
Abstract
Sorafenib has improved the median overall survival of unresectable or otherwise untreatable hepatocellular carcinoma (HCC) of ∼3 months, compared to supportive cares. Complete response, although rare, has been reported. The authors reported herein a case of complete biochemical and radiological remission of advanced unresectable HCC with lymph node metastasis and tumoral portal vein thrombosis treated by 5 months therapy with sorafenib followed by adjuvant Yttrium-90 radioembolization. At 12 months follow-up, there is no evidence of HCC recurrence.
Introduction
Advanced hepatocellular carcinoma (HCC), according to The Barcelona-Clinic Liver Cancer (BCLC) classification, is diagnosed when macrovascular tumor invasion is evident, independently to the hepatic parenchymal distribution. 1,2 It accounts for 10%–40% of cases at diagnosis. 3 Although portal vein tumor thrombosis (PVTT) is no longer considered an absolute contraindication for hepatic resection, the majority of cases are not suitable for surgical treatment. 1,4,5 Moreover, macrovascular invasion still represents a contraindication for orthotopic liver transplantation (OLTx) and also for transarterial chemioembolization (TACE). 1,5
Sorafenib is a multikinase inhibitor, which targets RAF kinase, vascular endothelial growth factor (VEGF), platelet-derived growth factor (PDGF), Fms-like tyrosine kinase 3 (Flt-3), and c-Kit. 6 –8 Since HCC shows a marked hypervascular pattern with overexpression of VEGF, sorafenib blocks tumor cell proliferation and angiogenesis and represents actually the new standard of treatment for advanced otherwise untreatable HCC. 7,8 It is administered orally at a standard dose of 400 mg b.i.d. Reported side-effects are constitutional toxicity (fatigue, fever, chills, anorexia, immunodepression, weight loss), dermatologic (palmar–plantar erythrodysesthesia syndrome, stomatitis, dermatitis, rash), cardiovascular (hypertension, myocardic ischemia, QT prolongation), gastrointestinal (abdominal pain, nausea, vomiting, diarrhea, gastrointestinal perforation, hematochezia, pancreatitis), hepatic (drug-induced hepatitis), renal (failure), and lung toxicity (pneumonitis, pulmonary fibrosis, cough, dyspnea). 9,10 The duration of therapy has not been standardized yet, although it is frequently discontinued because of the occurrence of side-effects. 7 Adjuvant treatments are advocated in these cases, particularly for those who show clinical response to treatment. 4,5
It has been hypothesized that a possible synergic effect between sorafenib and radioembolization as the antiangiogenic agent creates a “vascular normalization window,” which increases the sensitivity to radiation and enhances radiation-induced tumor regression. 11,12
Yttrium-90 microspheres radioembolization is a selective internal radiation therapy for advanced HCC, based on the arterial hypervascularization associated with PVTT and the radiosensitivity of the tumor. 2,3,5,13,14 Radiolabeled particles delivered through selective catheterization of the hepatic artery become trapped at the precapillary level where they emit high-energy beta-rays with short half-life (2.67 days) and short tissue penetration (mean 2.5 mm, maximum 11 mm). 2,14,15 Postradiation syndrome (fatigue, nausea, vomiting, anorexia, fever, and abdominal pain) has an incidence of 20%–55%, and the degree of symptoms is reported to be less severe than the postembolization syndrome observed after TACE. 2,14 Clinical absolute contraindications are decompensated cirrhosis (Child-Pugh score >8, jaundice with bilirubin level >2.5, encephalopathy, refractory ascites, or hepatorenal syndrome), massive tumor with both lobes involved (tumor burden >75% of liver parenchyma). 13
The authors reported herein a case of complete biochemical and radiological remission of advanced unresectable HCC with lymph node metastasis and tumoral portal vein thrombosis treated by 5 months therapy with sorafenib followed by adjuvant Yttrium-90 radioembolization.
