
Abstract
Background
In patients with contraindication for beta-blockers who are also under long-term calcium channel-blocker therapy for any reason, ivabradine may be used as an alternative treatment to achieve the target heart rate.
Purpose
To assess whether single dose oral ivabradine in patients referred for coronary computed tomography angiography (CCTA) is safe and can significantly decrease heart rate compared to intravenous (i.v.) metoprolol in patients receiving long-term calcium channel-blocker therapy.
Material and Methods
One-hundred and twenty patients who were under calcium channel-blocker therapy referred for CCTA were randomized to premedication with single dose (15 mg) ivabradine (n = 63) or i.v. metoprolol (5–10 mg) (n = 62). Hearth rate (HR) was assessed at admission (HR1), prescan (HR2), and during CCTA scan (HR3) for all patients. Blood pressure (BP) was measured before medication (BP1) and immediately before CCTA scan (BP2).
Results
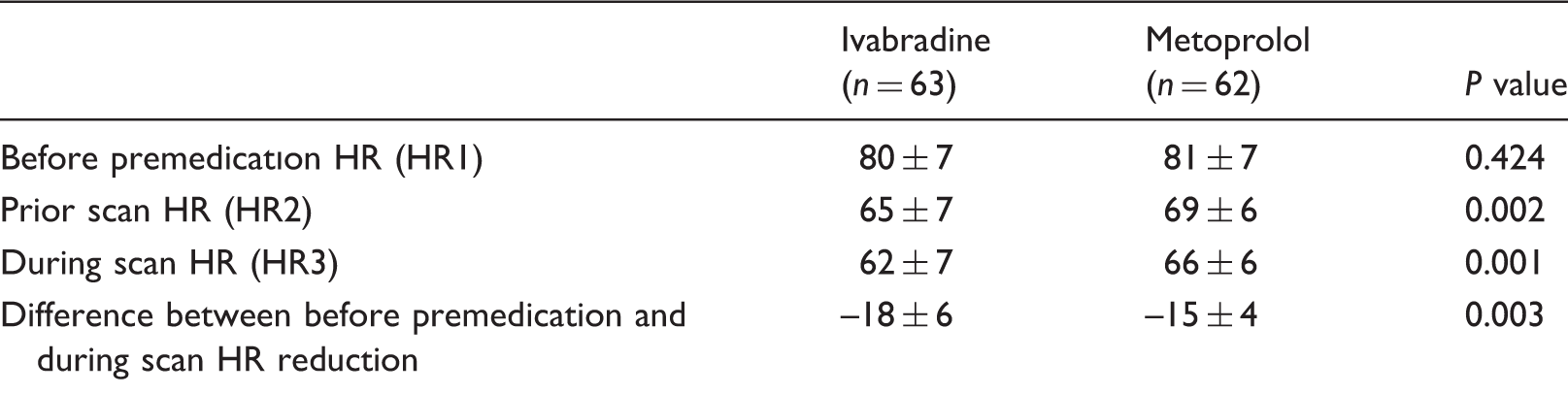
Although the HR averages of two groups were not significantly different before medication (HRIv1 = 80 ± 7 bpm vs. HRβ1 = 81 ± 7 bpm; P = 0.42), significant HR reduction was observed in the ivabradine group (HRIv3 = 62 ± 7 bpm) when compared to the metoprolol group (HRβ3 = 66 ± 6 bpm; P = 0.001). Decreases in HR forivabradine (18 ± 6 bpm) was significantly higher than for metoprolol (15 ± 4 bpm; P = 0.003) without relevant side-effects. Ivabradine showed no significant effect on either systolic BP or diastolic BP (siBPIv1, 139 ± 10; siBPIv2, 138 ± 10; P = 0.260; diBPIv1, 81 ± 7; diBPIv2, 81 ± 6; P = 0.59). Nevertheless, metoprolol group demonstrated significant reduction in both SiBP and DiBP (siBPβ1, 136 ± 11; siBPβ2 130 ± 11; P < 0.001; diBPβ1, 81 ± 6; diBPβ2, 78 ± 6; P < 0.001).
