
Abstract
Traditional immunotherapy for patients with refractory metastatic renal cell carcinoma (RCC) is limited because the tumors themselves induce immunosuppression. The aim of this article was to evaluate the clinical efficacy of the infusion of a high dose of interleukin (IL)-2-activated allogeneic haploidentical peripheral blood stem cells (haplo-PBSCs) in patients with advanced intractable RCC. Ten advanced RCC patients and their haploidentical relatives, who were haplo-PBSC donors, were enrolled in this study. All patients accepted one cycle of activated haplo-PBSCs. The clinical and immunologic responses were evaluated. A range from 2.3 to 5.5×1010 of activated haplo-PBSCs were harvested after exposure to recombinant human IL-2 (rhIL-2), along with a significant increase in the proportion of natural killer cells and activated lymphocytes (CD69+ and CD25+). Enhanced cytotoxicity of haplo-PBSCs for RCC was also observed. After treatment, 2 (2/10) cases of partial remission, 6 (6/10) cases of stable disease, and 2 (2/10) cases of progressive disease were identified in these 10 patients. The median progression-free survival of the 10 patients was 5.5 months (3–14 months). The adoptive transfusion of IL-2-activated haplo-PBSCs can induce sustained antitumor effects for advanced intractable RCC patients who have had no response to conventional immunotherapy.
Introduction
Renal cell carcinoma is the most frequent type of malignant carcinoma in the urinary system with an incidence rate that is rising every year. Most patients with early-stage renal carcinoma can be effectively treated using several therapeutic applications, such as surgical removal of the primary tumor and biotherapy. However, 30%-40% patients have metastases at the time of initial diagnosis and have extremely poor prognoses with a median survival of less than 1 year. 1,2 In such cases, systemic treatment with cytotoxic chemotherapy is usually ineffective. A few patients have complete response to cytokine-based therapies, such as high doses of interleukin-2 (IL-2) and interferon-gamma (IFN-γ), and survive for long periods of time. 3,4 However, the overall rate of response to these agents, either alone or in combination, is still usually less than 20%. 5
Renal cell carcinoma (RCC) is unusual among solid tumors because of its immunogenic properties. 6,7 The response of certain patients to immunomodulatory cytokines and the rare spontaneous regression of metastatic diseases suggest that other immunologic approaches can be used for the treatment of RCC. 8,9 In the last few years, studies using allogeneic stem cell transplantation (allo-SCT) have shown that allogeneic lymphocytes, which are derived from healthy human leukocyte antigen (HLA)-matched or haplo-matched donors and have not been previously subjected to tumor-derived suppression, can distinguish allogeneic major histocompatibility complex (MHC)-I/II molecules from combined tumor antigens on the surface of tumor cells. 10 This finding indicates that allogeneic peripheral blood stem cells (allo-PBSCs) may have great potential as an application for cancer immunotherapy.
The overt antineoplastic activity of large dose IL-2-activated HLA haploidentical peripheral blood stem cells (haplo-PBSCs) therapy for 11 refractory metastatic solid tumors without pretreatment was previously reported. 11 Evaluated in this study are the antitumor effects of an adoptive transfusion of IL-2-activated haplo-PBSCs as a single agent to treat 10 patients with metastatic and chemoresistant RCC. Here, all of the patients receiving this treatment showed significant therapeutic responses, including improved clinical symptoms, shrinkage of metastatic tumors, and a positive modulation of systemic immunologic status.
Materials and Methods
Patient and donor characteristics
Eligible patients were between 45 and 80 years old and had biopsy-confirmed metastatic RCC that was radiographically documented to be progressive, despite prior second or third line therapy involving IFN-α and IL-2. Patients were required to have tumors that could be evaluated radiographically. Each patient had a HLA haplotype identical donor, which was either a parent or a child. Patients were excluded if they had bone or brain metastasis, or if they had received any treatment for RCC within 30 days of enrolment.
