
Abstract
The introduction of the short-lived α-emitter 211At to intraperitoneal radioimmunotherapy has raised the issue of the tolerance dose of the peritoneum. The short range of the α-particles (70 μm) and the short half-life (7.21 h) of the nuclide yield a dose distribution in which the peritoneum is highly irradiated compared with other normal tissues. To address this issue, mice were injected with 211At-trastuzumab to irradiate the peritoneum to absorbed doses ranging between 0 and 50 Gy and followed for up to 34 weeks. The peritoneum-to-plasma clearance of a small tracer, 51Cr-ethylenediamine tetraacetic acid, was measured for evaluation of the small solute transport capacity of the peritoneal membrane. The macroscopic status of the peritoneum and the mesenteric windows was documented when the mice were sacrificed. Biopsies of the peritoneum were taken for morphology and immunohistochemical staining against plasminogen activator inhibitor-1 and calprotectin. Peritoneum-to-plasma clearance measurements indicated a dose-dependent decrease in peritoneal transport capacity in irradiated mice. However, macroscopic and microscopic evaluations of the peritoneal membrane showed no difference between irradiated mice versus controls. The results imply that the peritoneal membrane tolerates absorbed doses as high as 30–50 Gy from α-particle irradiation with limited response.
Introduction
The use of short-lived α-emitters, such as 211At and 213Bi, is currently being evaluated for internal radioimmunotherapy (RIT) by several research groups. 1 –7 The short range (<100 μm) and the high linear energy transfer of the emitted particles makes these radionuclides particularly suitable for targeted irradiation of small targets, for example, microscopic disease.
In systemic RIT the aim is to maximize the absorbed dose to the tumor and limit irradiation of normal tissues to tolerable levels. In many cases, the bone marrow is the most sensitive organ. Depending on the biodistribution and half-life of the radionuclide, however, other organs may be dose limiting. Important factors affecting the biodistribution are the properties of the carrier molecule, the stability of the conjugation to the carrier, and the properties of the free radionuclide. For short-lived radionuclides, the route of administration is also of great importance.
When administered intraperitoneally (i.p.), the short half-life, 7.21 hours and 45.6 minutes, respectively, for 211At and 213Bi, and the short range of the α-particles make it possible to deliver high absorbed doses to locally confined disease and to the surfaces of the peritoneal cavity with minimal irradiation of the rest of the body. In a clinical work from our group, 4211At labeled to the monoclonal antibody MX35 F(ab′)2 targeting ovarian cancer cells was infused i.p. The ratio between absorbed doses in peritoneum and bone marrow was >100. Considering a relative biological effect of the α-particles of about 5, 8,9 an absorbed dose of up to 0.4 Gy to the bone marrow would be acceptable. The corresponding peritoneum dose would be >40 Gy or >200 Bd (using RBE=5). 10
Very little is known of the radiosensitivity of the peritoneum. Previous experiences of irradiation of the abdomen are external beam therapy and internal radiotherapy with β-emitters, such as 90Y, 131I, 177Lu, 32P, and 198Au. 11 –19 In these settings the absorbed dose is limited by the kidneys or liver, or the intestinal crypt cells located at ≥1-mm depth in the intestine. With i.p. α-therapy, these cells and organs remain virtually unirradiated. 20
This led us to start this study with the aim of investigating the effects of α-irradiation of the peritoneum in a mouse model. Functional as well as morphological factors were considered. The peritoneum of mice was irradiated by injecting 211At-labeled monoclonal antibody trastuzumab i.p. The mice were followed for up to 34 weeks after the irradiation, at which time they were sacrificed and dissected, and biopsies were taken for morphological and immunohistochemical analyses. During the follow-up time, the peritoneum-to-plasma clearance (Cl P→Pl) of a small, inert tracer, 51Cr-ethylenediamine tetraacetic acid (51Cr-EDTA), was measured on a few occasions to evaluate the membrane function of the peritoneum. The transport of 51Cr-EDTA across the peritoneal membrane is representative of the small solute transport capacity of the membrane, or rather the peritoneal pore area available for small solute transport, a parameter which is sensitive to the status of the peritoneal membrane. 21 –24
Materials and Methods
Animals
Female BALB/C nu/nu mice (Charles River) were used in all experiments. The mice were delivered at 3–4 weeks of age and kept under standardized conditions, as stipulated by the Swedish Animal Welfare Agency at the Laboratory of Experimental Biomedicine, University of Gothenburg, Sweden. They were allowed at least 1 week of acclimatization to their environment before studies were initiated. All animals were monitored for their weight and appearance regularly. Animals showing signs of poor health were euthanized. The Ethics Committee for Animal Research at the University of Gothenburg approved of the experimental design.
Radionuclides and labeling
The α-emitter 211At (T ½=7.21 hours) labeled to the monoclonal antibody trastuzumab (Herceptin; Roche) was used to irradiate the peritoneum. 211At was produced from a bismuth target on aluminum backing through the 209Bi(α,2n)211At reaction at the PET and Cyclotron Unit, Rigshospitalet, Copenhagen, Denmark. The irradiated target was transported to Gothenburg, Sweden, for work up by a dry distillation technique described previously. 25
211At was labeled to an N-succinimidyl-3-(trimethylstannyl)benzoate conjugated monoclonal antibody trastuzumab (Herceptin; Roche) using a novel one-step method published by our group. 26 A high radiochemical yield, typically around 75%, and radiochemical purity (>95%), determined by methanol precipitation, were obtained. Trastuzumab binds specifically to the HER2/neu receptor overexpressed in certain types of malignant tissues. However, in this study only tumor-free mice were included and the antibody was used as an unspecific carrier for the radioactivity.
The tracers 51Cr-EDTA and 99mTc-diethylenetriamine pentaacetic acid (99mTc-DTPA) were used for Cl P→Pl measurements. 51Cr-EDTA (T ½=27.7 days; GE Healthcare) was commercially available. 99mTc-DTPA (T ½=6.01 hours) was prepared from a kit (Technescan DTPA; Mallinckrodt Medical) at the Department of Nuclear Medicine, Sahlgrenska University Hospital, Gothenburg, Sweden.
Radioactivity measurements
For measurements of injection solutions (>100 kBq) an ionization chamber (CRC-15 dose calibrator; Capintec) was used. Low-activity samples (<10 kBq) were measured in a NaI(Tl) γ-counter (Wizard 1480; Wallac). Samples containing both 99mTc and 51Cr were measured twice using dual-energy window settings—the second time after the decay of 99mTc, enabling spillover correction and accurate count determination.
Fluid sampling
Heparinized capillary tubes were used for all fluid sampling. The height of the fluid column was measured and converted to a volume via a conversion factor of 0.266 μL/mm. The blood sample volume was always <20 μL. Blood samples were centrifuged so that both the total sample volume and the plasma volume could be determined. The activity content was related to the amount of injected activity (IA) as determined by 3–5 standard samples from the injection solution.
Immunohistochemistry
To evaluate possible effects of radiation on the peritoneal surface after α-irradiation, markers for inflammation and the fibrinolytic system were used. Biopsies of peritoneum tissue fixed in Bouin's solution (Sigma Diagnostic) were, following an overnight fixation, washed in phosphate-buffered saline (PBS) at pH 7.4 and dehydrated in graded series of ethanol, cleared with xylene, and finally embedded in paraffin. Staining with hematoxylin and eosin (H&E) for morphologic assessment was performed.
