
Abstract
INTRODUCTION:
Testicular infarction is a rare complication of prolonged epididymitis and may be misdiagnosed as testicular torsion. In this study, we present three cases of testicular infarction and discuss their clinical characteristics, imaging features and clinical management.
PATIENTS AND METHODS:
Three adult males with prolonged epididymitis presented with chronic unilateral testicular pain, tenderness, and palpable swelling, including left varicocele in one case and hydrocele in the other two cases. Patient’s symptoms were not relieved after antibiotic therapy. We analyzed the diagnosis, management, and outcome of these three cases of testicular infarction resulting from prolonged epididymitis. This includes the clinical characteristics, features of color doppler ultrasound imaging for diagnosis, and treatment strategy for testicular infarction from prolonged epididymitis.
RESULTS:
Complete blood count (CBC) indicated a small leukocytosis (10.6±0.4×109/L; normal arrange 3.5–9.5 WBC×109/L). Color doppler images demonstrated appropriate blood flow to areas of interest at patient’s initial visit. At follow up visit several months later, the increased blood flow was detected at the edges of the involved testes with no blood flow to the center. The sizes of the involved testis (27±4 ml) was significantly larger compared to the non affected side (17±2 ml) (p < 0.05). Unilateral simple orchiectomy was performed on the involved testis in all three cases. Grossly, abscess cavities with caseous necrosis were found at the center of the testicle and epididymis in two patients. Histopathologic examination showed chronic inflammation with lymphocytic and macrophage infiltration of the involved testicle in two cases. The third case stained positive for acid fast bacteria. Left varicocele disappeared postoperatively in one patient. No pain, wound infection or other discomfort were noted 12 months after surgery.
COMMENTS:
This series revealed that testicular infarction may result from inappropriately treated prolonged epididymitis. Epididymal tuberculosis should be considered in cases with epididymitis not responding to broad spectrum antibiotics. Testicular infarction induced by prolonged epididymitis is easily missed due to a lack of symptom changes. Color doppler images are helpful in the diagnosis. This usually presents as a decrease in blood flow at the center of the testis with the increased flow at the periphery differentiating this from testicular torsion.
Introduction
Epididymitis, inflammation of the epididymis, is most often caused by bacterial infections, including sexually transmitted infections (STIs) and occasionally by tuberculosis [1]. When the testicle is involved, it is termed epididymo-orchitis. Epididymitis most often occurs in males between the second and fourth decades of life. During this time frame the most common cause is STIs, however men affected by epididymitis after the age of 35 the most common causes are E. coli and other coliform bacteria [2]. Acute epididymitis is typically characterized by symptoms of epididymal swelling, induration, and exquisite tenderness to palpation and may also be accompanied by fever, chills, dysuria, lower urinary tract symptoms (LUTS). Epididymitis that lasts for more than six weeks or that recurs becomes classified as chronic epididymitis. Symptoms of chronic epididymitis might come on gradually. Sometimes the cause of chronic epididymitis isn’t identified. Meanwhile, similar symptoms can arise from other scrotal pathologies, including testicular torsion, trauma, inguinal hernia and testicular cancer, which make it difficult to identify epididymitis. Ultrasound examination in epididymitis presents as an enlarged and hypoechoic epididymis due to resulting edema. Color Doppler imaging shows increased blood flow corresponding to hyperemia, which is the key criterion for the diagnosis of acute epididymitis, however reactive hydroceles and scrotal wall thickening may also be found. Color doppler imaging shows increased blood flow corresponding to hyperemia, which is the key criterion for the diagnosis of acute epididymitis [3].
Testicular torsion is a surgical emergency which occurs when the spermatic cord, becomes twisted and reduces blood flow to the testicle causing sudden pain and swelling. Testicular torsion most often occurs in boys and young men [4]. Infarction due to epididymitis is clinically indistinguishable from testicular torsion with acute scrotal pain. Severe complications, such as: abscess and infarction, lead to orchiectomy if not diagnosed and treated properly [5].
Inappropriately treated may progress to involve the testis, spermatic cord, or prostate. One of the most catastrophic complications is testicular infarction, which is thought to occur due to inflammation and edema resulting in compression of the testicular vein, artery, and lymphatics [6, 7]. Conservative treatment of epididymitis means rest, local physiotherapy, regular observation and antibiotic therapy. Surgical management includes drain for the formed abscess and orchiectomy for necrosis due to infarction. However, when acute epididymitis is not treated promptly, it progresses to chronic epididymitis testicular that might develops to infarction [2, 8]. Thus, prompt diagnosis and treatment are critical in saving the affected testicle.
