
Abstract
Three-dimensional (3D)-printed modeling in the treatment of cerebrovascular diseases is rapidly developing. The present study aimed to evaluate the clinical and educational efficacy of 3D-printed models in surgical clipping of intracranial aneurysms. A single-center, randomized, controlled study was conducted for patients with a single unruptured aneurysm was clipped via a keyhole approach using a 3D-printed model at a 1:1 scale between September 2021 and August 2022. A total of 28 patients were enrolled (n = 13 in the case group, n = 15 in the control). The usefulness of the model was determined based on treatment outcomes, patient counseling, and physician education. Compared to the control group, the total operation time was shorter (median 91 min versus 125 min; p = 0.02) and the volume of blood loss was lower (median 119.6 mL versus 234.0 mL; p = 0.01) in the case group. Patients’ understanding of the operation improved significantly after counseling using 3D-printed models in all aspects (p ≤ 0.02). Although they failed to achieve a high rate of selecting a proper type of keyhole craniotomy (p = 0.71), trainees subjectively considered that the 3D-printed models were helpful. The 3D-printed aneurysm models were useful in improving the treatment outcomes, patient satisfaction with the preoperative counseling, and education of the surgical trainees.
Introduction
Three-dimensional (3D) printing has brought many changes in the medical industry, including changes in materials, devices, education, and research.1–3 There have also been attempts to help treat cerebrovascular diseases, such as intracranial aneurysms (IAs) and cerebral vascular malformations, using 3D-printed models.4–14 Previous studies have suggested that 3D-printed models with high fidelity provide a tactile anatomical overview, interactive surgical rehearsal, and an advantage in patient counseling. However, unautomated segmentation and limitations in surgical simulation, such as arachnoid dissection, long production time, and high cost, have been noted as obstacles.
Surgical clipping via keyhole approaches is a minimally invasive method that has some advantages, including a shorter operation time, lower complication rate, and better cosmetic outcomes.15–17 However, this approach has a disadvantage in that the learning curve is long in order to become an expert. Some experience and 3D spatial aptitude of an aneurysm, adjacent blood vessels, surrounding brain structures, and skull structures are necessary. Therefore, the 3D-printed model may be a good method to shorten the learning curve and achieve satisfactory surgical outcomes. The present study aimed to evaluate whether 3D-printed IA models are helpful in the surgical clipping of IAs via keyhole approaches in terms of surgical outcomes, patient counseling, and physician training.
Methods
From September 2021 to August 2022, a prospective randomized controlled study was conducted with the approval of the institutional review board of
Patient selection
The study was performed in strict adherence to the applicable guidelines and regulations set forth by the committee. The initial registration took place on August 18, 2021. The inclusion criteria were as follows: (1) patients diagnosed with a single unruptured IA in the anterior circulation on magnetic resonance angiography (MRA) or computed tomography angiography (CTA) and digital subtraction angiography (DSA) with 3D reconstructed imaging; (2) patients with IAs inappropriate for endovascular intervention in terms of shape, access, underlying medical conditions, and patient preference; (3) patients aged from 20 to 79 years; (4) patients with a tolerable healthy condition with a Karnofsky Performance Scale, 18 (KPS) ≥ 70 and modified Rankin Scale, 19 (mRS) ≤ 2; and 5) patients who agreed to surgical clipping via keyhole craniotomy.
Initially, 30 patients were enrolled in the present study (Fig. 1). Informed consent was obtained, and the patients were randomized into two groups, namely, case and control groups. We used a website (http://mahmoodsaghaei.tripod.com/Softwares/randalloc.html) to perform the randomization. Two patients in the case group were excluded after randomization, one due to the diagnosis of cancer during a preoperative routine work-up, and the other due to the cancellation of surgery caused by a change of mind.
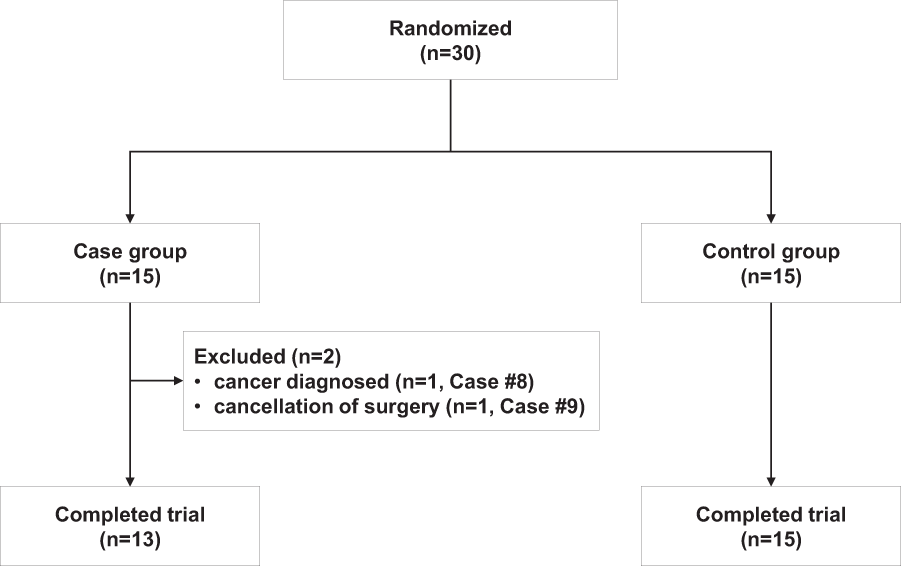
Diagram of patient enrollment.