HLA typing
HLA-A, B, DR, and C loci in paired patients and donors were assessed for HLA compatibility by polymerase chain reaction using sequence-specific primers (PCR-SSP). The matching of at least three of the six HLA-A/-B/-DR loci was defined as halploidentification. Alloreactivity induced by mismatches at the killer immunoglobulin-like receptor (KIR) epitopes between paired patients and donors was evaluated by HLA-C typing. On the basis of the codon-determining amino acid at position 80, alleles of the HLA-C locus were divided into two distinct groups: KIR-epitope-mismatched in the graft versus host (GVH) direction and KIR-epitope-mismatched in the host versus graft (HVG) direction, which means that donor graft contained cells expressing inhibitory KIRs whose specific ligands were absent on recipient tissues. Conversely, the absence in donors of recipient HLA-C alleles was defined as KIR-epitope-mismatched in the host versus graft (HVG) direction.
Treatment design
Written informed consent was obtained from each patient and his or her respective donor. The trial was approved by the ethics review committee of Tianjin Cancer Institute and Hospital. Every patient accepted one cycle of infusion of high-dose IL-2-activated haplo-PBSCs.
HLA haploidentical donors were mobilized with 10 μg/kg×d of granulocyte colony-stimulating factor (G-CSF) for 3 days before apheresis using the CS3000 plus cell separator (Baxter Healthcare Corp.). Apheresis was performed on two consecutive days until a minimum of 3×1010 PBSCs were obtained. The haplo-PBSCs in fresh apheresis products were separated by gradient centrifugation at 1800 rpm for 18 minutes and activated by 5000 IU/mL of rhIL-2 in serum-free X-VIVO 20 medium, for 4 hours at 37°C under 5% CO2 before being transfused into patients. A portion of sample aliquots were saved for functional examination.
To prevent fever and shivering, which are commonly seen in the allogeneic haematopoietic stem cell transplantation (allo-HSCT), indomethacin (25 mg) and hexadecadrol (5 mg) were given before the infusion of haplo-PBSCs. Patients who developed hematolymphoid toxicity, infection, immunosuppression, graft versus host disease (GVHD) or other side-effects were immediately symptomatically treated. Patients received maintenance treatment if they had been presented with no disease progression at the time responses were evaluated. On the other hand, patients who had been presented with progressive disease at the time of evaluation were eligible to receive other therapies upon request.
Bioactivity assay of activated haplo-PBSCS
The phenotypes of haplo-PBSCs were examined by flow cytometry. Cells (5×105) were suspended in 20 μL of phosphate-buffered saline (PBS) containing 2% newborn calf serum and 1% sodium azide. Then, the cells were incubated with 5 μL of the appropriate fluorescein isothiocyanate (FITC)/PE/PerCP-labeled CD4/CD8/CD3, FITC/PE/PEcy5-labeled CD3/CD16 +CD56/CD45, FITC/PE-labeled CD4/CD25, CD8/CD28, CD45RO/CD8, and FITC-labeled CD69 monoclonal antibodies (BD Pharmingen) for 30 minutes at 4°C. Following incubation, the cells were sorted on a flow cytometer (X-100; Beckman-Coulter) and analyzed using the Expo II software. Isotype-matched IgG1 (BD Pharmingen) was used as a control. Background staining using irrelevant antibodies was less than 2%.
The cytotoxicity assay of haplo-PBSCs against renal carcinoma cell lines was performed using a Cyto Tox 96 nonradioactive cytotoxicity assay (Promega). Briefly, 1×105 cells/mL of the target cells (GRC-1, renal cancer cell line) were seeded in a U-bottom 96-well tissue culture plate in triplicate. Activated haplo-PBSCs or untreated PBSCs were seeded at decreasing effector/target(E/T) ratios of 40:1, 20:1, and 10:1. After 4 hours of incubation, 50 μL aliquots from the supernatants of each well were transferred to a new flat 96-well plate. Then, 50 μL of the substrate mixture was added to each well of the plate, followed by incubation at room temperature for 30 minutes in the dark. Subsequently, 50 μL of the stop solution was added to each well, and the absorbance was measured at 490 nm using a 96-well plate enzyme-linked immunosorbent assay (ELISA) reader (Multiscan, Finland). Cytotoxicity was calculated using the following formula:
Basal release of the tumor targets was <5%. All experiments were performed in triplicate and the mean values were calculated.
