
Abstract
For more than 20 years interleukin-2 (IL2) was the preferred treatment for medically fit metastatic melanoma patients, but recently two new agents, ipilimumab and vemurafenib, were approved for stage IV disease. Single-institution data were used to determine the long-term survival rate for IL2-treated melanoma patients, and whether use of inpatient IL2 had declined recently. Between May 1987 and April 2010, 150 patients were hospitalized for high-dose, intravenous (i.v.) IL2. The average number of IL2 patients increased from 5.4 per year during 1987–1991 to 5.8 during 1992–1997 after regulatory approval of IL2, to 8.3 during 1998–2006 after a marketing indication in metastatic melanoma was granted, but dropped to 3.0 during 2007–2010. At the time of treatment, median age was 52 years; 27% were 60 years of age or older. At the time of analysis 122 patients were deceased. Median survival from the start date of IL2 treatment was 15.6 months, with a 20% 5-year survival. Among patients enrolled in clinical trials, there were as many nonresponders who survived 5 years as responders, which is consistent with a delayed immunotherapy benefit. In the absence of long-term survival data for these newer agents, IL2 probably should still be the preferred initial treatment for most patients with metastatic melanoma who are medically fit.
Introduction
Melanoma remains a significant medical problem in the United States with an estimated 76,250 new diagnoses in 2012 and 9,180 deaths, representing 4.7% of all newly diagnosed cancers and 1.6% of all cancer deaths. 1 Deaths from melanoma occur because of distant metastatic disease, which is identified in about 4% of patients at diagnosis, but can appear any time subsequently with about 20,000 new diagnoses of metastatic melanoma each year. Nationally, the relative 5-year survival rate for all melanoma patients diagnosed during 2001–2007 was 98%, but for patients with distant disease, the observed 5-year survival rate was about 10%, and the relative 5-year survival rate 15%. 1
The treatment of metastatic melanoma remains unsatisfactory. Agents commonly used include the chemotherapy agent dacarabazine, and its oral prodrug temozolomide, and the chemotherapy combination of paclitaxel and carboplatin. Other chemotherapy combinations that have been popularized include carmustine (BCNU) plus cisplatin and dacarbazine (BCD), as well as vinblastine, plus cisplatin, and dacarbazine (VCD). Biotherapy products include the immune cytokines interferon-α (IFNx) and interleukin-2 (IL2), and the recently approved anticytotoxic T lymphocyte antigen-4 (CTLA-4) monoclonal antibody ipilimumab. 2 Also recently approved was the oral tyrosine kinase inhibitor vemurafinib. Because of the recent introduction of these latter two agents, we wished to examine the use of inpatient IL2 over time in our hospital, and determine the long-term survival of patients who were so treated. We hypothesized that fewer patients were treated with IL2 in recent years, but that more than 10% of patients previously treated with IL2 would survive at least 5 years based on concepts of a delayed immunotherapy benefit that would not necessarily be associated with objective responses.
Materials and Methods
A retrospective analysis was performed to determine the long-term survival of patients with metastatic melanoma whose survival data were stored in the Hoag Hospital cancer registry, using computer software designed for this purpose (Electronic Registry Systems, Inc., Cincinnati, OH). Patients who had received inpatient IL2 were identified from clinical trial accrual lists, pharmacy logs, and financial billing records. The year in which inpatient IL2 therapy was initiated was noted for each patient. Kaplan-Meier curves for observed survival were calculated from the date of original diagnosis, and from the date the inpatient IL2 therapy was initiated.
Results
Table 1 summarizes the 150 patients who were hospitalized for IL2 infusional therapy between May 1987 and April 2010. All had regionally recurrent or distant metastatic melanoma at the time of IL2 therapy. Because they were not all treated in the context of a clinical trial, important prognostic information was not available, including sites and size of metastatic cancer lesions, Karnofsky or Eastern Cooperative Oncology Group performance status, and serum lactate dehydrogenase. Prior to 1998, many of the patients received IL2 alone, or in combination with other cytokines or adoptive cell therapies as part of ongoing clinical trials. 3 –5
IL2, interleukin-2.
