
Abstract
OBJECTIVE:
To demonstrate the ability of achieving low dose and high-quality head CT images for children with acute head trauma using 100 kVp and adaptive statistical iterative reconstruction (ASIR-V) algorithm in single rotation on a 16 cm wide-detector system.
MATERIALS AND METHODS:
We retrospectively analyzed the CT dose index (CTDI) and image quality of 104 children aged 0–6 years with acute head trauma (1 hour –3 days) in two groups: Group 1(n = 50) on a 256-row CT with single rotation at a reduced-dose of 100 kVp/240 mA and reconstructed using ASIR-V at 70%level; Group 2(n = 54) on a 64-row CT with multiple rotations at a standard dose of 120 kVp/ 180mA and reconstructed using a conventional filtered back-projection (FBP). Both groups used the 0.5 s/r axial scan mode. CT dose index (CTDI) and quantitative image quality measurements were compared using the Student t test; qualitative image quality comparison was carried out using Mann-Whitney rank test and the inter-reviewer agreement was evaluated using Kappa test.
RESULTS:
The exposure time was 0.5 s for Group 1 and 3.27±0.29 s for Group 2. The CTDI in Group 1 was 9.74±0.86mGy, 36.38%lower than the 15.31mGy in Group 2 (p < 0.001). Group 1 and Group 2 had similar artifact index (2.06±1.06 vs. 2.37±1.18) in the cerebellar hemispheres, and similar contrast-to-noise ratio (2.32±0.83 vs. 1.69±0.68), (1.47±0.72 vs. 1.10±0.43) respectively for cerebellum and thalamus (p > 0.05). Image quality was acceptable for diagnosis, and motion artifacts were reduced in Group 1 (p < 0.001).
CONCLUSION:
Single rotation CT with 100 kVp and 70%ASIR-V on 16 cm wide-detector CT reduces radiation dose and motion artifacts for children with acute head trauma without compromising diagnostic quality as compared with standard dose protocol. Thus, it provides a novel imaging method in management of pediatric acute head trauma.
Keywords
Introduction
Traumatic brain injury (TBI) is the most usual cause of death and disability in children worldwide, especially in children 4 years or younger [1, 2]. Prompt and accurate identification of the trauma-related brain injuries, especially of the injuries needing acute intervention, is very important in the acute management and is also a great challenge. Because of fast scan speed, computed tomography (CT) is typically the reference standard for diagnosing in emergent pediatric TBI [3–5].
During the past decade, CT use in pediatric emergency departments has increased significantly [6, 7]. It was reported that about 50%of children with head trauma managed in emergency departments would undergo CT [8, 9]. However, pediatric organs are more sensitive to ionizing radiation, CT imaging for children has risks of radiation-induced malignancy [10, 11]. It was estimated that the rate of lethal malignancy caused by pediatric cranial CT was between 1 in 1000 and 1 in 5000 [12]. So, reducing diagnostic radiation exposure and inappropriate CT use among children with head trauma become more and more important in pediatric clinical practice [13–15]. But, several factors hinder appropriate use of CT and there is no reduction in CT use for children with acute TBI [5, 17]. Lower radiation CT with diagnostic quality is in urgent need in the management of children with TBI in emergency departments.
Lower radiation CT can be achieved by reducing the tube current time product or tube voltage, and by modifying the reconstruction mechanism for CT images. The filtered back projection (FBP) algorithm is a traditional reconstruction method that is fast and has high fidelity but is also limited due to the high image noise in low x-ray signal conditions. Recently, a new volume-based adaptive statistical iterative reconstruction (ASIR-V) has been developed for noise reduction and contrast resolution improvements [18]. Compared to FBP and the previous version of iterative reconstruction algorithms, ASIR-V contains more advanced noise modeling, object modeling and physics modeling. The advanced system noise model includes the modeling of the data acquisition system (photon noise and electronic noise) as well as noise characteristics of the reconstructed images. The photon noise model includes characterization of the photon statistics as it propagates through the imaging chain. The modeling of the reconstructed image noise includes characterization of the scanned object, using information obtained from extensive phantom and clinical data. Study has shown that ASIR-V provides considerably better image quality with high diagnostic accuracy even at ultralow radiation dose [19].
