
Abstract
Purpose:
Peptide receptor radionuclide therapy (PRRT) with 177Lu-DOTATATE is an efficient new treatment option in patients with neuroendocrine tumors (NETs), with low risk of toxicity. Since the kidneys are critical organs in PRRT, renal function is known to deteriorate after PRRT. We analyzed the decline in glomerular filtration rate (GFR), increase in serum creatinine (SCr), and changes in hemogram parameters between pretherapy and at least 6 months after last cycle post-therapy with 177Lu-DOTATATE.
Methods:
Forty-seven patients with NETs received 2–6 cycles of 177Lu-DOTATATE, leading to a total renal radiation absorbed dose of 12.5±4.1 Gy. All renal dose estimates were calculated with the help of OLINDA/EXM software. All patients were infused with renal protective amino acids during the administration of the radiopharmaceuticals. In this study, we used GFR that was estimated by in vitro method using 99mTc-DTPA and SCr to assess renal toxicity.
Results:
The patients were administered a mean cumulative activity of 20.1±6.74 GBq of 177Lu-DOTATATE. There was a significant decrease in GFR from 86.8±15.4 mL/1.73 m2/min to 66.1±14.5 mL/1.73 m2/min and rise in SCr from 0.86±0.19 mg/dL to 1.0±0.2 mg/dL with treatment. Patients with WHO grade 1 renal toxicity (group 2) at baseline demonstrated an increase in SCr that was significantly higher compared with patients with normal baseline creatinine levels (group 1). No serious acute or remote adverse events were recorded. Self-limiting serious hematological toxicity was observed in 2 patients.
Conclusions:
The decline in renal function as measured by in vitro GFR tends to be of greater magnitude in patients with baseline impaired renal function than in patients with preserved renal function after PRRT. Hematologic toxicity is relatively rare and can be managed conservatively when encountered.
Introduction
Somatostatin (sst) receptors are typically overexpressed in many tumors of various origins, such as neuroendocrine tumors (NETs) of intestine, pancreas, lung, and thyroid. This has led to intensive research in the field of sst targeting in oncology for both diagnostic and therapeutic indications. 1 Currently, five subtypes (sst1–sst5) have been identified and cloned. 2,3 NETs predominantly express sst2 receptors. The presence of sst2 receptors has opened novel peptide receptor radionuclide therapy (PRRT). Primary tumors are generally subjected to surgery; however, metastatic lesions and unresectable primary disease may be treated with PRRT using radiolabeled sst analog 177Lu-DOTATATE. The theoretical basis of PRRT is the delivery of maximum radioactivity within the tumor cell, owing to the internalization of the receptor and radiolabeled sst analog complex. 4
PRRT aims to deliver therapeutic doses to a tumor while sparing normal tissues by selective retention of a radionuclide in a tumor. 5 Unlike external radiotherapy, the dosimetric effectiveness of PRRT is dependent on a targeting moiety—the molecular constituent that either binds onto or is sequestered by tumor cells. 6 –8 To be an effective targeting agent, the radiopharmaceuticals must have a greater affinity to tumors than normal tissues, thus increasing its therapeutic efficiency. The chemistry of the ligand determines the therapeutic radionuclide that can be coupled, whereas the pharmacokinetics within the body influences the dose to critical organs. 9 The pharmacokinetics of a targeting agent includes not only the biological path that the agent takes throughout the body but also the uptake and clearance characteristics within the tumor. In the clinical phase II trial with 177Lu-DOTATATE, 30%–47% overall response rate was recorded, with a median time to progression of >36 months. Also, significant biochemical and symptomatic responses in functioning tumors were encountered for PRRT. 10,11 PRRT with 177Lu-DOTATATE is a promising new tool in the management of patients with inoperable or metastasized NETs. 12 –15
The bone marrow is the dose-limiting organ in most types of radionuclide therapy, since its rapidly dividing cells are sensitive to radiation. 16 –18 However, the kidneys are sensitive to radiation as well, and given the relatively high renal retention of radio-peptides, the kidneys are the critical organs in PRRT. 19 –21 Although renal and hematologic toxicity is known to occur, PRRT is considered to be relatively safe treatment option for patients with NETs. Lu-DOTATATE owing to its low energy emission and short range of beta particle (E max=497 keV; T 1/2=6.73 days) shows lower renal and hematological burden compared with 90Y-DOTATOC. 22 Several patients showed a decline in creatinine clearance of >40% per year following peptide-receptor radiation therapy with 90Y-DOTATOC, with cumulative mean absorbed renal dose of ∼27 Gy. 23,24 177Lu-DOTATATE seems to share a better effect on small lesions, compared with 90Y-DOTATOC, which, in turn, appears more efficient in larger lesions. However, the patient's performance status, the biological characteristics of the tumor, the extent of liver involvement, and the uptake of radiopharmaceutical in Octreotide scan are crucial for the outcome.
