
Abstract
Purpose:
To evaluate the efficacy of radionuclide palliative therapy (RPT) in women suffering from painful metastatic bone disease (MBD) due to breast cancer (BrCa), and to investigate the possible relationship between the RPT efficacy and cytokines levels.
Methods:
Sixty-three BrCa women patients with MBD enrolled in a prospective, nonrandomized study. Thirty were treated with Rhenium-186-hydroxyethylidenediphosphonic acid (186Re-HEDP), 21 with Strontium-89-Chloride (89Sr-Cl2), and 12 with Samarium-153-thylenediaminetetramethylenephosphonic acid (153Sm-EDTMP). Blood samples were collected pre- and post-therapy to assess the interleukin (IL)-2, IL-6 and tumor necrosis factor (TNF)-a titers. The palliative effect of the treatment was evaluated using a modified Wisconsin test.
Results:
All three radiopharmaceuticals were equally effective in pain relief. Pain palliation was complete in 52% of patients, partial in 31%, and absent in 16%. Responders to therapy had higher IL-2 and lower IL-6/TNF-a concentrations, compared with nonresponders, even though statistically significant difference in cytokines levels between responders and nonresponders before treatment was noted only for IL-6.
Conclusion:
All used radiopharmaceuticals had the same therapeutic effect. Pretherapy low titers of IL-6 levels seems to have a favorable prognostic value for the therapeutic outcome, while IL-2 and TNF-a alterations pre- and post-therapy can only serve as markers of a better RPT response.
Introduction
Breast cancer (BrCa) is the most frequent cancer among women in the Western world. 1 Bone is the most common site of metastases at time of diagnosis 2 while being the first site of relapse. 3 At post–mortem examination, ∼70% of patients dying from BrCa have evidence of metastatic bone disease (MBD). 4 MBD increases the risk of fractures and spinal cord compression. Patients with MBD usually experience severe bone pain, especially in the advanced disease stages, resulting in poor quality of life. Metastatic bone management should be a multidisciplinary approach including use of conventional analgesia, radiotherapy, surgery, chemotherapy, hormone treatment, radioisotopes, and bisphosphonates. 5
Radionuclide palliative therapy (RPT) with bone-seeking radiopharmaceuticals serves as an alternative to external radiotherapy. RPT may be of particular importance when painful skeletal lesions are widespread in several anatomical regions, especially when cumulative toxicity from previous radiotherapy is at a critical point. β rays emitted from specific radionuclides, usually lead to a favorable therapeutic effect. Three radiopharmaceuticals have been developed: Samarium-153-thylenediaminetetramethylenephosphonic acid (153Sm-EDTMP) and Strontium-89-Chloride (89Sr-Cl2), which have been approved both in the USA and Europe, and Rhenium-186-hydroxyethylidenediphosphonic acid (186Re-HEDP) available only in Europe at the time of the study. All three share common characteristics. 5
The pathophysiology of MBD is complex. At the affected bone, a vicious cycle of signaling takes place: tumor-derived factors stimulate the osteoclasts, which degrade the bone matrix causing release of factors that stimulate tumor cell growth. The tumor cells secrete parathyroid hormone-related peptide, the principal stimulator of osteoclastic proliferation. They also produce other osteoclast-stimulating factors, such as interleukins (IL-11, IL-6, IL-2, and IL-1), prostaglandin E2, tumor necrosis factor (TNF), and macrophage colony-stimulating factor. These factors promote the expression of the receptor activator of nuclear factor κβ (RANK) and RANK ligand (RANKL) on the surface of stromal cells and osteoblasts. RANKL binds to RANK on osteoclast precursors and promotes their differentiation, leading to excessive bone loss. With reciprocal effect, the tumor growth in bone is accelerated by the production of growth factors from the stroma of the bone marrow, such as transforming growth factor-β-, insulin-like growth factors, fibroblast growth factors, and platelet-derived growth factor. 6 All the above-mentioned mechanisms lead to osteopenia and increased fracture risk. The calcium released from the bone matrix can cause malignant hypercalcemia. Consequently, pain and pathologic fractures are the major complications of MBD and can significantly deteriorate the quality of life. 7
