Editorial
Thinking Fast,Slow,and Forever: Daniel Kahneman Obituary
Donald A. RedelmeierORCID
Select search scope: search across all journals or within the current journal
Willingness-to-pay (WTP) estimates are useful to policy makers only if they are generalizable beyond the moment when they are collected. To understand the “shelf life” of preference estimates, preference stability needs be tested over substantial periods of time.
We tested the stability of WTP for preventative dental care (scale and polish) using a payment-card contingent valuation question administered to 909 randomized controlled trial participants at 4 time points: baseline (prerandomization) and at annual intervals for 3 years. Trial participants were regular attenders at National Health Service dental practices. Participants were randomly offered different frequencies (intensities) of scale polish (no scale and polish, 1 scale and polish per year, 2 scale and polishes per year). We also examined whether treatment allocation to these different treatment intensities influenced the stability of WTP. Interval regression methods were used to test for changes in WTP over time while controlling for changes in 2 determinants of WTP. Individual-level changes were also examined as well as the WTP function over time.
We found that at the aggregate level, mean WTP values were stable over time. The results were similar by trial arm. Individuals allocated to the arm with the highest scale and polish intensity (2 per year) had a slight increase in WTP toward the latter part of the trial. There was considerable variation at the individual level. The WTP function was stable over time.
The payment-card contingent valuation method can produce stable WTP values in health over time. Future research should explore the generalizability of these results in other populations, for less familiar health care services, and using alternative elicitation methods.
Stated preferences are commonly used to value health care.
Willingness-to-pay (WTP) estimates are useful only if they have a “shelf life.”
Little is known about the stability of WTP for health care.
We test the stability of WTP for dental care over 3 y.
Our results show that the contingent valuation method can produce stable WTP values.
Medical diagnosis in practice connects to research through continuous feedback loops: Studies of diagnosed cases shape our understanding of disease, which shapes future diagnostic practice. Without accounting for an imperfect and complex diagnostic process in which some cases are more likely to be diagnosed correctly (or diagnosed at all), the feedback loop can inadvertently exacerbate future diagnostic errors and biases.
A feedback loop failure occurs if misleading evidence about disease etiology encourages systematic errors that self-perpetuate, compromising future diagnoses and patient care. This article defines scenarios for feedback loop failure in medical diagnosis.
Through simulated cases, we characterize how disease incidence, presentation, and risk factors can be misunderstood when observational data are summarized naive to biases arising from diagnostic error. A fourth simulation extends to a progressive disease.
When severe cases of a disease are diagnosed more readily, less severe cases go undiagnosed, increasingly leading to underestimation of the prevalence and heterogeneity of the disease presentation. Observed differences in incidence and symptoms between demographic groups may be driven by differences in risk, presentation, the diagnostic process itself, or a combination of these. We suggested how perceptions about risk factors and representativeness may drive the likelihood of diagnosis. Differing diagnosis rates between patient groups can feed back to increasingly greater diagnostic errors and disparities in the timing of diagnosis and treatment.
A feedback loop between past data and future medical practice may seem obviously beneficial. However, under plausible scenarios, poorly implemented feedback loops can degrade care. Direct summaries from observational data based on diagnosed individuals may be misleading, especially concerning those symptoms and risk factors that influence the diagnostic process itself.
Current evidence about a disease can (and should) influence the diagnostic process. A feedback loop failure may occur if biased “evidence” encourages diagnostic errors, leading to future errors in the evidence base.
When diagnostic accuracy varies for mild versus severe cases or between demographic groups, incorrect conclusions about disease prevalence and presentation will result without specifically accounting for such variability.
Use of demographic characteristics in the diagnostic process should be done with careful justification, in particular avoiding potential cognitive biases and overcorrection.
Recommendations regarding personalized lung cancer screening are being informed by natural-history modeling. Therefore, understanding how differences in model assumptions affect model-based personalized screening recommendations is essential.
Five Cancer Intervention and Surveillance Modeling Network (CISNET) models were evaluated. Lung cancer incidence, mortality, and stage distributions were compared across 4 theoretical scenarios to assess model assumptions regarding 1) sojourn times, 2) stage-specific sensitivities, and 3) screening-induced lung cancer mortality reductions. Analyses were stratified by sex and smoking behavior.