Assessment of clinical response and toxic reaction
Clinical responses were assessed with respect to a relief of symptoms, improvement in quality of life [using the Karnofsky performance scale index (KPS)], and a shrinkage of primary and metastatic tumor size as detected by computed tomography (CT) scans. Clinical antitumor responses were determined using the following response Evaluation Criteria In Solid Tumors: a response was defined as complete response (CR) if all measurable tumors disappeared; as partial response (PR) if the sum of the longest perpendicular diameters of metastatic lesions decreased by at least 30% for a period of at least 30 days; as progressive disease (PD) if the sum increased by 20% or more or if new manifestations appeared; and as stable disease (SD) if the change was defined between PR and PD. All patients received a CT scan within 30 days before treatment; on 30, 90, and 180 days after treatment; and every 3 months, thereafter. Toxicities were evaluated according to the National Cancer Institute's (NCI) common toxicity criteria. Severity of GVHD was graded according to the Glucksberg grade. 12,13
Detection of patients' immune function
Patient serum samples were collected before infusion and 1 week after the haplo-PBSCs treatment. The phenotypes of monocytes and concentrations of cytokines in the patient's serum before and after treatment were detected by flow cytometry and ELISA respectively. 11 Five cytokines were selected, including interferon (IFN)-γ, tumor necrosis factor (TNF)-α, transforming growth factor (TGF)-β, IL-4, and IL-12.
Statistical analysis
Data are presented as the means±standard deviations. Statistical analyses were performed using the student's or pair-matched t-tests for quantitative data. A p-value of <0.05 was considered statistically significant.
Results
Patients and donors
Between March 2005 and March 2008, 10 consecutive patients with metastatic RCC who had suitable donors underwent IL-2-activated haplo-PBSCs treatment. All 10 patient-donor pairs were haploidentical: six pairs exhibited a matching of three of the six HLA-A/-B/-DR loci, and four pairs exhibited a matching of four of the six HLA-A/-B/-DR loci. A statistically significant correlation between KIR ligand incompatibility in the GVH direction and therapeutic antitumor response was previously identified. 11 In this study, the KIR-epitope mismatch was further investigated. Five pairs had the KIR-epitope mismatched in the GVH direction, and five pairs had the KIR-epitope mismatched in the HVG direction.
The patients' ages ranged from 51 to 79 years (median 60). Although it was not an inclusion criterion, all patients had undergone nephrectomy as part of their previous therapy for the primary tumor. Further, all patients had radiographically documented progressive disease despite prior therapy. Seven patients had previously received cytokine-based therapy (IL-2, interferon (INF)-α, or both). Most patients had multiple sites of metastatic tumor (Table 1).
A/G: Age and gender of patients and donors.
GVH: The absence in recipients of donor HLA-C alleles recognized by killer immunoglobulin-like receptors (KIRs) was defined as KIR-epitope- mismatched in the GVH direction.
HVG: The absence in donors of recipient HLA-C alleles was defined as KIR-epitope-mismatched in the HVG direction.
PR, partial response; SD, stable disease; PD, progressive disease; HLA, human leukocyte antigen.
Transplantation and bioactivity characteristics of haplo-PBSCs
After 3 days of mobilization with the G-CSF, the haplo-PBSCs were collected from 10 healthy donors by apheresis. Whole leucophoresis products, which included CD34+ stem cells, lymphocytes, and other white blood cells, averaged 4.27×1010 cells (3.12×1010 to 7.05×1010). The number of CD34+ hematopoietic stem cells ranged from 6.01×108 to 1.52×109 cells. After coculture with 5000 IU/mL of rhIL-2 for 4 hours in serum-free medium, the sum of activated haplo-PBSCs averaged 3.56×1010 cells (2.3×1010 to 5.5×1010). The number of CD34+ stem cells ranged from 5.07×108 to 1.06×109 cells.
As shown in Figure 1, the phenotypic characteristics of activated haplo-PBSCs were statistically different from that of untreated PBSCs. In activated haplo-PBSCs, T-cells, especially CD4+ T-cells and natural killer (NK) cells decreased and increased, respectively. Both these changes were statistically significant compared to the untreated PBSCs. After coculture with a high dose of rhIL-2, the number of activated lymphocytes, which were characterized by the elevated expression of CD69 and CD25, rapidly increased. Moreover, the number of CD8+CD28- inhibitory T-cells increased slightly. However, the number of CD4+CD25+ regulatory T-cells and CD45RO+CD8+ memory T-cells remained unchanged after rhIL-2 treatment, and the distribution of other functional subsets also appeared unchanged (Fig. 1).