Immune system reaction in MBD is not clearly understood; nevertheless it is well known that the prognosis of malignant disease correlates with the status of the immune system, especially with the cell-mediated immunity. 8,9 T-lymphocytes, cytokines, such as IL-2, IL-6, and TNF-a play an important role in tumor progression. Elevated serum IL levels in metastatic BrCa patients correlate with poor response to chemo-endocrine therapy and unfavorable outcome. 10,11 The relationship between serum IL, TNF-a, and the effectiveness of bone palliative therapy, has been yet minimally investigated. 9
Materials and Methods
Patients
All women with MBD due to BrCa referred to nuclear medicine department for RPT in a 5-year period (2006–2011) enrolled in this prospective, nonrandomized study. Before RPT all patients underwent bone scintigraphy, evaluation of renal function, hematological profile, and computed tomographic imaging, to fulfill the following enrolment criteria: (1) sufficient bone marrow function (platelet count >100×109/L, leukocyte count >3.0×109/L and hemoglobin >9.67 g/dL), (2) preserved renal function (creatinine <1.5 μM), and (3) bone scintigraphy consistent with multiple osteoblastic lesions. Patients with metastatic fractures, spinal cord compression, soft tissue tumors causing nerve compression and life expectancy less than 3 months were excluded from the study. MBD had been previously treated with at least three courses of chemotherapy and at least three cycles of bisphosphonates in all patients. Fifty-two women had previously undergone local radiotherapy. They were under analgesic therapy with bisphosphonates (zoledronic acid), nonsteroidal anti-inflammatory drugs and/or opioids, with poor analgesic result. A minimum period of 2 months postradio/chemotherapy and 2 weeks after bisphosphonates administration was required before RPT. In accordance to the Declaration of Helsinki, all women were informed about the study and signed a written consent. A local Ethics Committee approval was also obtained.
Radiopharmaceuticals
RPT was performed in 63 women according to the guidelines of the European Association of Nuclear Medicine. 12 Thirty patients were treated with 186Re-HEDP, 21 patients with 89SrCl2, and 12 with 153Sm-EDTMP, forming Group A, B, and C respectively. A standard dose of 35mCi (1.295 MBq) 186Re, 4mCi (148 MBq) 89Sr, and 1mCi/Kg (37 MBq/kg) 153Sm were slowly (for about 5 minutes) infused. The selection of radiopharmaceutical used was random, driven by the patients' insurance reimbursement strategy and by local radionuclide availability.
Bone scintigraphy
Bone scintigraphy was performed at least 1 month prior to RPT and a scintigraphic score (ScS) from 0 (normal bone scan) to 4 (super scan) was assigned on the basis of the number and/or the extent of metastases according to Soloway's criteria. 13,14
TNF-a, IL-6, and IL-2 measurement
Serum samples for TNF-a and IL-6/IL-2 were collected 1 week before treatment and 9–11 weeks postradiopharmaceutical administration. TNF-α–ELISA, IL-6-ELISA, and IL-2-ELISA Kit of DIAsource ImmunoAssays S.A were used for the immunoenzymetric assay. A group of 15 healthy women, mean age of 55±5.2 years, served as control for the IL-6, IL-2, and TNF-a levels.
Pain score, Karnofsky status
The pain score was assessed, considering the highest value reached, using a modified Wisconsin test (WS), consisting of a five-point pain-rating scale (from 0 to 4) including pain severity, pain frequency, analgesic intake, and change in sleep patterns as described in Table 1. 12 Pain evaluation was assessed before (WS-pre) and 6 weeks after therapy (WS-post), considering a complete response if pain score decreased more than 2 and as partial response if the score decreased 1 or 2 classes, on the basis of WS. The assessment of activity, mobility, and performance status was evaluated using the Karnofsky (KS) performance status score pre- and post-RPT.
Moderate narcotics including codeine at dose between 0.5–1 g.
Morphine or comparable opiates.