Furthermore, with the introduction of 16 cm wide-detector CT, it is possible to complete the whole head scan in an axial mode in single gantry rotation within sub-second, significantly reducing the probability of patient head motion during the CT scan.
In our study, we aimed to demonstrate the ability of achieving low dose and high-quality head CT images for children with acute head trauma using 100 kVp and adaptive statistical iterative reconstruction(ASIR-V) algorithm in single rotation on a 16 cm wide-detector system, in comparison with those of conventional 120 kVp data acquisition and FBP image reconstruction algorithm on a 64-row CT scanner.
Materials and Methods
Patient information
This was a retrospective study and was approved by the hospital ethics committee. All the parents involved in the project signed the informed consent for undergoing CT scans. Inclusion criteria were patients who need to be ruled out intracranial lesions after acute head trauma. Exclusion criteria were children with congenital lesions or acquired neurological sequelae of acquired neuropathy such as hypoxic-ischemic encephalopathy (HIE). Patients were all with acute TBI and were groupedchronologically. Group 1 (Study group, n = 50, age ranged from 5 months to 6 years; mean age 3.08±1.69 years) was acquired continuously on a newer scanner from April to August 2018, and Group 2 (n = 54) was selected from the hospital archive system who were scanned prior to April 2018 on an older CT scanner with matching age distribution (age ranged from 11 months to 6 years; mean age 3.30±1.50 years).
Image acquisition and scanning procedure
Patients in Group 1 were scanned on a 256-row, 16cm wide-detector CT (Revolution CT, GE Healthcare, Waukesha, WI USA) with a reduced-dose protocol of 100 kVp/240 mA, 0.5 s rotation speed. Scans were performed in single axial rotation with the detector collimation options of 12 cm, 14 cm, and 16 cm according to the size of the head of the child. The imaging matrix was 512×512, with imaging thickness and spacing of 5.0 mm. Images in Group 1 were reconstructed using the new volume-based ASIR-V algorithm at the 70%strength level. The scan protocol and ASIR-V strength level selection was based on our experience during the trial period after the installation of the Revolution CT scanner.
Patients in Group 2 were scanned on a 64-row CT (VCT, GE Healthcare, Waukesha, WI USA) with the standard-dose protocol of 120 kVp/180 mA, 0.5 s rotation speed. Scans were performed in axial scan mode with multiple scans with the collimation of 2 cm. The imaging matrix was 512×512, with imaging thickness and spacing of 5.0 mm. Images in Group 2 were reconstructed using the conventional FBP reconstruction algorithm.
All patients were scanned in a head-to-foot direction and in the supine position. The scanning range was from the canthus line to the cranial top. The neck, chest, abdomen and gonads of the child were shielded with lead aprons to reduce radiation risk to these organs. Radiation dose in terms of the volumetric CT dose index (CTDIvol) and dose-length-product (DLP) of each scan was recorded. The exposure time and exam time which included the time for translating the patient table (in Group 2 with the conventional scan protocol) for covering the entire brain were recorded.