The baseline characteristics of the patients are summarized in Table 1. Except for age, there were no significant differences in terms of the sex ratio and preoperative neurological status with KPS and mRS as well as the location and size of the IAs. The median age was 70 years old (range, 57–79 years) in the case group (n = 13) and 59 years old (range, 32–71 years) in the control group (n = 15), and the age was significantly different between the two groups (p < 0.01). The middle cerebral artery was the most common location of IAs (53.9% in the case group and 86.7% in the control group) followed by the anterior communicating and posterior communicating arteries.
Patient Characteristics
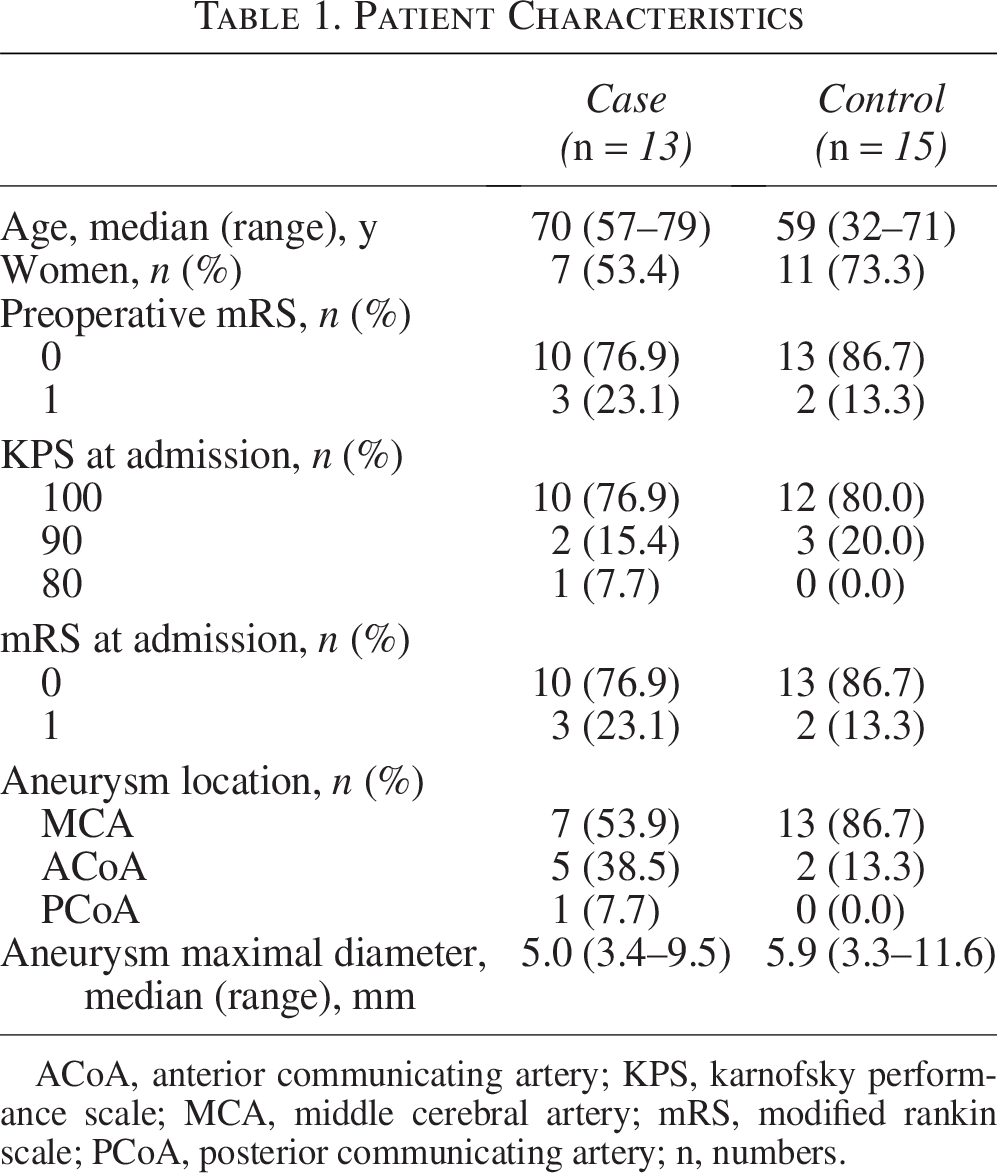
ACoA, anterior communicating artery; KPS, karnofsky performance scale; MCA, middle cerebral artery; mRS, modified rankin scale; PCoA, posterior communicating artery; n, numbers.