Several different approaches have been used to reduce the risk of nephrotoxicity in PRRT. Most of these methods aim at decreasing the radiation dose to the kidney. Reduction of proximal tubular reabsorption of peptides is one of the best approaches used in PRRT. The coadministration of positively charged amino acids, such as L-lysine and/or L-arginine, competitively inhibits the proximal tubular re-absorption of radio-peptide resulting in a reduction in the renal dose ranging from 9% to 53%. 25,26
Several studies on the effects of radiation on kidneys from internal irradiation have been presented within the field of PRRT. Analysis of glomerular filtration rate (GFR) and serum creatinine (SCr) as an indicator of renal function is a frequently used endpoint for renal toxicity in humans.
The aim of this study was to investigate the long-term behavior of renal function and hematological function in patients who underwent dosimetry studies of radionuclide therapy of NETs with 177Lu-DOTATATE.
Materials and Methods
Patients
From March 2008 to September 2011, a total of 57 patients were recruited in the study. All patients underwent 68Ga-DOTANOC PET-CT study at our department for staging and identification of distant metastases. Patients older than 18 years with intense sst receptor expression on tumor cells as visualized on 68Ga-DOTANOC PET-CT scan were included in this therapy. Ten patients (medullary thyroid cancer) demonstrated minimal uptake of 177Lu-DOTATATE and were not considered for further treatment. Only 47 patients with NETs underwent dosimetric studies and were followed up with renal and hematological function. Four patients among 47 patients were declined further treatment and exited from study (2 patients after single dose of activity administration, i.e., 5.55 GBq, whereas another 2 patients after second cycle of activity administration, i.e., 11.1 GBq). The study was approved by hospital ethics committee of All India Institute of Medical Sciences (AIIMS) (New Delhi, India). The patients were explained the potential benefits and complications of the treatment. Written consent was obtained from all participants before recruitment into trial.
Radiopharmaceuticals
GMP-grade sst analog precursor for radiolabeled DOTATATE acetate was obtained from ABX Advanced Biochemical Compounds, Germany. 177LuCl3 was obtained from BARC, AERB (Mumbai, India). 177Lu-DOTATATE was locally prepared as previously described by Das et al. 27 Greater than 95% radiolabeling yield of 177Lu-DOTATATE was ensured before therapy (radiolabeling yield or efficiency was determined by thin layer chromatography method).
177Lu-DOTATATE was prepared as described by Das et al. 27 About 1000 mL of mixture of L-arginine and L-lysine (25 g arginine and 25 g lysine) was infused to each patient 30 minutes before infusion of 177Lu-DOTATATE and continued over next 4 hours to reduce the radio-peptide uptake in kidneys. About 3.7–7.4 GBq of 177Lu-DOTATATE was infused to each patient using a continuous infusion pump system and completed within 45–90 minutes.
Method of dosimetry
The radiation absorbed dose estimations of kidney in this study were determined according to the MIRD scheme. 28 For calculating absorbed dose of kidney, an accurate determination of time-dependent activity in the tissues of the body is required.