Objective image quality measurement
The CT attenuation value and standard deviation (SD) of the gray matter (GM) (CTGM and SDGM, respectively) and white matter (WM) (CTWM and SDWM, respectively) at the level of cerebellum (Fig. 1.a) and thalamus (Fig. 1.b) were measured by using a region of interest (ROI) covering 75%of the corresponding area. The contrast to noise ratio (CNR) was calculated according to the following formula:
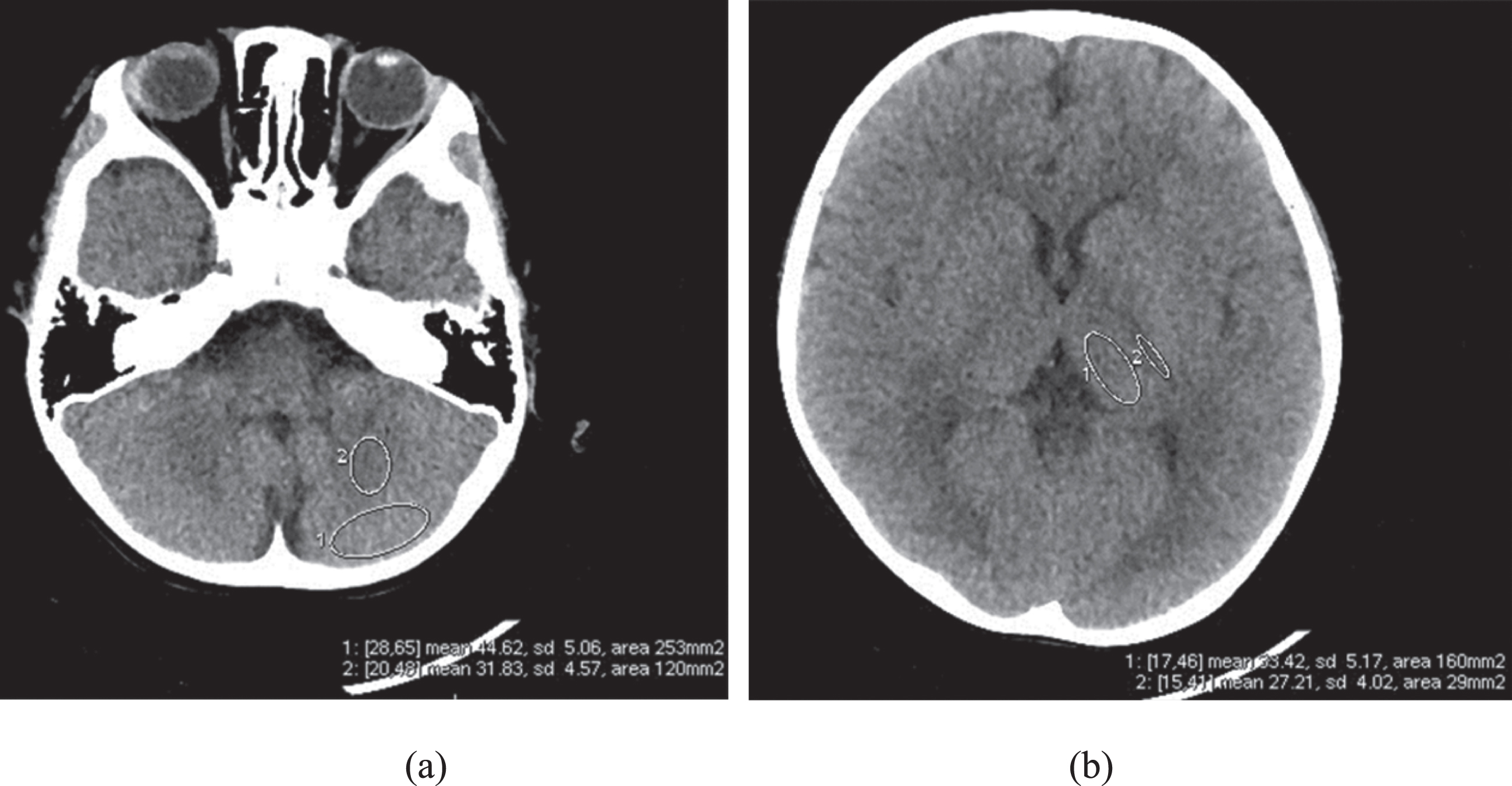
Region of interests were drawn at gray matter and white matter. (a) Axial CT image at the level of cerebellum. (b) Axial CT image at the level of thalamus.