Sections of 4–6-μm-thick were deparaffinized, and after rinsing in water and TRIS-HCI buffer (pH 7.4) a peroxidase blocking was performed, following immunostaining using primary antibodies toward mouse antigens. All antibodies were rabbit anti-mouse polyclonal IgG and were used together with the Dako EnVision system (Dako Cytomation), an immunohistochemical assay that has been previously described. 27 –31 The following concentrations were used: antibody against plasminogen activator inhibitor (PAI-1), diluted 1:10 (American Diagnostic) recognizing both free PAI-1 as well as Pa/PAI-1 complexes, and antibody against calprotectin, diluted 1:400–1:1000 (Novus Biologicals). All were detected with 3,3′-diaminobenzidine, according to the manufacturer's instructions (EnVision; DakoCytomation). As a negative control normal rabbit serum was used (DakoCytomation). As a positive control for calprotectin, human inflamed colon was used. 27
Slides were counterstained with hematoxylin prior to dehydration and mounting with cover slips. Evaluation with distribution and qualitative comparison was performed using a Nikon Eclipse E800 microscope together with Nikon Coolpix 995 digital photo equipment (Nikon Instruments, Inc.). All sections were compared and evaluated individually by 2 blinded observers.
Peritoneum-to-plasma clearance
The peritoneum-to-plasma clearance Cl P→Pl or transport capacity of the peritoneal membrane could be an indicator of the status of the peritoneum. Hence, Cl P→Pl of a small, inert tracer was measured in mice irradiated i.p. with the α-emitter 211At. With the use of a peritoneal catheter the clearance could be measured directly by microsampling of the peritoneal fluid after injection. The presence of a catheter may however influence the results, wherefore an indirect and minimally invasive method was developed for this study, comprising 2 simultaneous injections and 3 consecutive blood samples. The methodology was inspired by a method for glomerular filtration rate (GFR) measurements previously described. 32
A tracer, 51Cr-EDTA, was injected i.p. and the appearance in blood, rather than the disappearance from the i.p. fluid, was measured by blood sampling. The tracer was rapidly cleared from the blood by glomerular filtration, which needs to be corrected for in the calculation of Cl P→Pl. Therefore, a second tracer, 99mTc-DTPA, injected intravenous (i.v.) simultaneously with the first tracer, was used to evaluate this effect. The two tracers are of comparable size and charge and can be used interchangeably as explained below in experiment 1.
A two-compartment model (Fig. 1) was set up to describe the kinetics of a small tracer injected i.p. with a relatively large fluid volume (0.5–1.0 mL). The first compartment is the peritoneal cavity, the i.p. compartment, from which there are two transport routes to the extraperitoneal (e.p.) compartment, including plasma and all extracellular compartments accessible to a small tracer outside of the peritoneal cavity. The two routes between the i.p. and e.p. compartments represent diffusional flow across the peritoneum with rate constant k 1, and lymphatic drainage of the peritoneal cavity, a volumetric flow, L. Diffusion in the opposite direction, e.p. to i.p., depicted with a dotted arrow in Figure 1, was not considered in the application of the model. The lymphatic drainage leads to a volume decrease of the i.p. compartment over time. The volume of the e.p. compartment, however, is assumed to be constant over time, regulated by urinary excretion. Transport of tracer away from the e.p. compartment was assumed to go in one direction and via one type of transport only, that is, the glomerular filtration of the blood with rate constant k 2. See Appendix for a mathematical description of the compartment model.
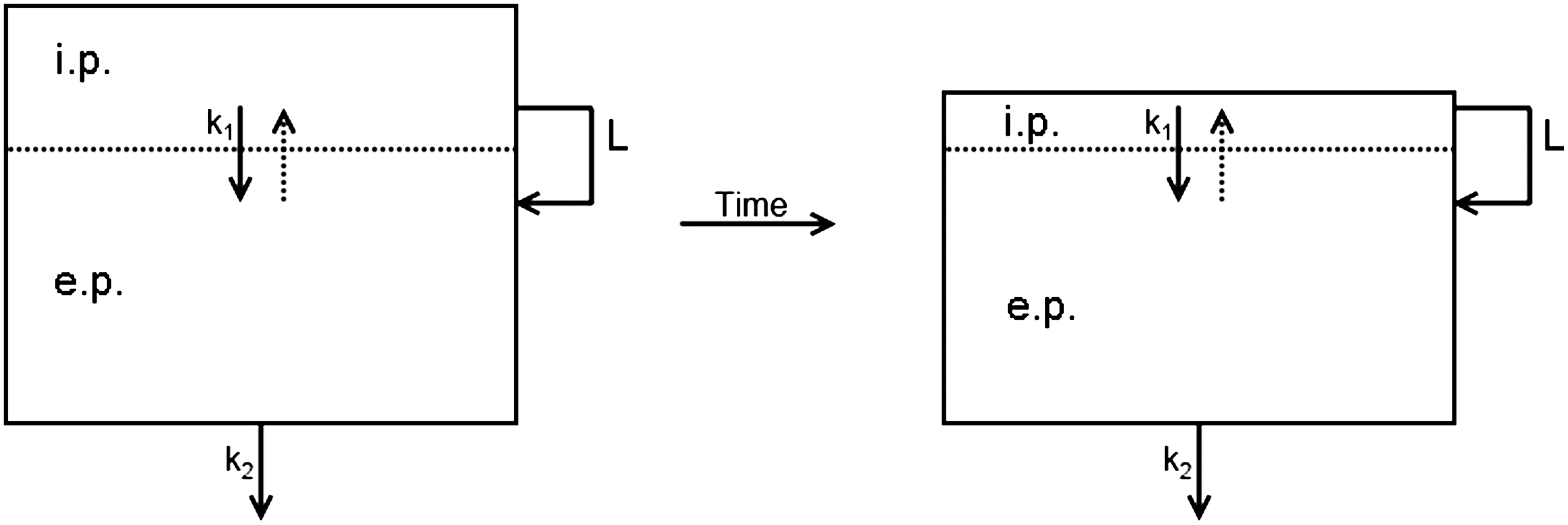
A two-compartment model for the transport of a small, inert tracer injected i.p. The dotted line represents the peritoneal membrane, separating the i.p. and e.p. compartments but allowing diffusional transport of tracer with rate constant k 1. The i.p. compartment volume decreases with time due to lymphatic drainage L. The e.p. compartment volume is constant, regulated by urinary excretion. The tracer is cleared from the e.p. compartment via renal filtration with rate constant k 2. e.p., extraperitoneal; i.p., intraperitoneal.
According to Zakaria and Rippe, 33 about half of the fluid loss of a saline solution injected i.p. in a rodent is due to lymphatic drainage of the peritoneal cavity. An experiment described in the dosimetry section below showed that the absorption rate of i.p. injected PBS was about 2.6 μL/min. The lymphatic flow L would then be 1.3 μL/min. This value was used in all Cl P→Pl calculations.