Distribution by year in which these patients were diagnosed is shown in Figure 1. While most patients were diagnosed after 1980, some had diagnoses dating back to the 1960s. The increase in numbers after 1990 likely reflects the increasing incidence of melanoma, but also the bias resulting from patients being referred for immunotherapy. The median survival for these patients was more than 5 years from the date of diagnosis.

Distribution of patients by year of first diagnosis of melanoma.
Distribution by year in which IL2 therapy was initiated is shown in Figure 2. The average number of IL2 patients increased from 5.4 per year during 1987–1991 to 5.8 during 1992–1997 after approval of IL2, to 8.3 during 1998–2006 after a marketing indication in metastatic melanoma was granted, but dropped to 3.0 during 2007–2010. Many patients were referred to Hoag Hospital for treatment in 1987 in order to have access to IL2 in investigational protocols, because few treatment sites existed at that time, and there was great enthusiasm for IL2 based on results published on 07 April 1987. 6,7 IL2 was approved for a marketing indication in renal cell cancer in 1992, but the highest annual numbers of melanoma patients treated with inpatient IL2 occurred after the U.S. Food and Drug Administration (FDA) granted a marketing approval for IL2 in metastatic melanoma in 1998. About this same time it was becoming apparent that lower dose outpatient schedules of IL2 administration were less effective than the higher dose regimens that required close monitoring in a hospital setting because of toxicity. 8 The recent dramatic decline in IL2 utilization was temporally related to the testing of sorafinib in combination with temozolomide, or with carboplatin and paclitaxel, and trials with ipilimumab and vemurafinib.

Distribution of patients by year in which they received inpatient intravenous (i.v.) interleukin-2 (IL2) therapy.
Survival following treatment with IL2 is shown in Figure 3. Follow-up was excellent; only two patients were censored within 6 months of starting IL2, and only three others were censored within 1 year. At the time of analysis there were 122 patients deceased; 28 were censored alive. The median survival was 15.6 months, the 2-year survival 41%, and the 5-year survival 20%. There were 23 patients known to have survived more than 5 years after initiating IL2, and 10 are known to have survived beyond 10 years. Of note, 9/62 (14%) of patients treated between 1987 and 1997 survived 5 years, compared with 14/41 (34%) treated during 1998–2004 (X 2 , p=0.019). This is likely because patients treated in the earlier era probably were more heavily treated and had higher tumor burdens at the time of treatment, than in more recent years.

Survival from initiation of inpatient i.v. IL2 therapy.
Discussion
In this article we report a 5-year survival rate of 20% following treatment with high-dose infusions of IL2 in patients with metastatic melanoma, but also document the marked decline in the use of inpatient IL2 therapy for such patients in recent years. The 5-year survival rate and recent decline in IL2 utilization are similar to what was observed in metastatic renal cell cancer. 9 The numbers of patients treated with intensive IL2 increased substantially after regulatory approval for marketing of IL2 in melanoma in 1998, but decreased markedly in recent years as newer effective therapies entered clinical trials (Fig. 2). The numbers of patients treated with inpatient IL2 likely would have been higher during 1992–1997 except for the enrollment of many patients into trials of lower doses of IL2 in the outpatient setting.
A representative experience with various systemic treatment regimens for metastatic melanoma is shown in Table 2. The data summarized include the following: (1) the eight IL2 trials that were collated for the submission that led to regulatory approval in melanoma 10 ; (2) multi-institution randomized trials of high-dose bolus IL2±IFNx i.v. interferon-α (IFN), 11 i.v. dacarbazine versus oral temozolomide, 12 cisplatin, vinblastine, dacarbazine, (CVD)±IL2/IFN, 13 ipilimumab±gp100 versus gp100, 14 dacarbazine±ipilimumab, 15 vemurafenib versus dacarbazine, 16 paclitaxel-carboplatin±the anti-K-ras TKI sorafenib, 17 paclitaxel-carboplatin±bevacizumab, 18 and pegylated IFN 19 ; (3) a multi-institution phase II trial of vemurafinib 20 ; and (4) single-institution randomized trials of IFN, 21 dacarbazine versus BCD-tam, 22 BCD±IL2/IFN, 23 and CVD±IL2/IFN, 24 and two single-institution trials of CVD±IL2/IFN. 25,26 For many of these trials the 2-year survival rates had to be extrapolated from published survival curves. At best, the 2-year survival rate for any of these trials is 20%, with the exception of the ipilimumab plus dacarbazine as first-line therapy for melanoma. 15 It appears that regimen is projected to be associated with a 4-year survival rate as high as 20%.