CNR = (CTGM-CTWM)/0.5(SDGM + SDWM).
The artifact index (AI) for cerebellar hemisphere (Fig. 1.a) was calculated according to the following formula [20]: AI = (SDGM2- SDWM2)1/2, where SDGM is the SD in the gray matter near the skull and SDWM is the SD in the white matter further away from the skull. Similar to reference 20 where the artifact index was first introduced, we assumed the potential beam hardening artifacts for the bone-brain interface may be reflected by the increase in the standard deviation in the area near the skull in comparison with the areas that are further away from it. In calculating the artifact index, SDWM was considered background noise and the difference in standard deviation between the gray matter and white matter was used to reflect the net change caused by beam hardening artifacts and smaller values would mean less beam hardening artifacts.
The subjective image quality was evaluated by two board-certified radiologists (Y.L. and Y.Z. with 14 and 16 years of CT experience, respectively) using a 4-point scoring system in terms of the gray matter (GM) and white matter (WM) contrast, motion artifacts and overall image quality with 2 and above being acceptable for diagnostic purpose. Specifically, the scores were: for GM–WM contrast (supratentorial: contrast between thalamus and internal capsule; posterior fossa: cerebellar GM–WM contrast): 1, insufficient for diagnosis, 2, suboptimal but diagnostic, 3, good, 4, excellent; for motion artifacts: 1, artifacts interfering with diagnosis, 2, considerable artifacts with preserved diagnostic quality, 3, minor artifacts, 4, very low or no artifacts; and for the overall image quality: 1, unacceptable, 2, only acceptable under limited conditions, 3, mostly acceptable, and 4, completely acceptable (Table 1).
Grading scales for image quality evaluation
Grading scales for image quality evaluation
In this study, CTDI vol, DLP were recorded and compared between the two groups. Then, all statistical analyses were performed with SPSS20.0 (Chicago IL, USA). Results were expressed as means±standard deviations for continuous variables such as age, mean CT value, SD value and were expressed as frequencies for ranked data such as the subjective image quality scores. The Student t test for independent samples was used to assess continuous variables. The Mann-Whitney rank test was used to evaluate the ranked data and non–normally distributed variables such as the scan time. P < 0.05 indicated statistical significance for all analyses. Interobserver agreement for imaging quality scores was determined by using the Kappa test. A k value of less than 0.20 was considered to indicate slight agreement; 0.21–0.40, fair agreement; 0.41–0.60, moderate agreement; 0.61–0.80, substantial agreement; and 0.81 or greater, almost perfect agreement.
Results
Patient information
The characteristics of the patient cohort are summarized in Table 2. In all, 17 of the 50 patients in Group 1 and 20 of the 54 patients in Group 2 had abnormal CT findings. There was no difference between Group 1 and 2 in terms of age (p = 0.266).
Patient Information
Patient Information
*Soft tissue injury was defined as scalp hematoma, scalp swelling and scalp laceration without skull fracture and intracranial lesions.
The total exposure time was 0.5s for Group 1 and 3.27±0.29 s for Group 2. There was 84.71%reduction in exposure time in Group 1. The exam time to coverage the entire brain was further reduced by 95.22%from 10.47±1.03 s to a single rotation time of 0.5 s (P < 0.001). There were 19 patients with 12 cm collimation, 31 with 14 cm collimation, and 0 with 16 cm collimation in Group 1. The CTDI vol in Group 1 was 9.74±0.86 mGy, 36.38%lower than the 15.31 mGy in the standard dose group (P < 0.001). The DLP in Group 1 was 130.56±7.99 mGy cm, 34.76%lower than the 200.15±17.56 mGy cm in the standard dose group (P < 0.001). Patient radiation dose information is listed in Table 3.
Patient scan time and radiation dose (Mean±Standard Deviation)
Patient scan time and radiation dose (Mean±Standard Deviation)
DLP, dose-length-product; CTDIvol, volumetric CT dose index; Exam Time, the time to cover the entire brain; Exposure Time, the X-ray on time.
