
Abstract
OBJECTIVE:
To improve safety and efficiency of radiotherapy process by customizing a Varian ARIA oncology information system following the guidelines provided in AAPM TG-100 report.
METHODS:
First, failure mode and effects analysis (FMEA) and quality management program were implemented for radiotherapy process. We have customized the visual care path in the ARIA system and set up a series of templates for simulation, prescription, contouring, treatment planning, and multiple checklists. Average time of activities’ completion and amount of planning errors were compared before and after the use of the customized ARIA to evaluate its impact on the efficiency and safety of radiotherapy.
RESULTS:
Completion time and on-time completion rate of the key activities in the care path are improved. The time of OAR/targets contouring decreases from (1.94±1.51) days to (1.64±1.07) days (p = 0.003), with the on-time completion rate increases from 77.4%to 83.3%(p = 0.048). Treatment planning time decreases from (0.81±0.65) days to (0.55±0.51) days (p < 0.001), with the on-time completion rate increases from 96.6%to 98.3%(p = 0.163). Waiting time of patients decreases from (4.50±1.83) days to (4.04±1.34) days (p < 0.001), with the on-time completion rate increases from 81.9%to 89.7%(p = 0.003). In addition, the average plan error rate decreases from 5.5%(2.9%for safety errors and 2.6%for non-normative errors) to 2.4%(1.6%for safety errors and 0.8%for non-normative errors) (p = 0.029).
CONCLUSION:
Our study demonstrates that the customized ARIA system has the potential to promote efficiency and safety in radiotherapy process management. It is beneficial to organize and accelerate the treatment process with more effective communications and fewer errors.
Introduction
The traditional quality assurance/quality control (QA/QC) contents and standards (as described in the AAPM TG-142 report) are keystones to ensure the quality and safety of the radiotherapy process. The consensus of the International Atomic Energy Agency (IAEA) 2007 Symposium pointed out that when advanced technology was introduced into clinical practice, the current equipment-based QA viewpoints should be modified with workflow-based viewpoints. The AAPM TG-100 report summarizes and establishes quality management programs based on risk analysis, which improves the effectiveness and efficiency of quality management [1].
ARIA is an oncology information system developed by Varian (Varian Medical Systems, Palo Alto, CA, USA). It has a variety of advantages in oncology information management, such as seamless connectivity across devices and platforms, quick access to information, integrated imaging, and assistance with regulatory compliance. In addition, this system is flexible for the users to develop their own extensions for different applications. The ARIA system holds the premise for customized local applications as it supports a variety of personalized templates, script development, analysis report customization, etc. In particular, the visual care path (VCP) in the ARIA system is designed to control all links in the whole care path and it facilitates the standardized management of the radiotherapy process [2]. To the best of our knowledge, no previous studies have been systematically conducted on the location design and practice of the ARIA system by combining with the AAPM TG-100 report. Based on quality management programs proposed in the AAPM TG-100 report, we have extensively explored and modified the functions of the ARIA system to maximize the localization application of the ARIA system, which has benefited in improving the radiation oncology information management, and the efficiency and safety of radiotherapy process in our institution.
Materials and methods
The software used in the current study mainly included ARIA (version 13.5) radiotherapy information management system, and Eclipse (Version 13.5) treatment planning system (TPS) (Varian Medical Systems, Palo Alto, CA, USA). The main equipment included a Philips Brilliance BigBore CT (Philips Healthcare, Netherlands), IX and 23EX linac of Varian. The capacity of treatment is over 200 patients per day, and the primary treatment mode is intensity-modulated radiation therapy (IMRT) (approximately 64%of total patients) in major (98%of all IMRT cases) by implementing volumetric modulated arc therapy (VMAT). Our quality improvement team carried out the Plan-Do-Check-Action (PDCA) method (as show in Fig. 1) to maintain the quality of our treatment. The details of this method are described below.

The flowchart of the PDCA loop.
The AAPM TG-100 report summarizes and establishes quality management programs and provides a basis for the care path design [3, 4]. Therefore, this step was divided into the following three parts: (1). Based on the AAPM TG-100 report, the quality improvement team carried out failure mode and effects analysis (FMEA) for the clinical process of our department, and further designed and established the quality management programs (protocols and standards, automation and computerization, double check system, etc.). (2). Customize the ARIA system based on the quality management programs provided by part 1. For example, we set up a series of templates and checklists, scan the bar codes to load the treatment plan, set peer review in the VCP. (3). Construct the visual care path (VCP) modules and build the VCP templates. In this process, the principle of minimizing human impact was strictly complied. Automatic care paths should be designed and used as much as possible. When a certain activity was completed, one or more subsequent activities will be activated automatically to minimize human ignorance. The optimized clinical process based on the AAPM TG-100 report needs to be improved gradually to achieve efficient and flexible.