Testicular infarctions have been rarely reported as a severe complication of epididymitis. To date, few reports have focused on testicular infarction in the presence of prolonged epididymitis. The best method for treatment is still a matter of debate [4]. Here, we present three cases with epididymitis progressed into scrotal abscess and testicular infarction depicted on Color Doppler ultrasonography from September 2014 and September 2019 were retrospectively analyzed (Table 1). Patient inclusion criteria were as follows: (i) prolonged epididymitis (>1 month) presented with chronic unilateral testicular pain, tenderness, and palpable swelling; (ii) patients’ symptoms were not relieved after antibiotic therapy; (iii) the involved testis were confirmed infarction and unilateral simple orchiectomy was performed. The purpose of this study was to investigate the correct clinical management of prolonged epididymitis.
Summary of 3 cases with testicular Infarction due to prolonged epididmitis
Summary of 3 cases with testicular Infarction due to prolonged epididmitis
Case 1
A 29-year-old male with a past medical history of left sided acute scrotal pain and left varicocele diagnosed four years previously, presented with a low-grade fever (37.4°) and severely painful right scrotal swelling for 3 days. He denied history drugs use, prior STIs, diabetes mellitus, and hypertension. One month prior, the patient was admitted for a 2-day history of right scrotal swelling and a dull right sided pain. Scrotal color doppler ultrasonography confirmed increased testicular vascularity and swollen right epididymis, suggesting epididymitis (Fig. 1A). The patient was treated with a 3-day course of antibiotics and his symptoms resolved. The patient refused to continue treatment in the hospital and requested discharged.
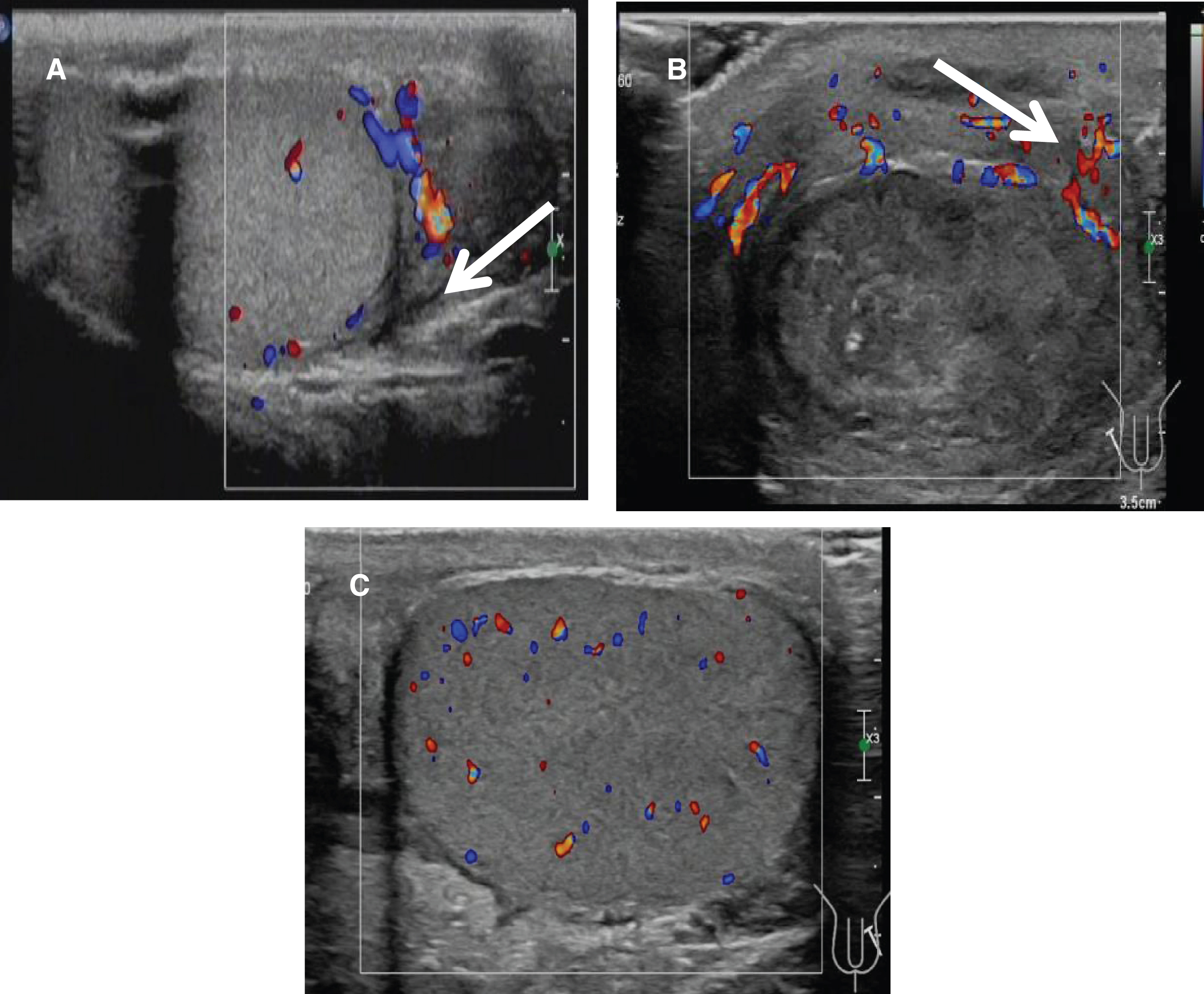
Color doppler signals in inflammatory epididymis in Case 1. (A) Increase blood flow signals (thick arrow) within the involved epididymis but decreased flow in the testicle at the acute phase (35 days prior to surgery); (B) Significantly increased blood flow in the right subcutaneous scrotum (thick arrow) but no flow within the right testicle (bottom) one day before surgery; (C) Blood flow was evenly distributed in the healthy left testis.