In a typical clearance measurement, blood samples were drawn at 10, 20, and 40 minutes after intravenous (i.v.) injection of 100 μL 99mTc-DTPA in PBS and i.p. injection of 800 μL 51Cr-EDTA in PBS. The 99mTc-DTPA plasma concentration was fitted to an arbitrary monoexponential function. The slope of the fitted curve corresponds to the GFR constant k
2. Division of the IA (100%) by the intercept with the y-axis gives the e.p. distribution volume V
ep. Since k
2 and V
ep for the two tracers are similar, the values derived for 99mTc-DTPA are valid also for 51Cr-EDTA. The 51Cr-EDTA plasma concentration was fitted to Equation 7 (see Appendix), which describes the plasma concentration of an i.p. injected tracer, using the obtained values for k
2 and V
ep as in data. The fitting process yielded a value for the peritoneum-to-plasma rate constant k
1 that finally was used to calculate the peritoneum-to-plasma clearance (Cl
P→Pl) using Equation 1.
Three kinetics experiments were made to verify the method and the compartment model. In all experiments, an i.v. injection (100 μL PBS) and an i.p. injection (800 μL PBS) were given. Tracers 99mTc-DTPA and 51Cr-EDTA were given with the i.v. injection or with the i.v. and i.p. injections, respectively. Blood samples were drawn from the tail vein after placing the mouse for a few minutes under a heating lamp to provoke vein dilation. i.p. fluid samples were taken after euthanasia.
In experiment 1, the two tracers were coinjected i.v. to 5 mice. The purpose of this experiment was to verify whether the GFR and e.p. distribution volumes V ep of the tracers were comparable. Blood samples were drawn at 10, 20, and 40 minutes after the injection and the plasma concentrations of the two tracers were compared. The experiment showed that the tracers had comparable kinetics. The concentration of both tracers decreased exponentially with time. Monoexponential curves were fitted to 99mTc-DTPA and 51Cr-EDTA data, respectively. Wilcoxon paired sign rank tests were performed on the intercepts and slopes of individually fitted curves, respectively. The tests indicated that there was no significant difference between the tracers kinetics at the 0.05 significance level. The experiment showed that 99mTc-DTPA can be used to estimate V ep and the GFR constant of 51Cr-EDTA in Cl P→Pl measurements.
In experiment 2, the difference in the plasma kinetics of i.v. versus i.p. injected tracer was studied. Five mice were administered 99mTc-DTPA i.v. and 51Cr-EDTA i.p. From 2 mice, 5 and 7 repeated blood samples were drawn from the tail vein during the first 10–12 minutes, respectively. From 3 mice, blood samples were drawn at 10, 20, 40, 60, 80, and 100 minutes. All data points from all five animals were plotted together in Figure 2A. The concentration of the tracer injected i.v., 99mTc-DTPA, decreased exponentially in plasma during the first hour after the injection, confirming the observation made in experiment 1. A monoexponential curve was fitted to the 99mTc-DTPA data (r 2=0.9256). The slope of the curve was −0.064 minutes−1 and the intercept was at 34% IA/mL, corresponding to a V ep of 2.9 mL. The fit was very good for the first 60 minutes. The data points at >60 minutes, however, deviated from the fitted curve. The plasma concentration of the i.p. injected tracer 51Cr-EDTA increased at first and then decreased slowly. A maximum of 6.5% IA/mL was reached at 20–30 minutes. Equation 7 (in Appendix) was fitted to the 51Cr-EDTA data, with input parameters acquired from the 99mTc-DTPA fit. The fitted curve followed the data nicely (r 2=0.9002). The rate constant for the transport of 51Cr-EDTA across the peritoneum was −0.015 minutes−1, corresponding to a Cl P→Pl of 53 μL/min, not corrected for the body mass of the mice.

Decay-corrected plasma
In experiment 3, another 20 mice were administered 99mTc-DTPA i.v. and 51Cr-EDTA i.p. This time the i.p. fluid concentrations were analyzed. Four mice were sacrificed and dissected at 5, 10, 20, 40, and 60 minutes, respectively. i.p. fluid samples were taken in triplicate upon opening the abdomen. The i.p. fluid concentrations are plotted in Figure 2B. 51Cr-EDTA decreased exponentially with rate constant of −0.022 minutes−1 (r 2=0.9740). The i.v. injected tracer 99mTc-DTPA appeared in the i.p. fluid with a flat peak at 5% IA/mL at 20–30 minutes, after which it slowly decreased. The rate constant for this transport was not calculated, but it is reasonable to assume it is similar to the rate constant for the flow of 51Cr-EDTA in the opposite direction. The e.p. to i.p. transport, the dotted arrow in Figure 1, is likely the reason for the deviation from the exponential concentration decrease observed for 99mTc-DTPA after 60 minutes in plasma. In the initial phase after the injection, the concentration is higher in plasma and the tracer is transported to the i.p. fluid. When the blood is cleared of the tracer, the net flow of tracer across the peritoneum switches direction and refills the blood with tracer. This effect was not taken into consideration in the compartment model because the renal filtration of the blood is an order of magnitude larger than the transperitoneal transport. Further, the gain in accuracy of the model was regarded small in relation to the increase in complexity brought on by including backflow across the peritoneal membrane and also the rise time for the i.p. injected tracer appearance in plasma is the important parameter to study in this case. Hence, the model fit at times >60 minutes is not crucial for the analysis.
Dosimetry
Absorbed doses to the peritoneum, the kidneys, and the bone marrow from 211At i.p. injections were estimated.
For the peritoneum dosimetry, the activity concentration cA (t) of the i.p. fluid was measured in a separate experiment. Ten mice were injected i.p. with trace amounts of 211At-trastuzumab in 700 μL of PBS. The mice were sacrificed and dissected at 60 minutes (n=5) and 200 minutes (n=5) after the injection. Samples of i.p. fluid and blood were taken in triplicate for radioactivity content measurement. The decay-corrected activity concentration in the i.p. fluid increased slightly with time. At 60 minutes the mean concentration in i.p. fluid was 113%±6% of the injected concentration (IC), and at 200 minutes it was 131%±11% IC. The plasma concentration was raised from 10.2%±4.5% IC at 60 minutes to 36.1%±8.1% IC at 200 minutes. The antibody leaves the peritoneal cavity mainly via the lymph flow, while the water is also transported across the peritoneal membrane. Hence, the observed concentration increase in both i.p. fluid and plasma was expected and in accordance with previously published data. 9,34
Another experiment was performed to estimate the rate at which an i.p. injection is absorbed by the body. The remaining i.p. fluid volume after injection of PBS was measured in 30 mice by a direct volume recovery method. 33,35,36 The animals were injected i.p. with 700 μL (n=10) or 800 μL (n=20) of PBS at the start of the study. After 5 (n=4), 10 (n=4), 20 (n=4), 40 (n=4), 60 (n=9), or 200 minutes (n=5) the animals were sacrificed and the abdomen was opened. The remaining i.p. fluid was collected with preweighed pieces of gauze and weighed. The experiment showed that of the injection solution, 93±38 μL was rapidly absorbed and after that the absorption rate was 2.6±0.4 μL/min. The experimental data and a linear regression with confidence interval bands are shown in Figure 3.
