Article commentary
Select search scope: search across all journals or within the current journal
A majority of adults with type 1 diabetes (T1D) are overweight (OW) or obese (OB) and often struggle to reach glycemic targets. Tirzepatide, a dual-incretin approved for type 2 diabetes (T2D) and OW/OB, has been shown to improve glucose control, reduce body weight, and insulin requirements in off-label adjunctive use for patients with T1D. This study evaluated changes in continuous glucose monitoring (CGM) data over 12-months of tirzepatide use in OW/OB adults with T1D.
This a single-center, retrospective, longitudinal case-control study included 61 OW/OB adults with T1D using tirzepatide and 54 computer-matched (for age, HbA1c, and weight) controls. CGM data were analyzed at baseline and every 3 months over a 15-month period (−3, 3, 6, 9, and 12 months). We assessed both within- and between-groups changes in CGM metrics from baseline at each time point.
Baseline characteristics were similar between tirzepatide-treated and control groups for age, HbA1c, and body weight. Compared with controls, tirzepatide-treated group significantly improved CGM metrics over 12 months. Time in range (TIR) was higher at 3 months (+4.6%,
We conclude that adjunctive tirzepatide treatment in OW/OB adults with T1D was associated with sustained improvements in CGM metrics over 12 months, without increased hypoglycemia risk in this real-world study. Proper long-term randomized control trials are needed to confirm our findings.
This is a visual representation of the abstract.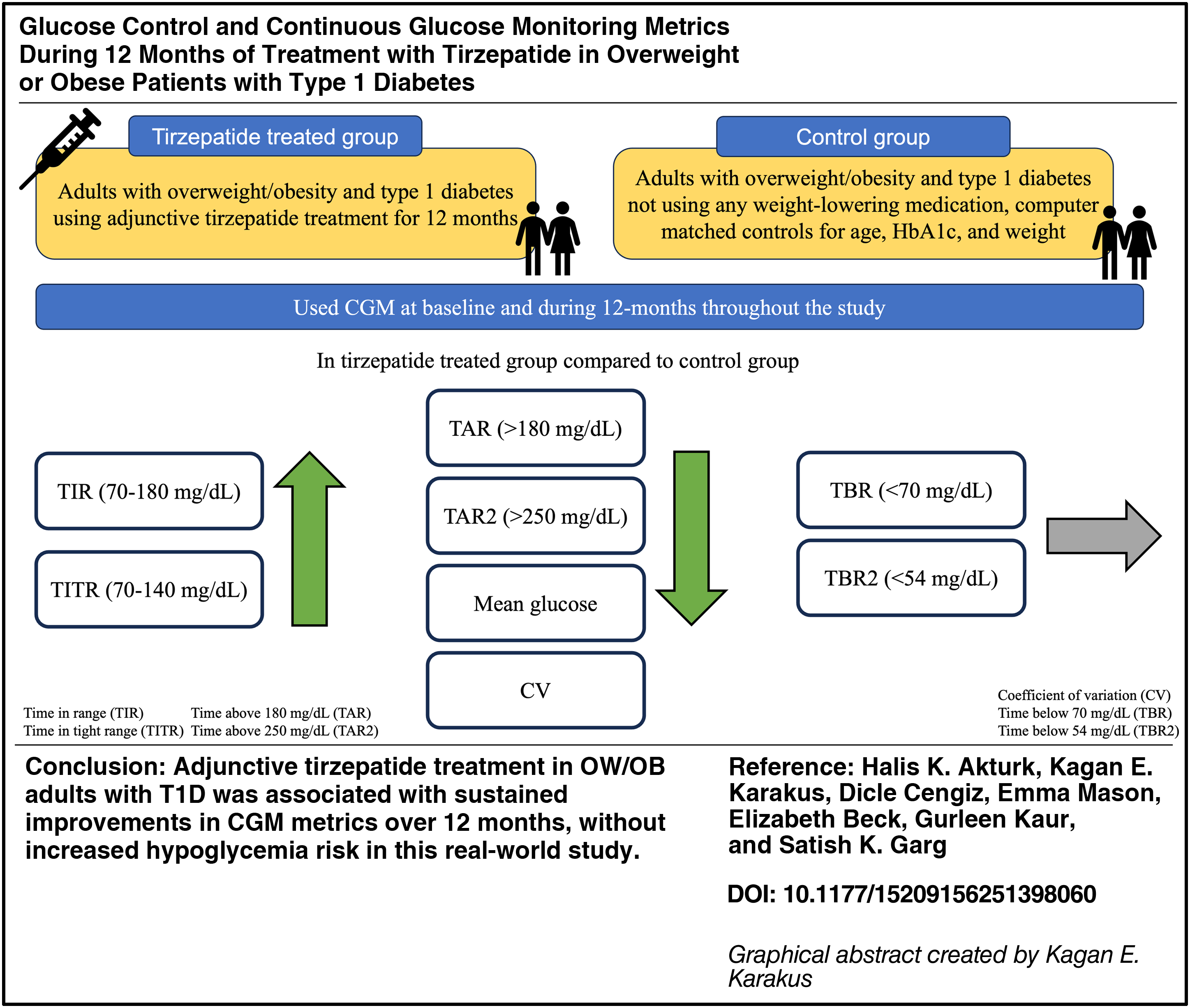
Inhaled insulin offers an alternative to subcutaneous administration, although concerns remain regarding pulmonary risks. We assessed the real-world safety of inhaled insulin versus rapid-acting analogue (RAA) insulin on lung malignancy and chronic obstructive pulmonary disease (COPD) in adults with diabetes.
This retrospective cohort study used the TriNetX Network to evaluate risk of lung malignancy and COPD in adults with type 1 or type 2 diabetes prescribed either inhaled insulin or RAA insulin.
After propensity score matching, between the inhaled insulin versus RAA insulin cohorts there was no difference in risk of any lung cancer (