Conclusion
Single dose ivabradine is safe and significantly more effective than i.v. metoprolol in decreasing HR in patients under calcium channel-blocker therapy.
Introduction
Coronary computed tomography angiography (CCTA) is a non-invasive tool for the diagnosis of coronary artery disease (1). CCTA has shown to have a high negative predictive value, in the range of 93–100%, for ruling out significant coronary stenosis (2–5), the sensitivity and specificity of the detection of coronary artery stenosis being 93% and 96%, respectively (6). Importantly, to achieve accurate results, sufficient image quality is mandatory. In this respect, achieving a target heart rate (HR) of <63 beats per minute (bpm) for 64-slice computed tomography (CT) or <70 bpm for dual-source CT is an important prerequisite for image quality and diagnostic accuracy (7–10). To achieve these HRs, beta-blockers, calcium channel-blockers, or the novel drug ivabradine is administered prior to the CCTA scan. For patients who receive calcium channel-blocker therapy, beta-blockers can be used to decrease the HR if there is no contraindication to beta-blockers. However, in patients with contraindications to beta-blockers who also receive calcium channel-blocker therapy for any reason (such as hypertension, arrhythmia, coronary artery disease, or peripheral arterial disease), ivabradine may be used as an alternative therapy to achieve the target HR. The pharmacokinetics of ivabradine may be influenced by long-term calcium channel-blocker therapy because of the drug’s metabolization through hepatic cytochrome P450 3A4. An evaluation of ivabradine safety with concomitant calcium channel-blocker therapy is mandatory for future protocols.
As far as we know, there is no study evaluating the safety and efficacy of ivabradine administration in patients receiving calcium channel-blocker therapy. The aim of this study was to assess whether a single dose (15 mg) of ivabradine before CCTA is safe and can significantly decrease the HR and to compare single-dose ivabradine with 5–10 mg intravenous (i.v.) metoprolol (single dose or two doses) in patients who were receiving long-term calcium channel-blocker therapy.
Material and Methods
A total of 125 consecutive patients receiving long-term calcium channel-blocker therapy were prospectively enrolled between February 2012 and February 2013. All patients had suspected coronary artery disease and were in a mild- or moderate-risk group or had progression of known coronary artery disease. Calcium channel-blocker (CCB) therapy for 1 month was accepted as long-term therapy. The exclusion criteria for this study were HR < 70 bpm, systolic BP < 100, diastolic BP < 70 mmHg, second or third degree atrioventricular block, atrial fibrillation, frequent premature heart beats, serum creatinine level of 1.5 mg/dl, and a known allergy to iodinated contrast media. The study protocol was approved by the institutional review board, and all patients gave written informed consent. All patients were first assessed during an outpatient visit by a cardiologist, and each patient’s history, demographics, risk factors, current medical treatment, and indication for CCTA were collected. Only one patient was using verapamil, and 124 patients were using diltiazem. After the assessment, patients were allowed a resting period of 10 min in a sitting position, and hemodynamic parameters, the premedication HR (HR1), the systolic and diastolic BP (siBP1 and diBP1) values, and a 12-lead electrocardiography (ECG) measurement were obtained. Subsequently, patients were randomized into two groups in blocks of 10 patients at a 1:1 ratio and received immediate oral premedication with either ivabradine 15 mg or i.v. metoprolol (5–10 mg). In total, 63 (63/125) patients in the ivabradine group were instructed to refrain from activities that could alter cardiac parameters or gastrointestinal function (intense exercise or eating). Ivabradine group scans started after 126 ± 18 min of medication.
A 5 mg IV initial dose was administered to 62 (62/125) patients in the metoprolol group in the CT unit while the patients were in the supine position, ready to be scanned on the CT bed. The HRs and BP of the patients were monitored, and CCTA was performed in 5–10 min. If the HR was >65 bpm during a test breath-hold command immediately before the scan (HRβ2), an additional 5 mg i.v. metoprolol was administered in addition to the initial 5 mg. Because all patients were receiving long-term calcium channel-blocker therapy, no additional dose was administered after the total dose of 10 mg i.v. metoprolol.