“Do” step
The VCP modules and templates were tested before they were launched. We set a transition phase defined as a 2-month period from the customized ARIA system launched. A pilot run was carried out in a selected number of staff members in the first month and then all the corresponding members were involved in the second month.
“Check” step
Review meetings were called up every week to discuss the issues occurred in the pilot run. In order to evaluate the impact of the customized ARIA system on the efficiency and safety, we compared the timeliness and average days of activity completion before and after the launch of the customized ARIA system. The activities included in the analysis were the high-risk activities of the radiotherapy process based on FMEA, including the organ at risk (OAR)/targets contouring, the treatment planning, and the waiting time of patients (the days from CT simulation to the initial treatment). The impact of the safety of radiotherapy was evaluated by comparing the number of plan errors detected by the medical physicist during the plan review before and after the customized ARIA system was launched.
“Action” step
According to the feedback, we refined the VCP modules and templates to allow the customized ARIA system to achieve a balance of usability, effectiveness, and safety. The PDCA loop was iterated continually to optimize the customized ARIA system.
Data in the current study were presented for two time periods: the native ARIA system phase (2 months before the transition phase), 354 patients and 382 plans were included in this analysis; the customized ARIA system phase (2 months after the transition phase), 348 patients and 375 plans were included in this analysis.
An independent T-Test (SPSS 17.0, SPSS Inc., Chicago, IL, USA) was used to evaluate the differences in the average days of task completion, the on-time completion of tasks and the number of plan errors were evaluated by Chi Square Test. A value of p < 0.05 was defined as the significance level.
Results
Based on the value of O (occurrence), S (severity) and D (lack of detectability), we compute the risk priority number (RPN) values of the 216 failure modes and identified the risky activities. The distribution of RPN values is shown in Fig. 2. The activities with more high risky failure modes (RPN≥200) are treatment prescription, OAR/targets contouring, treatment planning/evaluation, plan approval, and treatment preparation. The activities with more high-severity failure modes are plan approval, treatment preparation and initial treatment. These activities need to be paid more attention on when designing the care path.
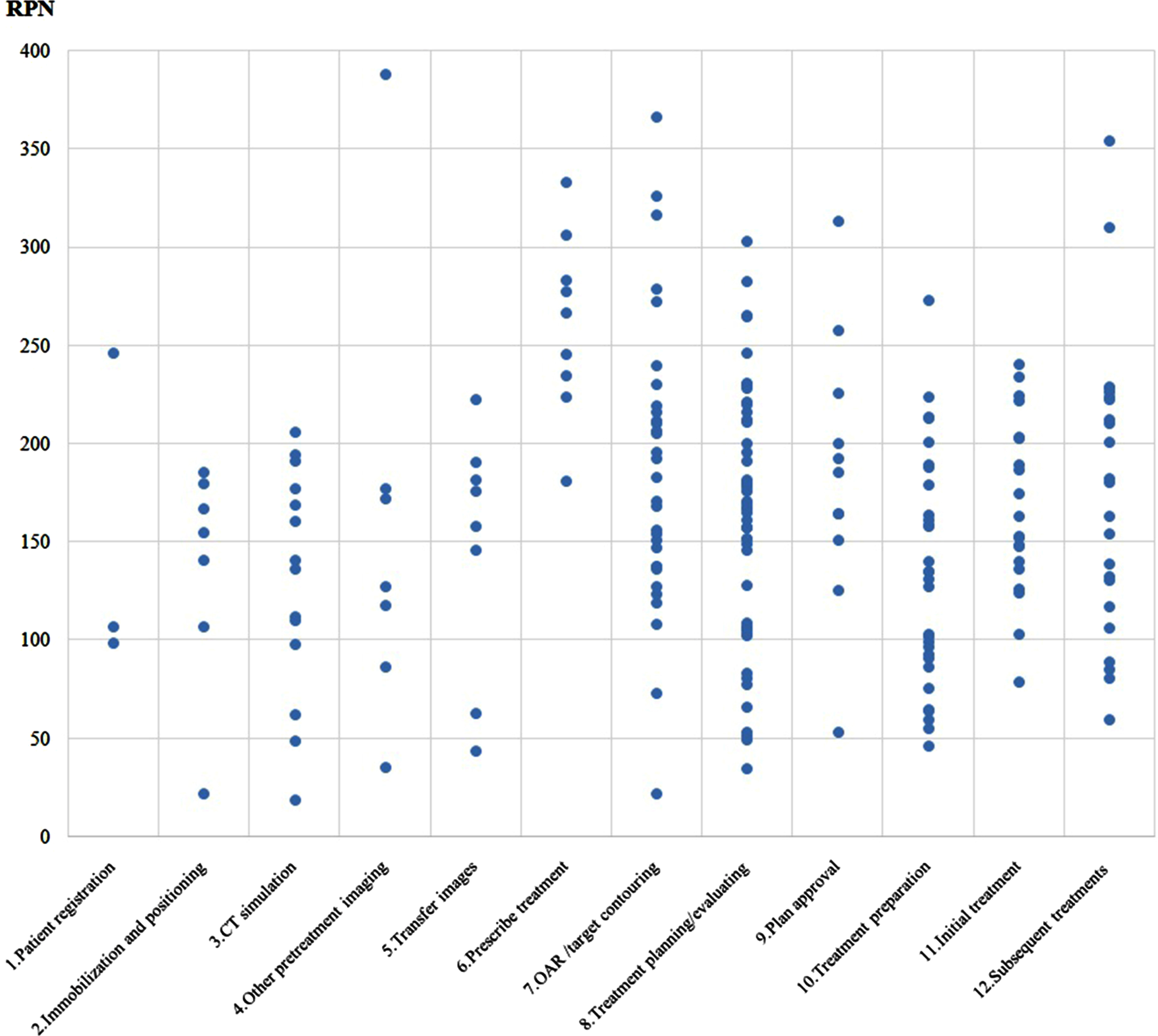
Distribution of RPN values in 12 activities of the IMRT process. Note: RPN values range from 18.9 to 387.8. The figure shows 12 steps of the IMRT process with the number of failure modes, including 1. Patient registration (3), 2. Immobilization and positioning (7), 3. CT simulation (14), 4. Other pretreatment images (7), 5.Transfer images (8), 6. Prescribe treatment (9), 7. OAR/ targets contouring (31), 8. Treatment planning/evaluating (53), 9. Plan approval (11), 10. Treatment preparation (30), 11. Initial treatment (20), and 12. Subsequent treatments (23).
