
Abstract
PURPOSE:
To avoid Iatrogenic ureteral injury during retroperitoneal laparoscopy for large renal cyst (diameter > 70 mm), we present two cases of iatrogenic ureteral injury and discuss their clinical courses and final outcomes.
PATIENTS AND METHODS:
Two male patients (47 years old and 74 years old) with large left simple renal cysts underwent a retroperitoneal laparoscopic operation to treat the cysts. In the first patient, the left proximal ureter was partially transected (Grade 3) during the operation. The injury was identified intraoperatively. The transection was managed with a primary ureteroureterostomy (end to end) along with a double J ureteral stent. In the second patient, the left proximalureter was partially transected (Grade 4). However, the injury was unrecognized postoperatively for two days. After recognition of the complication, the injury was managed with an early primary ureteroureterostomy, which followed a failed attempt to place ureteral stent endoscopically.
RESULTS:
In the first patient, a postoperative urinary leakage developed and lasted for 13 days. During long term follow-up of the first patient after the urine leak resolved, there were no reports of pain in the lumbar region or other discomfort. No recurrence of the renal cyst occurred, which was confirmed with an ultrasound at one year postoperatively. In the second patient a ureteral fistula and severe perirenal infection occurred and lasted for 86 days. The patient ultimately underwent a left nephrectomy after conservative management for this surgical complication failed. This patient developed a chronic wound infection that lasted for 3.14 months following the nephrectomy. During follow-up post nephrectomy, the patient developed stage 3B moderate chronic kidney disease (CKD) (GFR = 30 –44 ml/min).
CONCLUSIONS:
For single large (diameter > 70 mm) renal cysts located at the lower pole of the kidney, it is recommended to not completely dissect out and mobilize the entire renal cyst for cyst decortication in order to avoid injuring the ureter. Iatrogenic ureteral injury increases the risk of readmission and serious life-threatening complications. The immediate diagnosis and proper management ureteric injury can reduce complications and long term sequalae.
Introduction
Approximately,
The best method for avoiding iatrogenic ureteral injury is still a matter of debate. Ureteral injuries usually involve the distal ureter [1, 9]. Ureteroscopy is a common cause of iatrogenic ureteric trauma. The post-ureteroscopic lesion scale (PULS) may standardize intra-operative traumatic findings during ureteroscopy [8]. Iatrogenic injury of the proximal ureter has been rarely reported as a severe complication of retroperitoneal laparoscopic surgery.
Renal cysts are classified according to the Bosniak classification. They are classified as simple (Bosniak type I and II) or complex (Bosniak type IIF and III and IV) cysts. Laparoscopic decortication or marsupialization of the simple renal cyst (Bosniak type I and II) is a relatively straight forward operation. However, if one does not pay attention to certain circumstances, such as large cyst (diameter > 70 mm) and cysts located at the lower pole of the kidney with adhesions to adjacent tissue one may cause a proximal ureteral injury. Here, we present two cases of ureteral injury during retroperitoneal laparoscopic decortication of simple renal cysts (Table 1). The first patient’s iatrogenic injury of the proximal ureter was fortunately identified intraoperatively, we placed a double-J stent after a ureteral-ureteral primary anastomosis. The second patient unfortunately, had an unrecognized iatrogenic ureteral injury that was identified on the third postoperative day. Subsequently, the patient went on to receive an early open primary repair of the ureter. Unfortunately, a ureteral fistula with a severe perirenal infection developed postoperatively. This resulted ultimately with the involved kidney being removed after conservative therapy failed.
Summary of Iatrogenic Ureteral Injury due to retroperitoneal laparoscopic unroofing of simple renal cysts in two cases
Summary of Iatrogenic Ureteral Injury due to retroperitoneal laparoscopic unroofing of simple renal cysts in two cases
Case 1
The patient was a healthy 47-year-old male. He was hospitalized due to left lumbago for more than 15 months. As part of the work up for his chronic severe left flank pain, we obtained a computerized tomography (CT) scan of the abdomen with and without intravenous contrast enhancement. The scan revealed a large left renal cyst (Bosniak type I) located in the lower pole measuring 71 mm in diameter (Fig. 1a). He did not have diabetes mellitus and hypertension. The urinalysis test was normal. All serum chemistries were within normal limits.