Hematologic toxicity
Peripheral blood samples were collected within 1 week before and 20, 30, 40, 50, and 60 days thereafter. White blood cell and platelet counts were measured and the hematologic toxicity was assessed according to Common Toxicity Criteria (CTC). 15
Statistics
Statistical analysis was performed using software MedCalc® ver.12.2.1.0. Data are presented as mean±standard deviation. Shapiro–Wilk test was used for data normality assessment. Two step analysis was performed (intra- and inter-groups); pre- and post-therapy differences in WS, KS, and cytokines levels for patients in the same group were evaluated by Wilcoxon signed-rank test, for responders and nonresponders by Man–Whitney test, and for patients in different radiopharmaceutical groups by Kruskal–Wallis test. Correlations between pretherapy values and response to treatment were assessed by Spearman's rank correlation coefficient. Multiple regression analysis clarified the existence of predictors to the RPT outcome. Receiver operating characteristic (ROC) analysis was used to assess the most accurate description of response to RPT by change in pre- and post-treatment TNF-a and IL-2 levels, to resolve the prognostic efficacy of IL-6 in prognosis of radionuclide analgesia and to determine IL-6 levels with the highest sensitivity and specificity in predicting therapy outcome. p-values less than 0.05 indicated statistical significance.
Results
Mean patients' age, BrCa cells hormone receptor status, existence of visceral metastatic disease, pretherapy KS, ScS, and WS are presented in Table 2. Only KS and ScS pretherapy values significantly differ between responders and nonresponders to RPT (p<0.05). No significant differences in pretherapy variables (KS, WS, TNF-a, IL-2, and IL-6) among different radiopharmaceutical groups were observed. All these variables significantly differed before and after therapy in each group, except for IL-6 levels that did not significantly change before and after treatment (Table 3).
Significant difference between responders and nonresponders, p<0.05.
Mean patients' age, breast cancer cells hormone receptor status (HR), existence of visceral metastatic disease, Karnofsky performance status score (KS), modified Wisconsin test (WS), and scintigraphic score (ScS) pre-RPT in responders and nonresponders' group.
RPT, radionuclide palliative therapy.
Significant difference pre- and post-RPT in the same group, p<0.05 b p=0.051.
Pre- and post-RPT Karnofsky performance status score (KS); modified Wisconsin test (WS); and TNF-a (ng/mL), IL-2 (ng/mL), and IL-6 (pg/mL) levels among different radiopharmaceutical groups.
All data presented as mean±SD except WS presented median (min-max).
IL, interleukin; TNF, tumor necrosis factor.
Amelioration in pain symptoms started after the first week (8–10 day) after RPT. Pain “flare” phenomenon, expressed as a transient worsening of pain, occurred in 11% of the cases (7/63 patients): 4 patients treated with 186Re-HEDP, 2 with 89SrCl2, and 1 with 153Sm-EDTMP expressed a “flare” reaction, successfully controlled with mild analgesics. The overall treatment results in the 6-week follow-up period are presented in Table 4. No significant differences were evident among the three groups considering global response and the degree of response to RPT.
RPT outcome in the 6 weeks follow-up period for each radiopharmaceutical used. Pain score decrease more than two classes was considered as complete and one or two classes as partial response on the basis of Wisconsin test. 18
Not only the overall response to RPT, but also the response rate, expressed as pre- and post-therapy WS difference, showed a significant positive correlation with KS pretherapy (R:0.46 p<0.05) and a negative one with pretherapy ScS (R:0.59 p<0.05) and IL-6 levels (R:0.51 p<0.01). No other pretherapy variable showed any correlation with response to RPT.
A clear statistical difference in TNF-a, IL-2, and IL-6 serum levels was noticed between controls and patients. TNF-a and IL-6 levels were lower, while IL-2 levels were higher respectively in control group compared with patients. After RPT a statistically significant difference in TNF-a, IL-6, and IL-2 levels was found between responders and nonresponders. This difference was not evident before therapy, neither for TNF-a, nor for IL-2 (Table 5).
Statistically significant difference between controls and patients.
Statistically significant difference before and after therapy.
Statistically significant difference between responders and nonresponders.