The VCP management in the ARIA system can assist us to control all aspects of the radiotherapy process, to standardize management and collect data. After constructing the 15 activities needed for our clinical care path in the ARIA Data Administration, serial or parallel connections were made according to the execution sequence to build the customized VCP template. Figure 3 shows a template of the VCP for an IMRT process.

Example of an ARIA visual care path (VCP).
In addition, the use of templates was conducive to the standardized operations. Therefore, a variety of personalized templates were created in the ARIA system, including care path templates, positioning application form templates, electronic prescription templates, OAR/targets contouring templates, and planning templates.
In the native ARIA system phase, the activity completion time was obtained manually. In the customized ARIA system phase, the activity completion time was obtained by the customized statistics report automatically, and the time data statistics rules were consistent. The activities included in the analysis were the OAR/targets contouring, the treatment planning, and the waiting time of patients. The impact of the customized ARIA system on the safety of radiotherapy was evaluated by comparing the number of plan errors detected by the medical physicist during the plan review before and after the customized system was launched.
From the statistical results (refer to Table 1 and Table 2), it has been observed that after the customized ARIA system was launched, the days of activity completion and the rate of on-time completion had been improved to varying degrees. Among them, the time of OAR/targets contouring decreased from (1.94±1.51) days to (1.64±1.07) days, the on-time completion rate of activities increased from 77.4%to 83.3%; the days of treatment planning decreased from (0.81±0.65) days to (0.55±0.51) days, the on-time completion rate of activities increased from 96.6%to 98.3%; the days of simulation to treatment decreased from (4.50±1.83) days to (4.04±1.34) days, and the on-time completion rate of activities increased from 81.9%to 89.7%. When we evaluated the average completion time of high-risk activities, the completion rate of most activities increased to varying degrees after the system was launched, and the standard deviation of completion time decreased, which indicated that the consistency of the process had also been improved.
The average days of the completion of tasks
A: After the customized ARIA system was launched. B: Before the customized ARIA system was launched.
On-time completion statistics [n(%)]
A: After the customized ARIA system was launched. B: Before the customized ARIA system was launched.