No association was found between inhaled insulin and any lung malignancy. Inhaled insulin was associated with a threefold increase in COPD versus RAA although the absolute risk was low. The biological plausibility of this association is not definitive. Given the retrospective design and potential for ascertainment bias, causal inference is limited although findings underscore the need for continued evaluation of inhaled insulin’s pulmonary safety.
Time in range (TIR) has emerged as a key target in managing people with type 1 diabetes (PwT1D). The time spent in a glucose range of 70–180 mg/dL (3.9–10.0 mmol/L; TIR) is recommended to be >70%, which has been linked to reduced complication incidence. While frequently used in evaluating automated insulin delivery, TIR has rarely been applied in health economic assessments. This analysis therefore examined the impact of a 10-percentage point increase in TIR on clinical and economic outcomes for PwT1D.
Four baseline TIR levels (50%, 60%, 70%, 80%) and the investigated TIR increase were mapped to glycated hemoglobin (HbA1c) using two published statistical approaches. HbA1c estimates informed the IQVIA CORE Diabetes Model, projecting cumulative complication incidence, life expectancy, quality-adjusted life expectancy (QALE), and costs over 20 years from an English public health care system perspective. Cohort baseline data, complication costs, and utilities were sourced from an economic assessment by the National Institute for Health and Care Excellence. Sensitivity analyses were performed to assess the robustness of results.
A 10-percentage point TIR increase reduced the cumulative incidence of complications, by 15.6%–53.0%, 8.8%–47.1%, 8.1%–33.5%, and 10.1%–17.6% for ophthalmic, renal, neuropathic, and cardiovascular complications, respectively, when averaged across baseline TIR levels. Fewer complications translated into life expectancy gains of 0.031–0.051 years and QALE gains of 0.056–0.143 quality-adjusted life-years, with higher gains for lower baseline TIR. Total projected cost reductions versus constant TIR were 7.5%–9.9%, driven by reduced complication costs.
Long-term projections for England suggested that a 10-percentage point increase in TIR reduced diabetic complications in PwT1D, thereby reducing spending on complication treatment. Improvements were seen across baseline TIR levels but were disproportionately accrued in those with lower baseline TIR.
To evaluate long-term changes in glycemic control after switching from nonautomated insulin therapy to various automated insulin delivery (AID) systems in children and adolescents with type 1 diabetes (CwD).