The patient returned home and received continuing antibiotics therapy for about one month at the local hospital. During his treatment course, his right scrotal swelling and pain recurred. The patient was re-admitted with worsening pain in the right hemi-scrotum 1 month later. Physical examination showed an enlarged, rigid, and painful right scrotum, with a markedly thickened scrotal wall. Repeat color doppler demonstrated left varicocele, and increased blood flow to the right subcutaneous scrotum, with no evidence of any blood flow within the right testis. There were two hypoechoic areas under the right scrotal skin, the largest of which was 18×8 mm, one of which has a sense of flow, the other has strong echo and gas is considered (Fig. 1B). Normal blood flow was seen in the contralateral testis (Fig. 1C). A small leukocytosis was noted at that time (12.2×10*9/L), blood potassium is 3.28 mmol/l and all other serum chemistry parameters were within normal limits. Based on the confirmation of the absence of blood flow on ultrasound, the diagnosis of right testicular infarction secondary to epididymitis was made.
The patient underwent immediate scrotal exploration. During surgery, the right testis appeared pale and no evidence of torsion. In combination with the imaging findings, the decision was made to conduct a right orchiectomy. A cavity with 40 mL of yellowish purulent pus at the center of the right testis and the pus material was sent for bacterial culture (Fig. 2.A). Laboratory test reported that multidrug resistant E. coli was detected in the pus specimen and a midstream urine sample. Histologic examination revealed inflammatory infiltration within the seminiferous tubules and interstitium with multiple micro-abscesses (Fig. 2B). On post-operative day 5 scrotal ultrasound revealed a normal left testis with an absence of varicocele.
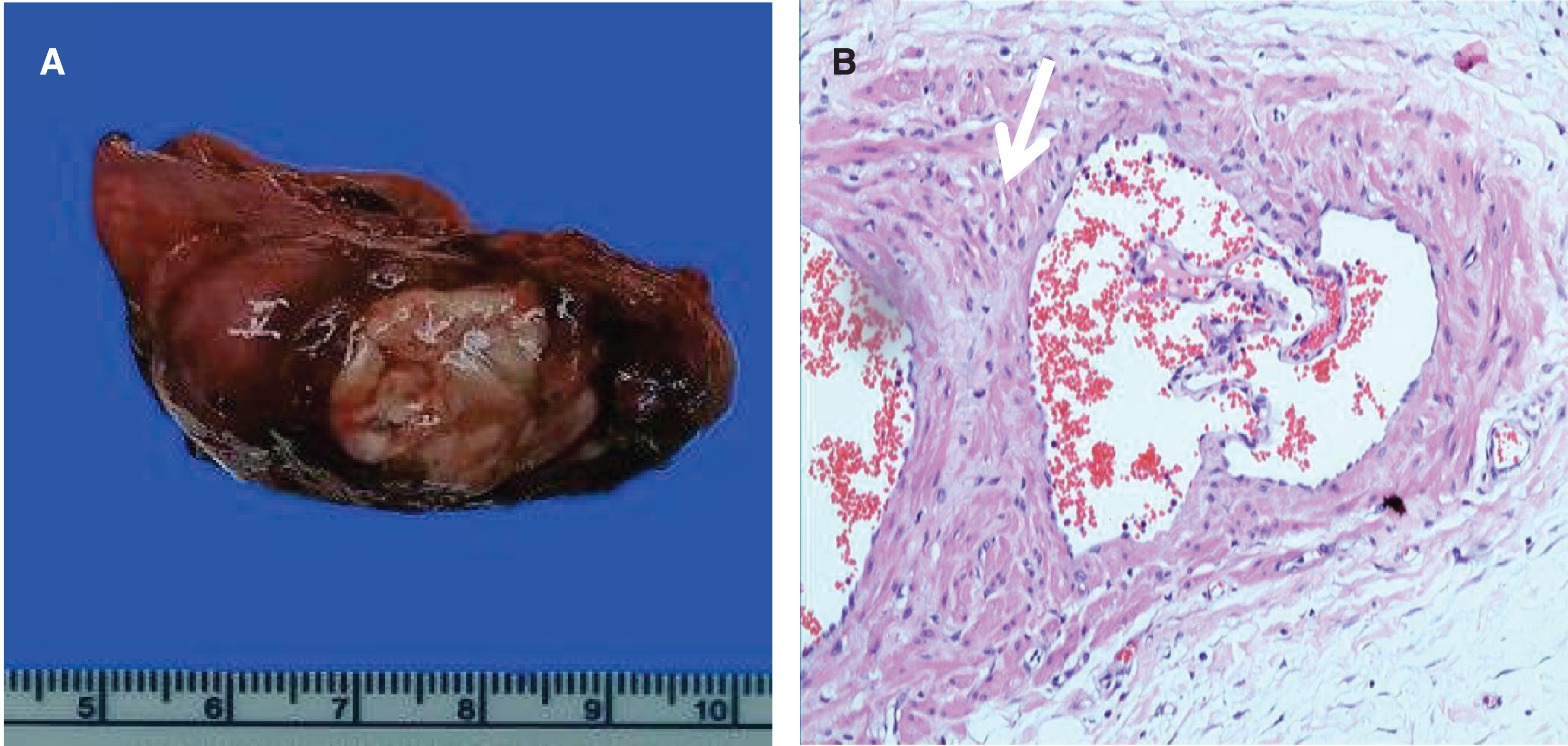
Gross specimen (right) and histological changes (left) case 1. (A) A purulent cavity at the cross section of the involvedepididymis and testis after unilateral orchiectomy. (B) Thick fibrous septum formation (thick arrow) with suppurativeinflammation and inflammatory cell infiltration (long arrow) in the purulentcavity (H & E stain, 200×).
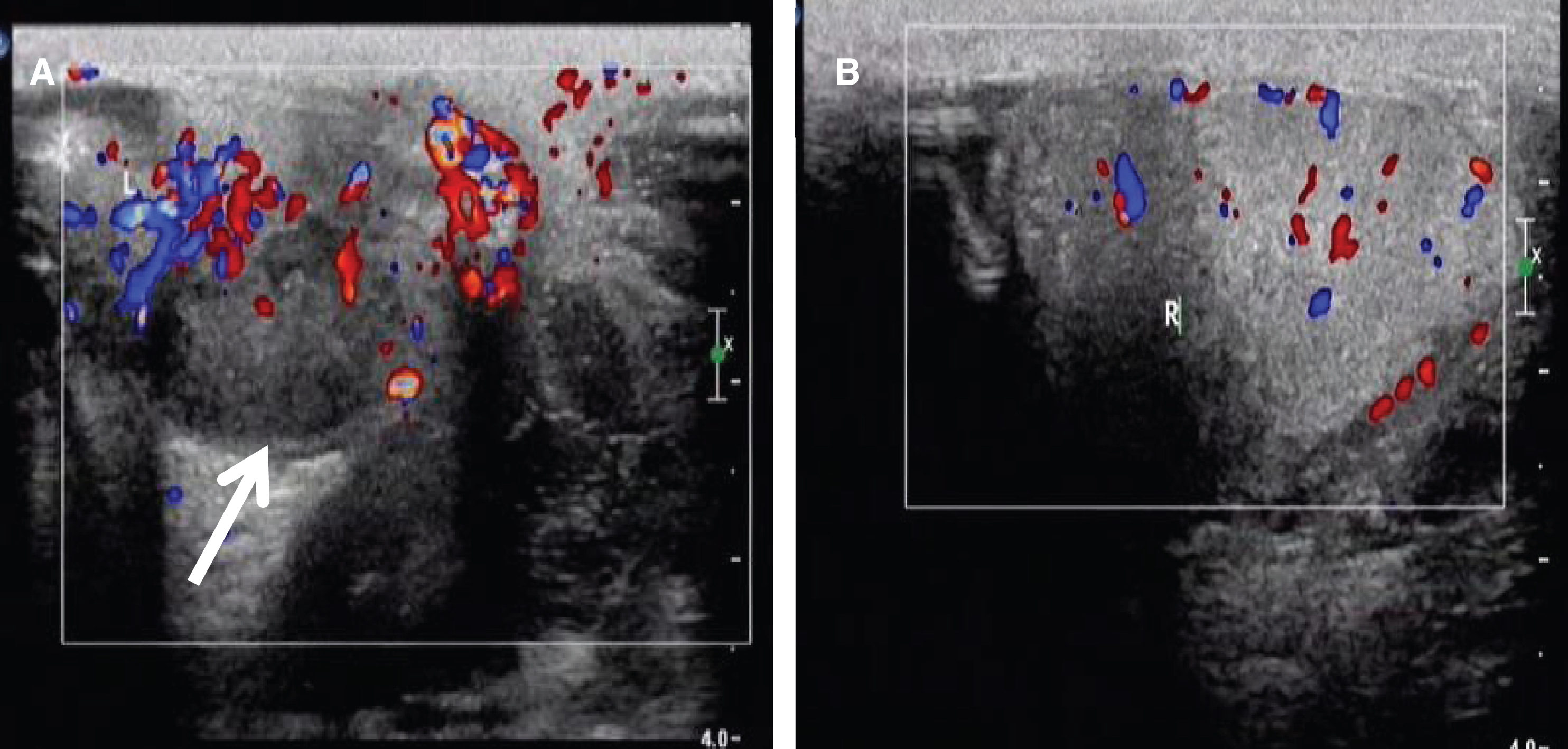