Most cancers had sojourn times <5 y (model range [MR]; lowest to highest value across models: 83.5%–98.7% of cancers). However, cancer aggressiveness still varied across models, as demonstrated by differences in proportions of cancers with sojourn times <2 y (MR: 42.5%–64.6%) and 2 to 4 y (MR: 28.8%–43.6%). Stage-specific sensitivity varied, particularly for stage I (MR: 31.3%–91.5%). Screening reduced stage IV incidence in most models for 1 y postscreening; increased sensitivity prolonged this period to 2 to 5 y. Screening-induced lung cancer mortality reductions among lung cancers detected at screening ranged widely (MR: 14.6%–48.9%), demonstrating variations in modeled treatment effectiveness of screen-detected cases. All models assumed longer sojourn times and greater screening-induced lung cancer mortality reductions for women. Models assuming differences in cancer epidemiology by smoking behaviors assumed shorter sojourn times and lower screening-induced lung cancer mortality reductions for heavy smokers.
Model-based personalized screening recommendations are primarily driven by assumptions regarding sojourn times (favoring longer intervals for groups more likely to develop less aggressive cancers), sensitivity (higher sensitivities favoring longer intervals), and screening-induced mortality reductions (greater reductions favoring shorter intervals).
Models suggest longer screening intervals may be feasible and benefits may be greater for women and light smokers.
Natural-history models are increasingly used to inform lung cancer screening, but causes for variations between models are difficult to assess.
This is the first evaluation of these causes and their impact on personalized screening recommendations through easily interpretable metrics.
Models vary regarding sojourn times, stage-specific sensitivities, and screening-induced lung cancer mortality reductions.
Model outcomes were similar in predicting greater screening benefits for women and potentially light smokers. Longer screening intervals may be feasible for women and light smokers.
The COVID-19 pandemic underscored the criticality and complexity of decision making for novel treatment approval and further research. Our study aims to assess potential decision-making methodologies, an evaluation vital for refining future public health crisis responses.
We compared 4 decision-making approaches to drug approval and research: the Food and Drug Administration’s policy decisions, cumulative meta-analysis, a prospective value-of-information (VOI) approach (using information available at the time of decision), and a reference standard (retrospective VOI analysis using information available in hindsight). Possible decisions were to reject, accept, provide emergency use authorization, or allow access to new therapies only in research settings. We used monoclonal antibodies provided to hospitalized COVID-19 patients as a case study, examining the evidence from September 2020 to December 2021 and focusing on each method’s capacity to optimize health outcomes and resource allocation.
Our findings indicate a notable discrepancy between policy decisions and the reference standard retrospective VOI approach with expected losses up to $269 billion USD, suggesting suboptimal resource use during the wait for emergency use authorization. Relying solely on cumulative meta-analysis for decision making results in the largest expected loss, while the policy approach showed a loss up to $16 billion and the prospective VOI approach presented the least loss (up to $2 billion).
Our research suggests that incorporating VOI analysis may be particularly useful for research prioritization and treatment implementation decisions during pandemics. While the prospective VOI approach was favored in this case study, further studies should validate the ideal decision-making method across various contexts. This study’s findings not only enhance our understanding of decision-making strategies during a health crisis but also provide a potential framework for future pandemic responses.
This study reviews discrepancies between a reference standard (retrospective VOI, using hindsight information) and 3 conceivable real-time approaches to research-treatment decisions during a pandemic, suggesting suboptimal use of resources.
Of all prospective decision-making approaches considered, VOI closely mirrored the reference standard, yielding the least expected value loss across our study timeline.
This study illustrates the possible benefit of VOI results and the need for evidence accumulation accompanied by modeling in health technology assessment for emerging therapies.
Liver transplantation is an alternative treatment for patients with nonresectable colorectal cancer liver-only metastases (CRLM); however, the potential effects on wait-list time and life expectancy to other patients on the transplant waiting list have not been considered. We explored the potential effects of expanding liver transplantation eligibility to include patients with CRLM on wait-list time and life expectancy in Norway.
We developed a discrete event simulation model to reflect the Norwegian liver transplantation waiting list process and included 2 groups: 1) patients currently eligible for liver transplantation and 2) CRLM patients. Under 2 alternative CRLM-patient transplant eligibility criteria, we simulated 2 strategies: 1) inclusion of only currently eligible patients (CRLM patients received standard-of-care palliative chemotherapy) and 2) expanding waiting list eligibility to include CRLM patients under 2 eligibility criteria. Model outcomes included median waiting list time, life expectancy, and total life-years.