This monocentric retrospective study included CwD under 20 years of age previously treated with multiple daily injections, continuous subcutaneous insulin infusion, or predictive low glucose management systems. Real-world data from 12 to 24 months following transition to AID were analyzed. Systems included the calibration-requiring Medtronic MiniMed™ 670G and noncalibration systems Medtronic MiniMed™ 780G and Tandem Control-IQ. Outcomes assessed included hemoglobin A1c (HbA1c), time in range (TIR), mean glucose, coefficient of variation, glycemia risk index (GRI), body mass index standardized deviation score, and total daily dose (TDD) of insulin. Nonparametric tests assessed between-system differences and longitudinal changes. Multiple linear regression analyses were performed to investigate factors influencing HbA1c.
Among 305 CwD initiating AID between 2019 and 2022, 83 (27.2%) used 670G and 222 (72.8%) used noncalibration systems. Across all groups, AID use led to significant improvements in TIR, time above range (181–250 mg/dL), time below range (<54 mg/dL), mean glucose, and GRI (all
AID systems improve key glycemic outcomes and reduce hypoglycemia compared with prior therapies. Noncalibration systems demonstrate superior performance over time. However, the initial HbA1c benefits wane after the first year, highlighting the need for strategies to sustain long-term metabolic improvements.
To obtain clinical features of diabetic ketoacidosis (DKA) in adults leading to hospital admission.
Multicenter observational study investigating DKAs treated in five German tertiary hospitals between 2022 and 2023.
A total of 179 patients with 203 episodes of DKA were registered: 64% of cases in pre-existing type 1 diabetes mellitus (T1DM), 14% in new-onset T1DM, 14% in pre-existing type 2 diabetes mellitus (T2DM), 3% in new-onset T2DM, 6% in latent autoimmune diabetes in adults, and 6% in pancreatogenic diabetes. Seven cases of SGLT 2 inhibitor (SGLT 2-I)-associated euglycemic DKA (EDKA) were encountered. In pre-existing T1DM, DKA occurred despite continuous glucose monitoring in 51% of patients and insulin pumps or automated insulin delivery in 24%. Only 21% of individuals with T1DM were in possession of ketone test and only 6% applied ketone testing. In total, 71% of patients with pre-existing T1DM experienced recurrent episodes of DKA. Suboptimal adherence to diabetes therapy was the most common triggering factor for DKA in known T1DM (56%), whereas infections contributed most in pre-existing T2DM (32%). The entirety of patients pretreated with SGLT2-Is and particularly also those with SGLT2-I associated EDKA were not educated concerning sick-day-rules. The inpatient mortality risk of DKA was 2.3% and restricted to multimorbid patients with known T2DM.
The clinical and etiological pattern of DKA is heterogeneous. Patients with pre-existing T1DM showed educational deficits concerning diagnostic and therapeutic measures to prevent DKA. Individuals with recurrent episodes of DKA require individual therapeutic concepts within the multidisciplinary diabetes care team. Emphasizing sick-day-rules in patients being treated with SGLT 2-Is is indispensable to prevent EDKA. Individuals with pre-existing T2DM represent a vulnerable group with severe comorbidities and high mortality risk due to DKA.
Preliminary research suggests that continuous glucose monitoring (CGM) can be used to guide food and lifestyle choices. The objective of the Using Nutrition to Improve Time in rangE (UNITE) study was to compare the glycemic and dietary impact of using either a nutrition-focused approach (NFA) or a self-directed approach (SDA) during CGM initiation in people with type 2 diabetes (T2D) not on insulin.
UNITE was a 60-day, two-arm, randomized clinical trial. The NFA arm was designed to help participants use CGM data to guide evidenced-based food choices to improve percent time in range with glucose 70–180 mg/dL (TIR70-180) and diet quality, whereas the SDA arm was designed to guide participants to use CGM data in any way that felt useful to them. Changes in outcomes from baseline (Base) to postintervention (Post) were estimated by arm and compared between arms using difference-in-differences; analyses were limited to those with adequate CGM data at Base and Post.
Adults (NFA:
Changes in mean TIR70-180 did not differ between the NFA and SDA arms; however, both arms experienced significant within-arm improvements, which support the use of CGM to improve glycemia in people with T2D not on insulin.
The CRISTAL trial indicated that advanced hybrid closed loop (AHCL) therapy with MiniMed™ 780G in type 1 diabetes pregnancy did not improve time in range (TIRp) compared with standard insulin therapy (SoC), but improved TIRp overnight and reduced time below range (TBRp). We aimed to evaluate the effect of AHCL therapy across different subgroups.