We included photopsia and bradycardia on our checklist for the side-effects of ivabradine. Severe headache, severe gastrointestinal symptoms, and bradycardia were checked in the beta-blocker group.
All patients were scanned after these medications, regardless of the final HR.
The systolic and diastolic BP values and the HR immediately before the scan (siBP2, diBP2, and HR2) and the HR during the scan (HR3) were recorded. After the CT scan, the patients were observed for 2 h at the hospital. All patients received a telephone call after 1 day of treatment to inquire about probable outcomes.
CT was performed with a dual-source CT system (Definition Flash, Siemens Medical Solution, Forchheim, Germany) with 280 ms of rotation time, 2 × 128 slices, a pitch of 3.4, and triggering at 60% of the R-R interval. The tube current for the protocol was set at 180–300 mAs. Slice collimation of 0.6 mm was achieved using a continuous helical scan with the ECG-dependent maximum tube current-modulation technique. A dose of 100 mL of non-ionic contrast material (iomeprol; Iomeron 400 mgI/mL; Bracco, Milan, Italy) was administered at a rate of 5 mL/s with a dual-head power injector attached to an 18- to 20-gauge needle positioned in an antecubital vein. The bolus tracking technique was used, and images were obtained during a single breath-hold of 6 s. Image quality was assessed for all coronary segments according to the modified 15-segment American College of Cardiology and American Heart Association (AHA) classification and using a four-point grading scale: 3, excellent (no artifacts); 2, good (minor artifacts); 1, fair (moderate artifacts); and 0, not interpretable (major artifacts, with severe image degradation due to coronary motion or severe blurring caused by extensive calcification or stents) (11).
Statistical analyses were performed using SPSS software version 17. The variables were investigated using visual (histograms and probability plots) and analytical methods (Kolmogorov-Smirnov/Shapiro-Wilk’s test) to determine the normal distribution. Descriptive analyses were presented using means and standard deviations for normally distributed variables. The categorical variables were expressed as numbers and percentages. Numerical variables were compared using the Student’s t-test. Categorical data were compared by the chi-square test. The paired Student's t-test was used to compare measurements at two time points (baseline and before the scans) for the systolic and diastolic BP. A P value < 0.05 was considered significant.
Results
Patient characteristics in both randomized groups.
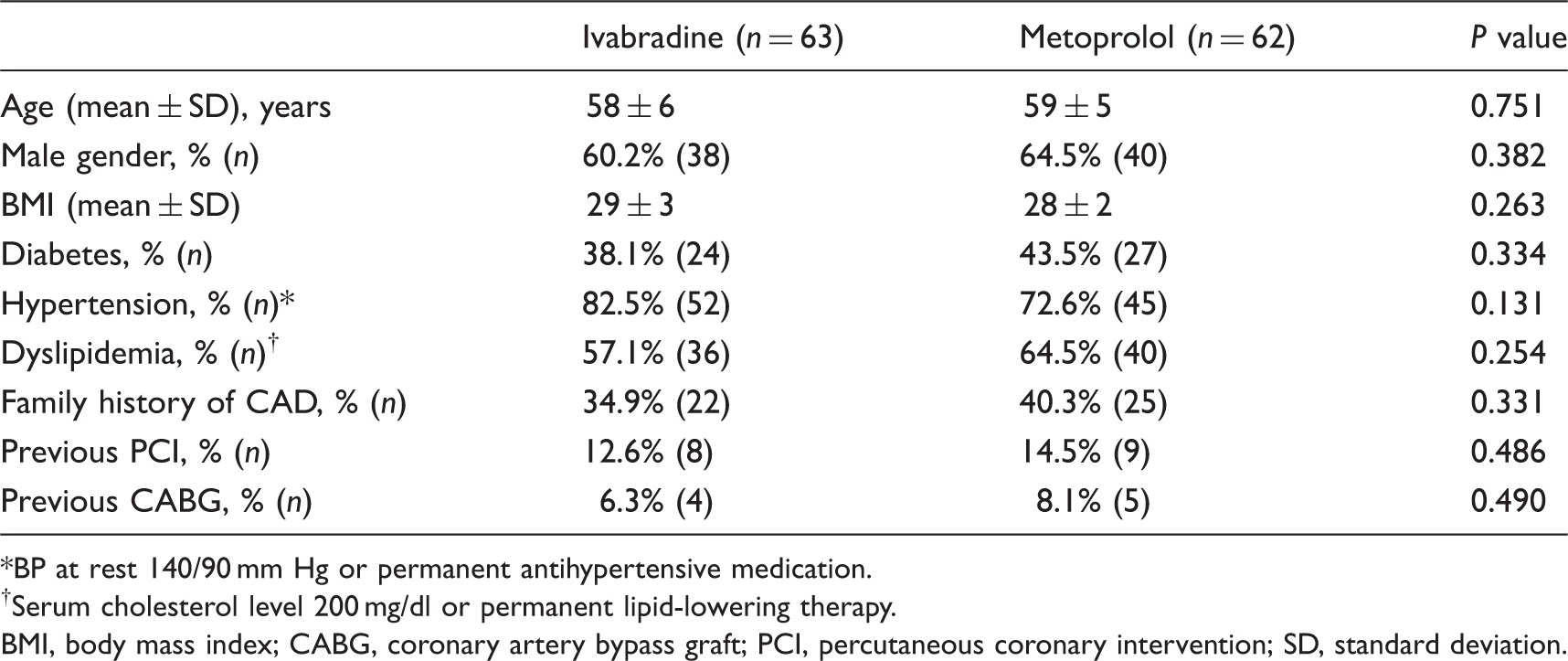
BP at rest 140/90 mm Hg or permanent antihypertensive medication.
Serum cholesterol level 200 mg/dl or permanent lipid-lowering therapy.