IL-6 levels after treatment in the responders group were maintained or decreased (12.43±5.3 pg/mL) compared to pretreatment, while levels of IL-6 in the nonresponders group increased (37.99±15.86 pg/mL). This statistically significant difference between responders and nonresponders after radionuclide analgesia (p<0.01) was also noticed even before therapy (Table 5). The pretreatment level of IL-6 in responders (16.51±7.5 pg/mL) was significantly lower than in nonresponders (29.56±13.08 pg/mL, p<0.01), regardless of the radiopharmaceutical used (Fig. 1).
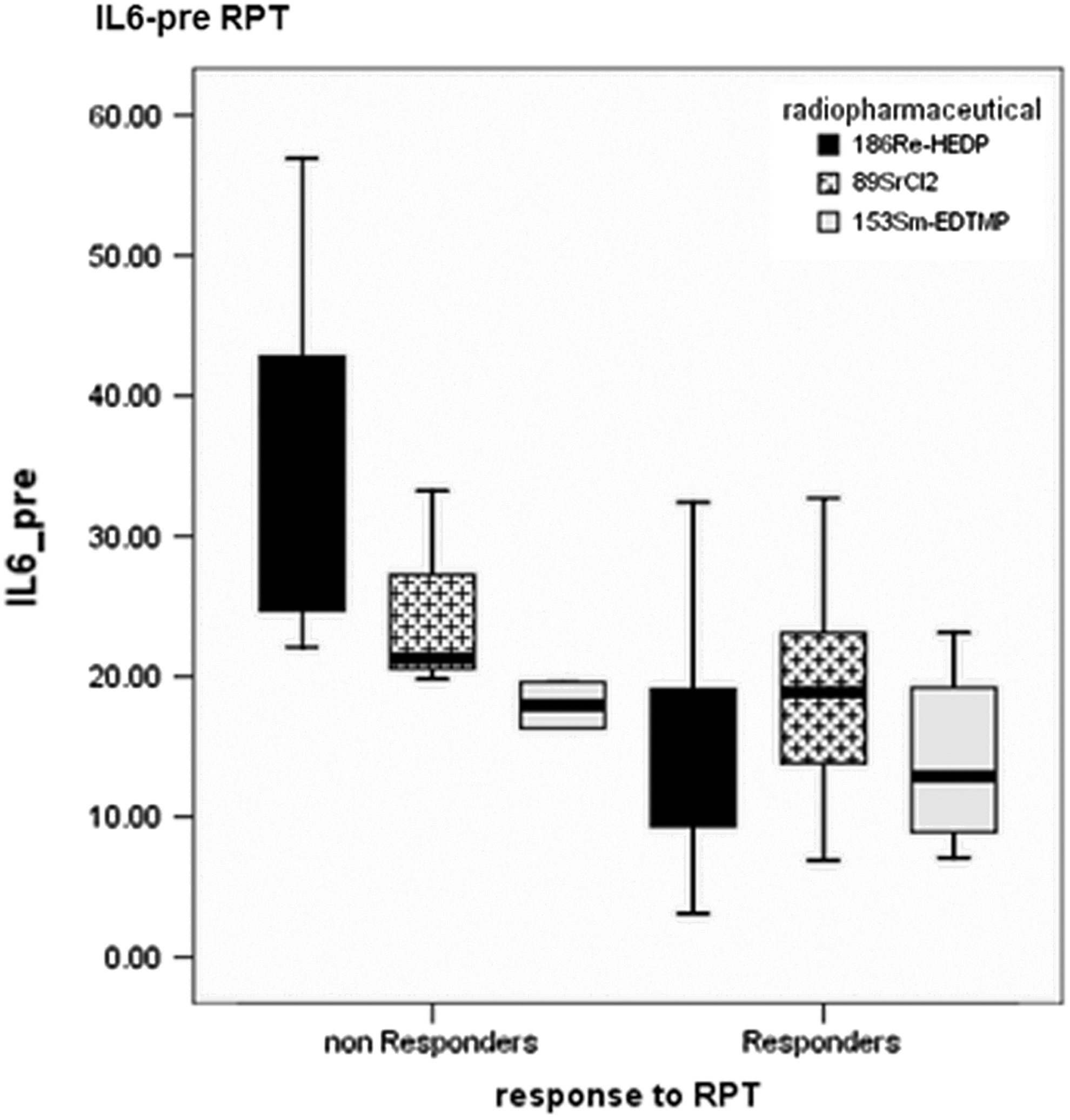
Boxplot of interleukin (IL)-6 pretherapy levels in all patients according to radiopharmaceutical administered and radionuclide palliative therapy (RPT) outcome. The pretreatment level of IL-6 of patients with complete or partial response was significantly lower than that of nonresponders, regardless the radiopharmaceutical used (p<0.01).