Case Presentation
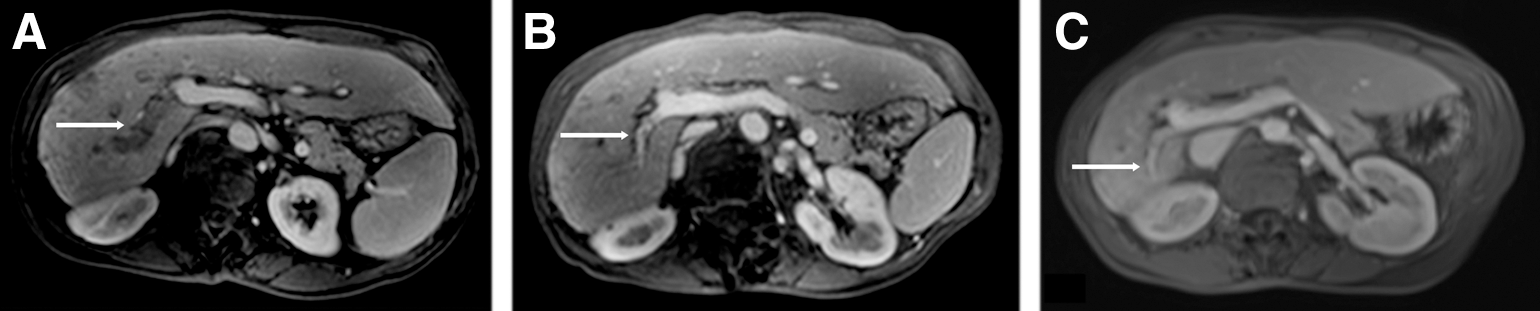
A 49-year-old Caucasian female was referred to this structure with a diagnosis of advanced HCC on HCV-related cirrhosis. On clinical surveillance, an exponential increase up to 2900 ng/mL of serum dosage of alfafetoprotein levels was detected. Therefore, a magnetic resonance imaging (MRI) scan was performed showing the presence of multifocal bilobar lesions with a vascular feature compatible with infiltrative HCC (Fig. 1A). The largest lesion had a diameter of 9 cm and completely subverted the right hepatic lobe, while other two nodules were located in the II and IV liver segment, respectively. In addition, a metastatic lymphadenopathy located at the ilar, celiac, and interaortocaval stations and a PVTT extended up to the posterior right branches were also evident (Fig. 2A). The thoracic computed tomography (CT) scan was negative for lung metastasis. The HCC was classified as BCLC stage C. The patient was in overall good clinical condition, without signs of encephalopathy or ascites; liver cirrhosis was well compensated and was classified as Child-Pugh class A. Upper endoscopy showed mild esophageal varices (F1).

Magnetic resonance imaging (MRI) showing the hepatocellular carcinoma (HCC) at the diagnosis
MRI showing the portal vein tumor thrombosis (PVTT) at the diagnosis
Surgery was not indicated due to the extent of the portal tumor thrombosis and insufficient liver remnant. Thereafter, chemotherapy with sorafenib was planned at a standard dose of 400 mg b.i.d. After 2 months, the CT scan demonstrated a moderate shrinkage of the major lesion in the right hepatic lobe with nearly complete loss of the hypervascular pattern, the persistence of PVTT but without signs of arterial hypervascularization, and a reduction of the lymphadenopathies both in terms of dimension and distribution. Seriated serum dosage of alfafetoprotein level demonstrated a rapid decreasing trend to normalization (Fig. 3).