To determine the time activity profile in kidney or specific organ, serial planar anterior and posterior whole-body scans (WBSs) were acquired (ECAM Dual Head Siemens gamma camera: LEAP collimator, dual energy window, peak at 208 keV and 110 keV; 15% energy window; 15% energy window; 15 cm/min) at different times following an injection. The first WBS (with full bladder) was acquired 30 minutes after the administration of 177Lu-DOTATATE, whereas subsequent WBS (with empty bladder) was acquired at 4, 8, 24, 48, 96,144, and 168 hours (Fig. 1). The whole-body counts of first WBS with full bladder were defined to be 100% activity of the administered activity. All other activities were expressed as percentage of administered activity (%IA). These percentages at different time points of WBS were used to describe the uptakes of the radioactivity in the body. Regions of interest (ROIs) were drawn manually over the source organs, including kidneys. ROI data were quantified by using geometric mean of anterior and posterior WBS with geometric-based background subtraction method. As a result of geometric mean and background correction, time-dependent %IA for the kidneys was calculated. These %IA were then fitted depending on the degree of correlation to a mono- or bioexponential function with the help of OLINDA/EXM software. 29 The total number of disintegration obtained from kinetic input form option of OLINDA/EXM that was equivalent to the cumulated activity and S-values for the 177Lu and different phantoms were used to calculate the radiation absorbed dose in kidney in the unit of mGy/MBq.

Whole-body scans after 24 hour postinjection of 177Lu-DOTATATE. Anterior and posterior images showing ROI on kidneys and tumors used for dosimetric calculation. ROI, regions of interest.
Radiation dose of kidney over single administered activity was calculated from radiation absorbed dose of kidney (mGy/MBq) obtained from OLINDA/EXM. Dosimetry was performed during the first and second cycles of treatment by using earlier mentioned method and was used to plan further treatments. Similarly, total radiation absorbed dose of kidney for the cumulated administered activity was calculated for each patient.
Determination of GFR
All recruited patients underwent GFR estimation before each therapy cycle and follow-up. About 7.4 MBq of 99mTc-DTPA was injected intravenously and the syringe was flushed with blood of the patient. Standards were prepared by dilution from duplicate syringes. Two blood samples were drawn into standard EDTA anticoagulated sample tubes at 60 and 180 minutes after injection, using a vein other than that used for injection. After centrifugation, duplicate samples of plasma and standard were pipetted, they were counted, and the results were averaged. The two-point GFR was calculated from the integral of the plasma time-activity curve. The two-point GFR estimates were obtained by fitting the data to the open linear single-compartment model. 30,31
Mathematical derivatives
Two-sample method (error <4 mL/min) was used to calculate the GFR. First sample was withdrawn 60 minutes after injection of 99mTc-DTPA (T
1=60 minutes) and the second sample at ∼180 minutes (T
2=180 minutes).
where D is dose (counts/min), P 1 is plasma activity at time T 1 (counts/min·mL), and P 2 is plasma activity at time T 2 (counts/min·mL).
Programmable software based on this equation was used to calculate GFR.
Follow-up and data analysis
The interval between each cycle of therapy was typically between 10 and 12 weeks. Patients were treated up to a cumulative activity of 29.6 GBq unless the dosimetric calculations indicated that the radiation dose to the kidneys would exceed 23 Gy. Routine hemogram, liver function test, kidney function test, and specific biochemical markers of tumors were performed before each treatment administration and continued up to 6 months after last cycle of therapy. Baseline variables were compared with variables measured 6 weeks after last therapy administration.
Statistics
Kolmogorov–Smirnov's test was used to assess normality of data. Mean and standard deviation were used to describe normally distributed continuous variables. Pearson's correlation coefficient was calculated to assess relationship between continuous variables. Independent sample t-test and paired t-test were used wherever applicable and multivariate analysis was performed when there was more than one significant variable.
Results
Baseline patient characteristics
The mean age of 47 patients (men=32; women=15) was 48.1±15.3 years. The mean SCr and GFR were 0.86±0.19 mg/dL and 86.8±15.4 mL/1.73 m2/min, respectively. The mean cumulative activity administered to patients was 20.1±6.7 GBq resulting in total renal absorbed dose of 12.7±4.1 Gy.
Renal toxicity
Serum creatinine
The mean SCr in 47 patients increased to 1.0±0.2 mg/dL, which was a significant increase from baseline value of 0.86±0.19 mg/dL (p<0.0001). Baseline SCr was the only significant predictor of post-treatment SCr (r=0.430; p=0.003). Post-treatment SCr did not show any statistically significant correlation with age (p=0.436), cumulative activity (p=0.733), and total renal dose (p=0.183). Baseline SCr had no statistically significant correlation with mean absorbed dose of kidney (p=0.232).