Segmentation, rendering, and modification of the 3D printed IA model
Most of the segmentation process for the skull and artery was automated using a program based on a machine learning-based threshold, region growing algorithms, and graph-cut algorithms (MEDIP PRO v2.0.0.0, https://medicalip.com/, MEDICAL IP Co. Ltd., Seoul, Korea). Axial source DICOM images were obtained from the CTA data. The 3D virtual models that are primarily rendered after segmentation can be interactively shared with physicians and manufacturers on the website by the MEDIP PRO software, through which the prototypes of 3D virtual models can be shared and modified.
A PolyJet 3D printer (Stratasys J750) was used with the following parameters: 600 dpi on the X-axis, 600 dpi on the Y-axis, 1800 dpi on the Z-axis of the resolution, and 20–85 microns (0.02–0.085 mm) for features below 50 mm and up to 200 microns (0.2 mm) for the full model size (for rigid materials only) in accuracy. The implementation of the 3D-printed models consisted of the following three stages: (1) creating a stereolithography file for 3D printing; (2) printing a primary model using a 3D printer; and (3) a postprocessing step, including manual editing. All the printed models were made at a scale of 1:1. The final product was fixed to a rotatable stand (Fig. 2). Finally, we investigated the cost of pure materials. The detailed methods of the 3D modeling are described in Supplementary Data S1.
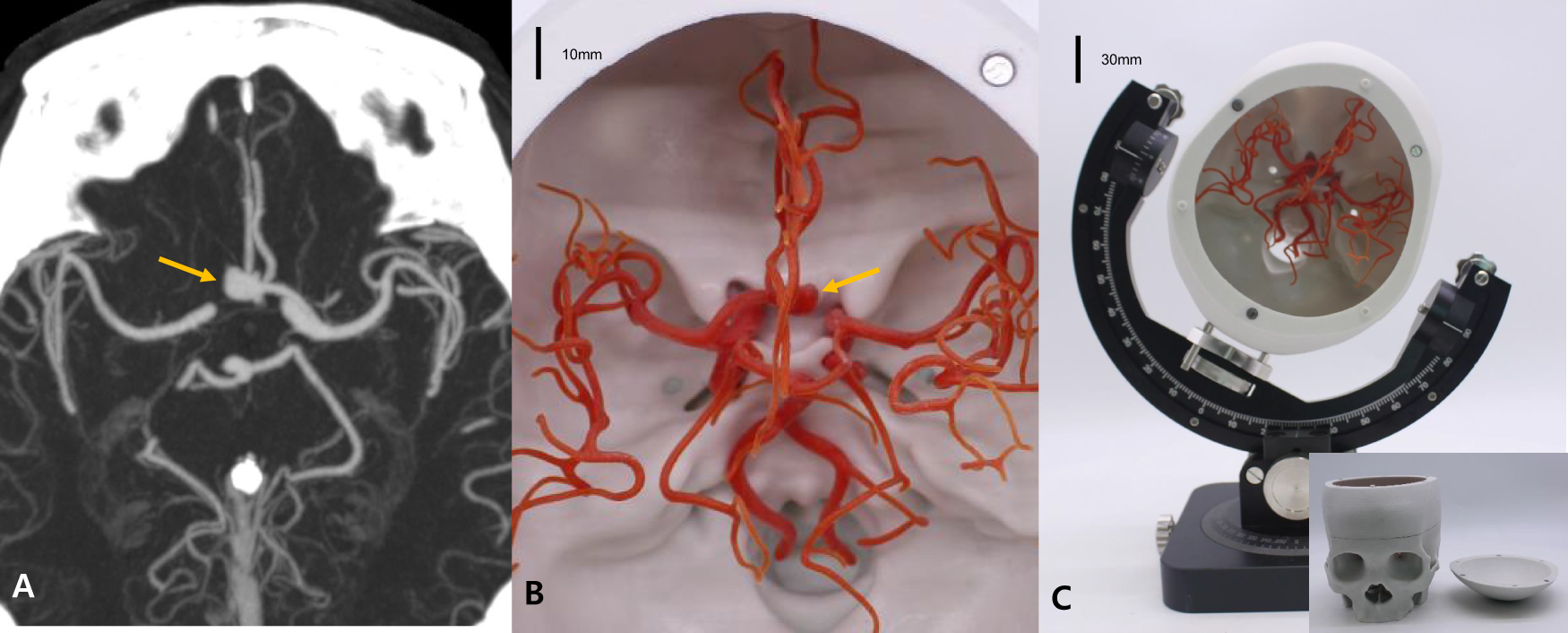
Setting of the three-dimensional printed aneurysm model (case #14).
Simulations and surgery
In the case group, a 3D printed IA model was made before the surgery, and surgical planning by the faculty and trainee as well as patient counseling and presurgical simulation with the model by trainees were conducted with a 3D printed model according to the predetermined schedule. In the control group, all the steps were conducted with preoperative conventional imaging with MRA or CTA and DSA.