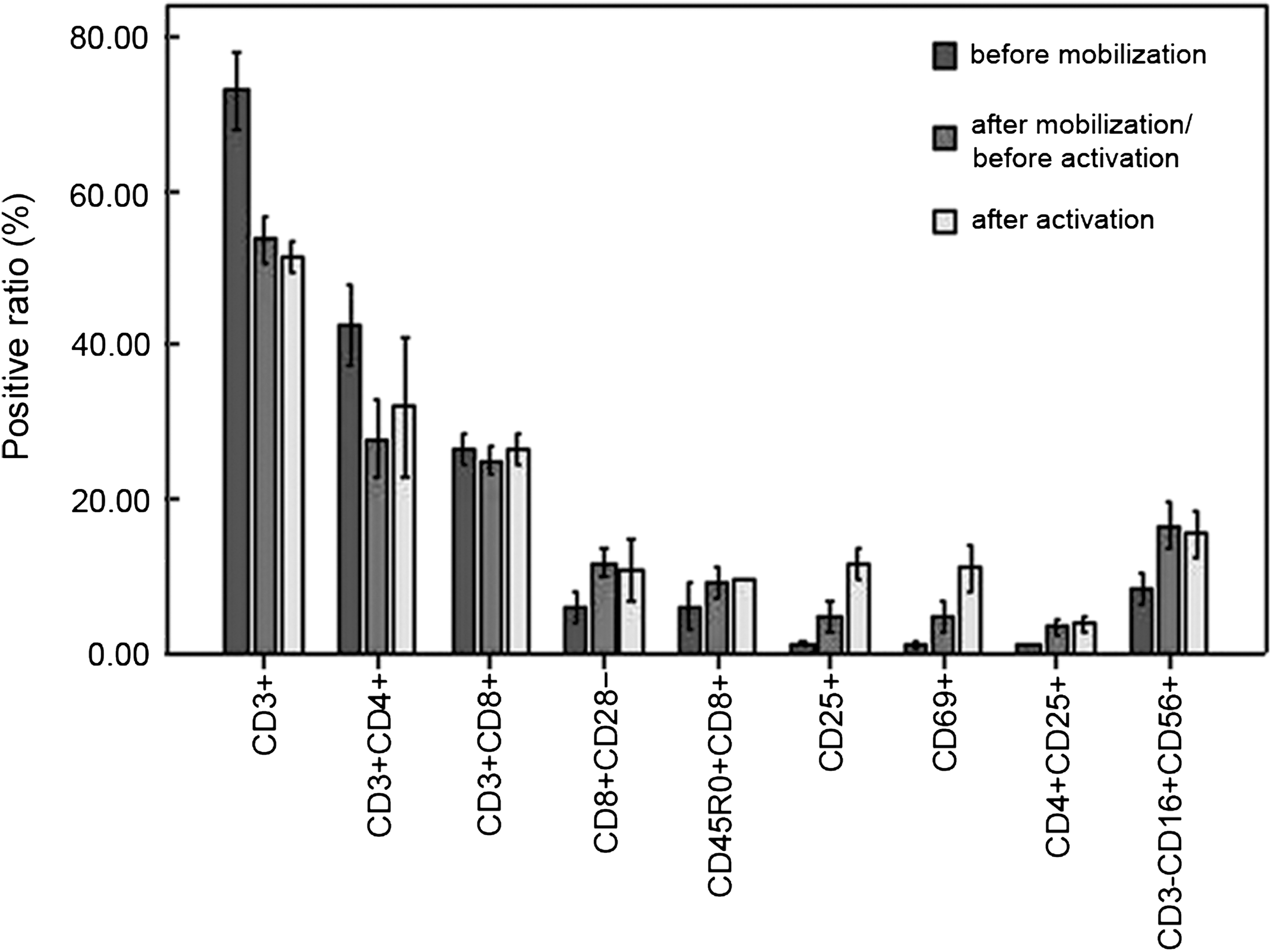
Diverse phenotypic characteristics of activated haplo-PBSCs collected from the 10 healthy donors by apheresis were compared with untreated peripheral blood stem cells (PBSCs). The proportion of T-cells, especially CD4+ T-cells, significantly decreased from 76.5% and 43.3% to 56.5% and 29.45%, respectively, with p-values both less than 0.01.The proportion of natural killer (NK) cells increased from 9.36% to 19.86% with a p-value of less than 0.05. Following activation, the proportion of CD69 and CD25 positive cells, known as activated lymphocytes, increased dramatically from 4.48% and 4.39% to 12.21% and 13.01%, respectively, with p-values both less than 0.05. The proportion of CD8+CD28- inhibitory T-cells increased slightly. In addition, the proportions of CD4+CD25+ regulatory T-cells and CD45RO+CD8+ memory T-cells were not statistically different, and the distribution of other functional subsets appeared unchanged.
