be familiar with their appearances, thus avoiding diagnostic uncertainty and unnecessary investigation for suspected complex renal cysts. When the clinical symptoms or imaging features of calyceal diverticula are atypical, clinicians or radiologists are liable to misdiagnose. A poor treatment plan will damage the physical and mental health of the patient. The first patient relapsed in a short time after multiple treatments in many hospitals. Doctors and radiologists should pay attention to the possibility of calyceal diverticula and adopt targeted inspection methods. The first patient’s renal cystic lesions were more than 60 mm in diameter, no concomitant calculi were found in the diverticulum, no abnormalities were found in our urine routine examinations and urine culture, and the diagnosis of a simple renal cyst was made by ultrasound, CT, and IVP many times in other hospitals, which were treated by laparoscopic renal cyst unroofing and multiple puncture sclerotherapy of renal cysts, and hence, recurrence occurred many times within a short time after operation. The above information suggests that the patient was likely to suffer from calyceal diverticulum. The patient demanded to be treated for the calyceal diverticulum when he came to our hospital. Preoperative puncture was performed by bedside ultrasonography. The puncture fluid was measured for CR and confirmed to be urine. Therefore, the preoperative diagnosis of calyceal diverticulum was made.
Image characterization between single renal cysts and calyceal diverticula
The treatment principles of renal cysts and hydronephrosis are totally different. Renal cysts are located in the renal parenchyma or pararenal pelvis and are not connected with the collecting system. Cysts do not contain urine [20]. Hydronephrosis relates to the collecting system, which is a secondary change caused by urinary obstruction. It is manifested by dilatation of the pelvis and the calyx to different degrees. The component of hydronephrosis is urine. Clinically, if a calyceal diverticulum is misdiagnosed as a simple renal cyst, an unroofing operation can cause some complications such as urinary leakage and infection. In order to avoid misdiagnosis, we need to objectively and comprehensively review as many studies as possible and consider all diagnoses in the differential. In addition to identifying suspicious details pointing to a diverticulum, a variety of examination methods should be combined, such as CT enhanced delayed scanning, IVU multi-directional photography and delayed tracking photography, and ultrasound observation of volume changes in anechoic areas before and after urination. The presence of a calyceal diverticulum can also be judged by extracting cystic fluid (guided by ultrasound) and measuring CR levels. If the CR in the hydrocele is much higher than that in serum, urine should be considered. All above methods can improve the diagnostic rate of calyceal diverticulum and avoid misdiagnosis.
In summary, to distinguish calyceal diverticula from symptomatic renal cysts, color Doppler ultrasonography, and CT plain scan plus enhanced scan are routinely performed. Delayed scan is required for patients at early stage with highly suspected calyceal diverticulum. If it is difficult to diagnose before operation, puncturing the hydrocele under the guidance of B-mode ultrasound could aid for the further diagnosis preoperatively, and taking the drainage fluid to detect CR levels can aid in the further preoperative diagnosis of calyceal diverticulum. Intravenous injection of methylene blue through a ureteral catheter also aided in the diagnosis before operation. Either calyceal diverticulum or symptomatic renal cysts require surgical intervention.
Conflict of interest
None of the contributing authors have any financial or personal relationships with people or organizations that could inappropriately influence work on this article.