Among pre-RPT cytokines, only IL-6 pretherapy levels were significantly negatively correlated with pretherapy KS (R:0.51 p<0.01), BrCa cells hormone receptor status (R:0.31 p<0.05) and positively with pretherapy ScS (R:0.64 p<0.05) and the existence of visceral metastatic disease (R:0.35 p<0.05). Using multivariate regression analysis (stepwise method) with IL-6, ScS, and KS pretherapy values as “predictor variables” of global response to RPT, only pretherapy IL-6 was included in the model with R2:0.3 and p<0.001.
The ROC analysis of IL-2% rise and TNF-a% decrease after RPT, set a cutoff of 10% increase and 22% reduction respectively (AUC 0.91 p<0.01 for IL-2, AUC 0.92 p<0.01 for TNF-a). The sensitivity and specificity of these serum markers in describing the result of radionuclide therapy were assessed (Table 6). The ROC analysis of the pretherapy IL-6 levels provided a threshold of 19.4 pg/mL (criterion corresponding to the higher Youden index) for optimal pretreatment discrimination between radionuclide analgesia responders and nonresponders (AUC 0.825) (Fig. 2).
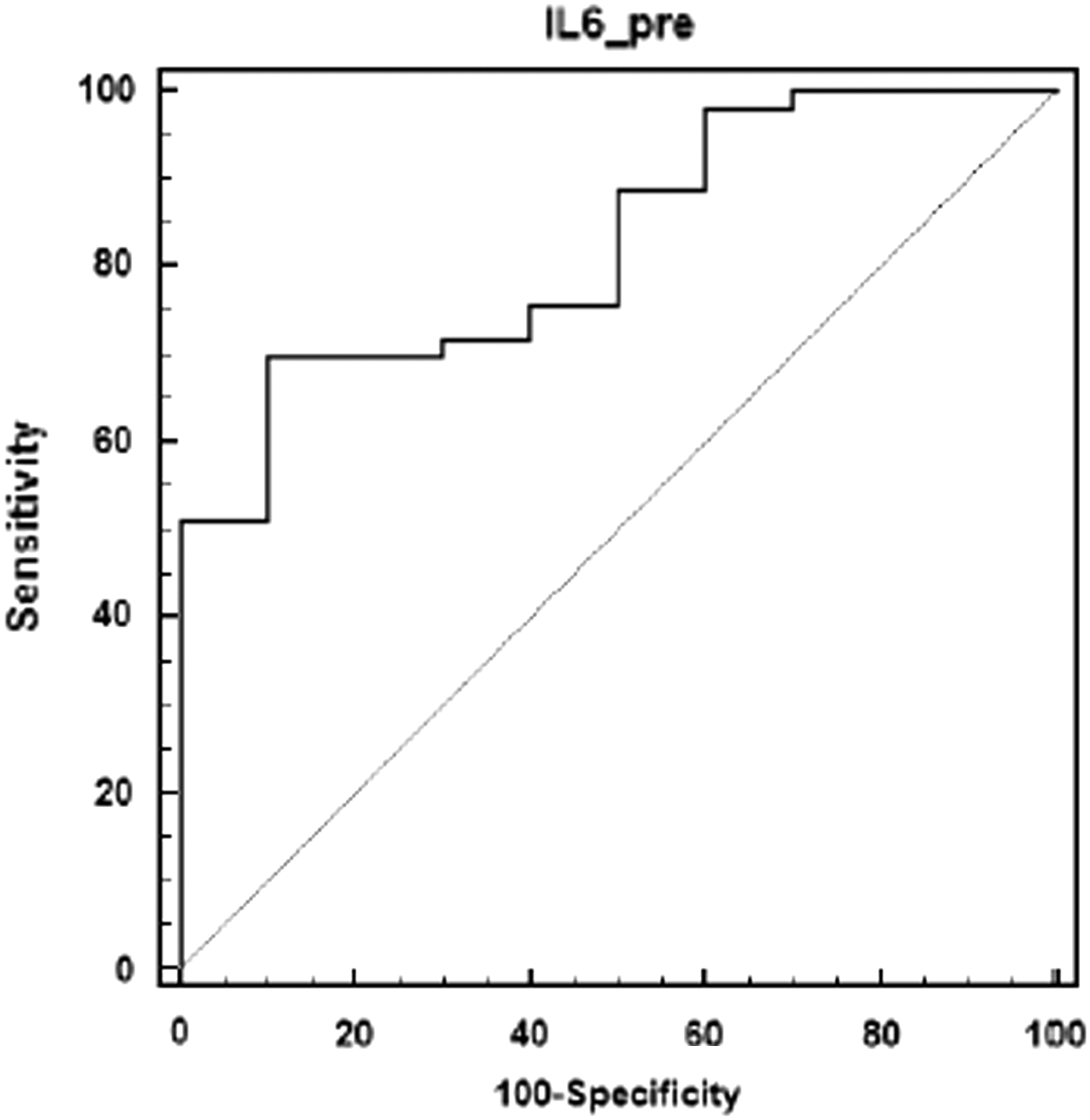
Receiver operating characteristic analysis of pretherapy IL-6 levels; area under curve is 0.825.
No acute adverse reactions were seen in patients treated either with 89SrCl2 or 153Sm-EDTMP. Only one patient treated with 186Re-HEDP reported some “flushing” during administration. Moderate hematological toxicity was apparent in 11/63 patients; grade I in 10 patients with a mild platelet toxicity (5/30 patients treated with 186Re-HEDP, 4/21 with 89SrCl2, and 1/12 with 153Sm-EDTMP) and grade II, concerning leukocytes, in just one patient (having a “superscan” scintigraphic pattern, treated with 89Sr). A transient decrease in white blood cell count was found (mean decrease was 11%±3%) in the rest of the patients, with no toxicity according to the CTC criteria. This phenomenon peaked during the fourth week after therapy. Peripheral blood counts returned to normal during the following weeks. No patient showed neurological signs from nerve compression. No significant differences were noticed in mean decrease of white blood cells and platelets among different radiopharmaceutical groups.
Discussion
Osseous painful metastases are a major complication of BrCa, constituting the most frequent etiology of pain in cancer patients. It is a distinct type of pain, dull and of low intensity initially, progressing to a chronic state, with intermittent severe acute episodes. 16 Stimulating factors released by tumor cells, tumor-induced cytokines, direct nerve injury, and bone matrix infiltration by tumor-causing osteolysis have all been proposed as mechanisms generating skeletal pain. It is significantly related to poor quality of life, thus its control is of paramount importance. Various nonradiotherapeutic modalities such as analgesics, hormone therapy, cytostatic and cytotoxic drugs, biphosphonates, and surgery are proven not to be effective in all cases, especially in the late stage of the disease. 