Compared to untreated PBSCs, the nonspecific cytotoxicity of activated allo-PBSCs against GRC-1 cells was enhanced significantly at all E/T ratios, declining from 40:1 to 10:1 (Fig. 2). These results implied that short-term high dose of IL-2 activation might enhance the antitumor cytotoxicity of a donor's allogeneic PBSCs against RCC in vitro.
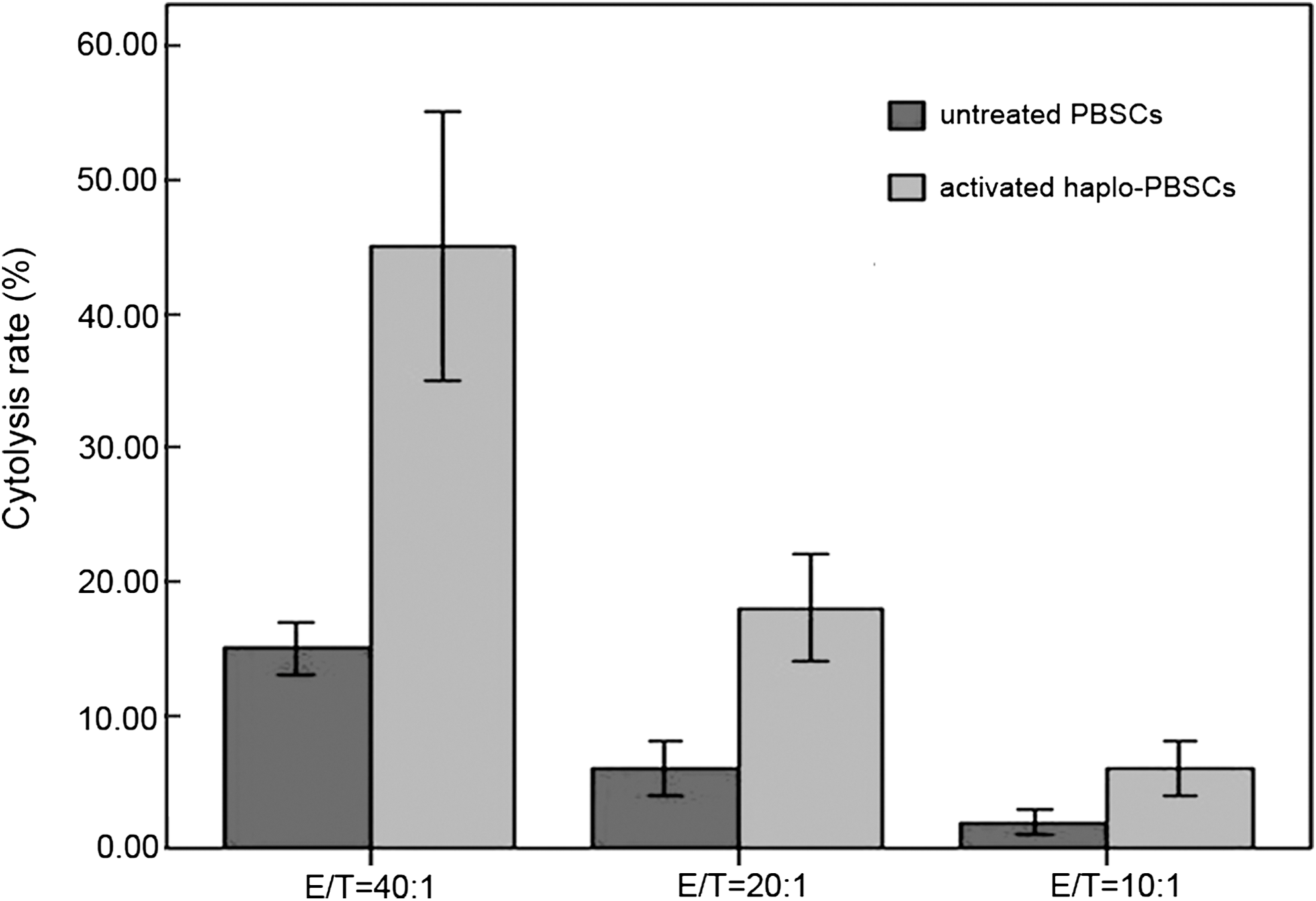
The LDH method was used to examine the cytotoxicity of activated haploperipheral blood stem cells (PBSCs) against renal cancer cells. Briefly, 1×105 cells/mL renal cancer cells were seeded in a U-bottom 96-well tissue culture plate in triplicate. Activated haplo-PBSCs or untreated PBSCs were seeded at various E/T ratios declining from 40:1 to 20:1 to 10:1. After 4 hours of incubation, 50 μL aliquots of the supernatants from each well were pipetted out to estimate the concentration of LDH released. Cytotoxicity was calculated using the formula shown in Methods. The antitumor cytotoxicity increased more than three times to 18.42% at 20:1 and reached as high as 45.21% at 40:1, both statistically significant increases (p<0.01).