A 36-year-old male visited urological clinic because of the right scrotal dull pain for one month and turned to severe pain and scrotal swelling for 7 days. The patient denied prior history of STIs, diabetes mellitus, or hypertension. Physical examination showed an enlarged and painful right scrotum, with a markedly thickened wall. Scrotal color doppler ultrasound demonstrated an increased size of the right testicle, tunical effusion, and intratesticular cystic lesions. There was poor testicular blood flow but increased flow around the affected testis (Fig. 3A). Blood flow to the left testis was normal (Fig. 3B). Diagnosis of right testicular infarction secondary to epididymitis was suggested, so the patient was admitted. WBC count at the time was 10.2×10*9/L. All other serum chemistry parameters were within normal limits. Routine urinalysis and urine culture was negative.
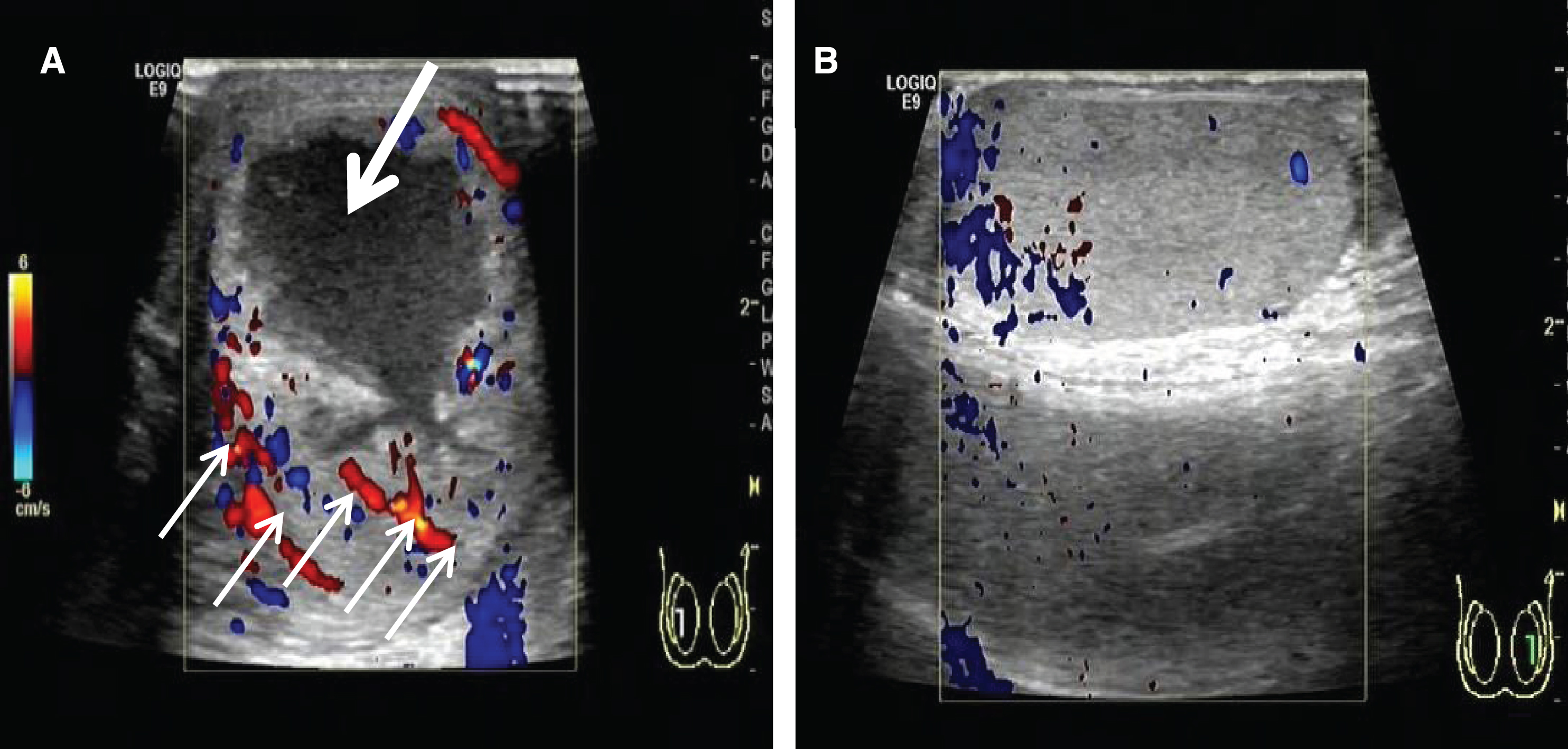
Color doppler signals in inflammatory epididymis in Case 2. (A) An intratesticular cystic lesion (thick arrow) with few blood signals in the right testis but increased blood flow around the involved testis (thin arrows). (B) Blood flow was noted in the healthy left testis as control.