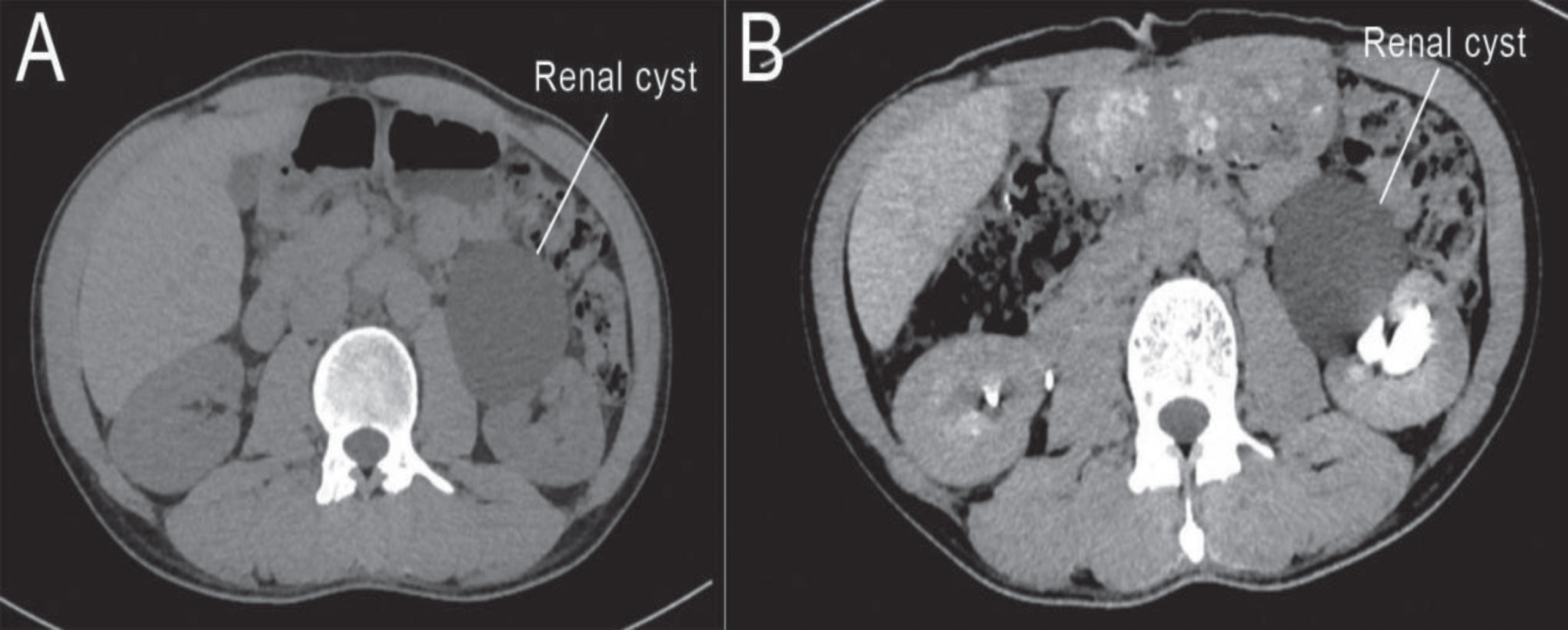
The kidney CT scan shows the left single large sole renal cyst located at the lower pole (71 mm in diameter) in Case 1.
Renal cyst marsupialization using a laparoscopic approach was offered to the patient for definitive management of the cyst which was felt to be the cause of the chronic pain. Patient agreed to proceed with the procedure after informed consent was obtained.
We performed a retroperitoneal laparoscopic renal cyst decortication. During the operation after completely mobilizing the lower pole cyst and unroofing it, we identified a ureteral injury while evaluating the surgical field. The ureter was found to be partially injured (about a 40% partial transection, Grade 3, based on post-ureteroscopic lesion scale [8]) (Figs. 1b, c), a 6 Fr double-J stent was placed during the repair of the ureter. The ureter was repaired with a primary end to end anastomosis, watertight mucosa-to-mucosa reapproximation, using interrupted No.4-0 absorbable suture. This was also performed laparoscopically and the sutures were placed one centimeter (cm) apart. A retroperitoneal drain was also placed. A postoperative urinary leak occurred and lasted for 13 days. Creatinine of this fluid was elevated confirming the diagnosis of urine leak. A plain film of the abdomen (KUB) and abdominal CT scan were done (Fig. 1d). Histologic examination revealed the lining of the cyst consisted of fibro collagenous tissue. The double-J stent was removed cystoscopically after the leak resolved at 6 weeks post-operation. The patient was followed up with routine urinalysis and serum creatinine. All were within the normal ranges. Intravenous pyelography (IVP) at six months post-operation was normal. There were no reports of pain in the lumbar region or other discomfort at 6 months. At one-year post-operation no lower pole renal cyst was identified using renal ultrasonography.