BCNU, carmustine; DTIC, dacarbazine; CSP, cisplatin; VBL, vinblastine; IFN, interferon; Mab, monoclonal antibody; TKI, tyrosine kinase inhibitor; BCD, BCNU (carmustine), cisplatin, dacarbazine; CVD, cisplatin, vinblastine, dacarbazine; Med PFS mos, median progression free survival in months; Med OS mos, median overall survival in months.
The immune-stimulating cytokine IL2 was originally approved in the United States in 1992 for the treatment of metastatic renal cell cancer, but in 1998 a marketing indication in metastatic melanoma was granted based on a compilation of 270 patients enrolled in eight phase II trials that utilized high-dose bolus IL2 therapy. 10 The objective response rate was only 16%, but the probability of remaining in complete remission was about 60% during 2 to 10 years of follow-up for the 6% of patients who experienced a complete response. The 10% with a partial response had median duration of response of less than 3 months, but two patients were still progression free 6 to 9 years following treatment. The high-dose bolus regimen was adopted by the Surgical Branch of the National Cancer Institute and the NCI-funded Cytokine Working Group. High-dose continuous infusion IL2 was adopted as the preferred treatment for metastatic melanoma in Europe and by the community-based National Biotherapy Study Group (Cancer Biotherapy Research Group). 27 As a monotherapy, lower doses of i.v. bolus IL2 or low-dose continuous infusion IL2 were associated with disappointing response rates. 2 The importance of dose was also supported by the observation of a 19% response rate with four durable complete responses among 26 patients whose disease had not responded to biochemotherapy utilizing lower doses of IL2. 28
As summarized elsewhere, 2 numerous trials explored various doses and schedules of IL2 in combination with other biologicals and/or chemotherapy. The combination of IFNα and IL2 failed to show an advantage compared with single-agent high-dose bolus IL2 in randomized trials 11 or in a multicenter phase II trial in which IFNα was combined with high-dose continuous infusion IL2. 29 For several years the most popular biochemotherapy regimens combined IL2 with BCD±tamoxifen, or CVD. These regimens included administration of intensive IL2 in the hospital setting. An MD Anderson retrospective comparison of 264 patients treated with CVD/IL2/IFNα and 352 patients treated with CVD±IFNα (but not IL2) revealed a superior survival for the patients who received IL2, including a 5-year survival rate of 17%. 25 Another single-institution series for this same regimen followed by maintenance biochemotherapy showed that 135 patients (including 9 with inoperable stage III disease) had a 5-year survival rate of 28%. 26 The response rates in all of these biochemotherapy trials were much higher than that reported for IL2 alone. As shown in Table 2, randomized trials reported somewhat lower response rates, but confirmed that response rates were higher for IL2-based combination biochemotherapy. But the regimens appeared to be no better than chemotherapy alone in terms of survival. However, many of the patients who were randomized to chemotherapy alone subsequently received IL2, and none of these regimens were compared with IL2 alone.
Unfortunately, the intensive inpatient IL2 regimens, whether given as bolus, continuous infusions, or a combination of both, are associated with significant toxicities that can be life-threatening. 30 Such treatment requires close monitoring in the inpatient hospital setting and medical management by physicians and nurses experienced in delivery of the therapy. Therefore, patient selection and treatment in centers experienced in IL2 treatment are critical, especially since most oncologists have had limited or no experience in the delivery of intensive IL2. 8
In the past 2 years, two new agents, the oral tyrosine kinase inhibitor vemurafinib, which targets the VE600 B-Raf mutation, and the anti-CTLA-4 monoclonal antibody ipilimumab, were approved for the treatment of metastatic melanoma. The effect of these agents on long-term survival is not yet clear. Although these are administered in the outpatient setting, both are also associated with significant toxicities, the timing of which is not predictable. Ipilimumab is administered as 4 doses every 3 weeks while vemurafinib is given indefinitely. Both of these treatments are associated with charges of over $100,000 per year, but do not require hospitalization. Inpatient IL2 treatment is associated with charges of about $10,000 per day, so two cycles may be associated with charges of $100,000.