This secondary analysis of the CRISTAL randomized controlled trial compared glycemic outcomes (TIRp, TIRp overnight, TBRp, and TBRp overnight) averaged over the antenatal period (14-, 20-, 26-, and 33-weeks’ gestation) between the AHCL and SoC groups, within subgroups defined by baseline characteristics.
In women with baseline HbA1c <7.0%, the AHCL group (
AHCL therapy improved glycemic management in pregnant women with baseline HbA1c <7.0%, in women without prior AHCL use, and in women without higher education, indicating that AHCL might particularly benefit these subgroups.
This is a visual representation of the abstract.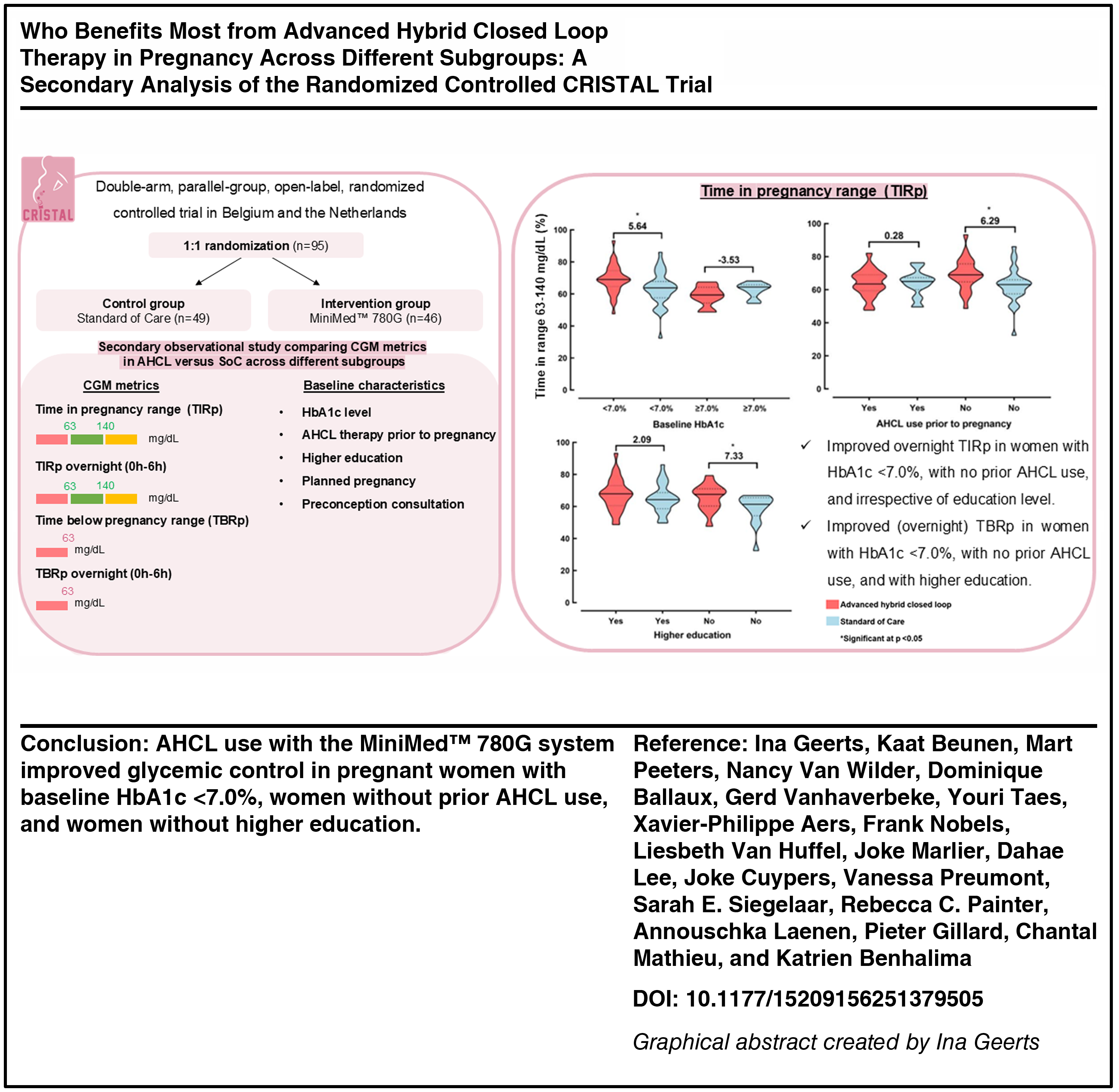
Rebound hyperglycemia (RHyper), rebound hypoglycemia (RHypo), extended hyperglycemia (EHyper), and extended hypoglycemia (EHypo) are newly defined continuous glucose monitoring (CGM) metrics. Here, we investigated the characteristics of these new metrics and the relationship between new CGM metrics and standard metrics.