In the present study, one of the trainees (Y.H.C., H.O., and H.C.L. consisting of three junior neurosurgeons with less than 4 years of experience) who was scheduled for the surgery conducted a presurgical simulation with a 3D-printed IA model (Fig. 3). By themselves, the trainees determined the appropriate type of keyhole approach among the frontolateral, lateral supraorbital, mini-pterional, mini-interhemispheric, and routine pterional approaches,15,16 and they also determined the optimal head position and the optimal type of aneurysm clip for the targeted IA. The accuracy of the trainee in predicting craniotomy type was compared between the two groups. The faculty who was willing to perform the main surgical procedure also determined the surgical plan based on the radiological data and a 3D printed IA model. Finally, 1 day before the surgery, faculty members (S.H.L., W-.S.C.) and one of the trainees discussed the surgical plan based on their own decision and decided on the final plan. Thereafter, the patient’s counseling was provided, and preoperative informed consent was obtained. At first, all patients from the two groups received preoperative counseling based on conventional radiological data alone. Then, patients in the case group had an additional explanation with their own 3D-printed IA model.
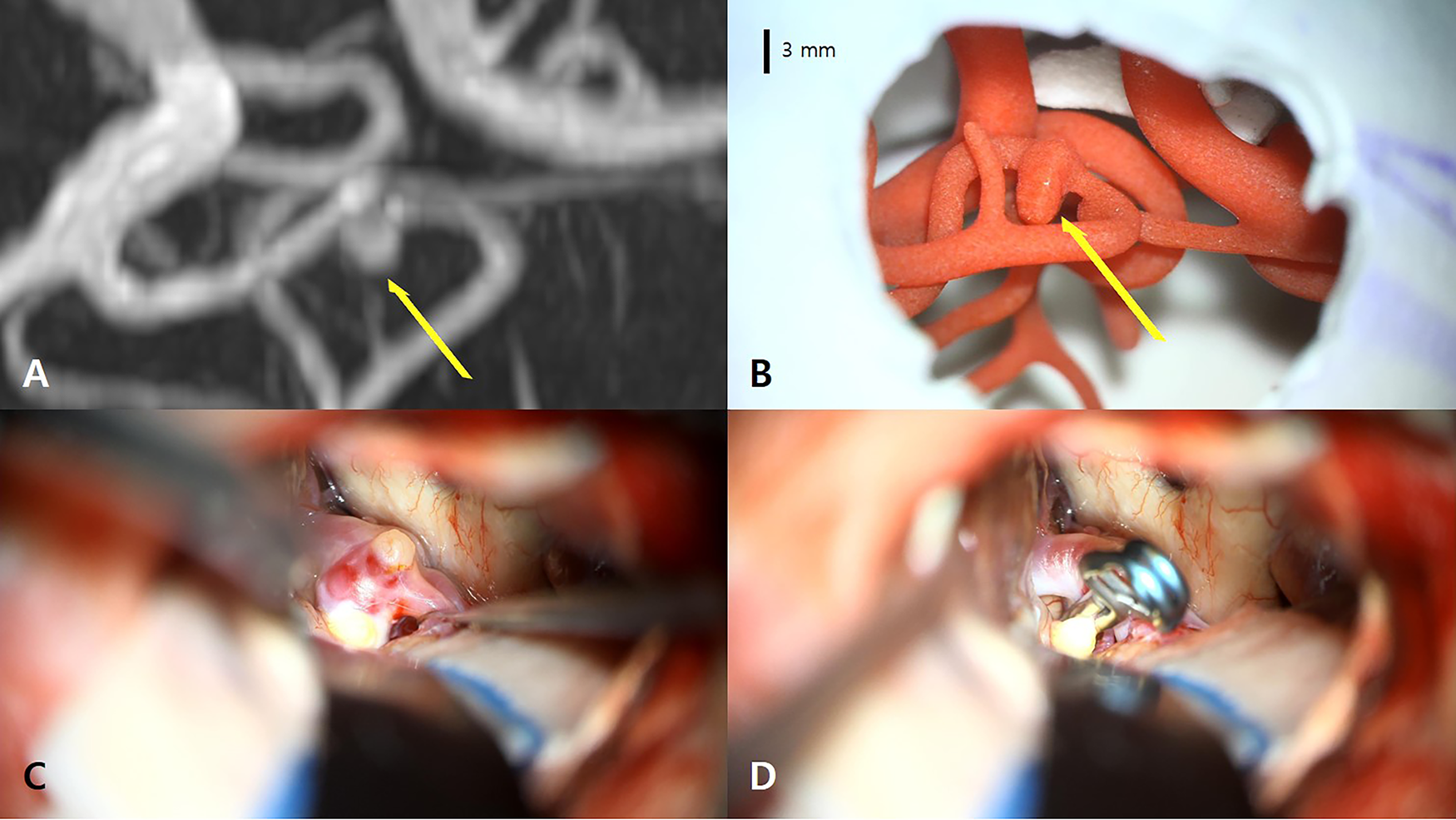
Simulation in case #11.
Surgery was performed in the following three steps: (1) Step 1: procedures involved from the skin incision to craniotomy; (2) Step 2: procedures involved from the dural opening via the main intradural procedure to dural closure; and (3) Step 3: procedures involved from the fixation of the bone flap to the closure of the scalp wound. Steps 1 and 3 were performed by one trainee who was scheduled for the operation, and step 2 was performed by one predetermined faculty member.