The approval of ipilimumab is noteworthy because in 676 previously treated patients, the progression-free survival and objective tumor response rates (6% to 11%) were unimpressive, but survival was improved: median 10.0 versus 6.4 months compared to a gp100 peptide vaccine control arm. 14 In 502 patients previously untreated for metastatic disease, ipilimumab plus dacarabazine was superior to dacarbazine alone for both response rate (15.2% vs. 10.3%) and survival (11.2 vs. 9.1 months). 15 Ipilimumab is associated with a high rate of autoimmune adverse events, with grade 3 or 4 autoimmune adverse events reported in 10% to 15% of patients. 14 The combination of ipilimumab plus dacarbazine was associated with a 56% rate of grade 3 or 4 toxicity, which was about twice as high as documented for placebo plus dacarabzine. 15 The severe autoimmune colitis and dermatitis can be life-threatening, and require vigilant monitoring. At the moment ipilimumab plus dacarbazine is the only ipilimumab-based biochemotherapy for which high-level evidence has been published. Despite the increased toxicity of this regimen, in a clinical setting in which a rapid response is needed (such as high tumor burden and rapidly progressing disease), ipilimumab-based biochemotherapy is probably the preferred initial therapy for patients who are not candidates for IL2-based therapy, and whose melanomas lack the VE600 B-Raf mutation. IL2-based biochemotherapy regimens were never compared with IL2 alone, and it is unclear whether ipilimumab-based biochemotherapy regimens will be compared with ipilimumab alone, but this would be an informative trial to conduct.
Vemurafinib is limited to patients who harbor the VE600 B-Raf mutation, but this may be present in up to 50% of melanoma patients. 31 It has the advantage of being an oral agent. About 50% of patients have an objective regression of measurable tumor, and tumor regression is rapid. 18,20,31 The long-term survival benefit for this agent is unclear, but the duration of response is relatively short because of the rapid development of resistance. 32 Vemurafenib is associated with significant photosensitivity and the appearance of cutaneous squamous cell cancers.
It is increasingly evident that immunotherapy may be associated with only stable disease initially, or even some disease progression, but subsequently results in a delayed tumor response and survival benefit. These delayed effects were major issues in the approval for ipilimumab for melanoma, and the immune cell therapy sipileucel T for prostate cancer. 33 Both of these products produced low response rates and no benefit in progression-free survival, but long-term survival benefit was eventually documented in randomized prospective trials. Such observations have led to formulation of newly proposed criteria for determining the efficacy of immunotherapy products, because benefit is not limited to objective responders. 34 Our long-term observations, and those of others, suggest that this is also probably true for IL2 as well.
Most reports of IL2 therapy have emphasized the association between objective response rate and long-term survival, and suggested that there was no benefit for nonresponders. It is well documented that among patients treated with either high-dose bolus IL2 or high-dose continuous infusion IL2, survival is better for patients who achieve a complete response, and patients who achieve a partial response survive longer than patients who do not have an objective response, which includes patients who are considered to have stable disease, or progressive disease. 10,35 However, about 85% of patients treated with IL2 do not have an objective response. Because our study was not prospective, there was no reliable response rate data to correlate with survival, and limited prognostic information for individual patients. However, many of these patients did participate in national IL2-based clinical trials of the Cancer Biotherapy Research Group, in which 37/217 (17.0%) of metastatic melanoma patients had an objective response to regimens containing high-dose infusional IL2. 3 –5 It was previously noted that among 188 melanoma patients who were treated in multi-institutional IL2-based clinical trials, 2/33 (6%) of responders were known to have survived 3 years compared with 8/155 (5%) of nonresponders. In our retrospective study, the 5-year survival rate was 20% for a cohort that included both patients who were not enrolled in clinical trials, as well as those who were.