For every additional CRLM patient listed per year, the overall median wait-list time, initially 52 d, increased by 8% to 11%. Adding 2 additional CRLM patients under the most restrictive eligibility criteria increased the CRLM patients’ average life expectancy by 10.64 y and decreased the average life expectancy for currently eligible patients by 0.05 y. Under these assumptions, there was a net gain of 149.61 life-years over a 10-y programmatic period, which continued to increase under scenarios of adding 10 CRLM patients to the wait-list. Health gains were lower under less restrictive CRLM eligibility criteria. For example, adding 4 additional CRLM patients under the less restrictive eligibility criteria increased the CRLM patients’ average life expectancy by 5.64 y and decreased the average life expectancy for currently eligible patients by 0.12 y. Under these assumptions, there was a net gain of 96.36 life-years over a 10-y programmatic period, which continued to increase up to 7 CRLM patients.
Our model-based analysis enabled the consideration of the potential effects of enlisting Norwegian CRLM patients for liver transplantation on wait-list time and life expectancy. Enlisting CRLM patients is expected to increase the total health effects, which supports the implementation of liver transplantation for CRLM patients in Norway.
Given the Norwegian donor liver availability, adding patients with nonresectable colorectal cancer liver-only metastases (CRLM) to the liver transplantation waiting list had an overall modest, but varying, impact on total waiting list time.
Survival gains for selected CRLM patients treated with liver transplantation would likely outweigh the losses incurred to patients listed currently.
To improve the total life-years gained in the population, Norway should consider expanding the treatment options for CRLM patients to include liver transplantation.
Other countries may also have an opportunity to gain total life-years by extending the waiting list eligibility criteria; however, country-specific analyses are required.
To calibrate Cancer Intervention and Surveillance Modeling Network (CISNET)’s SimCRC, MISCAN-Colon, and CRC-SPIN simulation models of the natural history colorectal cancer (CRC) with an emulator-based Bayesian algorithm and internally validate the model-predicted outcomes to calibration targets.
We used Latin hypercube sampling to sample up to 50,000 parameter sets for each CISNET-CRC model and generated the corresponding outputs. We trained multilayer perceptron artificial neural networks (ANNs) as emulators using the input and output samples for each CISNET-CRC model. We selected ANN structures with corresponding hyperparameters (i.e., number of hidden layers, nodes, activation functions, epochs, and optimizer) that minimize the predicted mean square error on the validation sample. We implemented the ANN emulators in a probabilistic programming language and calibrated the input parameters with Hamiltonian Monte Carlo–based algorithms to obtain the joint posterior distributions of the CISNET-CRC models’ parameters. We internally validated each calibrated emulator by comparing the model-predicted posterior outputs against the calibration targets.
The optimal ANN for SimCRC had 4 hidden layers and 360 hidden nodes, MISCAN-Colon had 4 hidden layers and 114 hidden nodes, and CRC-SPIN had 1 hidden layer and 140 hidden nodes. The total time for training and calibrating the emulators was 7.3, 4.0, and 0.66 h for SimCRC, MISCAN-Colon, and CRC-SPIN, respectively. The mean of the model-predicted outputs fell within the 95% confidence intervals of the calibration targets in 98 of 110 for SimCRC, 65 of 93 for MISCAN, and 31 of 41 targets for CRC-SPIN.
Using ANN emulators is a practical solution to reduce the computational burden and complexity for Bayesian calibration of individual-level simulation models used for policy analysis, such as the CISNET CRC models. In this work, we present a step-by-step guide to constructing emulators for calibrating 3 realistic CRC individual-level models using a Bayesian approach.
We use artificial neural networks (ANNs) to build emulators that surrogate complex individual-based models to reduce the computational burden in the Bayesian calibration process.
ANNs showed good performance in emulating the CISNET-CRC microsimulation models, despite having many input parameters and outputs.
Using ANN emulators is a practical solution to reduce the computational burden and complexity for Bayesian calibration of individual-level simulation models used for policy analysis.
This work aims to support health decision scientists who want to quantify the uncertainty of calibrated parameters of computationally intensive simulation models under a Bayesian framework.
Detection of colorectal cancer (CRC) in the early stages through available screening tests increases the patient’s survival chances. Multimodal screening policies can benefit patients by providing more diverse screening options and balancing the risks and benefits of screening tests. We investigate the cost-effectiveness of a wide variety of multimodal CRC screening policies.