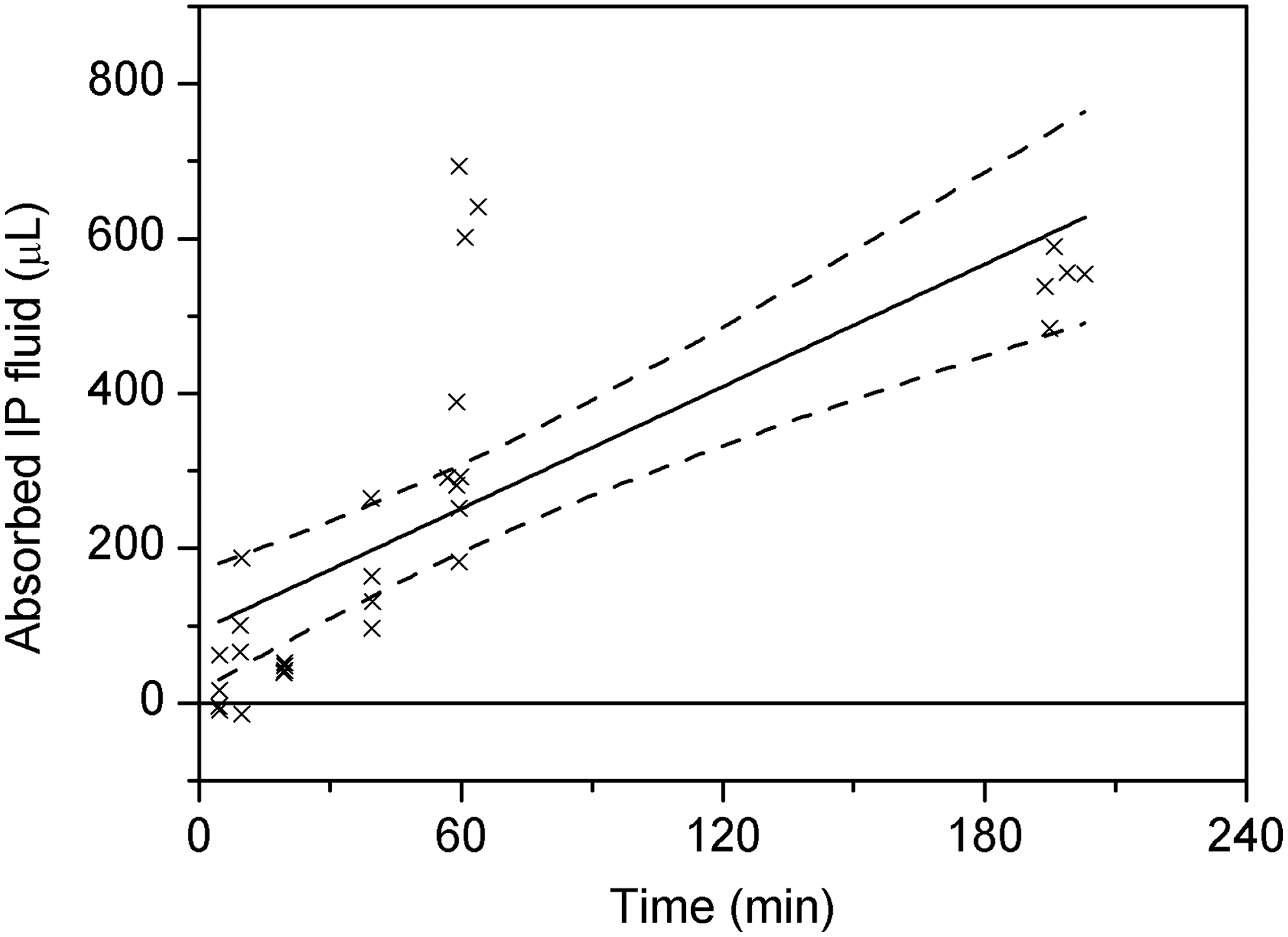
Absorbed i.p. fluid volume after i.p. injection of phosphate-buffered saline. Linear regression (fitted line with CI bands) indicates an i.p. fluid absorption rate of 2.6±0.4 μL/min.
When estimating the absorbed dose to the peritoneum, the peritoneum was approximated as a flat wall in direct contact with the i.p. fluid. With this geometry, the absorbed dose to the surface is half of the equilibrium dose to the i.p. fluid, as long as the fluid layer covering the surface is 70 μm (the maximum α-particle range) or thicker. The absorbed dose to the tissue layers under the surface rapidly decreases with depth, due to the short range of the α-particles. The equilibrium absorbed dose to the i.p. fluid was calculated using the general dose equation (Equation 2), in which the mean energy released per decay of 211At Δα is 1.09×10−12 J·(Bq·s)−1 and the half-life T
½ of 211At is 7.21 hours. The absorbed fraction φα is 1 in this case and the peritoneum absorbed dose is half of the equilibrium absorbed dose.
The integration time T depends on the i.p. injection volume. According to the results of the i.p. fluid volume change experiment, the mean time for a 700 μL injection and a 1000 μL injection to be absorbed is 230 and 345 minutes, respectively. Considering though the fact that a very thin fluid film is sufficient to achieve absorbed dose equilibrium, a “worst case scenario,” assuming the lower limits of the estimated initial absorption and absorption rate, that is, the upper limit of the clearance time, was used for the estimation of the peritoneum dose, resulting in integration times of 293 and 430 minutes for the two aforementioned injection volumes, respectively.
Absorbed doses from 211At to kidneys and bone marrow were calculated for comparison with previous studies. Biodistribution data for i.p. injected 211At-trastuzumab published by Palm et al. 34 were used for the activity concentration parameter. For the kidneys, Equation 2 was used with absorbed fraction φα=1. The bone marrow dosimetry was performed as described by Elgqvist et al. 9 The method takes into consideration the bone-marrow-to-blood uptake ratio, as well as the bone-to-blood uptake ratio. The integral was solved by numeric integration of a linear interpolation of the activity concentration up to 19 hours.
The absorbed dose from the trace amounts of 51Cr and 99mTc used in clearance measurements was estimated insignificant compared with the absorbed dose from the 211At injection, and was not calculated.
Effects of α-irradiation of the peritoneum
Healthy mice were given repeated injections of 211At-labeled trastuzumab (Herceptin; Roche) in PBS i.p. to irradiate the peritoneal membrane. The administered activity was 2×700 kBq (n=6), 4×350 kBq (n=12), 4×700 kBq (n=12), and 4×1000 kBq (n=12). The antibody concentration was 3 μg/mL. The injection volumes were 700 μL for the 2×700 kBq group and 1000 μL for the other groups. The injections were given at 2-week intervals (3 weeks for the 2×700 kBq group), because reversible myelotoxicity was expected, from which the mice were allowed time to recover. 9 A total of 26 control animals were used, of which 4 received 2 i.p. injections with PBS, 12 received 4 i.p. injections of PBS, and 10 were untouched.
The peritoneum-to-plasma clearance of a small tracer, 51Cr-EDTA, was measured for evaluation of the small solute transport capacity of the peritoneal membrane, the details of which are described in a separate section. Clearance measurements were made at weeks 24 and 30 after the first 211At injection for the groups receiving 4 injections. The 2×700 kBq group was evaluated for Cl P→Pl before and after the second injection of 211At and again at weeks 14 and 28.