Clinical efficacy
Eight patients achieved symptom relief, including ache, fatigue, dyspnea, and edema. Partial response was achieved in 2 patients, and 6 patients had a stable disease. As shown in Table 1, the total response rate, including CR, PR, and SD, was 80% (8/10). Two patients had progressive disease, one of which was fatal. Regression of metastases was observed at multiple sites, including the lymph nodes, adrenal glands, liver, bones, and lungs, as well as in abdominal, pelvic, and chest-wall tissues. The onset of tumor regression was typically delayed, occurring 2 months after the treatment. In 1 patient (patient no. 2, female), the lung metastases were found to be decreased in both size and number after a single treatment; this patient reached PR and remained in a progression-free state for 6 months, which was confirmed by a CT scan (Fig. 3A, B). In another patient (patient no. 5, male), the size of the metastases in both lobes of lung decreased significantly, with relief in the correlative symptoms, including breath holding and dyspnea; this patient reached PR and remained in a progression-free state for 6.5 months, which was determined by a CT scan (Fig. 4A, B).

Computed tomography (CT) scan images of a renal cancer patient (no.2, female) with lung metastases who reached partial response after one cycle of PBSCs treatment. The patient received activated haplo-PBSCs from her daughter, who was positive for a mismatching of KIR/human leukocyte antigen-C in the GVH direction. After treatment, the number and size of the lung metastases decreased significantly, together with relief in the correlative symptoms, including cough, blood sputum.

CT scan images of a renal cancer patient (no.5, male) with lung metastases who reached partial response after one cycle of PBSCs treatment. The patient received activated haplo-PBSCs from her daughter, who was positive for a mismatching of KIR/human leukocyte antigen-C in the GVH direction. After treatment, the size of the metastasis in both lobes of lung decreased significantly, together with relief in the correlative symptoms, including breath holding and dyspnea.
No serious adverse events such as fever, chill, and fatigue were observed during the activated haplo-PBSC treatment. Only 2 patients suffered slight side-effects, which were attributed to high-dose rhIL-2 exposure. For example, 1 patient showed nonspecific GVHD-like symptoms, including diarrhea, decreased appetite, and rashes. All symptoms were resolved promptly after symptomatic treatment within 2 days.
Progression-free and overall survival
As of June 25, 2008, 9 patients survived 186 to 751 days after the activated haplo-PBSCs treatment (median follow-up, 402 days). One patient died from progressive metastatic disease. Two patients who achieved partial response survived 9 and 19 months without disease progression after the treatment. For 10 patients, the median progression-free survivals (PFS) was 5.5 months (range 3–14), while the median PFS time of 8 patients who responded to the treatment (including CR, PR, SD) was 8 months (range 3–16) after one cycle of treatment.