Sixteen patients developed WHO grade 1 renal toxicity (SCr, 1.1–1.5 mg/dL), which was designated as group 2, and no renal toxicity was found in 31 patients (group 1). The baseline SCr of patients in group 1 was 0.80±0.17 mg/dL, which was significantly lower compared with 0.98±0.19 mg/dL in group 2 (p=0.002). On multivariate analysis, a statistically significant increase was observed in SCr post-treatment, the rise being greater in group 2 than in group 1 (p<0.001) (Fig. 2).
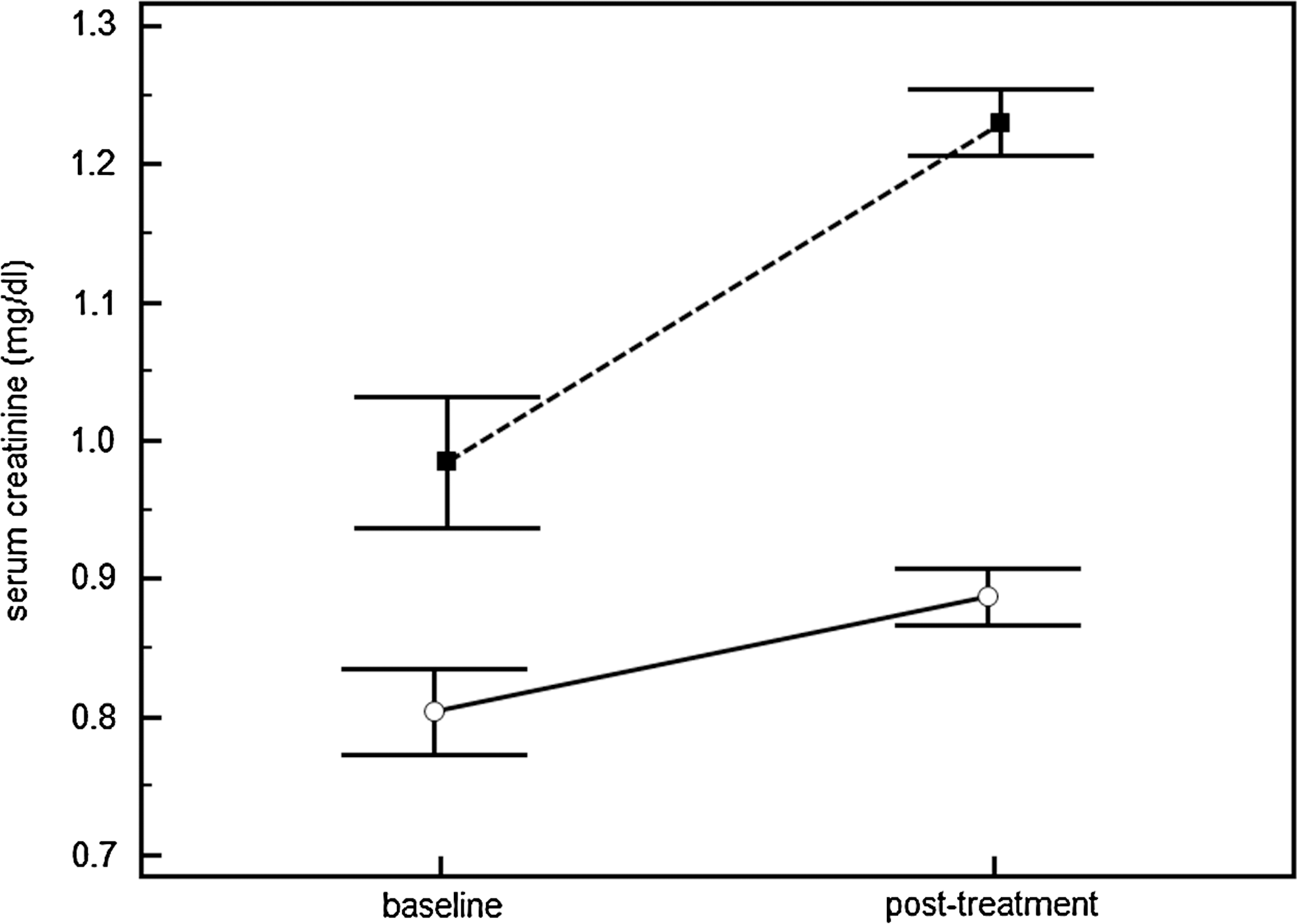
Clustered variable graph showing mean±SEM of SCr in group 1 and group 2. Circular markers represent SCr of patients in group 1 (patients with normal SCr after PRRT); solid square markers represent SCr of patients in group 2 (patients developing WHO grade 1 toxicity after PRRT). PRRT, peptide receptor radionuclide therapy; SCr, serum creatinine.