The errors found in the process of plan review were mainly divided into safety errors and non-normative errors. The common safety errors included prescription errors, the overdose of OARs, incomplete contouring of OARs, failure to consider the influence of couch board (dose attenuation), wrong reference points, unreasonable planning parameters setting, suboptimal planning, etc. The non-normative errors included nonstandard plan name, nonstandard planning field name, and improper prescription name, etc. After the customized ARIA system was put into use, the average error rate of the plan was reduced from 5.5%(safety error and non-normative error were 2.9%and 2.6%, respectively) to 2.4%(safety error and non-normative error were 1.6%and 0.8%), (refer to Table 3).
Plan errors [n(%)]
A: After the customized ARIA system was launched. B: Before the customized ARIA system was launched.
Firstly, the automatic correlation between treatment plan and electronic prescription greatly reduced the probability of prescription error. Secondly, the use of contouring, treatment planning and optimization templates reduced the problems of overdose of OARs, incomplete contouring of OARs, the unreasonable setting of planning parameters, and nonstandard naming. Finally, the use of the checklists had played an important role in reminding and standardizing the activities. The customized ARIA system has not only improved the efficiency of process but also reduced errors.
Radiotherapy is commonly used to treat cancer patients in current clinical practice. Thus, improving its safety and efficiency is an important clinical issue [5]. In this study, the whole process quality control concept of the AAPM TG-100 report was introduced into the local practice of the ARIA system in our institution. Traditional QA/QC focused on the detection of mechanical and physical parameters of the equipment but paid little attention to the whole process of radiotherapy. Compared with intelligent machines, humans are more likely to make mistakes in operations. Most of the artificial errors and accidents in radiotherapy were probably caused by process defects and violations of operating procedures. Therefore, it is more meaningful to establish a comprehensive and efficient QA/QC program to ensure the safety of the whole treatment process. In the United States, Kalapurakal [6] and Ford [7] reported that the probability of radiotherapy errors ranged from 0.09%to 0.2%. Ma [8] introduced some new quality management methods of radiotherapy in recent years. Compared with the traditional methods focusing on equipment performance, the new quality management methods paid more attention to formulating corresponding risk management programs for possible errors in each activity of radiotherapy. Xie [9] reported that the probability of radiotherapy error decreased from 1.7%to 0.9%after the implementation of the whole process QA, which can effectively improve the accuracy and safety of radiotherapy. Since the customized ARIA system was put into use in our institution, it has promoted more rhythmic and organized operation of the radiotherapy process, improved the timeliness of activity completion, reduced the occurrence of radiotherapy errors, and improved the satisfaction of patients and staff. The possible reasons are described below.
The VCP in ARIA based on the actuality of our department worked effectively and safely. Kovalchuk [2] reported that the VCP of the Varian ARIA system helped to eliminate errors in a hurried environment and reduce the number of near-miss events. First of all, the circulation of activities was changed from the original manual round-trip delivery mode to the current network -driven, so as to realize the one-click flow of activities, which was efficient and fast. The activities of the care path were automatically pushed. That is, after completing an activity, one or more subsequent activities would be activated automatically, minimizing the impact of human factors. For example, when a cone-beam CT (CBCT)scan was completed, the system would automatically send the offline review task to the physician concerned, and the physician would input the review result into the system, then the therapist could obtain the feedback in the system before the next treatment. The customized ARIA system has successfully been used to manage the whole treatment process.
By setting a reasonable time limit and the number of activities, the reasonable and orderly operation of the process was ensured. Mohindra [10] reported that the implementation of standardized IMRT planning process improved the planning of treatment. Yeung [11] defined the completion time for each activity in the process through the time arrangement of standardized process: OAR/targets contouring for three days, treatment planning for two days (IMRT plan for three days), plan review and approval for one day, and therapist inspection for one day before treatment, so as to reduce the rush to complete the activity and ensure complete final safety inspection. When constructing the VCP, according to the actual situation of our department, this study also set the time limit for the completion of each activity and a reminder before the expiration of the activity so as to avoid the omission of the activity and reduce the possible error caused by the rush to complete the activity. In the process of appointment of CT simulation and the initial treatment, the number of patients was limited. Among them, the number of the CT simulation was limited to 14 patients/day, and the number of the initial treatment was limited to 8 patients/day. The limitation of the number of tasks reduced the fluctuation of tasks in the process and achieved balanced management so as to reduce errors caused by hasty completion of tasks or personnel fatigue, reduced the equipment failure rate, and provided more safe and high-quality care services for patients.