The patient underwent scrotal exploration. No evidence of torsion was identified, however there was no blood flow to the right testis and epididymis. A right orchiectomy was performed. The surgical specimen had a purulent cavity within the infarcted testis (Fig. 4A). Histologic examination revealed chronic suppurative inflammation and inflammatory cell infiltration in the sample (Fig. 4B).
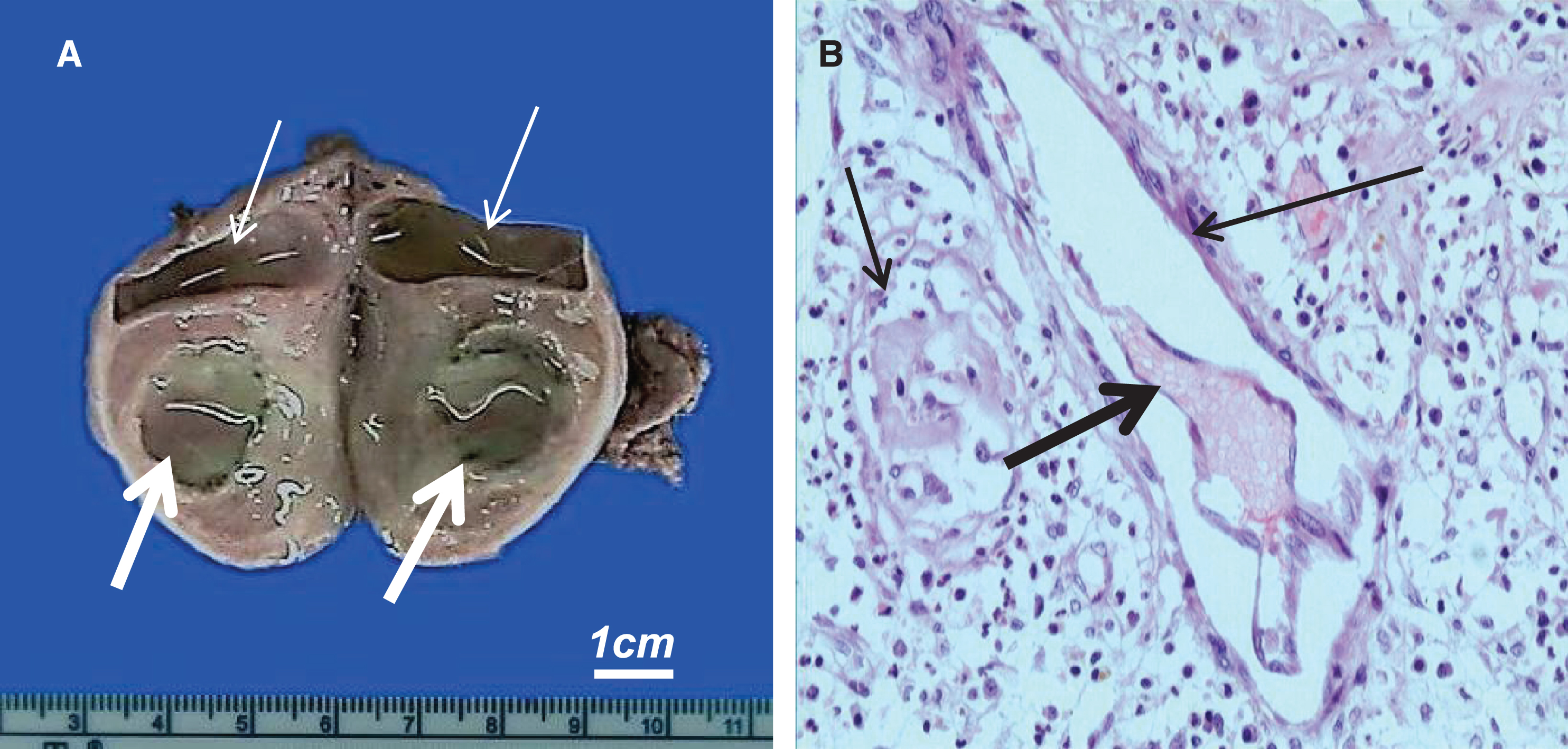
Gross specimen (right) and histological changes (left) Case 2. (A)< /b>Purulent cavities in the epididymis (thin arrows) and testis with a central purulent cavity (thick arrows). (B). Chronic suppurative inflammation and inflammatory cell infiltration (short arrow), vasculitis (long arrow) and thrombus formation (thick arrow) in the testis (H & E stain, 200×).