Glomerular filtration rate
The mean GFR in 47 patients demonstrated a significant decrease to 66.1±14.5 mL/1.73 m2/min compared with baseline GFR of 86.8±15.4 mL/1.73 m2/min (p<0.0001). There was a moderately strong negative correlation between last measured GFR and age of patients (r=−0.370; p=0.01). Similarly, lower post-treatment GFR values were observed with increasing cumulative dose (r=−0.339; p=0.019) and total renal radiation absorbed dose (r=−0.440; p=0.002). A strong positive correlation was observed between pretreatment and post-treatment GFR (r=0.579; p<0.0001). However, on multivariate analysis, post-treatment GFR correlated with total renal radiation absorbed dose (p=0.034) and pretreatment GFR (p=0.005) whereas other variables were rendered insignificant (Figs. 3 and 4). Interestingly, there was a moderately strong inverse correlation between mean absorbed dose to kidneys (mGy/MBq) and baseline GFR estimation (r=−0.383; p=0.008).
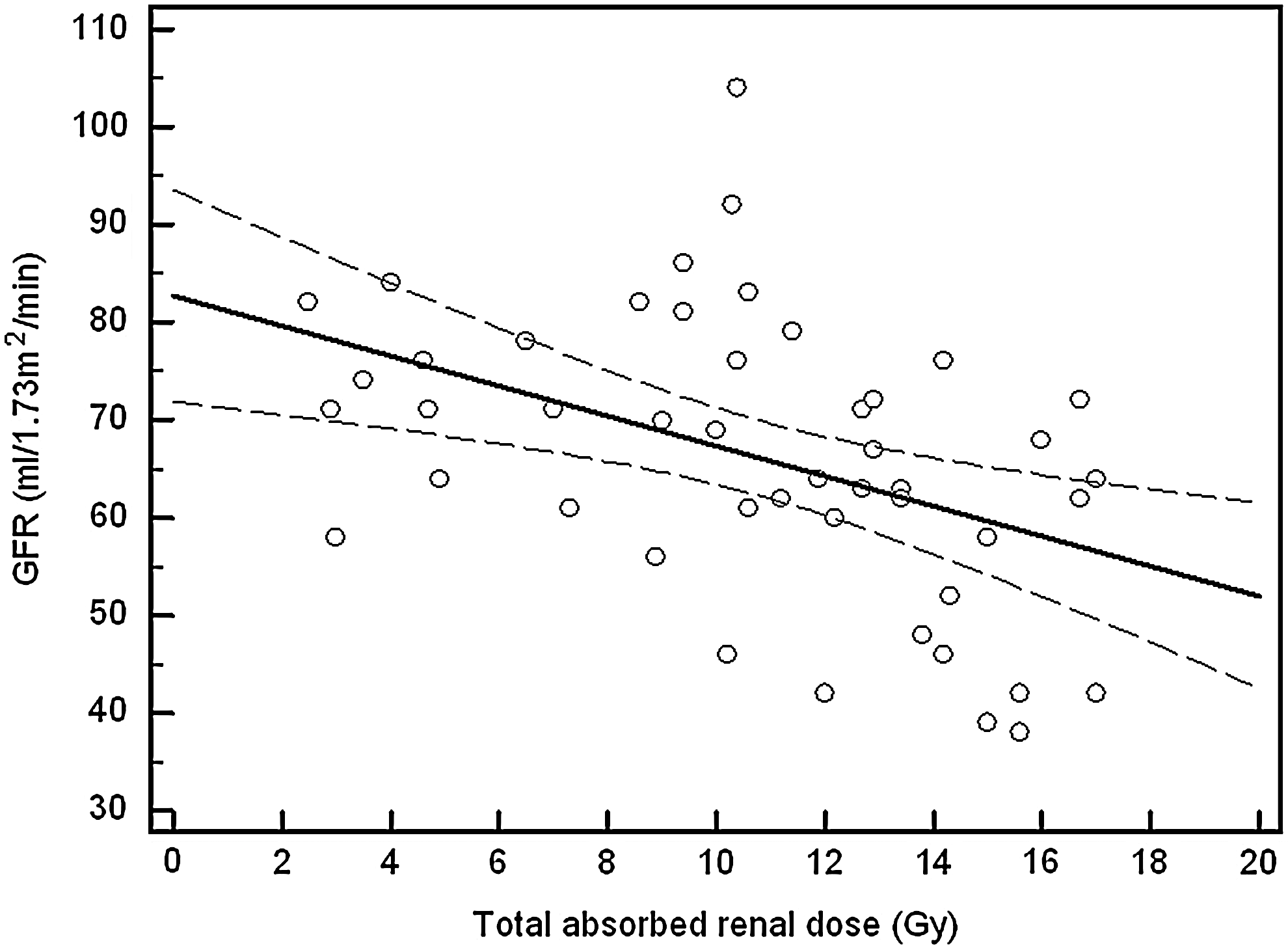
Scatter diagram with regression line (solid straight line) showing relationship of GFR after treatment and total absorbed renal dose. Curved dotted line represents 95% confidence interval curve. GFR, glomerular filtration rate.

Scatter diagram showing relation of baseline GFR on X-axis and last measured GFR after treatment on Y-axis.
Hematological toxicity
Two patients developed WHO grade 4 32 anemia (Hb<4.9 gm/dL) 4 weeks after the first cycle, which resolved to grade 2 spontaneously 4 weeks later. One of them recovered after 10 weeks and was administered second cycle, whereas the other patients required blood transfusion support. One patient developed grade 1 thrombocytopenia 4 weeks post-PRRT. No significant WHO grade toxicity was observed for white blood cells (WBCs). However, a significant decrease in WBC counts was observed with treatment when paired t-test was applied. Baseline and post-treatment of hematological parameters are summarized in Table 1.