BMI, body mass index; CABG, coronary artery bypass graft; PCI, percutaneous coronary intervention; SD, standard deviation.
Alteration of blood pressure between the premedication, prior to scan and during scan in both groups.
Alteration of blood pressure between the premedication and prior to scan in both groups.

Both of the drugs were well tolerated. No adverse reactions or symptomatic bradycardia was identified. In total, 21 patients (21/63, 33%) in the ivabradine group and 12 patients (12/62, 19%) in the beta-blocker group had asymptomatic sinus bradycardia (HR <60 bpm, mean value, 57 bpm). Sinus bradycardia was more common in the ivabradine group. Only one patient (1/63) in the ivabradine group experienced transient visual symptoms (photopsia), whereas none of the patients in the beta-blocker arm reported such a side-effect. Two patients developed minor systemic allergic reactions due to the contrast material, and their symptoms were relieved without any treatment. All patients were called 1 day after CCTA. No patients reported a relevant side-effect after the following day of therapy.
Discussion
The pharmacokinetics of ivabradine may be influenced by long-term calcium channel-blocker therapy because of the drug’s metabolization through hepatic cytochrome P450 3A4. As far as we know, the risks and the efficacy of ivabradine in patients who are receiving calcium channel-blocker therapy have not yet been investigated. This is the first study to assess the safety of a single dose (15 mg) of ivabradine in patients who are receiving long-term calcium channel-blocker therapy. Additionally, this study provides preliminary data comparing the efficacy of single-dose ivabradine and i.v. beta-blockers on altering the pre-scan HR of patients who are receiving calcium channel-blocker therapy.
To the best of our knowledge, a single dose (15 mg) of oral ivabradine premedication is a safe and effective way of reducing the HR to target values in the presence of concomitant, long-term calcium channel-blocker use. We found that in our group of patients, the ivabradine group showed no significant change in their BP in contrast to the IV metoprolol group, which demonstrated a statistically significant reduction in both the systolic and the diastolic BP. Moreover, none of the patients experienced symptomatic bradycardia due to the ivabradine treatment.
Since the introduction of new multidetector CT scanners with 64,128, or 320 detectors, CCTA has been widely used not only for the detection of coronary artery disease but also for the assessment of atherosclerotic plaques. Even with newer scanners, such as dual-source and 320-detector scanners, HR control is mandatory to achieve sufficient image quality (12,13).