A 70-year-old male with past medical history of left epidiymitis, hypertension, and left renal cyst and no history of STIs, DM, or tuberculosis presented for painful left scrotal swelling for more than 2 months. He had been treated with antibiotics for 4 weeks without improvement. Physical exam demonstrated an enlarged and painful left scrotum, with a tender left testis 50×40 mm in size and a painful left cord. Color doppler ultrasound was obtained which demonstrated disorganization and hypertrophy of the left testicle and epididymis with a mixed-density 40×24 mm mass. There was poor blood flow in the left testis and increased blood flow around the mass (Fig. 5A). The right testis appeared normal (Fig. 5B). Chest radiography demonstrated pulmonary cavity formation suggestive of tuberculosis. However, there was no a sputum culture with acid fast staining and TB test. Diagnosis of left epididymitis with testicular abscess was suggested. All serum chemistry parameters were within normal limits. Urine tests showed 233 WBC/high power field (Normal: <20 WBC/hpd) and a negative urine culture. Diagnosis of left epididymitis with testicular abscess was suggested.
Alternation of blood flow (BF) signals in inflammatory epididymis in Case 3 examined by Color Doppler. (A) A mixed-density mass with poor blood flow in the left testis (thick arrow) 40×24 mm in size with increased blood flow around the mass. (B) Blood flow was evenly distributed in the healthy right healthy testis.
The patient underwent scrotal exploration. The left testis and epididymis appeared ischemic with caseous necrosis. 60 mL of purulent material was drained and a left orchiectomy was performed (Fig. 6A). Histologic examination revealed a tuberculous granuloma of the left testis and epididymis, which corresponded pathologically to central confluent caseous necrosis and peripheral tuberculoid granulomas involving the surrounding structures. Acid fast cultures demonstrated mycobacterium tuberculosis (Fig. 6B).

Gross specimen (right) and histological changes (left) case 3. (A) Caseous necrosis (arrows) in the epididymis and testis after 10% formalin fixation. (B) Mycobacterium tuberculosis were visible within the infected testicular tissue (Acid fast stain, 1000×).
In our study, the sizes of the involved testis (27±4 ml) was significantly larger compared to the nonaffected side (17±2 ml) (p < 0.05) (Table 1). Patients with a follow-up duration of no less than 6 months. At 6 months follow up there have been no reports of pain, sexual dysfunction, or other postoperative complications. The third patient was lost follow-up 12 months after operation. The other two patients are still being followed without further complications.
Scrotal pain is a common cause for presentation to the emergency department and urgent care settings [9]. Acute scrotal symptoms can be caused by infectious, traumatic or vascular etiologies including testicular torsion. Infection is the most common cause of acute scrotal pain and can be due to epididymitis, orchitis, or epididymo-orchitis [10]. Epididymitis is a common condition with incidence ranging from 25 to 65 cases per 10,000 adult males per year and can be acute, chronic or recurrent [11]. Epididymitis is most often caused by a bacterial infection from STIs such as gonorrhea or chlamydia, however Enterobacteriaceae and N. gonorrhoeae are often culprits. Acid fast bacteria such as Tuberculosis and viral infections have also been noted [1, 12]. In children and men older than 35 years, urinary tract-contaminating organisms such as E.coli and Pseudomonas species are the more likely pathogens [13]. Empirical antimicrobial therapy is selected with consideration given to the most probable pathogen and degree of penetration into the inflamed epididymis and is narrowed based on culture results.
Epididymitis may be complicated by abscess and even infarction if undiagnosed or inappropriately treated. Surgical drainage may be required if the abscess fails to resolve after conservative therapy. Prolonged presence of an untreated abscess or a large abscess may cause pressure necrosis of the testicular parenchyma [14]. In extreme cases, the affected testis may infarct, the cause of which is uncertain, though several theories have been proposed. The widely held hypothesis is compartment syndrome and thrombosis secondary to venous congestion and bacterial exotoxins [15]. Adorisio et. al. reported a pediatric patient with segmental infarction of the testis for epididymitis [16, 17]. A second theory is that acute inflammation of epididymis may progress to chronic epididymitis resulting in vasculitis and thrombus formation, ultimately resulting in infarction (Fig. 7).