Peer review was an effective way of quality management [1]. In the design of the VCP in the ARIA system, the high-risk activities of the process, such as OAR/targets contouring, treatment planning, and plan initial evaluation, were added with contouring review, plan review, and plan final evaluation to realize peer review or superior review. The OAR/targets must be reviewed by the superior physician, so the VCP avoided physicians submitting plans bypassing superior physicians, thereby standardizing the process and reducing the possibility of errors. As shown in Fig. 1, in addition to OAR/targets contouring, plan evaluation, plan approval, and treatment preparation also included multiple serious failure modes. Therefore, we put the plan review after the treatment preparation. The physicist completed the plan review activities of each patient in the form of group discussion in the morning meeting every day, which ensured the double independent check of treatment plan and improved the safety of radiotherapy.
Checklists were widely used in key activities, which reduced the incidence of human errors. In other complex non-medical environments, such as the aviation industry [12], checklists had been successfully used to reduce human errors. Over the years, checklists had been widely used in both non-medical and medical fields and proved to be an effective tool for error management, as well as a key tool for reducing the risk of errors. Similar safety checklists in surgery had been shown to reduce patient mortality, reduce complications, and improve team communication [13]. Albuquerque [14] had developed a checklist in Elekta’s MOSAIQ electronic medical record. The use of the checklist ensured the standardization of the procedures and documents for the pretreatment examination of patients so as to improve the safety of patients and reduce the possibility of treatment errors. Donaldson [15] and Hende [16] also confirmed the role of the checklist in the safety of radiotherapy.
In our study, the content of the checklist was equivalent to a simplified version of the operating procedures, including the basic quality control elements of each step of the activity. In addition, the downstream activity checklist also contained the content of the upstream activity checklist, which implemented the redundant verification. Checklists could effectively reduce errors caused by interruptions and human errors. When dealing with critical activities, the risk caused by interruptions was unpredictable, the checklists and non-interruptions can reduce the risks [17]. Donaldson [15] and Hende [16] also gave suggestions in their report to minimize the interruption of the diagnosis and treatment process. When the activity was interrupted, the checklist could record the progress of the work at the time of interruption and resume the previous work to minimize the risk of interruption; Human error was usually related to inattention, distraction, or fatigue [1]. When an activity was completed, the key quality control points of the activity can be checked one by one with the checklist, which can effectively avoid human negligence mistakes. The second major cause for failure modes in the AAPM TG-100 report is the lack of standardized procedures. Clark [18] and others pointed out that the absence or deficiency of standard operating procedure (SOP) was related to errors. However, even if there were complete operating procedures, operators may still dismiss guidelines. The checklist provided a framework for managing and reducing the risk of errors due to negligence or omission. In addition, the use of checklists helped to standardize operations and reduce individual differences.
It is also helpful in improving the quality of our work by using a large number of templates. Standardization had many advantages, such as facilitating the data collection of clinical trials, making the data analysis between institutions more accurate, reducing the communication errors between department staff [19], and also conductive to the quality control of treatment plan [20]. For many of the most critical steps in planning and treatment, the standardization of the methods used solved many of the most common failure modes, and it was a key method to avoid training and process interruption. The use of templates was an effective means of operation standardization.
The standardized naming of the structure in the contouring template can effectively avoid the ambiguity caused by inconsistent or inappropriate naming, which also brought some difficulties to the later treatment planning and statistical analysis [21]. The standard naming method improved the clinical process by improving the way of information exchange, reduced the omissions and errors in planning evaluation, and improved the quality and safety of patients. The use of contouring templates reduced the time for doctors to create names for OAR/targets. At the same time, physicists can also asses the dose limit of corresponding organs and targets by the color of lines to improve the efficiency of treatment planning. By unifying the names and colors of OAR/targets within the department, it was conducive to the communication and connection of various processes, improve the overall operational efficiency of the department, improve the safety and quality of radiotherapy, and also provide the premise for the statistical analysis of big data in the future.
Using planning and optimization templates could simplify the operation steps of planning and shorten the planning time [22]. In the customized ARIA system, we had created a number of planning and optimization templates. Through the use of the planning optimization parameter templates, the physicists could reduce the repetitive work in the planning. At the same time, the use of planning and optimization templates also promoted standardization of planning and reduced the differences between individuals.
Conclusions
In this report, combined with the AAPM TG-100 report, the FMEA of the actual process of our department and the design of the quality management programs were carried out. The quality management programs were integrated into the localization design and practice of the ARIA system, which standardizes the radiotherapy process management and reduces the occurrence of radiotherapy errors.
Footnotes
Acknowledgments
This work was supported by the National Natural Science Foundation of China (No. 81872699).