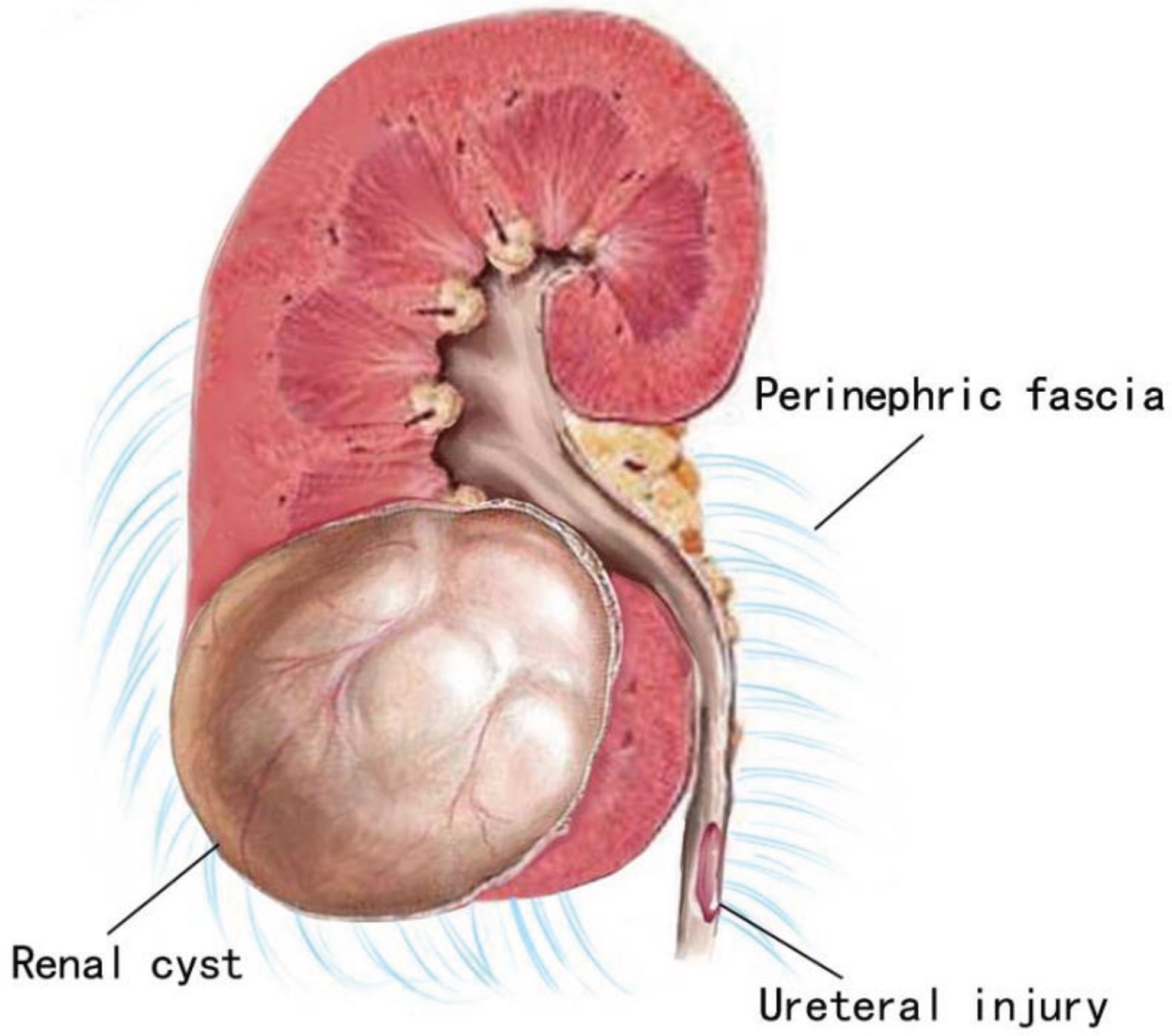
Posterior view of left upper urinary tract system shows a renal cyst at the lower renal pole and the injured ureter (Grade 3) during retroperitoneal laparoscopy in Case 1.

The left ureter was partially injured (Grade 3) at the segment of proximal ureter due to partial transection in Case 1.