Pathological processes of prolonged epididymitis in 3 cases with testicular infarction.
The main principles in the management of epididymitis include testicular function preservation and minimization of morbidity [17]. Conservative treatment means a period of rest, serial blood tests, regular observation, local physiotherapy and antibiotic therapy. For scrotal compartment syndrome it is imperative that the diagnosis be made early before irreversible damage to the testicles occur. Prompt assessment and recognition of ischemia may lead to reperfusion interventions, ultimately saving the testis [18]. The therapeutic efficacy for epididymitis depends on (i) duration and the severity of epididymitis and (ii) general condition of the patient. For patients in good health, early diagnosis and correct treatment can achieve good results. However, there are still some patients that may progress and develop long-term testicular atrophy and even testicular infarction. In cases of uncertainty, immediate surgical exploration is a reasonable approach [19].
Diagnosis of acute scrotum mainly depends on a variety of imaging examinations, including Color Doppler Ultrasound, contrast-enhanced ultrasound, and MRI [20]. Color doppler imaging is useful but is experience dependent with limitations in the presence of low flow. The Color Doppler Ultrasound is routinely applied for monitoring the blood flow of testis in our clinical practice. Contrast-enhanced sonography (CEUS) better depicts tissue perfusion as compared to conventional ultrasound and can provide an imaging adjunct when ultrasound findings are inconclusive [9]. For cases which are difficult to diagnose, MRI can provide superior localization; identification of fat, hemorrhage, and fibrous tissue; and differentiation between avascular cases, such as intratesticular hematoma or segmental testicular infarct [21, 22].
The ability to differential diagnosis the various acute scrotum entities is critical for the initiation of proper treatment. Testicular torsion and epididymitis are two of the most common disease of acute scrotum [9]. Testicular torsion occurs when the testis and spermatic cord twist within the scrotum, resulting in vascular occlusion and subsequent infarction if not immediately reset. The clinical findings of testicular torsion overlap with those of other acute scrotal pathologies. Testicular infarction in the presence of epididymitis should be differentiated from testicular torsion (Table 2). Torsion can occur at any age, although it most commonly affects young boys and peaks in early adolescence [23]. The typical characteristics of testicular infarction due to prolonged epididymitis are 1) decreased blood flow at the center of the test is at the early stage of epididymitis; 2) no blood signal at the center but increased blood signal at the edge of the involved testicular.
Differential diagnosis and treatments between testicular infarction due to prolonged epididymitis and testicular torsion
The third patient was treated as epididymitis but did not respond to antibiotics and was ultimately diagnosed tuberculoid epidiymitis. Tuberculous infection of epididymis and testis is difficult to differentiate clinically from pyogenic infection, tumor or infarction [24]. Tuberculous epididymitis may present similar to chronic or prolonged epididymitis in high-risk groups. The kidney or prostate is hypothesized to be the reservoir for tuberculous infection in the male genitourinary tract. Spread is thought to be hematogenous in nature, spreading from pulmonary tuberculosis. Patients with tuberculosis risk factors presenting with epididymitis that is refractory to empiric antibiotic therapy warrants consideration of tuberculosis epididymitis [25].
Early diagnosis and is crucial in the treatment of acute epididymitis. Blood flow to the testis can be monitored by doppler ultrasound to evaluate the degree of testicular blood flow helping urologists determine if surgical exploration is needed. If scrotal swelling and pain is not improved after conservative management or the degree of blood flow is diminished, immediate surgical intervention including open decompression should be carried out to save testicular function. Otherwise, severe and progressive infectious processes involving the epididymis and testicle may result in testicular loss [26].
The courses of the three patients were all more than 1 month. The symptoms of the patients were not improved after conservative treatment, and the testis were removed for testicular infarction. In the setting of refractory pain or recurrent epididymitis, clinicians should be suspicious of a testicular abscess or ischemia [14, 17] as were evident in our cases. Three cases accentuate the need for a high index of suspicion to rule out concomitant testicular ischemia secondary to epididymitis that might be salvaged in the future with immediate surgical intervention.
Testicular infarction is a rare consequence in patients with recurrent or prolonged epididymitis. No improvement in symptoms after conservative therapy with antibiotics, should increase suspicion of disease progression. Tuberculosis infection must be considered in cases of epididymitis not responsive to antibiotics and in high risk patients. Progression of pain suggests that scrotal exploration is required. In addition, patients should be advised to seek the help of specialists early for recurrent testicular pain and consistent pain after conservative treatment.
Conflict of interest
None of the contributing authors have any financial or personal relationships with people or organizations that could inappropriately influence this work.