Evaluations
The operation time was recorded in three steps separately and as a whole. Immediate postoperative pain in the visual analogue scale (VAS) was evaluated just after the patient returned to the intermediate care unit. The length of stay in the intermediate care unit, the length of the entire hospital stay, complications related to surgery, and neurological conditions, including KPS and mRS at discharge, were investigated. The volume of blood loss (mL) in the operating theater was measured using the following formula: volume of blood loss = (total volume in the canister [mL]—irrigated fluid volume [mL]) + (weight change of the bloody surgical gauze [g] × 1/1.06 [mL/g] as a density of blood). 20 The results of IA clipping were classified as complete, residual neck, residual sac, or wrapping based on the intraoperative findings and postoperative CTA and/or DSA.
The survey was conducted on trainees, faculty, and patients (Supplementary Data S1
Statistical analysis
Continuous variables are presented as the median (range), and categorical variables are presented as frequencies (percentages). The Mann–Whitney U test, Fisher’s exact test, Cochran–Armitage trend test, and chi-squared test were used for comparisons. p < 0.05 was considered statistically significant. All of the statistical analyses were performed using SAS software (version 9.2; SAS Institute, Cary, NC).
Results
Treatment outcomes
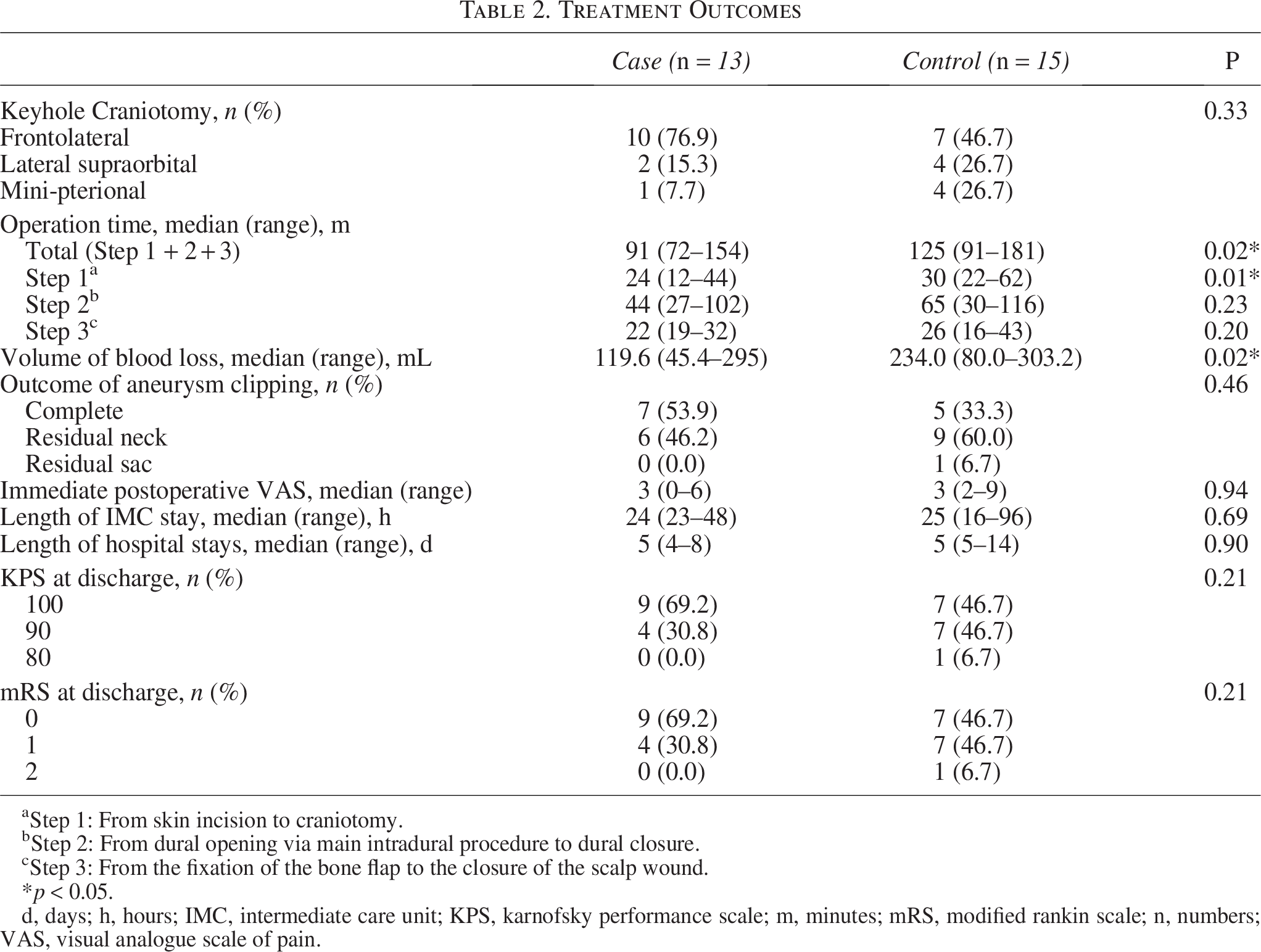
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request. Compared to the control group, the entire operation time and Step 1 operation time were significantly shorter in the case group (p = 0.02 and 0.01, respectively), while the volume of blood loss was also significantly lower in the case group (p = 0.02) (Table 2). The frontolateral approach was the most commonly performed among the keyhole craniotomies (10 in the case group and seven in the control group). The accuracy in predicting craniotomy type by the trainee was 7/13 in the case group and 7/15 in the control group (p = 0.71). In the case group, there was one case for which the final approach was changed after evaluating a 3D printed IA model. All cases in both groups, except one case in the control group, were satisfactorily clipped as complete and residual neck states (p = 0.46). Immediate postoperative VAS, length of intermediate care unit stay, length of hospital stay, and neurological status at discharge did not differ between the two groups. There were no cases of permanent morbidity or mortality. However, two cases experienced postoperative transient neurological deficits as follows: transient memory disturbance due to a small infarction at the territory of the anterior cerebral artery perforator (case #1 in the control group); and transient frontalis paralysis (case #11 in the control group). Repeat clipping for clip repositioning was performed in a patient with an aneurysm arising from the anterior communicating artery (case #1 in the control group) due to incomplete clipping identified on postoperative CTA.