Should high-dose IL2 still be the preferred treatment for patients with metastatic melanoma? For those patients who are medically fit enough for intensive IL therapy, we feel the answer is still “yes.” As shown in Table 2, at this time, IL2-based regimens are still the only ones for which long-term survival have been documented, although longer follow-up may establish the long-term survival benefit of ipilimumab plus dacarbazine. Figure 4 shows a treatment algorithm that we feel is appropriate for patients newly diagnosed with metastatic melanoma who are not being entered into a clinical trial. For patients with a large tumor burden, but medically fit for IL2, it is better to utilize IL2-based biochemotherapy, because as shown in Table 2, response rates are typically much higher than are observed with IL2 alone. For patients who are not medically fit for IL2 and have a low tumor burden, ipilimumab as single agent is preferred to avoid the toxicity associated when it is combined with chemotherapy. For patients who are not fit for IL2, and have a high tumor burden, then whether the B-Raf mutation is present becomes important. In such patients who are B-Raf mutation negative, ipilimumab-based biochemotherapy is the preferred treatment because of the low response rates and delayed responses associated with ipilimumab alone. For patients who have B-Raf mutation–positive tumors, with extensive distant metastatic disease, vemurafinib is the preferred initial treatment of choice because of the high probability of a rapid response. However, these patients quickly develop resistance, and it is probably best to treat with ipilimumab or IL2 either while these patients are still in remission, or at the first sign of disease progression before clinical status deteriorates. B-Raf is not recommended as the initial approach in patients who are good candidates for IL2 or ipilimumab because of the rapid emergence of resistance, and lack of data for survival benefit.
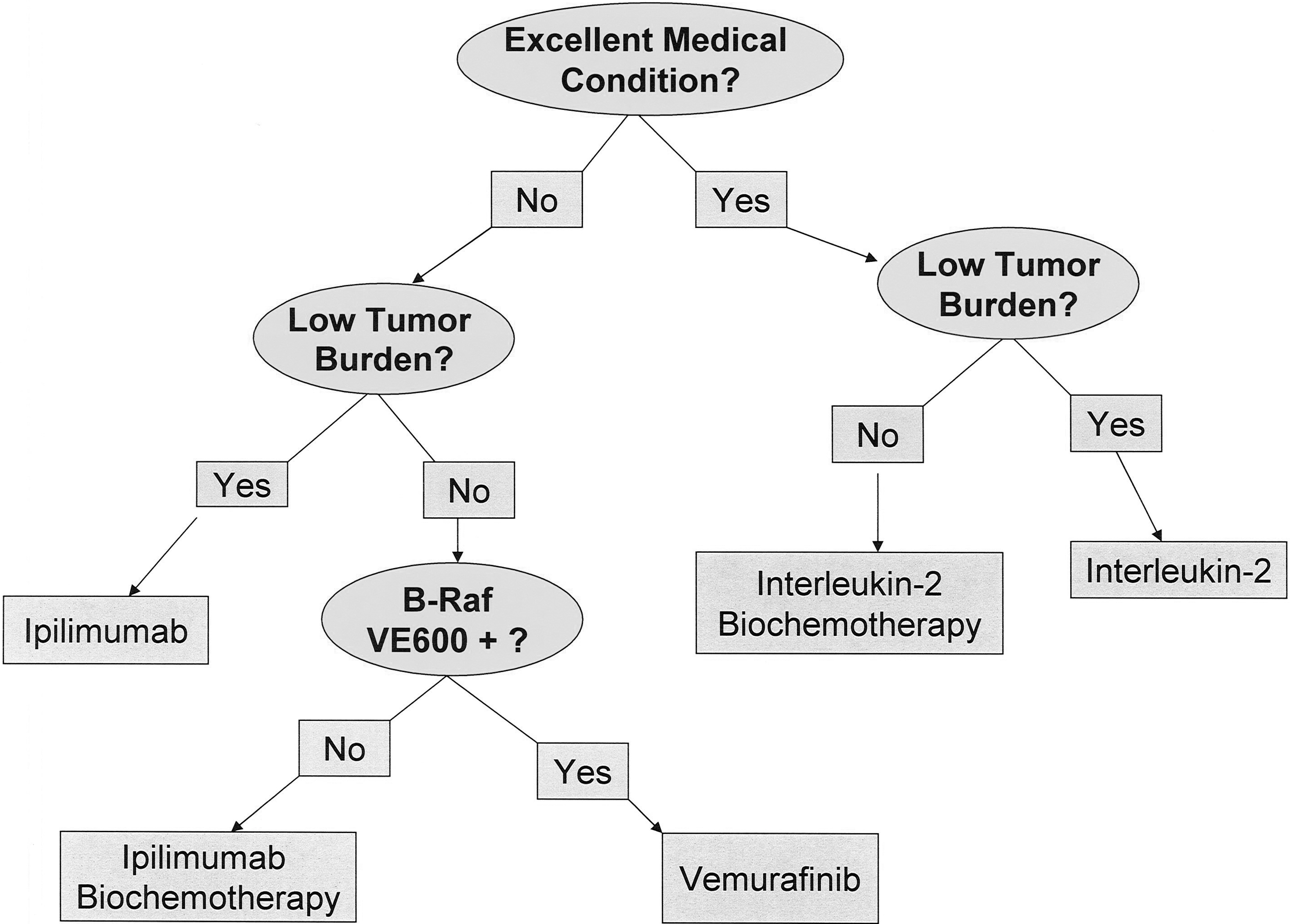
A suggested algorithm for treatment decision making in patients with metastatic melanoma who are healthy enough for treatment, and have no active brain metastases.