Many investigators have recommended the administration of a single dose of oral or i.v. beta-blockers to decrease the HR (14,15). However, several other studies have reported that these drugs are not sufficiently effective (16).
A novel drug, ivabradine, was found to be safe and effective as an HR-reducing agent in patients. Ivabradine is a pure HR-lowering agent that acts by selective and specific inhibition of the cardiac pacemaker If current, which controls the spontaneous diastolic depolarization in the sinus node and regulates the HR. The cardiac effects are specific to the sinus node, with no effect on intra-atrial, atrioventricular, or intraventricular conduction times; myocardial contractility; or ventricular repolarization. Therefore, ivabradine is suitable for a wide range of patients, including those individuals for whom other HR-lowering agents may be contraindicated. Indeed, the safety of ivabradine has been demonstrated in large clinical trials, with minor side-effects, such as mild-to-moderate visual symptoms (17). Guaricci et al. (18) showed that the administration of ivabradine for 5 days before CCTA is adequate in reducing the HR. Pichler et al. (11) reported sufficient and similar HR reductions in patients randomized to receive ivabradine and in those patients randomized to receive single-dose oral metoprolol. Tardif et al. reported that ivabradine can also safely be used in the presence of concomitant beta-blocker use (19). In this study, we also found that ivabradine can safely be used as an alternative therapy in patients who have contraindications to beta-blockers (such as asthma and severe long-term obstructive pulmonary disease) in the presence of concomitant, long-term calcium channel-blocker therapy.
Pichler et al. (11) reported that ivabradine sufficiently decreases the HR, with significantly less depression of the systolic BP compared with oral metoprolol (50 mg). In the same study, the researchers reported that in a subgroup of patients who were receiving long-term beta-blocker therapy, a significantly stronger HR reduction was achieved with ivabradine, whereas the decrease in the systolic BP was lower compared with metoprolol.
Our data demonstrated that in patients receiving long-term calcium channel-blocker therapy, single-dose ivabradine (15 mg) produced a greater reduction in the HR compared with i.v. metoprolol (5–10 mg), without any significant change in the systolic or diastolic BP. However, the metoprolol arm showed a significant decrease in both the systolic and the diastolic BP in our study group. In contrast to our study, Pichler et al. (11) found no statistically significant difference in the diastolic BP decreases between the ivabradine group and the metoprolol group.
Adile et al. (20) compared ivabradine with oral metoprolol at 5–15 mg and 50–150 mg total doses, respectively. Similar to our results, Adile et al. reported a better reduction in the HR compared with oral metoprolol, without any significant change in the systolic or diastolic BP. Regarding the lack of significant effects on the BP, ivabradine may also be preferred in patients with left ventricular systolic dysfunction/heart failure. Further, more specific studies are warranted to address this issue. By giving the maximum daily dose of ivabradine at one time, the HR reductions in our study group (18 ± 6 bpm) were weaker when compared with the results of a previous study on ivabradine by Guaricci et al. (17), who studied patients treated with chronic beta-blocker therapy (24 ± 10%). In this study, Guaricci et al. used ivabradine 5 mg twice per day for 5 days prior to the CCTA scan.
Our study had some limitations. First, we did not control for irregular rhythms in our study, but we did not have many patients with artifacts (motion or stair step) due to rhythm irregularity. Second, we also did not include an image quality comparison between the two drugs, as we know from several studies that a decreased HR means increased image quality (10,12,21). Finally, because all patients were receiving long-term calcium channel-blocker therapy, the beta-blocker dose was limited to a maximum of 10 mg, which could have had an influence on the lower decrease in the HR in the beta-blocker arm. Additionally, due to inadequate numbers, we did not include a subgroup safety analysis for the patients with the contraindications to beta-blocker treatment.
In conclusion, our study indicates that CCTA with single-dose (15 mg) oral ivabradine premedication is a safe and effective way of reducing the HR to target values in the presence of concomitant, long-term calcium channel-blocker use. Thus, ivabradine can successfully substitute for beta-blockers in patients receiving calcium channel-blocker therapy, particularly in those patients with contraindications to beta-blockers.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.