Changes in recipient's immune function after treatment
After one cycle of activated haplo-PBSCs treatment, the CD3+, CD4+, CD4+/CD8+and CD3-CD16+56+ (NK) increased significantly (p<0.05), while the CD8+ and CD4+ CD25+ (regulatory T-cells, Tregs) decreased significantly (p<0.05) (Table 2). The concentrations of Th1-type cytokines (TNF-α and IFN-γ) increased (p<0.01) after the treatment, whereas the levels of Th2-type cytokines (TGF-β) decreased significantly (p<0.05). In addition, the concentrations of IL-4 were not statistically different with pretherapy (p=0.55) (Table 3).
Detected by flow cytometry.
p<0.05, versus pretreatment.
Analyzed by the ELISA method.
p<0.05, versus pretreatment.
p<0.01, versus pretreatment.
ELISA, enzyme-linked immunosorbent assay.
Factors affecting the responses to therapy
No multivariate analysis was performed due to the small size of our patient population, but summarized the characteristics of the patients that reached a partial response (PR) or remained alive. Common features included a pathology of renal clear cell carcinoma; less than two metastatic sites; and a high Karnofsky score (>80) when the activated haplo-PBSCs infusion was performed. The characteristics of patients with progressive disease (PD) included: multiple metastatic sites (>2); a low Karnofsky score (<70) before treatment; a short time from the diagnosis of primary tumor to metastasis (<1 year); and the presence of liver metastases.
Discussion
Given that renal-cell carcinoma appears to be susceptible to immunologic control, the efficacy of IL-2-activated HLA haploidentical PBSCs on metastatic RCC refractory to conventional management was evaluated. It was found that the adoptive transfusion of activated haplo-PBSCs, which were derived from HLA haploidentical healthy donors, had potent antitumor effects against the refractory cancer both in vitro and in vivo.
The donor cells that mediate the graft-versus-tumor effects and their target antigens were a central focus of investigation of the haplo-PBSCs treatment. The prolonged interval from transplantation to tumor regression was consistent with the time required for the activation and expansion of antitumor cytotoxic T-cells. Patients who had no response to conventional cytokine-based immunotherapies would respond well to transplantation therapies, which provided evidence that allogeneic immunotherapy might enhance the autologous antitumor immunity of patients. The mechanisms involved in the antitumor activity of IL-2-activated haplo-PBSCs are still unknown.
The haplo-PBSCs infusion without preconditioning could lead to rapid rejection by an undisturbed haploidentical immune system. Thus, proper activation processes were needed to ensure strong antitumor activity and an adequate number of adoptively transferred cells in the short term before haploidentical allogeneic rejection. As reported by Asai 14 and Slavin, 15 HLA haploidentical allogeneic NK cells purified from peripheral blood stem cells after 4 days of rhIL-2 stimulation, exhibited more potent therapeutic capabilities than traditional donor lymphocytes. Pretreatment with G-CSF effectively increased the sum of haplo-PBSCs, including hematopoietic progenitors, mature lymphocytes and dendritic cells, 16,17 which were thought to be the most important immune effectors. In this study, the haploidentical healthy donors were pretreated to obtain haplo-PBSCs that were almost 20–40 times greater than that without pretreatment. After activation by high doses of rhIL-2, the cytotoxicity of haplo-PBSCs against renal carcinoma increased significantly.
As determined by flow cytometry, the number of NK cells in activated PBSCs increased approximately two-fold, compared to the untreated cells. After 3 hours of coculture with a high dose of rhIL-2, the expression of CD69, a primary activation marker of NK and T-cells, increased quickly and prominently. These findings suggested that in addition to donor T-cells, whose strong allo activity contributes to graft versus tumor (GVT) and GVHD, donor NK cells might also be an important antitumor effector in activated haplo-PBSCs.
KIRs are members of the immunoglobulin superfamily that are expressed on the surface of NK cells 18 and can deliver an inhibitory signal through binding with HLA-C molecules, their natural ligands. 19 Studies of hematopoietic stem cell transplantation (HSCT) have demonstrated that the mismatching of KIR/HLA-C in the GVH direction generated a favorable alloreactive response against recipient cells, including hematopoietic stem cells, dendritic cells, and tumor cells. 20 In this study, a significant correlation between KIR ligand incompatibility in the GVH direction and therapeutic antitumor response was identified. The 5 patients who were positive for a KIR/HLA-C mismatch in the GVH direction experienced identifiable antitumor responses following treatment. However, only 3 of the 5 patients who had a mismatch in the HVG direction experienced antitumor responses. These results suggested that allo-NK cells have a dramatic correlation with the antitumor effects of activated haplo-PBSCs in vivo.