17 Generally, the bone pain exacerbates at the end, despite the high dose of analgesics and it is often difficult to treat without serious side effects. External-beam radiotherapy is suitable for localized bone metastases. Extended field radiation may be useful in patients with diffuse metastases, but is accompanied by severe toxicity. 16 In most cases, multiple painful lesions need an immediate and effective therapy. In selected patients, radionuclide therapy can also be used as a systemic treatment for bone pain palliation and a synergistic antitumor effect can be expected by the combination with chemotherapy or bisphosphonates. 18
The mechanism of bone palliation by ionizing radiation is poorly understood. Radionuclides exert their action mainly on cells in the vicinity of the peripheral nerve cells (unlike opioids that act on central nervous system) where inflammatory, immune, and malignant cells accumulate and release chemical pain modulators that lower pain threshold or promote pain transmission. 19 Reduction of cytokines and growth factors produced at the interface between tumor and normal bone and radiation-induced mechanical factors, such as reduction of periosteal swelling, are among the RPT's mechanisms of action. 19
Although the β-emitting radioisotopes used in RPT significantly differ in their physical properties, they seem to have the same pain palliation effect. During the last two decades, many studies confirmed their effectiveness (Table 7). Sciuto et al. describe a pain relief in women with BrCa reaching 84% for 89SrCl2 and 92% for 186Re-HEDP, 14 while the mean pain palliation rate after a single treatment with 153Sm-EDTMP is about 80%. 18 In other reports, the response rate ranged from 60% to 96% for 89SrCl2, from 55% to almost 90% for 186Re-HEDP, and 60% to more than 80% for 153Sm-EDTMP. 20 –31 In our study 186Re-HEDP, 89SrCl2, and 153Sm-EDTMP showed similar results, being in agreement with Liepe et al. 32
The value of early treatment is well recognized. Most of the researchers conclude that using RPT merely as a last maneuver should be avoided. Although patients with extensive MBD may report dramatic pain relief, the quality of response is better in patients with a moderate skeletal tumor burden. 6 In many studies no correlation between overall response and any pretherapy variable associated with tumor burden is presented. 20 Nevertheless, some predictive factors have been described, including limited skeletal involvement, higher performance status, and predominantly osteoblastic MBD. 18 Similarly, in our study a positive correlation between the response rate and the pretherapy KS and ScS was noticed. Likewise, Shmeler et al. 33 proposed that patients with low pretherapy KS are not the suitable candidates for RPT, presenting a limited response rate, a short period of pain palliation, and high myelotoxicity risk.