The mice were followed up to 34 weeks. Mice showing signs of poor health were euthanized earlier. All animals were dissected prior to euthanasia according to a fixed protocol. First, the mouse was anesthetized with isoflurane (Isofluran Baxter; Baxter Medical AB) and the abdominal skin was opened and separated from the abdominal wall. The abdominal wall, including the ventral part of the peritoneum, was cut out in one piece and photographed separately, after which part of it was fixated in Bouin's solution (Sigma Diagnostic) for immunohistochemical staining and morphology with H&E staining. The mesenteric windows, connecting the intestines to the mesentery, were carefully lifted while still attached to the body, and photographed. The animal was then euthanized by heart puncture.
Results
The absorbed doses to the peritoneum delivered were ∼0, 17, 35, or 50 Gy for the animals receiving 4 injections of 211At-labeled antibody and about 0 or 18 Gy (9 Gy/inj) for the animals receiving 2 injections. The estimated absorbed dose per IA was not the same between these groups because the injection volumes differed. The irradiation resulted in a general toxicity, manifesting itself as a weight difference between the groups and on the survival of the animals. Unfortunately, only one of the animals in the highest dose group was still alive for the first clearance measurement. The median survival for this group was 159 days (22.7 weeks) after the first injection of astatine-labeled antibody. The animals in the other groups survived until the end of the study with a few exceptions.
Macroscopic findings
All animals were dissected when sacrificed. The anterior abdominal wall was cut out in one piece and photographed. Also, the mesenteric windows were photographed while still attached to the body. Examples of these photographs are shown in Figure 4. The surfaces of the peritoneal cavity were clear and moist in all animals. No adhesions were found. The vasculature of the abdominal wall and the mesenteric windows was similar between the groups. In all, no macroscopic differences could be found between irradiated and unirradiated mice.
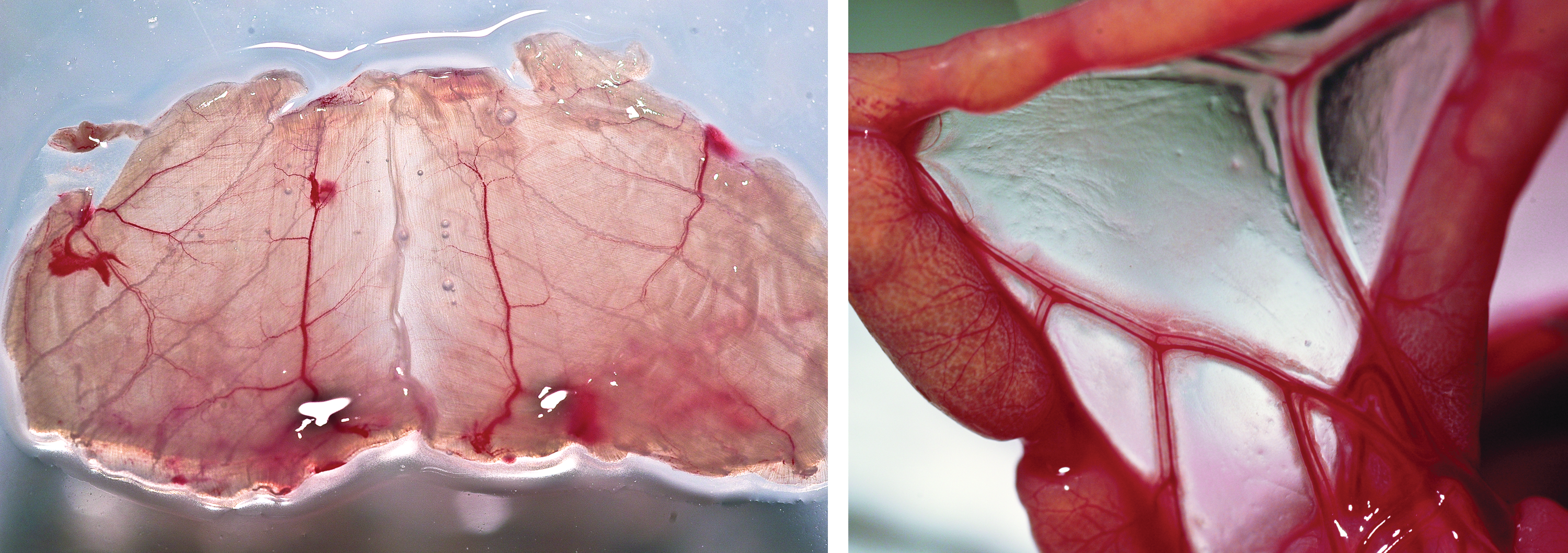
Photographs taken at the dissection. Left: the anterior abdominal wall. Right: mesenteric windows. Color images available online at
Microscopic findings
In H&E-stained sections of the abdominal wall, no detectable differences in morphology could be seen between the different doses of i.p. injected 211At-mAb and unexposed controls. The immunostaining for PAI-1 (Fig. 5) revealed no differences in detection between the groups. Similarly, immunostaining for calprotectin (Fig. 6) indicated no difference between the highest level of irradiation and the untreated controls. Both calprotectin- and PAI-1-immunostained biopsies showed similar patterns. Minor positive detection was found in areas close to or connected to vascular tissue and blood cells; however, there was no difference between the groups.