The quantitative measurements for the two groups are listed in Table 4. There were no statistically significant differences in mean CT value and CNR for cerebellum hemispheres between Group 1 and Group 2 (39.66±2.91HU vs. 37.25±3.95HU in mean CT value, and 2.32±0.83 vs. 1.69±0.68 in CNR) (P > 0.05), and for thalamus between Group 1 and Group 2 (33.23±1.94HU vs. 32.79±2.14HU in mean CT value and 1.47±0.72 vs. 1.10±0.43 in CNR) (P > 0.05). Also, there were no statistically significant differences in AI for cerebellum hemispheres between Group 1 and Group 2 (2.06±1.06 vs. 2.37±1.18) (P > 0.05). Although all images were accepted (Table 5) (Fig. 2 to Fig. 3), the image quality of Group 1 was better than that of Group 2 (P = 0.001), especially in the evaluation of motion artifacts (P < 0.001) (Fig. 4), there was excellent agreement in image quality assessment between the two reviewers (k > 0.81 for all) (Table 5).
CNR and AI (Mean±Standard Deviation)
CNR and AI (Mean±Standard Deviation)
GM, gray matter; WM, white matter; CNR, contrast to noise ratio; AI, artifact index.
Image Quality Score distribution
GM, gray matter; WM, white matter.
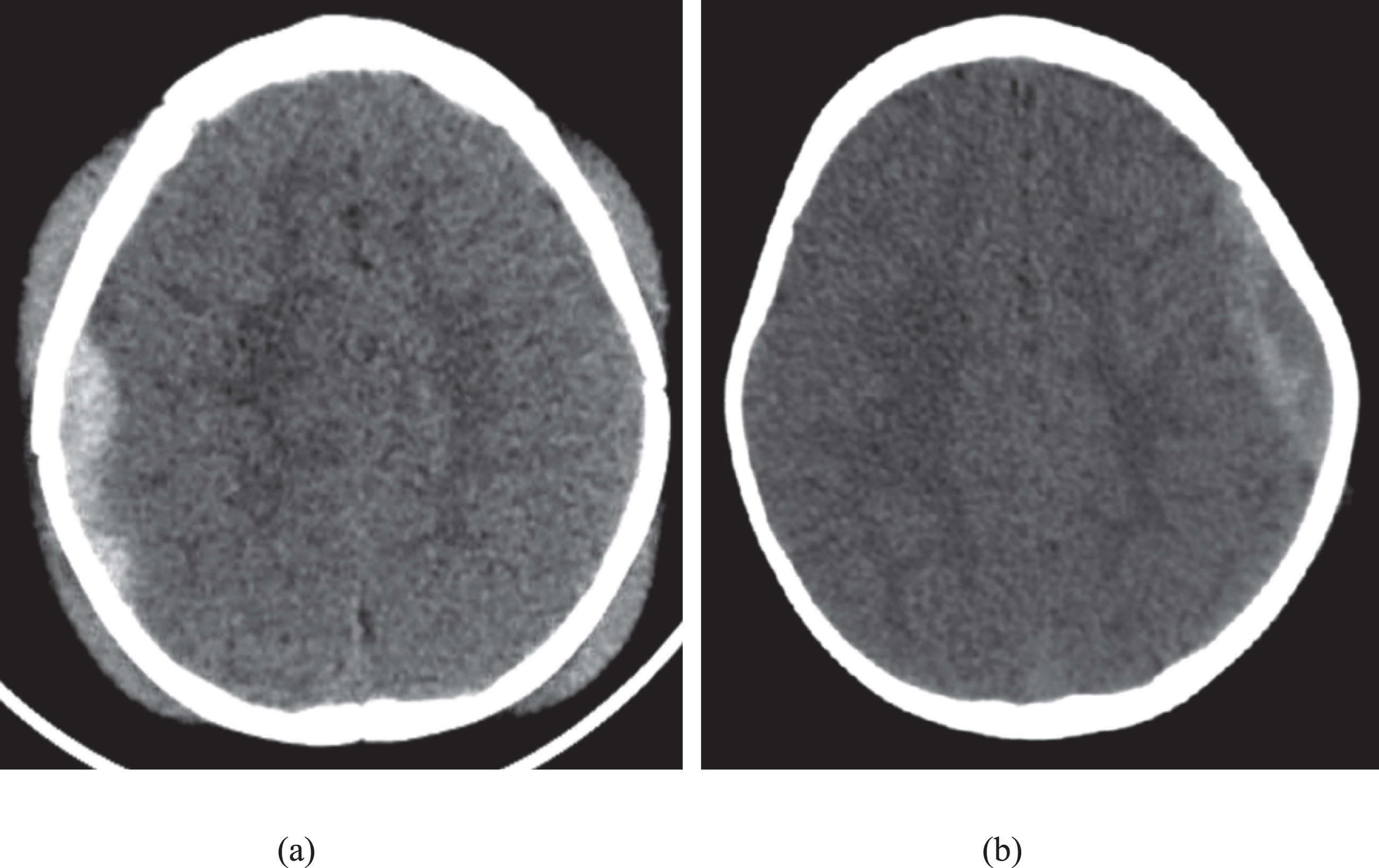
Axial CT image of children with TBI. (a) a 3 years old patient obtained by using the low dose axial scan mode on a 16 cm wide-detector CT, showing an epidural hematoma and scalp hematoma. (b) a 2 years old patient obtained using a conventional 64-row VCT, showing an epidural hematoma and scalp hematoma.