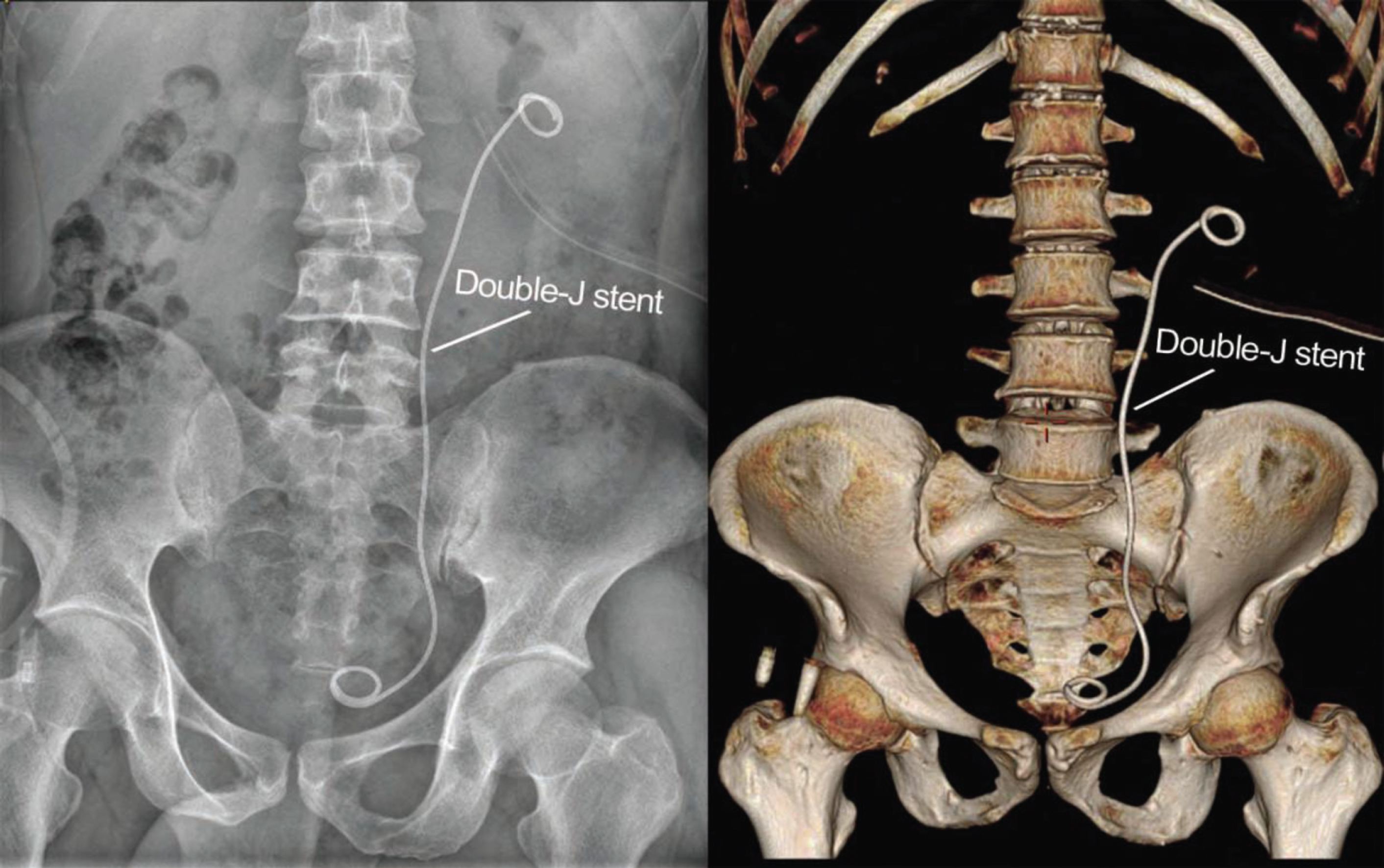
The KUB (left) and CT scan (right) confirm the upper Double-J stent is located inside the left ureter in Case 1.
A 74-year-old male patient was admitted for left flank pain. The spiral three -dimensional CT reconstruction of the urological system (CTU) identified a left renal cyst (Bosniak type I) located at the lower pole measuring 128 mm in diameter. There were also multiple smaller cysts in the right kidney and prostatic hyperplasia incidentally identified. The patient also suffered from hypertension but denied diabetes mellitus. The level of serum prostate specific antigen (PSA) was 12.64 ng/ml. All other serum chemistry panels were within normal limits. Urine microscopy demonstrated microscopic hematuria.