The powerful antitumor effects of IL-2-activated haplo-PBSCs were confirmed by their clinical efficacy. Additionally, no serious side-effects or GVHD occurred in the 10 patients. At present, however, it is impossible to compare the outcomes of patients treated with HSCT and conventional therapies, or treatments involving IL-2, IFN-α, or new inhibitors of the vascular endothelial growth factor (VEGF) receptor, or their combinations. Until now, the efficacy of immunotherapies was evaluated by the therapeutic evaluation criteria that were designed for chemotherapy and radiotherapy. This resulted in bias of the actual therapeutic effects of the immunotherapies, such as IL-2-activated HLA haploidentical PBSCs therapy. For this reason, now it is an emergency requested standard efficacy evaluation criterion for immunotherapy specially.
Besides the direct cytotoxicity for tumor cells, it seemed that the stimulation of a recipient's immune system by using activated haplo-PBSCs could generate long-term antitumor responses in vivo. Immunologic study demonstrates that the patient's cytoimmunity was correlated with tumorigenesis and progression. The T-cell subset is an important factor that constitutes a patient's immune defense, and the immune balance is maintained by the interaction of the CD4+ T helper (Th) cells and CD8+ suppressor T (Ts) cells. The lopsided change in the relationship of these two cytotypes, which is caused by the decrease of CD4+ Th cells or increase of CD8+ Ts cells, could result in defects in immune function. CD4+ CD25+ Tregs are another important factor regulating immune balance, and they have a significant role in the formation and maintenance of tumor immunosuppression. Tregs could promote tumor growth and progression by restraining T-cell proliferation and NK cell-mediated cytotoxicity reactions. 21 In this study, the number of CD4+ and CD4+/CD8+ cells increased significantly (p<0.05), while immunosuppressive cells, such as CD8+ and CD4+CD25+ (Tregs), decreased significantly (p<0.05). This phenomenon demonstrated that the activated haplo-PBSCs treatment could promote autoimmunity of the renal carcinoma patients.
In this study, a discrepancy in the direction of change in terms of the concentrations of two types of cytokines after treatment was also found. A significant increase and decrease was observed among Th1-type and Th2-type cytokines, respectively. This result suggests that immunotolerance, which is rooted in a tumor-induced bias toward Th2 dominance, could be reversed and overcome by high doses of rhIL2 activated haplo-PBSCs infusion. Additionally, this “Th1 bias” may be important in establishing a relatively advantageous microenvironment that sustains the antitumor activity of activated haplo-PBSCs in vivo. 22 –24
Previous retrospective studies identified better performance status, longer disease-free interval, and less than two metastatic sites as predictors of overall survival. 25 –28 This study confirmed this prediction, but also finds that the factors that predicted a response could not be used to select patients effectively. For this reason, prognostic factors have been identified for rapid progression under treatment, which can be used to select patients with little chance of response. Patients with more than two metastatic sites, liver involvement, and an interval from diagnosis of the primary tumor to the appearance of metastatic disease of less than 1 year had a higher probability of rapid progression and poor survival.
It is probable that metastatic RCC requires several therapeutic strategies to significantly improve long-term survival. It may be necessary to combine haplo-PBSCs with other therapies, such as irradiation against metastases, anti-VEGF antibodies, TKIs, IFN-γ, and IL-2, to prevent the risk of tumor escape mechanisms. 29 Combining the more direct tumor necrotizing and inflammatory effect of the latter with the slowly developing allogeneic antitumor effect of IL-2-activated haplo-PBSCs treatment might offer a new approach for renal cancer therapy.
In conclusion, this study indicates that IL-2-activated haplo-PBSCs are safe and have considerable antitumor properties. They offer a new approach for treating patients with metastatic or chemotherapy-resistant renal cancer. However, additional patients and further research are needed to determine the frequency and durability of the responses to this immunotherapeutic treatment.
Footnotes
Acknowledgments
This work was supported by grants from the National Key Technologies R & D Program of China during the 10th Five-Year Plan Period (No: 2005BA740C). This article has been reviewed by Dr. John E. Anderson, nephrologist, Johns Hopkins Medical Institution.
Disclosure Statement
The authors declare that they have no competing interests.