Mean±standard deviation of variables at baseline and after treatment. a p<0.05 is considered significant.
WBCs, white blood cells.
Discussion
Although 177Lu-DOTATATE has proven to be an effective therapeutic strategy in NETs, nephrotoxicity is the major limiting factor associated with PRRT. 33 Since this radiopharmaceutical has a predominantly renal clearance, the kidneys have always been considered the “critical organs.” As 177Lu-DOTATATE is excreted through kidney, it is reabsorbed by the proximal convoluted tubules (PCTs) of kidney which then irradiate glomerular capillaries (GCs) of kidney causing nephrotoxicity. 34,35 Hence, function of kidneys is reduced and it depends on radiation absorbed dose in PRRT.
Reduction of radiation nephropathy from 177Lu-DOTATATE can be accomplished by administration of positively charged amino acids before and during the course of infusion of radio-peptide. Coinfusion of mixture of amino acids inhibits the uptake of radiolabeled peptides, such as L-lysine and/or L-arginine, which has been found to be useful in experimental and clinical studies to counteract the reabsorption of peptides. Typically, renal dose reduction of up to 25% is possible with administration of mixed amino acids. Additional investigations revealed that solutions with a combination of 25 g lysine and 25 g arginine in 1 L (pH=7.3 and osmolarity=400 mOsmol/L) were safe and more effective than mixed amino acids. 36 –39 In this study, we have used this combination in all patients receiving PRRT.