After informed consent, the patient underwent a retroperitoneal laparoscopic decortication of the large lower pole renal cyst which included complete mobilization of the cyst. A retroperitoneal drain was also placed. The daily drainage from the drain was 270 ml and 400 ml day 1 and 2 after operation. Because of the volume and color, the drainage was presumed to be urine. Retrograde placement of a 6 Fr double-J stent via cystoscope without fluoroscopy was performed. Then a plain film of the abdomen (KUB) and abdominal CT scan were performed. The X-ray examinations showed part of double-J stent outside of the ureter (Fig. 2a), which clearly indicated a large ureteral injury that was not properly stented. An open surgical exploration was performed on the third day after initial retroperitoneal laparoscopy. The partially transected ureter was identified (about 75% partial transection, Grade 4) (Fig. 2b) and the stent was outside of the proximal ureter. A 6 Fr double-J stent was placed in conjunction with an end to end primary ureteral anastomosis and it was performed in a watertight mucosa-to-mucosa fashion with interrupted No. 4-0 absorbable sutures. The sutures were placed one cm apart. A drain was placed peri-renally. Histologic examination of the cyst wall revealed no obvious lining epithelium, and the blood vessels of cyst wall were dilated and congested, with an inflammatory cell infiltrate. Unfortunately, there was continuous urine leakage from the drain that (ranged from 310 ml to 435 ml), and a small amount of purulent secretion from the wound both of which persisted for 86 days after the open surgical repair. An abscess had formed around the left kidney as well. The patient developed complaints of intermittent incision pain. He also developed a leukocytosis and elevated sedimentation rate without fevers and without chills. His vital signs were otherwise normal and stable. He did not have and new gastrointestinal complaints. Eventually an open left nephrectomy was performed to remove the chronically infected and fistulized ureter. During the operation, the ureteral fistula was confirmed, and the left kidney appeared to be atrophied being (82 mm×51 mm) compared to the right kidney (113 mm×67 mm, measure by ultrasound).

The KUB (left) and CT scan (right) show the Double-J stent coursing outside the left proximal ureter terminates outside of the renal collecting system day 3 after initial retroperitoneal laparoscopy in Case 2.
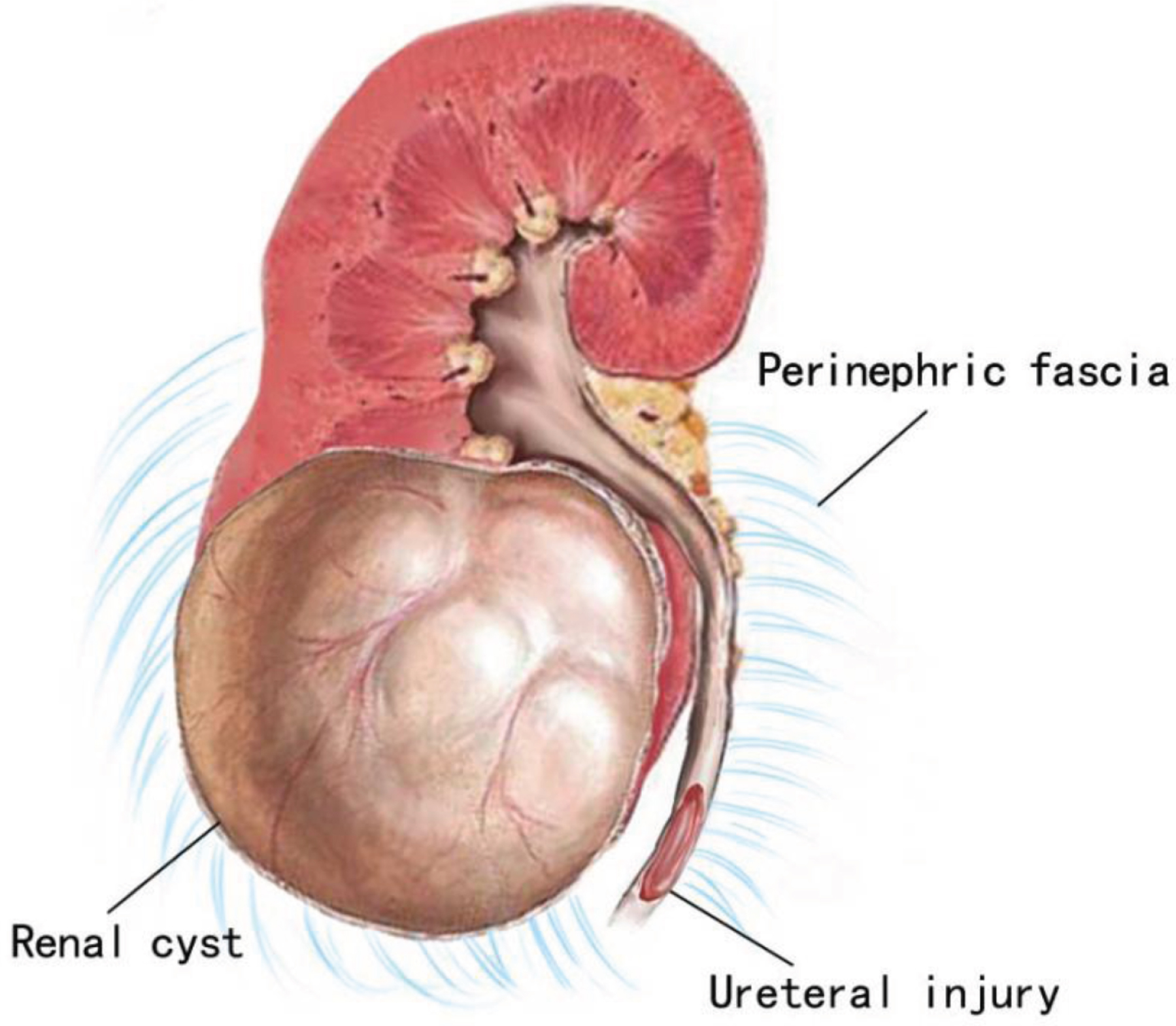
Posterior view of left upper urinary tract system shows a large sole renal cyst (128 mm in diameter) located at the lower renal pole and the injured ureter (Grade 4) during retroperitoneal laparoscopy in Case 2.