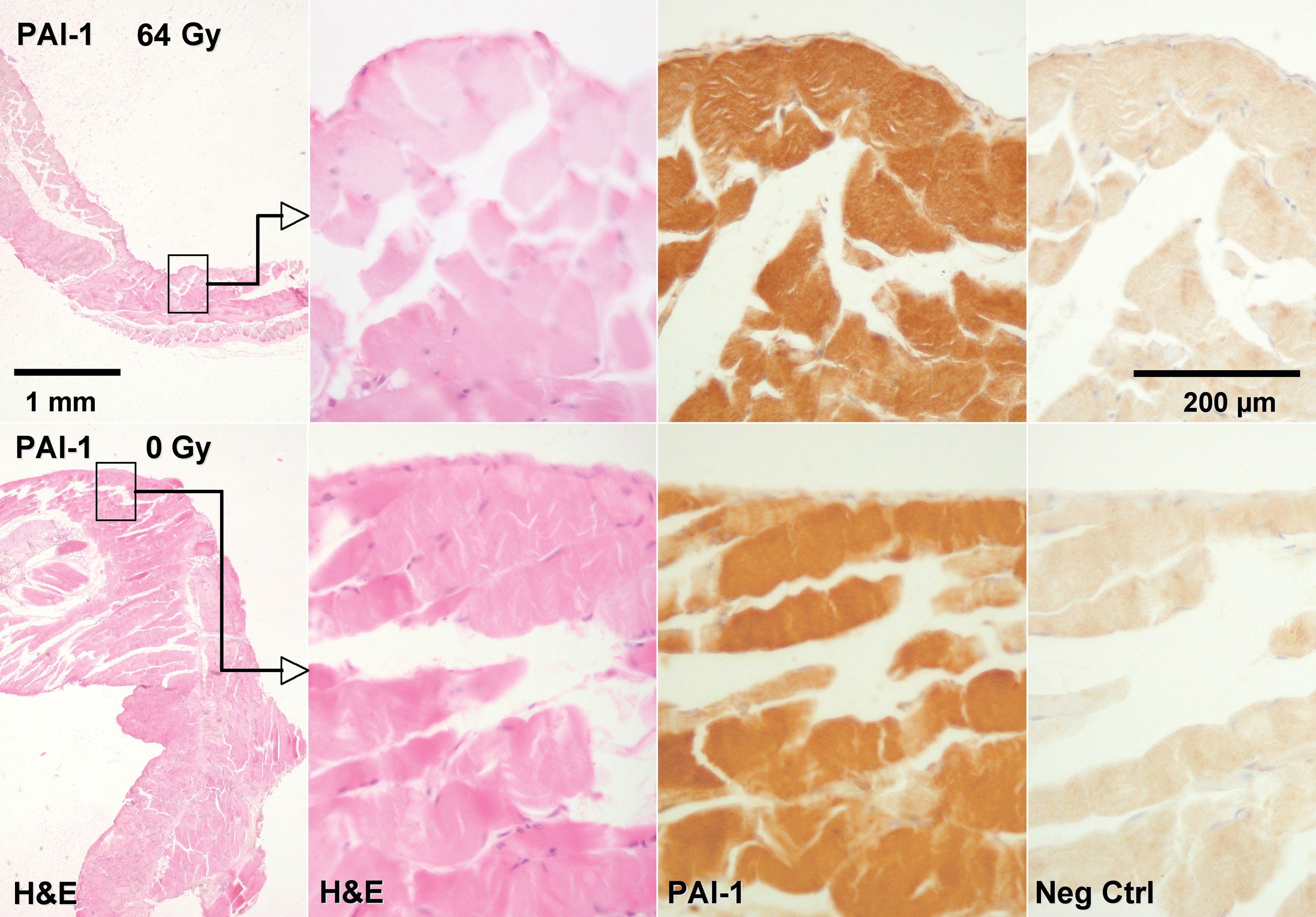
Immunostaining for PAI-1 in peritoneal biopsies. No differences were seen between the different absorbed dose levels. PAI-1, plasminogen activator inhibitor. Color images available online at
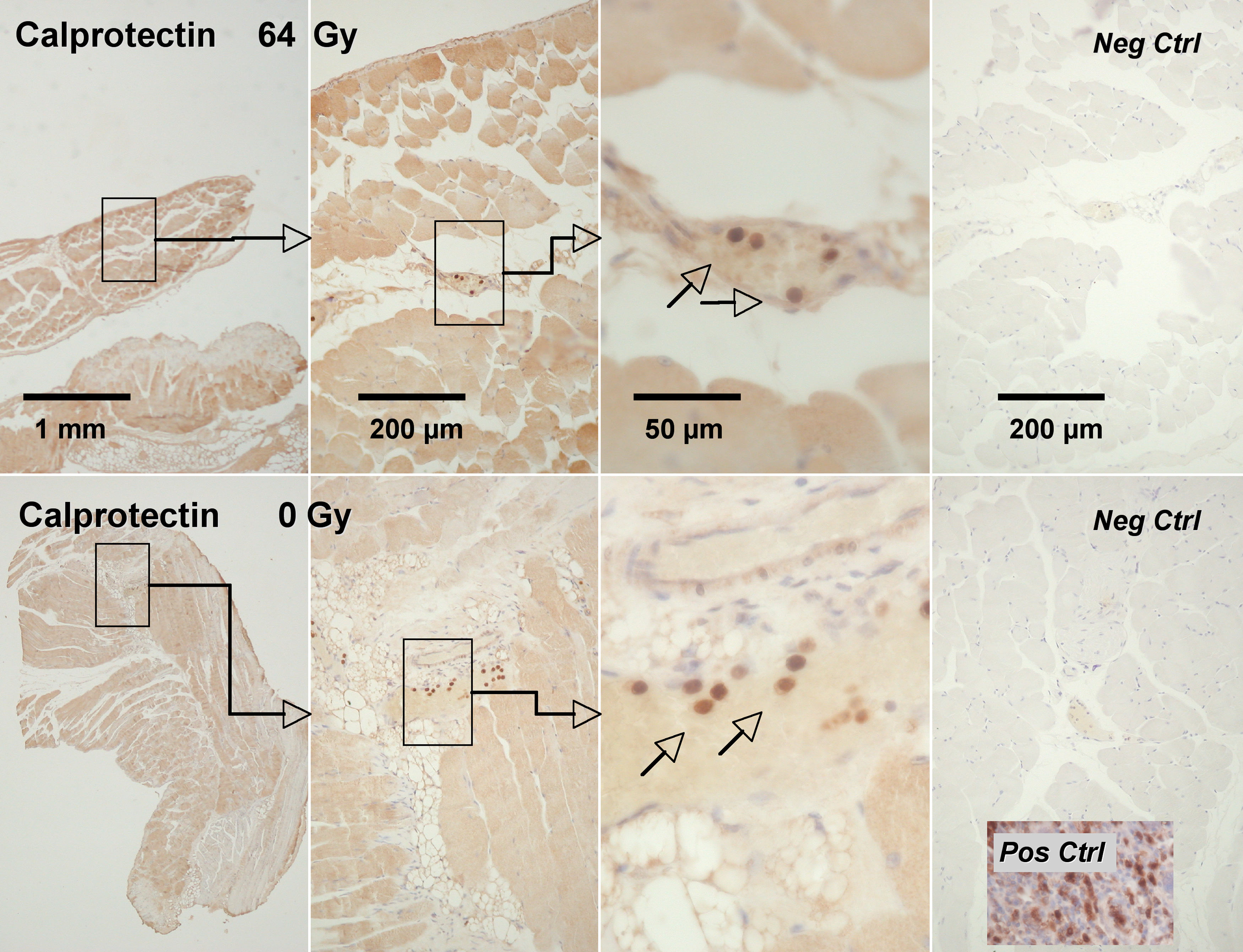
Immunostaining against calprotectin in peritoneal biopsies. No differences were seen between the different absorbed dose levels. Positive detection was found in areas close to or connected to vascular tissue (arrows) in both irradiated and unirradiated biopsies. Immunostaining for PAI-1 showed a similar pattern. Color images available online at
Functional findings
The peritoneum-to-plasma clearance, the Cl P→Pl, of a small, inert tracer was measured in animals irradiated to different absorbed dose levels. The small solute transport across the peritoneal membrane is a complex function of serveral factors, such as the peritoneal surface area and the diffusion distance between the peritoneal cavity and the blood vessels. The peritoneal surface area is strongly correlated to the weight of the animal. Because there was a significant weight difference between the groups, the clearance data were normalized to the body mass. In Figure 7, all successful Cl P→Pl measurements were plotted against the peritoneum absorbed dose. Measurements with 99mTc-DTPA plasma concentration data fitting with r 2<0.9 (24 measurements) were discarded, because the uncertainty of the measurement was considered to be too great. No such restrictions were used on the 51Cr-EDTA fitting. The variability of the data was high but the results indicate that a dose-dependent decrease in the transport capacity of irradiated mice compared with unirradiated controls cannot be ruled out. A trend line (y=1.61–0.014X, r 2 =0.08) with 95% CI was added to the plot. Expressed differently, an absorbed dose to the peritoneum of 25 Gy would cause a decrease in the peritoneum-to-plasma clearance of ∼20%.