Variations in response rates reported by other studies using all three radiopharmaceuticals and discrepancy in correlation between response/response rates and pretherapy variables, are likely due to the heterogeneity of populations treated, different criteria used for pain evaluation or, less likely, in the activities of radiopharmaceutical administered.
Cytokines are known to have both tumor-promoting and inhibitory effects on BrCa growth, presumably depending on their relative concentrations and the presence of other modulating factors. Different cytokines play an important role in controlling the immune system. IL-2 and TNF-a are cytokines released from T-helper lymphocytes and mononuclear macrophages respectively, influencing the antitumor immune responses. 34 It has been reported that IL-2 secretion correlates with long-term survival, 35 while its pretreatment serum levels proved to be an independent prognostic factor in patients with advanced non–small cell lung cancer. 36
TNF-a's role is not absolutely clear, being actually a paradox; although appropriate concentrations of TNF-a in serum increase immunologic response and inhibit the development of tumors, high levels of TNF-a can promote tumor aggressiveness and metastatic potential. 37,38
Fang et al. investigated the correlation between serum IL-2 and TNF-a levels and the response to 89SrCl2 therapy in patients with painful MBD. Serum IL-2 and TNF-a levels correlated well with the number of bone lesions and pain score. Differences between pre- and post-therapy levels of IL-2 and TNF-a were significant in responders, but not in nonresponders. In responders, these variables did not differ before 89SrCl2 therapy, but after therapy they showed a significant difference. 9
Similarly, in our study there was no difference in IL-2 and TNF-a levels before therapy among responders and nonresponders. This difference reached statistical significance only post-therapy and solely at the responders' group, demonstrating that after-therapy concentrations of IL-2 and TNF-a can serve as a useful indicator for response to therapy. Using the serum titles of IL-2 and TNF-a, in an attempt to accurately describe the result of palliative radionuclide therapy, we used the 22% decrease in TNF-a and 10% rise in IL-2 levels (compared to the pretreatment titles, provided by ROC analysis) as a cut-off point. A PPV and NPV of 0.96/0.69 for TNF-a and 0.98/0.75 for IL-2 were respectively demonstrated.