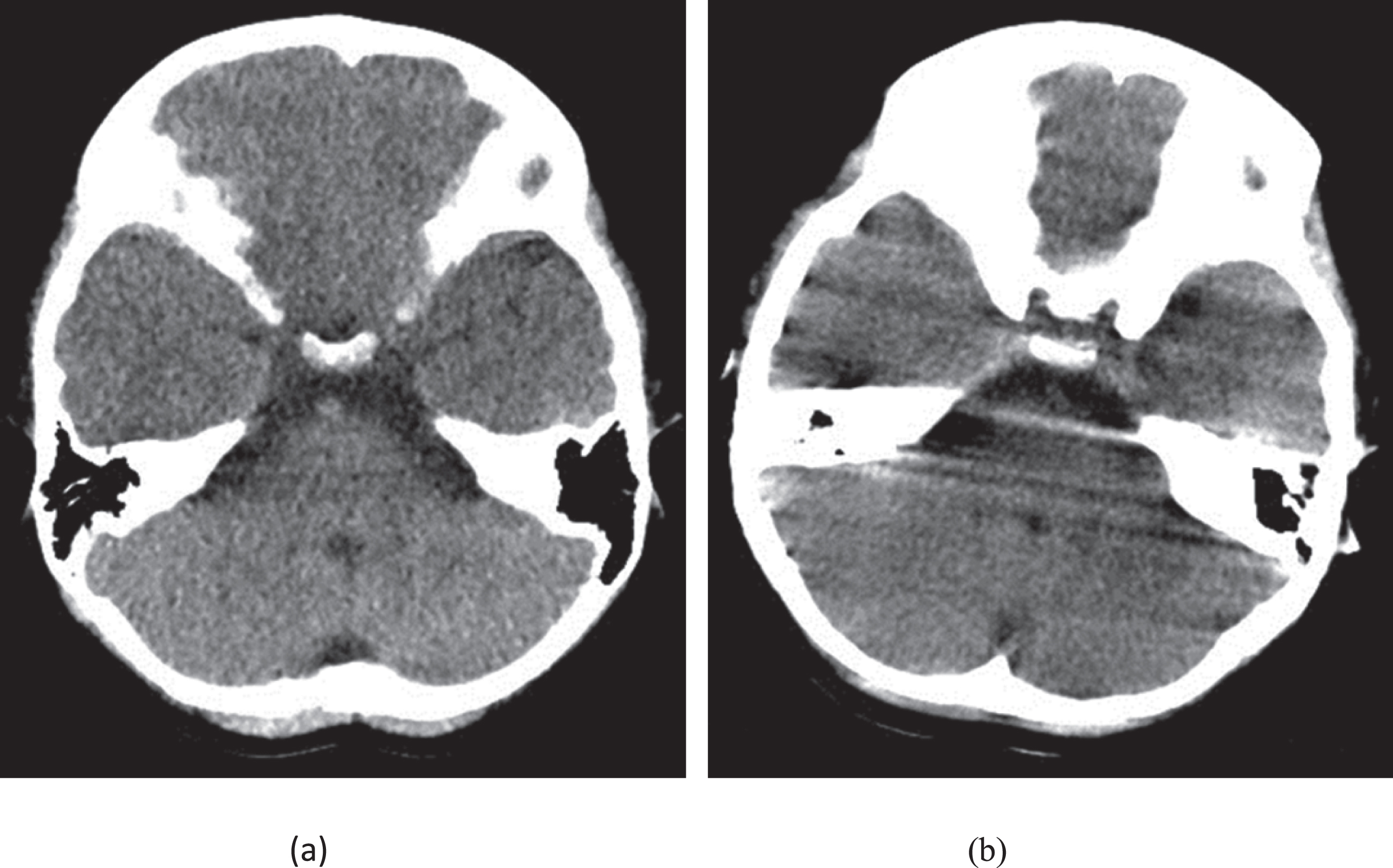
Axial CT image of children with TBI. (a) 4 years old patient obtained by using the low dose axial scan mode on a 16 cm wide-detector CT, showing both parietal bone fracture and scalp hematoma. (b) a 2 years old patient obtained using a conventional 64-row VCT, showing left frontal bone fracture and scalp hematoma.
Axial CT image of children with TBI. (a) a 1 year old patient obtained by using the low dose axial scan mode on a 16 cm wide-detector CT, showing no motion artifacts.(b) A head CT image of a 1 year old patient obtained using a conventional 64-row VCT, showing some motion artifacts.
In our study, we evaluated the image quality, radiation dose and exposure time of scanning children with acute head trauma using 100 kVp in single rotation on a 16 cm wide-detector CT system and reconstructed with a new generation adaptive statistical iterative reconstruction (ASIR-V) algorithm. Images were compared with those of using the conventional 120 kVp on a 64-row CT scanner and reconstructed with a filtered back projection (FBP) reconstruction algorithm. Our results demonstrated that using 100 kVp and 70%ASIR-V produced similar CNR and AI as the conventional 120 kVp and FBP protocol at 35%less radiation dose, and the faster scanning in Group 1 resulted in much less motion artifacts in the images.
There are many ways to reduce radiation dose in CT imaging of children, and scan protocols such as lowering tube voltage and tube current time, shortening scan time, limiting scan coverage are utilized in clinical practice [21–24].
Using lower tube voltage is one of the most effective methods because radiation exposure rises proportionally to the square of tube voltage [25]. In our study, despite the slightly higher mAs setting in Group 1, the use of 100 kVp tube voltage in Group 1 provided about 35%dose reduction compared to the conventional 120 kVp in Group 2. Although lower tube voltages are often used in the contrast-enhanced body CT scans to take the full advantage of increased contrast for iodine [26] and less common in the non-contrast head CT imaging to avoid potential beam hardening artifacts caused by bony structures, such as the skull [27]. However, our results indicated that the AI at cerebellum hemispheres with 100 kVp in Group 1 were similar with the conventional 120 kVp in Group 2. We believe this may be due to the following two reasons. First, the skull of pediatric patients is softer than that of adult patients [28] and reducing tube voltage does not increase the severity of beam hardening. Second, the 256-row Revolution CT used in Group 1 is equipped with a volume high definition (VHD) reconstruction algorithm which incorporates spectrum correction in the reconstruction process and was able to provide more effective beam hardening artifact correction in our study.