We developed a Monte Carlo simulation framework to model CRC dynamics. We proposed an innovative calibration process using machine learning models to estimate age- and size-specific adenomatous polyps’ progression and regression rates. The proposed approach significantly expedites the model parameter space search.
Two multimodal proposed policies (i.e., 1] colonoscopy at 50 y and fecal occult blood test annually between 60 and 75 y and 2] colonoscopy at 50 and 60 y and fecal immunochemical test annually between 70 and 75 y) are identified as efficient frontier policies. Both policies are cost-effective at a willingness to pay of $50,000. Sensitivity analyses were performed to assess the sensitivity of results to a change in screening test costs as well as adherence behavior. The sensitivity analysis results suggest that the proposed policies are mostly robust to the considered changes in screening test costs, as there is a significant overlap between the efficient frontier policies of the baseline and the sensitivity analysis cases. However, the efficient frontier policies were more sensitive to changes in adherence behavior.
Generally, combining stool-based tests with visual tests will benefit patients with higher life expectancy and a lower expected cost compared with unimodal screening policies. Colonoscopy at younger ages (when the colonoscopy complication risk is lower) and stool-based tests at older ages are shown to be more effective.
We propose a detailed Markov model to capture the colorectal cancer (CRC) dynamics. The proposed Markov model presents the detailed dynamics of adenomas progression to CRC.
We use more than 44,000 colonoscopy reports and available data in the literature to calibrate the proposed Markov model using an innovative approach that leverages machine learning models to expedite the calibration process.
We investigate the cost-effectiveness of a wide variety of multimodal CRC screening policies and compare their performances with the current in-practice policies.
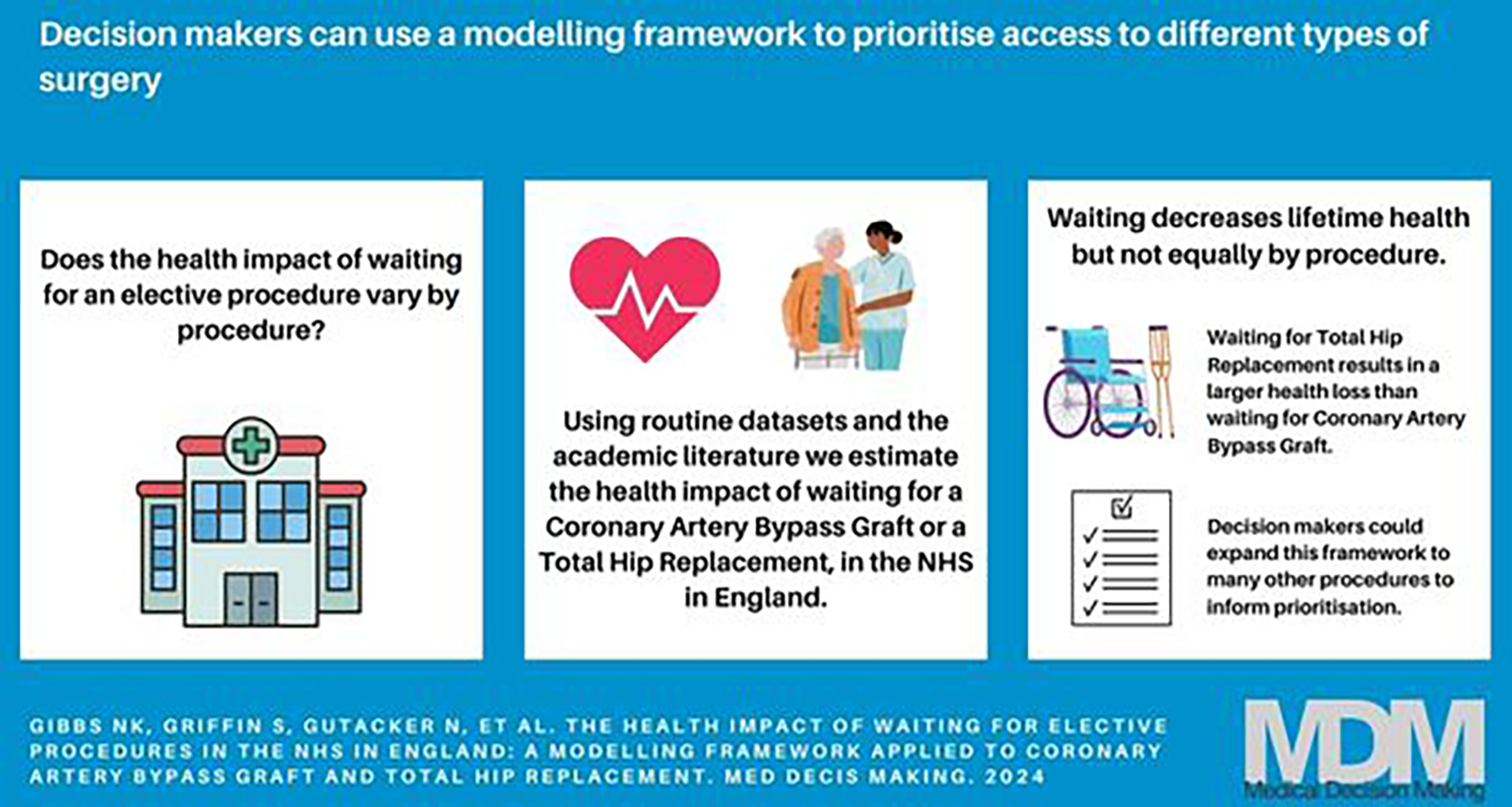
The aim of this study is to demonstrate a practical framework that can be applied to estimate the health impact of changes in waiting times across a range of elective procedures in the National Health Service (NHS) in England. We apply this framework by modeling 2 procedures: coronary artery bypass graft (CABG) and total hip replacement (THR).
We built a Markov model capturing health pre- and postprocedure, including the possibility of exiting preprocedure to acute NHS care or self-funded private care. We estimate the change in quality-adjusted life-years (QALYs) over a lifetime horizon for 10 subgroups defined by sex and Index of Multiple Deprivation quintile groups and for 7 alternative scenarios. We include 18 wk as a baseline waiting time consistent with current NHS policy. The model was populated with data from routinely collected data sets where possible (Hospital Episode Statistics, Patient-Reported Outcome Measures, and Office for National Statistics Mortality records), supplemented by the academic literature.