Various methods are available to evaluate the renal toxicity, such as SCr, creatinine clearance, and GFR (methods: GFR by inulin, GFR by in vivo, and GFR by in vitro two-sample single injection). GFR is likely to change after irradiation as radiopharmaceutical in PCTs is close to GCs and cross-fire effect causes glomerulosclerosis. 25 99mTc-DTPA, on the other hand, measures glomerular filtration that is a function of GCs in Bowman's capsule, with minimal regeneration repair capability. 30,40
In our study, post-therapy SCr did not increase proportionately with cumulative radioactivity and renal absorbed dose of kidney (Fig. 5). SCr is dependent on multiple parameters, such as body weight, exercise, diet, tumor burden, sex, and muscle mass, which need to be corrected for accuracy of assessing renal function. 41 Since correction of any variable is associated with an increase in statistical error, SCr may not provide precise information about renal toxicity of 177Lu-DOTATATE. Also changes in SCr are often delayed since it is mainly secreted by PCTs that have considerable repair capacity postirradiation. 42 An interesting observation of the present study was a significantly greater increase in SCr after PRRT in patients with SCr levels of 0.98 mg/dL at baseline compared with patients with SCr of 0.8 mg/dL. Thus, patients with high normal baseline SCr must be closely monitored for nephrotoxicity after PRRT.
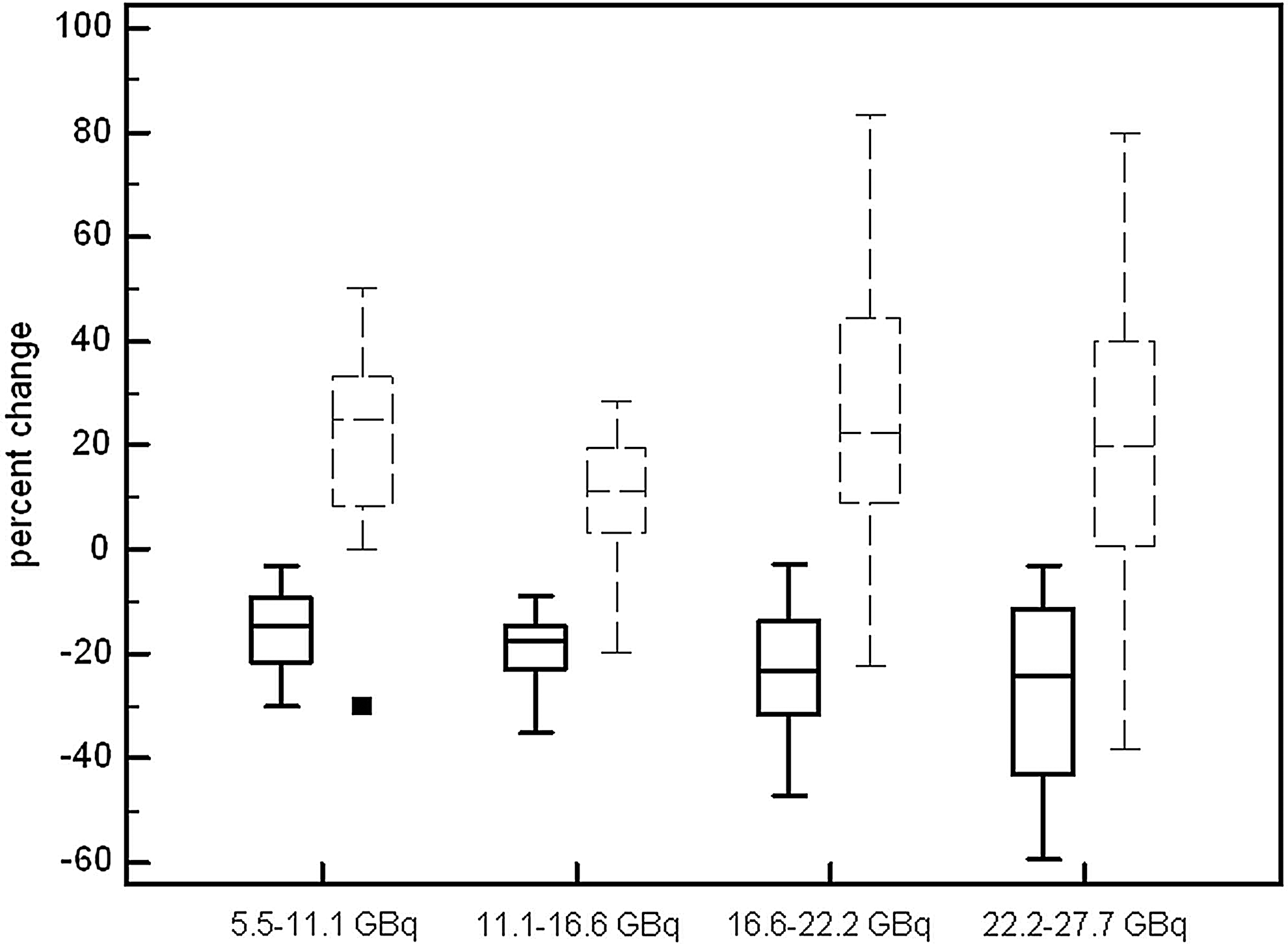
Box and whisker plot showing percentage change in GFR and creatinine plotted on Y-axis with respect to cumulative activity administered. Solid line represents GFR and broken lines represent creatinine. Percent change was calculated as [(post-treatment variable − baseline variable)/baseline variable]×100.