Histologic examination of the left kidney revealed extensive coagulative necrosis, inflammatory cell infiltration and formation of multiple abscesses. The patient had a wound infection that lasted for 3.14 months after nephrectomy, nontuberculous mycobacteria (NIT) was cultured from the fluid collected from the drain. During long term follow-up post nephrectomy, the patient developed elevated serum creatinine (CR) levels between 140 to 180μmol/l (serum CR levels men <133μmol/l). The calculated glomerular filtration rate (GFR) of the patient fluctuated between 31.25 ml/ (min×1.73 m2) and 42.35 ml/(min×1.73 m2), which is consistent with stage 3B moderate chronic kidney disease (CKD) (GFR arrange between 30 and 44 ml/min). One year after nephrectomy, transrectal ultrasound-guided prostate biopsy was performed to evaluate the elevated PSA and pathological results showed a benign hyperplasia of prostate. Up to now, the patient has been followed for more than four years without further complication and stable but poor renal function.
Due to their close proximity to vital abdominal and pelvic organs, the ureters are highly susceptible to iatrogenic injury. In fact, an estimated 75% of all ureteric injuries are iatrogenic [12–14]. More than half of operative ureteral injuries occur in gynecological and obstetric surgery. This is largely attributed to the close position of the ureters to vascular structures, combined with their course along virtually every level of the retroperitoneum and upper pelvis [2]. In urologic procedures, ureteroscopy is the most common cause of ureteral injury. The ureter is at risk for injury from ureteroscopy at the three anatomical ureteral segments (ureterovesical junction, pelvic brim and the ureteropelvic junction) [3].
Proximal ureteral injury is rarely reported in retroperitoneal laparoscopic surgery. However, the ureters are difficult to identify during surgical procedures due to their close adherence to the posterior peritoneum and due to other confounding variables, such as unexpected congenital anomalies (e.g. ureteral duplication) [8]. In high-risk procedures, prophylactic ureteral catheterization can be used to detect ureteral injury early [15]. However, the efficacy of ureteral catheterization is a debatable point [16]. The prevention of ureteral injury during laparoscopic procedures is not addressed in the guidelines on urinary trauma by the American Association of Urology (AUA) [16]. Preoperative ureteral catheter placement has not been associated with a significant reduction in the ureteral injury rate to date. However, it does help to improve early identification and timely repair [4, 17]. Some scholars have speculated that preoperative catheter/stent placement may actually increase the risk of ureteral injury, because it may cause the ureter to deviate from its normal anatomical location and reduce its mobility [18]. In our study, if prophylactic ureteral catheter/stent had been performed for the patient in case 2, the ureteral injury may have been identified intraoperatively. An immediate repair could have been then undertaken and ultimately prevented the loss of the left kidney. This could suggest that in high-risk simple renal cyst decortication surgery (e.g., huge simple renal cyst or cysts located at the lower pole of the kidney), pre-operative ureteral catheter/stent should be performed.