In this retrospective cohort study, 30,000 CGM users with at least 90 days of CGM data were randomly selected from Dexcom Clarity database. Standard and new CGM metrics were calculated for each user. Four different cutoffs were used to define RHyper and RHypo, and two cutoffs were used to define EHyper and EHypo events. The number of RHyper, RHypo, EHyper, and EHypo events per week, mean duration of events, and mean area under the curve of events were calculated. For rebound events, the rate of change (ROC) was calculated. Pearson correlation and simple linear regression were used to analyze the data.
Mean time in 70–180 mg/dL was 61.8 ± 20.7%, mean glucose was 173 ± 37.1 mg/dL, and coefficient of variation (CV) was 32.1 ± 7.2%. RHyper, RHypo, and EHyper were more frequent during daytime and increased throughout the day. EHypo mostly occurred during nighttime. CV correlated strongly with RHyper (70–180 mg/dL) events/week (
For rebound and extended metrics, the most important metric was the number of events/week. RHyper and RHypo had a stronger correlation with CV and hypoglycemia metrics (TBR) than the correlation between CV and TBR. Thus, rebound events have the potential to detect hypoglycemia events caused by glycemic variability.
This is a visual representation of the abstract.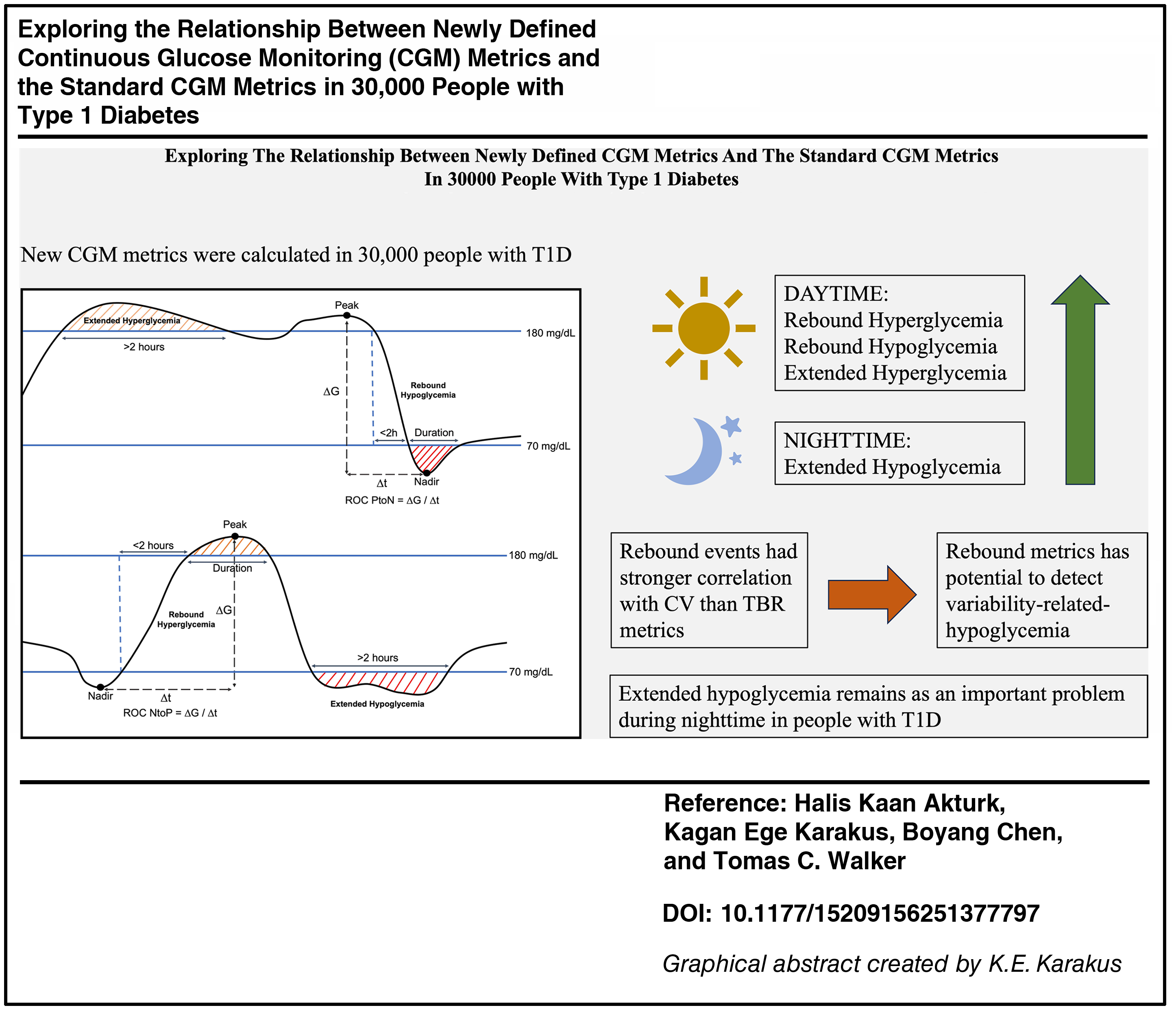
Glucagon-like peptide 1 receptor agonists (GLP-1 RAs) with or without glucose-dependent insulinotropic polypeptide (GIP) are Food and Drug Administration approved for patients with type 2 diabetes (T2D) and weight loss and are increasingly being used off-label in patients with type 1 diabetes (T1D). We evaluated all-cause mortality and health care resource utilization (HCRU) among patients with T1D receiving GLP-1 RA or GLP-1 RA/GIP dual agonist over a 2-year period.
Using the TriNetX database, we identified patients with T1D using ICD-10 codes, excluding those with T2D or sodium–glucose cotransporter-2 inhibitor use. Patients with T1D were divided into two cohorts of 4212 patients each based on whether or not they received a GLP-1 single/dual receptor agonist (comparison cohort vs. control cohort). We performed 1:1 propensity matching for demographics (age, sex, race), body mass index, hemoglobin A1c, and several comorbidities. Primary outcomes included all-cause mortality, HCRU, endoscopic procedures, and use of gastrointestinal prescriptions. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated for all outcomes except all-cause mortality, for which Cox regression analysis was performed to obtain the hazard ratio (HR) over 2 years.