In this study, we analyzed the most relevant parameter of renal function, the GFR (in vitro method), in individual patients at baseline and 6 weeks after last cycle of treatment after PRRT with 177Lu-DOTATATE. Our results demonstrate that after PRRT an individual rate of decline varies widely among patients. The decline in GFR tends to be irreversible and proportional to radiation absorbed dose of kidney. This suggests that treatment with 177Lu-DOTATATE may trigger a process at the level of GCs that persists long after the last cycle of PRRT.
Patients with mildly impaired renal function (GFR) at baseline tend to receive higher mean absorbed renal dose likely because of greater retention of radiotracer by kidney and higher radioactivity from other source organs due to decreased clearance. This explains the greater detriment in renal function in such patients with increasing cumulative activity. However, this pattern was not observed with baseline SCr and mean absorbed renal dose.
It is known that substantial variation exists in uptake and mean residence time of 177Lu-DOTATATE in the kidneys between individual patients. Clinical experience and dosimetric studies clearly indicate that this renal threshold does not accurately correlate with the renal toxicity observed in patients undergoing PRRT. 43 However, as per our observations, baseline GFR can provide an estimate of the mean absorbed dose to kidney making it possible to make estimates for cumulative activity to be administered to the patients, finding which has been recently published in literature. 44
Hematological toxicity was reported in 2 patients (4.3%) after PRRT. In our study, 2 patients with poor general condition and low KPS had evidence of grade 4 toxicity (WHO) after single administration. Fall in WBCs was observed virtually in all patients in our study, though significant toxicity was not witnessed. This decrease can be explained by the fact that WBCs are known to be the most radiosensitive cells of body. 20 However, hemoglobin and platelets remained relatively unchanged with treatment. Villard et al. 44 have also reported severe transient hematologic toxicity in 11 out of 249 (4.4%) patients, leucopenia being the most predominant type of toxicity.
In our present study, GFR and SCr levels were analyzed 6 weeks after completion of PRRT. However, Bodei et al. 45 have described decline in renal function even up to 2 years after PRRT. Thus, a long follow-up is mandatory to observe the final outcome and toxicity of PRRT.
Conclusions
Our data concluded that PRRT with 177Lu-DOTATATE leads to deterioration of renal function manifested by a decline in GFR and rise in SCr. The rate of decline in GFR is less in patients having relatively preserved renal function at baseline, which can be attributed to lower renal retention of radio-peptide and hence lesser renal absorbed dose. Also, GFR before treatment influences the retention of isotope and can thus predict the rate of detriment of renal function with PRRT. Serious hematologic toxicity may not occur in PRRT; however, mild WBC toxicity may appear because of radiosensitivity of lymphocytes.
Footnotes
Acknowledgments
The authors greatly appreciate and acknowledge the invaluable contributions of Dr. Meera Venkatesh, Dr. Sharmila Banerjee, Dr. Tapas Das, and Dr. Sudipto Chakraborty of BARC and Dr. MRA Pillai of IAEA to start 177Lu- DOTATATE therapy at All India Institute of Medical Sciences (AIIMS).
Disclosure Statement
No competing financial interests/conflicts of interest exist for this article.