Most iatrogenic ureteric injuries are not recognized intraoperatively and are diagnosed late when patient becomes symptomatic [7, 19]. Given that intraoperative detection allows for immediate repair with significantly lower complication rates, the implication of this work is that every effort should be made to detect these injuries before leaving the operating room2. Risk factors for iatrogenic trauma include conditions that alter the normal anatomy, e.g. prior surgery, advanced malignancy or radiation, endometriosis, anatomical abnormalities, and massive space occupying lesions [6, 21]. In our study, one patient’s injury of the ureter was recognized and repaired intraoperatively; the second patient’s ureteral injury was unrecognized and repaired three days post-operation.
The presenting signs of ureteric injury are often not specific, and diagnostic tests often are specific but not sensitive [22]. Ureteral injury must be suspected in the postoperative period when upper urinary tract obstruction, acute renal insufficiency or sepsis appear. Other clinical signs include delayed flank pain, drain urinary leakage, hematuria, fever, urinoma or uremia [23].
Unrecognized ureteral injury results in high readmission rate as well as life threatening medical conditions, including sepsis, acute renal failure or renal necrosis. Thus, early detection and early diagnosis are very important. Several imaging studies have been used in the diagnosis of ureteral injury. Ultrasound (US) is a non-invasive simple examination. However, the US is generally not useful, except in showing a urinoma or hydronephrosis, all which suggest a delayed ureteric injury, so it is of limited use in the acute setting [24]. When the ureteral injury is suspected postoperatively, CT scan with delayed excretory phase should be performed [15, 16]. Findings on CT urogram include ureteral contrast extravasation, urinoma, hydronephrosis, and peri-renal fluid collection. In case 2, the ureteral injury was suspected due to leakage of urine and diagnosed was confirmed by CT urogram (Fig. 2a). Retrograde or antegrade pyelography is also a sensitive radiographic test for ureteral injury, while also allowing simultaneous placement of a stent. Unrecognized ureteral injury occurred in case 2, and failure of proper retrograde ureteric stenting was confirmed by abdominal CT scan (Fig. 2a). Thus, the retrograde ureteric stenting is often unsuccessful [2, 25].
The close proximity of the ureters to important abdominal and pelvic structures increases the risk of iatrogenic injury. Therefore, tumors or cysts in the lower pole of the kidney make the ureter susceptible to damage during laparoscopic retroperitoneal surgery. The following signs should be considered to make the diagnosis of ureteral injury following retroperitoneal laparoscopy: (1) prolonged high output from drains; (2) elevated creatinine in fluid collections [26], if it is significantly higher than the serum creatinine level, the drainage is considered urine, which can assist in the diagnosis of ureteral injury. In this study, creatinine (CR) level of drainage was 9499μmol/l (serum CR levels men <97μmol/l) in case 1, indicating that the drainage was urine; and (3). Intravenous urogramy (IVU) or enhanced CT scanning can tell the urine leakage by contrast agent leakage from the affected kidney ifneeded.
Surgical decortication procedures via laparoscopy is the most commonly used method in the management of hepatic cystic lesions [27]. It is not recommended to cut a big open of hepatocyst to avoid the liver tissue including bile ducts. This strategy should also work well in the treatment of kidney cyst(s). Our study showed that over dissection and trying to make a large sized defect of the kidney cyst increases the risk of surgical complications, such as ureter injury or kidney damage, causing urine leakages, kidney infections. It requires the extra surgical interventions and even results the entire kidney loss.
The treatment of ureteral injury depends on the type, location, grade of injury, the time of diagnosis and the patient’s overall clinical condition [28]. The European and American guidelines adopted very similar approaches regarding the timing at which to repair ureteral trauma [15, 16]. Essentially, repair should be attempted intraoperatively in stable patients if the injury is identified intraoperatively because delayed diagnosis results in higher rate of complications (i.e. infection, urinary leakage, stricture, etc.) and renal impairment. Ureteral injuries identified after a significant delay are best managed initially by percutaneous nephrostomy (PCN) drainage or endoscopic ureteric stenting [1, 28–30]. Placing a PCN drains are usually safer and more universally accepted. Retrograde ureteral stenting is often unsuccessful (50–95%) and should be attempted only for grade1 and grade 2 injuries [8, 32]. The success rate of antegrade stenting is high, particularly after a few days of proximal urinary diversion [33]. In case 2, we were unsuccessful in placing a stent retrograde. Perhaps if we had placed a percutaneous nephrostomy tube instead then maybe we could have spared a second and third operation because a stent could have maybe been eventually placed in an antegrade fashion.