The cohorts were predominantly white and female. Compared to the control cohort, patients taking GLP-1 single/dual receptor agonists had lower rates of all-cause mortality (HR = 0.18, 95% CI: 0.11–0.30,
These findings suggest that use of GLP-1 RA/GIP analogs in patients with T1D was associated with significantly lower HCRU, including hospitalizations and ED visits, and reduced all-cause mortality. Further studies are warranted to confirm these observational findings.
Gastroparesis (GP) is a well-recognized complication in patients with long-standing type 2 diabetes (T2D), impacting glycemic control and continuous glucose monitoring (CGM) metrics. We performed a prospective study to characterize real-time glucose metrics in patients with T2D with gastroparesis.
This pilot prospective study involved 11 adult patients with T2D and GP (GP group) and 20 patients with T2D without GP (non-GP group). Patients used real-time CGM (rtCGM) FreeStyle Libre 3 throughout the 4-week study. Fifteen glycemic metrics, including time in range (TIR), time above range (TAR), and time below range (TBR), were analyzed from the rtCGM profiles of study participants.
Compared with the non-GP group, patients in the GP group had higher mean CGM glucose levels (GP group [172 ± 51 mg/dL] vs. non-GP group [157 ± 41 mg/dL]) and lower TIR, indicating inadequate glucose control. The GP group also had greater TAR, increased TBR, and higher standard deviation (SD) and coefficient of variation (CV), indicating greater glucose excursions and glucose variability.
Patients with T2D and GP showed distinct and altered CGM glucose metrics compared with those with T2D without GP. These findings highlight the need for better glycemic control in this population. Whether CGM metrics could help identify a specific biomarker for gastroparesis remains to be determined. Further validation with a broader population, including patients with T1D and GLP-1RAs, is necessary.