The ramifications of different sequences of these therapies, in patients who subsequently relapse, are not clear at this time. The efficacy of both vemurafenib and ipilimumab has been demonstrated in patients who previously received IL2, but we have no data regarding the toxicity or efficacy of IL2 following these new therapies. Unfortunately, patients who are candidates for IL2 at the time of initiating treatment may experience clinical deterioration while progressing during other treatment, and may never again be medically fit enough to receive IL2. In patients receiving IL2 or ipilimumab, there is no need for a quick change to another therapy in the presence of stable disease or even some mild degree of disease progression, because immune effects can be delayed. Initiation of additional treatment should be withheld until it is clear that the patient has steadily progressing disease. In the relapse setting, the non-IL2 side of the algorithm shown in Figure 4 can be applied as a guide therapy. Other than the B-Raf mutation, at present there are no other biomarkers to guide therapy for patients who relapse after immune therapy with IL2 and/or ipilimumab, although a small percentage of patients with acral and mucosal melanomas carry a c-KIT mutation that may respond to imatinib and related agents that target the tyrosine kinase that results from this mutation. 36 It is also noteworthy that patients previously treated with ipilimumab, who are then treated with vemurafinib, may have a much higher rate of dermatitis, 37 and possibly other toxicity. It is possible that administering IL2 after ipilimumab also could be associated with much more severe autoimmune toxicity than traditionally observed with IL2. Because ipilimumab has a demonstrated long-term survival benefit, we would consider that it is used alone or in combination with chemotherapy as the preferred regimen in patients who relapse after previous IL2, even if B-Raf mutation positive, unless there is a high tumor burden and rapidly progressing disease.
Conclusions
Based on existing long-term survival data, we feel that those patients with metastatic melanoma who present in excellent medical condition should still be offered intensive IL2-based treatment regimens as initial treatment.
Footnotes
Acknowledgments
This work was funded by the Hoag Hospital Foundation through the Grace E. Hoag Endowed Chair. The authors wish to thank Stacy Wilton, Michelle Hoffpauer, Carol DePriest, and Pete Vanderplas for their assistance in identifying patients who had received inpatient IL2.
Disclosure Statement
Dr. Dillman has recently served as a consultant to Prometheus, Inc. Other authors declare that they have no proprietary, financial, professional, or other personal interest in any product, service, and/or company that could be construed as influencing the position presented in this article.