IL-6 is a pleiotropic cytokine with tumor-promoting and tumor-inhibitory effects. In vitro studies have shown that exposure of a preosteoblast MC3T3-E1 cell line to 89SrCl2 produced an increase in prostaglandin-E2 production and enhanced production of IL-6, having a direct positive effect on bone biology, which may partially explain the palliative effectiveness of bone-seeking radiopharmaceuticals. 39 Results regarding its effect on breast tumor cells and on breast tumor tissues are controversial, indicating both tumor-promoting and inhibitory effects of IL-6. 40,41 On the contrary, concerning patients' serum IL-6 levels, data are surprisingly converging, showing IL-6 to be a negative prognostic indicator for BrCa patients. Salgado et al. suggested that at advanced stages of BrC, IL-6 may have a stimulatory effect on tumor growth. 42 Yokoe et al. showed that IL-6 levels at the beginning of therapy can serve as a predictive indicator for treatment response in patients with recurrent BrCa; the pretreatment IL-6 levels in the stable/partial response group was significantly lower (11.0±2.1 pg/mL) than that in the progressive disease group (15.3±2.7 pg/mL). 11
In concordance to Fang et al., 9 in our study there was a statistically significant difference in IL-6 levels, between responders and nonresponders (12.43±5.3 pg/mL vs. 37.99±15.86 pg/mL respectively) (p<0.01). Interestingly, this difference was noticed even before therapy. The pretreatment levels of IL-6 in responders (16.51±7.5 pg/mL) was significantly lower than in nonresponders (29.56±13.08 pg/mL, p<0.01), regardless of the radionuclide injected. Using the threshold of 19.4 pg/mL provided from the ROC analysis, pretherapy IL-6 levels can predict the response to RPT with a sensitivity and specificity of 70% and 90%, respectively.
Pretreatment IL-6 levels, significantly correlated negatively with pretherapy KS, the existence of hormone receptors in BrCa cells and positively with pretherapy ScS and the presence of visceral metastases, are in fact a surrogate of the extent of the disease. Since high tumor burden, low KS, and absence of hormone receptors enhance the likelihood of a poor response to therapy, the prognostic character of pretreatment IL-6 levels for RPT outcome may be explained. 16,33
Bone marrow toxicity was mild in all groups, with no significant differences among them. A grade II hematological toxicity, concerning leukocytes, was apparent in only one (1/63) patient after 89SrCl2 administration, who was multi chemo/radio-treated, with high tumor burden, visceral metastatic disease, and a “superscan” scintigraphic pattern. Diffuse bone marrow involvement presented as a superscan, or an increased uptake in the proximal long bones in the bone scan indicate extensive marrow replacement by tumor and are associated with unfavorable prognosis. Bone imaging predicts myelotoxicity more reliably than bone marrow scintigraphy. 19
Study Limitations
The relatively small number of the patients involved and the nonrandomized character of the project are the main limitations, affecting statistical analysis for comparisons among the three groups. Nevertheless, statistics to serve prognostic role of pretreatment cytokines levels were performed to the total of patients, irrespective of the radiopharmacheutical used, providing a significant conclusion.
Conclusions
Bone-seeking radiopharmaceuticals play an important role in the treatment of pain caused by multiple blastic or mixed-type skeletal lesions of BrCa. 89SrCl2, 186Re-HEDP, and 153Sm-EDTMP have the same therapeutic effect in controlling MBD pain in BrCa patients combining a favorable toxicity profile and a high rate of overall clinical response, reaching the 84% of the cases. Additionally, assessing pretreatment IL-6 levels seems to prognose the therapeutic outcome while IL-2 and TNF-a serum levels changes pre- and post-treatment can only serve as markers of the radioanalgetic treatment response. Further research is necessary to elucidate the role of cytokines in BrCa osseous disease. Results should be interpreted with caution since the use of serum IL-6 levels for RPT response prediction in a clinical setting is limited not only by the partial understanding of mechanisms by which IL-6 specifically mediates the progression of metastatic disease but also by the lack of large clinical trials assessing both the baseline levels and the range of fluctuation of serum IL-6 levels in the frame of RPT for BrCa osseous metastases.
Footnotes
Disclosure Statement
No competing financial interests exist.