Shortening scan time is particularly important in imaging pediatric patients, especially pediatric patients with head trauma who typically could not cooperate. Higher pitch helical and wide-detector axial are the two common methods to reduce scan time. However, using high-pitch helical scan mode would require extending the scan range at both ends beyond the intended coverage for proper data interpolation in image reconstruction for the intended coverage. This extension is called over-ranging and would contribute to the increased radiation dose. In our study, the use of single gantry rotation axial scan to cover the entire brain enabled by the 16 cm wide-detector CT in Group 1 greatly reduced the total exposure time and total exam time from the 3.27±0.29s and 10.47±1.03 s, respectively in the conventional 64-slice CT system to only 0.5 s, thereby significantly reduced motion related artifacts in Group 1. We have published a paper pointing out the advantages of using the single axial rotation to image the chest for infant patients without the need of sedation [29], and the current study further demonstrated the benefit in imaging the head of pediatric patients with head trauma. The findings in our current work suggested a new scan protocol to image the head for non-cooperative pediatric patients using a single axial scan for fast coverage to provide low-dose and high-quality images with virtually no motion artifacts.
With the reduction of X-ray dose, image noise rises accordingly. Iterative reconstruction (IR) algorithms have been introduced and used clinically in CT scans with reduced radiation dose to either reduce image noise or improve image quality [30–32]. ASIR-V is a modification of the previous IR version (ASIR) and has been equipped with more advanced noise and physical modeling, providing further noise reduction and low-contrast resolution improvements [33, 34].
In our study, the radiation dose of 100 kVp with 70%ASIR-V in single rotation on a 16 cm wide-detector was 35%lower compared to that of the 120 kVp with FBP algorithm on a 64-row CT scanner, while image quality was similar in both protocols. In another words, the ASIR-V effectively compensated for the signal lose and maintained the image quality [35].
Our study had several limitations. First, the sample size in our study was still small. It should be noted that the lack of statistical significance for AI and CNR values between the two groups reported in this study may be due to the small sample size. Second, we did not select the lower tube voltage than 100 kVp on the 16-cm detector CT, and tube current in Group 1 was still on the high side. We will try to further reduce the radiation dose in the future. Third, we only focused on image quality evaluation in the current study, and further study should involve diagnostic accuracy. Fourth, we only compared the image quality at 70%ASIR-V level with that of FBP based on our initial experience. Studies have shown that with the change of ASIR-V level, image noise and texture changes as well. Higher ASIR-V levels will further reduce image noise; but may also produce images with more blotchy appearance with reduced acceptance clinically. Further investigations will be needed to confirm the optimal ASIR-V level and the image quality improvements of ASIR-V with an optimal level. Fifth, we used the historic scan data from an older CT system as the baseline for comparison. There were many confounding factors for the dose reduction and motion artifacts reduction due to the use of two different CT systems. However, since the axial scans were used in both groups and the detection technique was similar between the two CT systems, the dose reduction in the study group was mostly from the use of iterative reconstruction algorithm. Similarly, since the gantry rotation speed was the same in both groups, the motion artifacts reduction was largely attributed to the wider z-axis coverage in the study group.
Conclusions
Single rotation CT with 100 kVp and 70%ASIR-V on a 16 cm wide-detector CT reduces dose by 35%and provides high-quality images with less motion for children with acute head trauma, compared with standard dose protocol on an older 64-row CT system, and provides a novel method in the management in imaging pediatric acute head trauma.
Footnotes
Acknowledgments
We gratefully acknowledge Dr. Heping Zhou from Medical Imaging Centre, Affiliated hospital of Ankang University (Ankang Central Hospital) for his technical support in this study.