Treatment Outcomes
Step 1: From skin incision to craniotomy.
Step 2: From dural opening via main intradural procedure to dural closure.
Step 3: From the fixation of the bone flap to the closure of the scalp wound.
p < 0.05.
d, days; h, hours; IMC, intermediate care unit; KPS, karnofsky performance scale; m, minutes; mRS, modified rankin scale; n, numbers; VAS, visual analogue scale of pain.
Surveys on counseling and education
According to the survey for the trainees’ evaluation of the usefulness of 3D-printed IA models, all the items were marked with at least a median score of 4 (Fig. 4). In the survey for the faculty evaluation, patient counseling and trainee education for appropriate craniotomy and patient positioning were marked with median high scores of 4 and 5. Moreover, the usefulness of 3D-printed IA models for faculty members was marked with lower median scores of 3 and 4.
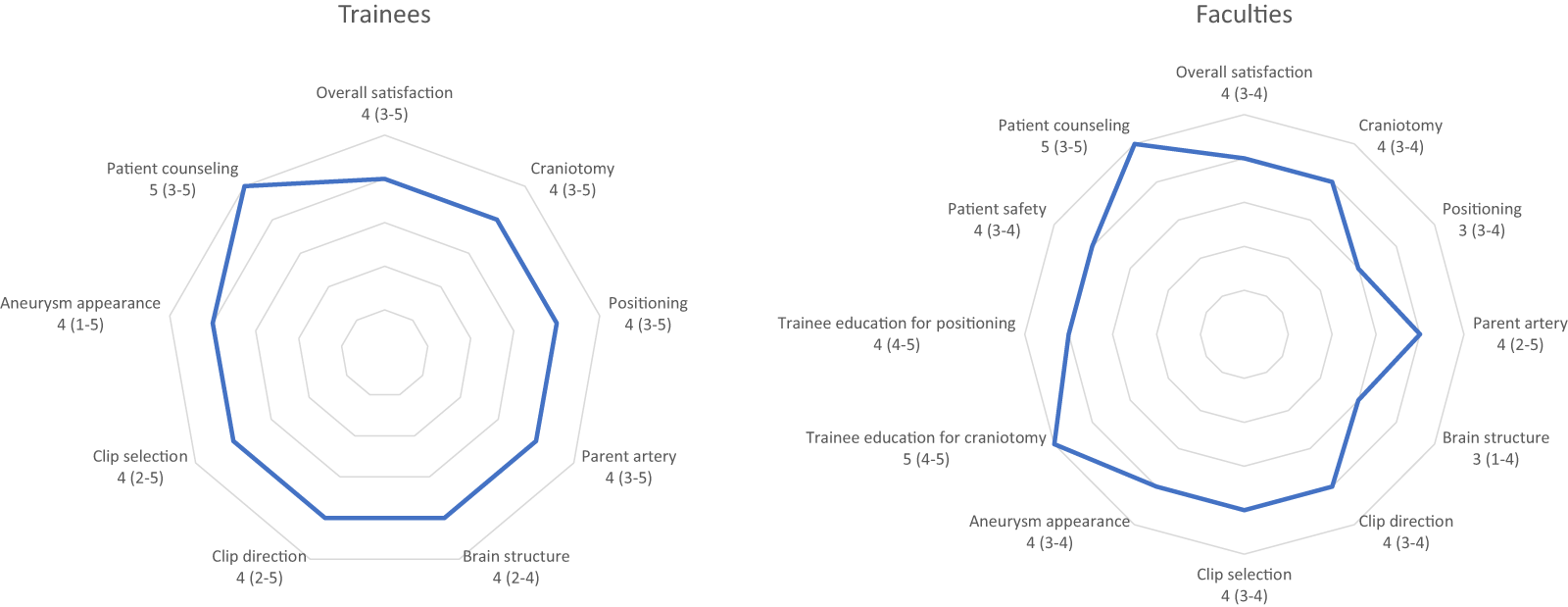
Results of the questionnaire for trainees and faculty members. That evaluated the degree to which the 3D model helped with surgery (median [range]).