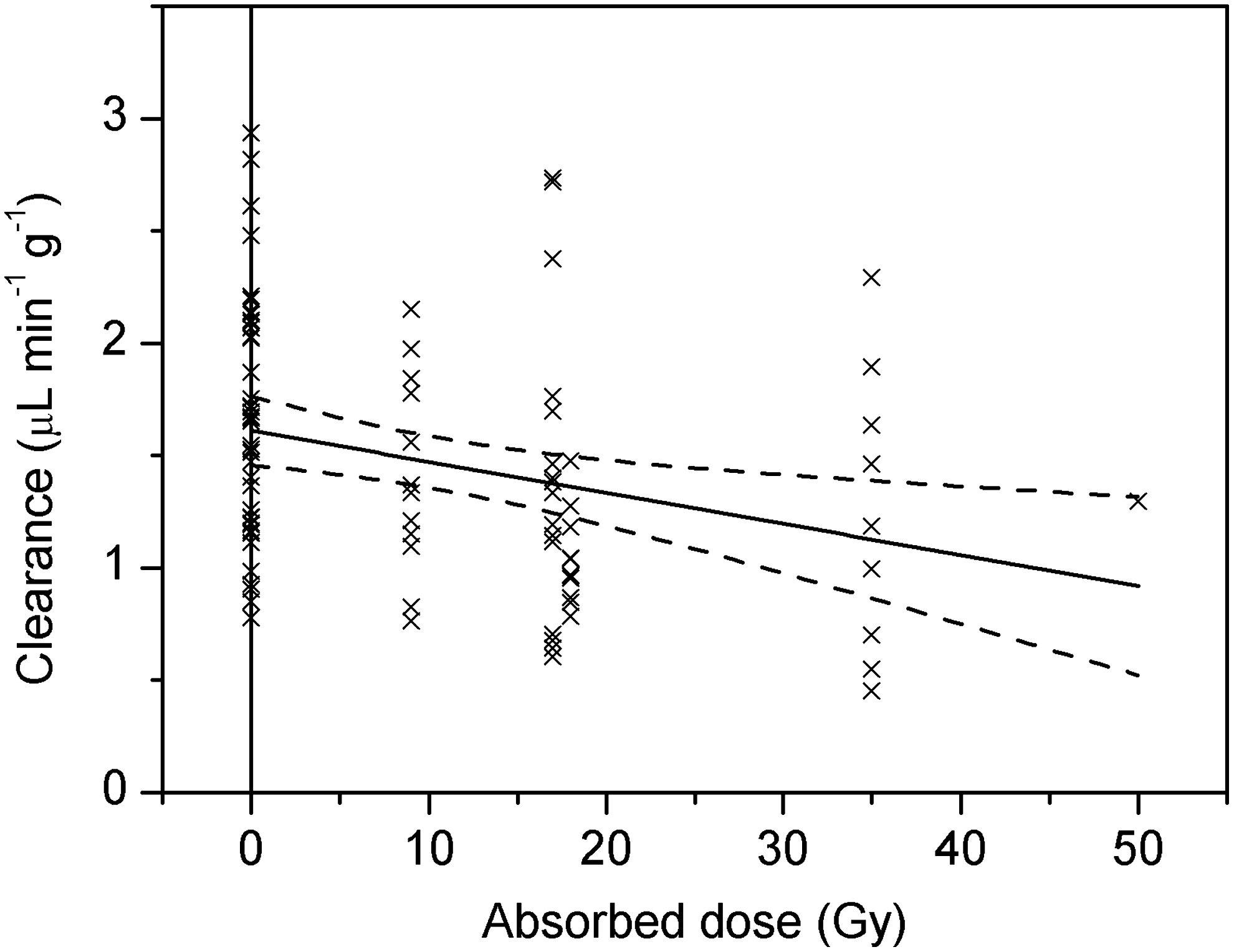
Peritoneum-to-plasma clearance normalized to body mass in mice irradiated to different absorbed dose levels.
The method for measuring the Cl P→Pl used in this study is based on a technique for GFR evaluation. Measuring the GFR at the same time as the Cl P→Pl was necessary in order to evaluate the Cl P→Pl with some accuracy, because the GFR can vary between individual mice, both over time and as a consequence of the administered radioactivity. The absorbed dose to the kidney was estimated to be 1.7 Gy/MBq. Absorbed doses to the kidney of mice evaluated for GFR and Cl P→Pl ranged between 0 and 4.8 Gy in the present study. For this dose range and the time interval studied, no significant change in the GFR was observed. For comparison, in a study by Back et al., 32 an absorbed dose of 14±4 Gy resulted in a 50% reduction of the GFR at 8–30 weeks after administration of the radioactivity.
Discussion
i.p. RIT is associated with risks, such as hematologic toxicity and bowel obstruction. The choice of radionuclide, amount of activity, and, if any, carrier molecule are of great importance for the outcome. Peters et al., 37 investigating 32 P as an ovarian cancer consolidation therapy, reported a radiation dose-dependent occurrence of bowel injury. In older studies using 198Au-colloids, there are reports of complications, such as nausea, abdominal pain, fever, intestinal obstructions, and even death. 38 The abundance of complications was believed to be caused by the γ-radiation associated with the 198Au decay, which erroneously was disregarded in absorbed dose estimations. No reports have been found regarding problems associated with the peritoneal surface itself that is bathed in the radioactive solution for the duration of the treatment.
Using α-emitting radionuclides in i.p. RIT, the dose distribution is radically different from previous clinical experience of radiation therapy. The α-particles reach only the superficial layers of cells lining the cavity in which the radioactive solution is infused. In our phase I study on the pharmacokinetics of astatinated monoclonal antibody injected i.p. in women with ovarian cancer, 4 it was evident that the peritoneal membrane could be exposed to high absorbed doses. However, the consequences and risks are unknown, since localized peritoneal exposure to α-particles has not previously been tried. For the absorbed dose levels used in the aforementioned clinical study (up to 1.6 Gy) no subjective abdominal discomfort related to the irradiation was noted.
The choice of an α-emitter for targeted radiotherapy is particularly suitable for minimal residual disease due to the short range of the α-particles that conforms well with the dimensions of small cell clusters. Hence, the patient category suitable for i.p. α-RIT has typically undergone primary cytoreductive surgery and chemotherapy. Some of these patients may be tumor free and have a healthy peritoneal lining in the whole or part of the peritoneal cavity. To study the effects of the α-irradiation on the normal peritoneum, this study was made on healthy tumor-free mice.
An important function of the peritoneal lining is to provide optimal conditions for intestinal movements. Surgery and irradiation may trigger a fibroblast response leading to adhesion formation and subsequent intestinal obstruction. 39 The peritoneal membrane can be used as a dialysis membrane in patients with renal insufficiency. Whether exchange with vascular and abdominal compartments has a major role in normal physiology is not clear. Peritoneal dialysis may eventually give rise to inflammation and fibrosis, which can be demonstrated by an altered transperitoneal transport of 51Cr-EDTA. 21,23 With this background, we considered it reasonable to investigate whether the exchange function of the peritoneal lining was affected by the localized absorbed dose from α-irradiation. In addition, we wanted to investigate whether irradiation would induce any morphological changes or increased expression of biomarkers related to fibrosis in the peritoneal tissue.