Compared with 18 wk, increasing the wait time to 36 wk resulted in a mean discounted QALY loss in the range of 0.034 to 0.043 for CABG and 0.193 to 0.291 for THR. The QALY impact of longer NHS waits was greater for those living in more deprived areas, partly as fewer patients switch to private care.
The proposed framework was applied to 2 different procedures and patient populations. If applied to an expanded group of procedures, it could provide decision makers with information to inform prioritization of waiting lists. There are a number of limitations in routine data on waiting for elective procedures, primarily the lack of information on people still waiting.
We present a modeling framework that allows for an estimation of the health impact (measured in quality-adjusted life-years) of waiting for elective procedures in the NHS in England.
We apply our model to waiting for coronary artery bypass graft (CABG) and total hip replacement (THR). Increasing the wait for THR results in a larger health loss than an equivalent increase in wait for CABG.
This model could potentially be used to estimate the impact across an expanded group of procedures to inform prioritization of activities to reduce waiting times.
A risk-stratified breast screening program could offer low-risk women less screening than is currently offered by the National Health Service. The acceptability of this approach may be enhanced if it corresponds to UK women’s screening preferences and values.
To elicit and quantify preferences for low-risk screening options.
Women aged 40 to 70 y with no history of breast cancer took part in an online discrete choice experiment. We generated 32 hypothetical low-risk screening programs defined by 5 attributes (start age, end age, screening interval, risk of dying from breast cancer, and risk of overdiagnosis), the levels of which were systematically varied between the programs. Respondents were presented with 8 choice sets and asked to choose between 2 screening alternatives or no screening. Preference data were analyzed using conditional logit regression models. The relative importance of attributes and the mean predicted probability of choosing each program were estimated.
Participants (
A deintensified screening pathway for women at low risk of breast cancer, especially one that recommends a later screening start age, would run counter to women’s breast screening preferences. Further research is needed to enhance the acceptability of offering less screening to those at low risk of breast cancer.
Risk-based breast screening may involve the deintensification of screening for women at low risk of breast cancer.
Low-risk screening pathways run counter to women’s screening preferences and values.
Longer screening intervals may be preferable to a later start age.
Work is needed to enhance the acceptability of a low-risk screening pathway.