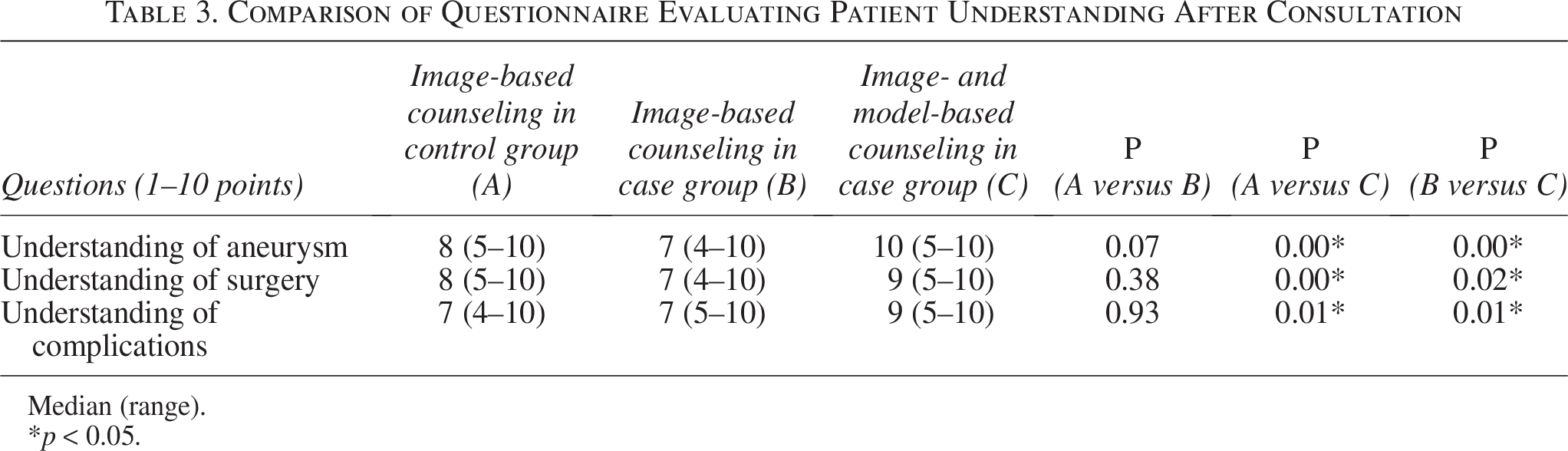
The results of the patient survey regarding preoperative counseling are shown in Table 3. There was no difference between the two groups in the score for understanding after image-based counseling alone. However, the scores in all items were significantly higher in the case group after counseling using the 3D- printed models as well as imaging data as follows: angioarchitecture of the IAs (median 10 [range 5–10] in the case group versus 8 [range 5–10] in the control group; p < 0.01); surgical procedures (median 9 [range 5–10] versus 8 [range 5–10]; p = 0.02); and possible complications (median 9 [range 5–10] versus 7 [range 4–10]; p = 0.01). In addition, the scores in all items were significantly different when compared before and after model-based counseling in the case group. Regarding the question of how much the patients were willing to pay if they would undergo surgery using the 3D printed IA models, the median cost was 1,000,000 KRW (range of 200,000–4,500,000 KRW).
Comparison of Questionnaire Evaluating Patient Understanding After Consultation
Median (range).
p < 0.05.
Cost and time to make a 3D-printed model
The median cost of raw materials used in a 3D-printed IA model was 126,197 KRW (range of 70,530–255,453 KRW). The median time for 3D-printed IA model production was 20.5 days (range of 14.5–28 days), including segmentation (median 2.5 days; range of 1.5–5 days), modeling (4 days in all cases), 3D printing (median 12 days; range of 6.5–19.5 days) and postprocessing (2 days in all cases).
Discussion
In the present study, the entire operation time and the time for craniotomy was significantly shorter in the case group compared to the control group, and the amount of intraoperative blood loss was lower in the case group than in the control group. However, 3D models were not helpful in the selection of an appropriate keyhole approach by the trainees. A survey regarding the usefulness of 3D printed IA models for surgery by trainees showed overall satisfactory responses in terms of counseling, education, and operation. Moreover, the faculty expressed higher satisfaction in terms of counseling and education than in terms of operation. The patients’ satisfaction with the preoperative counseling based on 3D-printed IA models as well as imaging data was higher than counseling based on imaging data alone in comparison between the two groups as well as before and after based on the 3D-printed IA model within the case group.
Since 3D printing technology was introduced into the medical industry, patient-tailored human models for surgical simulation and education as well as human replacement production (including implants for transplantation), drug delivery with nanoprinting technology and bioprinting are being developed.1,2 In particular, in the surgical field, a patient-specific 3D-printed model has been introduced, and there have been extensive attempts to use it to establish an optimal surgical plan through a 3D-printed model that is physiologically, anatomically and tactilely similar to reality. In this study, the thinnest part of the brain artery visible on the CTA measured 0.6 mm, and the PolyJet printer utilized in this study, with its minimum print thickness of 0.016 mm, was able to produce results of satisfactory quality. While fused deposition modeling-type printers are more economically feasible, their ability to render fine details is limited due to the lower resolution they can achieve. 1 Moreover, the PolyJet method offers the advantage of easier postprocessing, which is particularly beneficial when expressing intricate structures, such as those examined in this study.