No specific recommendations exist on the optimal stenting duration. Depending on the grade of injury, ureteral stents should be kept for different lengths of time [34]. Nevertheless, there is a tendency to leave the stent in place for a minimum of six weeks [22]. In cases of ureteral contusion with a leak, percutaneous nephrostomy and ureteral stenting for at least six weeks proved to be effective in over 80% of cases [35].
The most reliable method to avoid iatrogenic ureteral injury is adequate surgical exposure, meticulous surgical technique, moderate dissection of the renal cyst, and to identify the ureter throughout its course in the operative field [29]. If the injury to the ureter is suspected intraoperatively, the ureter must be meticulously examined. Once the injured ureter is exposed, the general principles for ureteric reconstruction include (1) careful ureteral mobilization (with care to preserve the adventitia); (2) debridement of devitalized tissue [11]; (3) watertight mucosa-to-mucosa anastomosis with absorbable sutures [7, 36]; and (4) ureteral drainage (internal Double J stent or PCN drainage) [17, 37].
In our study, two cases of proximal ureteral injury during retroperitoneal laparoscopic decortication of renal cysts were reported. The characteristics of these cases including: (1) renal cysts located in the lower pole of the kidney; (2) large cyst (diameter >70 mm) [38], and (3) there are adhesions in perirenal tissue. Therefore, if the patients have the above conditions, to avoid damage to renal parenchyma, ureter or peripheral vessels when excessive free adherent tissue is present, the methods of laparoscopic decortication of renal cysts in the previous literature are as follows [39]: cutting along the junction between the cyst wall and 5 mm away from the renal parenchyma. When the renal cyst is unroofed, up to 2/3 of the renal cyst wall is removed to make the cyst completely open. It is unnecessary to dissect free the entire renal cysts and periureteral tissue, which will avoid injuring, the surrounding tissues.
In our study, the first patient had the urine leakage after repairing the ureter and the leak resolved following conservative management which included aperirenal/retroperitoneal drain. In case 2, the ureteral injury was identified due to leakage of urine and therefore the repair was delayed. Development of a urinary fistula and repeated infection after repair, progressing gradually to renal necrosis ultimately led to kidney loss. These two patients had completely different disease outcomes. This was because of the following factors: (1) different degrees of ureteral injury (Grade3 vs. Grade4), (2) the time of detection of ureteral injury is different (intraoperative recognition vs delayed diagnosis), (3) the two patients are different ages (47 years vs. 74 years), and (4) the perirenal tissue infection was not effectively controlled in case 2.
The lessons we learned in these two cases are that (1) it is not necessary to dissect the tissue around renal cystic or completely free the renal cystic when unroofing, in order to avoid damaging the ureter and the surrounding vascular tissue; (2) preoperative prophylactic ureteral catheterization does not necessarily assure preventing ureteric injury, but it can assist in intraoperative recognition; and (3) the prompt repair of ureteric injuries is preferred, and early intervention with endourological procedures can improve outcomes. Retrograde stenting of the ureter is often unsuccessful for the delayed diagnosed ureteric injury. In cases of delayed diagnosis, percutaneous drainage and ureteral stenting should be performed simultaneously, following a ureteroneocystostomy.
Conclusion
Iatrogenic ureteral injury during retroperitoneal laparoscopic unroofing of simple renal cysts is rare. For single large (diameter >70 mm) renal cysts located at the lower pole of the kidney, and with adhesion of the surrounding tissues, measures to prevent ureteral injury or to reduce the incidence of complications include (1) minimizing surgical exposure with careful surgical technique, (2) visual identification of the ureters during surgery, and (3) use of pre-operative prophylactic stents/ureteral catheters.
Conflict of interest
None of the contributing authors have any financial or personal relationships with people or organizations that could inappropriately influence work on this article.
Footnotes
Acknowledgments
This study was supported by the Shenzhen Foundation of Science and Technology (No. JCYJ20170307094908637).