It has previously been described that calprotectin could be used as a marker for active inflammatory disease in human biopsies. 40,41 In 2009, Angenete et al. 27 described the presence of the protein complex in inflamed intestinal tissue as a response to radiation treatment in patients undergoing radiotherapy. However, a similar response in treated animals could not be seen in the present study. It is possible that the inflammatory response is not present or detectable with this method. Since the α-particle irradiation only affects cells far from the microcirculation, cytokines might not be able to recruit inflammatory cells. It is also possible that the inflammatory response differs between α- and γ-irradiations. PAI-1 is known for its importance in peritoneal healing, 42,43 and the absence of a difference in PAI-1 immunostaining is promising. All the clinical and immunohistochemical results point to a limited response of peritoneal tissue to 211At irradiation, which must be considered promising.
The peritoneum-to-plasma clearance (Cl P→Pl) of a small tracer, studied as a measure of the peritoneal membrane small solute transport capacity, is a complex function of the blood flow in the capillaries of the peritoneum, the surface area exposed to the i.p. fluid, the distance from the surface to the capillary, and the concentration gradient between the blood and the i.p. fluid. 22 α-Particle irradiation of the peritoneum could affect the Cl P→Pl in either direction. An increase could be explained by increased vascularization of the peritoneum. Access to more capillaries would result in a faster transport rate. Fibrosis of the peritoneum, on the other hand, could lead to thickening of the submesothelial tissue, which would decrease the Cl P→Pl. Both vascularization and fibrosis could follow radiation-induced inflammation of the peritoneum.
The important parameter for solute transport capacity in the three-pore model 22,44 is the “area parameter,” or the unrestricted pore area over diffusion distance (A 0/Δx). This parameter is independent of the peritoneal surface area and can only be determined using functional measurements. Transperitoneal transport of 51Cr-EDTA has been studied in mice 24 and rats. 21 In both these studies, 51Cr-EDTA was administered i.v. and the blood-to-peritoneal passage was studied. 51Cr-EDTA behaved according to the established three-pore model and the concentration of the tracer increased gradually in the dialysate. It is thus a good candidate for evaluation of the overall small solute transport capacity of the peritoneal membrane. In the present study, we have measured the peritoneum-to-blood clearance of 51Cr-EDTA. One might ask if there is a relationship between the uptake rate k 1 and the A 0/Δx. As far as we know, this has not been studied in mice, but there is a relevant study in patients with peritoneal dialysis, where iohexol was added to the dialysate prior to instillation and the serum concentrations were determined up to 120 minutes into the dwell. 45 Iohexol is a contrast agent, but it is also used for GFR determination as 51Cr-EDTA is. The two substances have similar properties and are both freely filtered in kidneys and neither reabsorbed nor secreted. The study showed that the rate constant k 1 for iohexol was closely related to A 0/Δx with a correlation coefficient of 0.9.
In the present analysis, the clearance data were normalized to the body mass of the individual mice. The normalization made the relative difference between irradiated animals and controls less pronounced when compared with the raw clearance data. This was because the irradiated mice were leaner than the controls. Normalizing the clearance data with the body surface area would perhaps be more physiologically correct. 46 Such normalization would have a smaller effect on the slope of the trend line than using the body mass, and the result of the analysis would not change.
The clearance measurements indicated that the transperitoneal small solute transport in irradiated mice is slower than in normal controls, which could be an indication of fibrosis. The importance of this finding is very difficult to evaluate, especially since no macroscopic nor microscopic differences could be found between the groups. The consequences of a reduced transperitoneal transport capacity for an otherwise healthy individual are unclear. The effect observed is therefore considered tolerable at 35 Gy. Unfortunately we have no clearance data at higher dose levels since the animals receiving 50 Gy did not survive until the clearance measurements. The tolerance dose for the peritoneum may therefore be as high as 50 Gy or even higher. The cause of death for these animals was more likely related to thyroidal issues and/or myeoltoxicity—an important issue for further study.
The uncertainties in the peritoneum absorbed dose calculations are indeed great. First of all, the assumed geometry is a rough model of the true irradiation geometry that is highly complex. Further, the concentration of the i.p. fluid after 200 minutes is not known, nor is the time it takes for the 211At-labeled antibody to clear from the peritoneal cavity. It may be longer than the time it takes for the i.p. fluid to be absorbed. The assumptions made have a great impact on the calculations. The reported absorbed doses to the peritoneum are therefore to be interpreted as mere estimates.
Here, the effect of α-particle irradiation of the peritoneum was studied in a nude mouse model. The translation of the results to humans is complex, since the model system is far from ideal. For humans infused with an osmotic solution containing the radioimmunocomplex, the peritoneal retention is high, resulting in a peritoneum-to-bone-marrow absorbed dose ratio of >100. In the mouse, an i.p. injection is absorbed by the body over ∼4 hours and the corresponding ratio is ∼9. This makes it problematic to selectively irradiate the peritoneum in mice without causing toxicity to other organs. In spite of this problem, the absorbed peritoneum doses achieved in this study are up to a factor 25 higher than the highest doses delivered to the patients included in the recent phase I study from our group, 4 and there are no current plans to increase the activity administered to a corresponding level.
The tolerance for α-irradiation of different organs is currently a relatively unexplored field of study. The bone marrow tolerance dose has been assessed to 0.4–1 Gy using 211At, 9,47 4–7.6 Gy using 213Bi, 48 and 2.1–3.5 Gy using 227Th. 7 Back et al. report a tolerance dose of 10 Gy from 211At to the kidneys. 32 The risk of inducing secondary disease, such as mesothelioma, in the case of i.p. α-RIT must also be assessed in a clinical situation. In the present study the peritoneal membrane seems to recuperate from absorbed doses up to 50 Gy. The maximum tolerable dose was probably not achieved and may not be possible to achieve in the mouse model due to the fast abdominal-to-blood transport of the radiolabeled antibody, leading to a high whole-body irradiation and general toxicity. The results must be considered promising for the future of i.p. RIT with α-emitters.
Conclusion
Peritoneum-to-plasma clearance measurements indicated a dose-dependent decrease in peritoneal transport capacity in irradiated mice. The mechanisms leading to or the consequences of a lowered Cl P→Pl are, however, unclear, and no macroscopic or microscopic differences could be found in peritoneal biopsies from irradiated and unirradiated animals for the studied absorbed dose levels and time interval. Further, a lack of inflammation was indicated by low and homogeneous PAI-1 and calprotectin staining in the same biopsies.
From this study, we conclude that the risk for irradiation-related peritoneal complications after i.p. α-irradiation is limited. The intended absorbed dose levels for patient therapies, up to 5 Gy, are considerably lower than the levels studied here. The results are promising for the continued use of α-emitters in i.p. RIT.
Footnotes
Acknowledgments
Helena Kahu is gratefully acknowledged for tending to the mice and for experimental assistance, Sofia Frost for helping out with 211At distillations, and Jörgen Elgqvist for scientific discussions.
This work was supported by research grants from the King Gustav V Jubilee Clinic Cancer Research Foundation, The Swedish Cancer Society, The Swedish Research Council, The Swedish Radiation Safety Authority, and The Assar Gabrielsson Foundation.
Disclosure Statement
No financial conflicts of interest exist.