Before performing brain surgery, it is important to understand the complex 3D structures of the skull, brain tissues, and vessels within the narrow intracranial space based on 2D radiological images to establish surgical plans. However, a long learning time through repeated surgical experience and cadaveric training is required to become an expert because 2D-based 3D planning in the neurosurgeons’ intellectual imagination as well as surgical skills are not easily established. A patient-tailored 3D-printed model can assist relatively inexperienced neurosurgeons to understand the anatomical structures and to make an appropriate surgical plan. 13
The number of surgical clippings continues to decrease every year due to the development of endovascular treatment,21–23 resulting in paradoxical situations, such as a decrease in the surgical experience of neurovascular surgeons and a relative increase in complex IAs that cannot be treated completely with neurointervention. As a result, the need to undergo systematic training for young cerebrovascular surgeons is increasing. 24 In addition, the growing social interest in patient safety and the generalization of medical litigation is inhibiting surgeons’ development. Therefore, 3D-printed modeling may be a good solution to overcome the lack of experience and achieve a satisfactory outcome.
Keyhole surgery is a minimally invasive surgical method with the advantages of minimizing patient inconvenience and reducing the duration of hospitalization compared to conventional surgery.15,17 However, the appropriate selection of the keyhole approach and adjusted craniotomy require some experience compared to the conventional approach. In that sense, 3D-printed IA models are expected to provide an effective opportunity for education and training. Although the selection of an appropriate keyhole craniotomy by trainees was not satisfactory in the present study, the clinical efficacy was demonstrated in terms of reduction in operation time and intraoperative blood loss. Selection of an appropriate approach is thought to require more than just modeling of skull and intracranial arteries, such as relationship with the brain parenchyma, availability of clipping, and possible complications during the surgery.
However, there are still a few obstacles for 3D-printed modeling to overcome before becoming a final solution. First, the production time is long. In the present study, an average of 19 days was required to produce the model because it did not require rapid production. However, other studies have reported that at least approximately 24 h (usually several days) was required to produce the model. 2 Second, direct simulation by using actual surgical instruments is possible only during craniotomies, which may have affected the results of the present study with a significantly shorter craniotomy time and less bleeding volume. It should also be noted that possible carcinogenesis by 3D printing materials has recently been reported. 25 Third, it is still inconclusive whether 3D-printed models can be provided at a reasonable price. There seems to be a discrepancy between the expectation and the actual cost of materials and intangible efforts. Fourth, due to limitations in imaging quality and materials, some tissues, such as the brain parenchyma, venous channels, membrane of the arachnoid, and membrane of pia, cannot yet be reproduced. However, such limitations are expected to soon be overcome according to technical advancements. Virtual reality and augmented reality are emerging technologies, and they may be able to compensate for the shortcomings of 3D printing. 26 However, there is a clear distinction in that direct surgical practice using a real model is possible.
The present study had the strength of a prospective randomized trial and evaluation of objective factors to demonstrate clinical efficacy. However, the present study also had some limitations. First, the number of cases was small, and the study was conducted in a single institution. Second, the 3D model used in the present study was an incomplete model that lacked hair, skin, and brain tissues. In a pilot study, we attempted to reproduce skin and brain tissues, but they were not finally applied because they were not realistic.
In the present study, the 3D-printed IA models helped perform surgery by reducing surgical time and bleeding volume. Compared to conventional image-based counseling, the application of the 3D-printed model improved patient understanding and satisfaction. The 3D-printed models also helped surgeons in both clinical and educational aspects. To date, the 3D-printed models have limits in reproducibility and economic feasibility. However, these limits are expected to be resolved through the development and universalization of technology.
Authors’ Contributions
W.-S.C.: Conception, methodology, project administration, and resources. S.H.L. and W.-S.C.: Writing—original draft. S.H.L., Y.H.C.: Visualization. Y.H.C., H.O., H.C.L. and J.P.: Data curation. S.H.L., W.-S.C.: Formal analysis. M.P. and S.J.P.: Software. J.E.K. and C.-K.P.: Supervision. All authors: Review.
Footnotes
Acknowledgment
The authors wish to thank Sulgina Kim and Da-yeong Lee for manufacturing the 3D-printed models.
Author Disclosure Statement
S.J.P. is the founder and CEO of MEDICALIP. C.K.P. owns stock options in MEDICALIP. M.P. is a researcher at MEDICALIP. Other authors have no conflict of interest to declare.
Funding Information
This research was supported by a grant from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute, funded by the Ministry of Health and Welfare, Republic of Korea (grant number: HI20C2092), and a grant from the SNUH Research Fund (grant number: 1120215060).
Disclosure of Artificial Intelligence (AI)-Assisted Technology
No AI technology was used when writing this article.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.