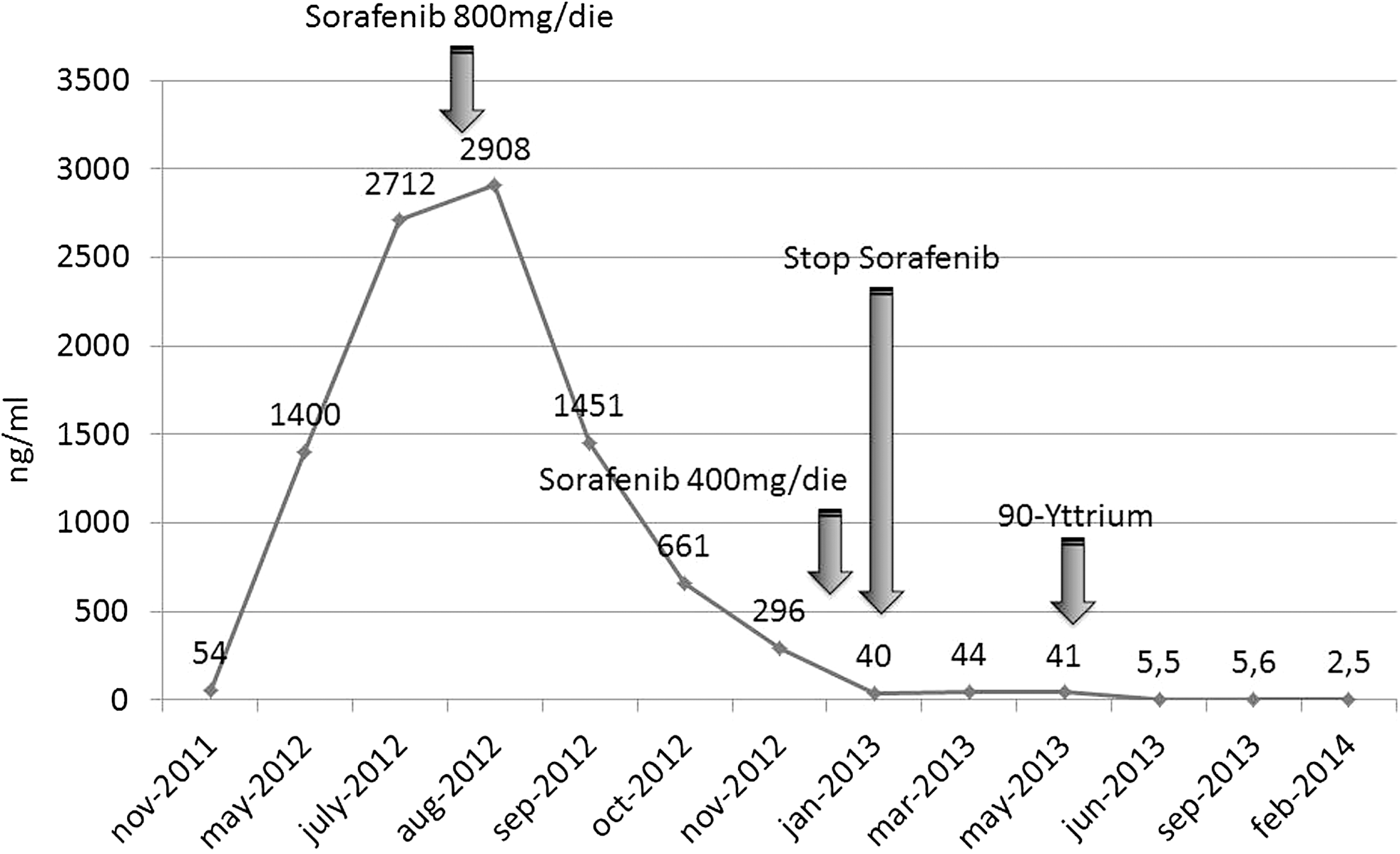
Effect of sorafenib therapy and 90Y radioembolization on the serum level of alfafetoprotein.
A full standard dosage of sorafenib was well tolerated with just mild asthenia for 5 months. Thereafter, peripheral paresthesia, hyperkeratosis of hands and feet, perithrocanteric ischemic lesions, and a dermatitis of ears and face, all resistant to topical dermatologic treatments, developed. Sorafenib dosage was reduced to 200 mg b.i.d., but the worsening of the aforementioned side-effects required treatment discontinuation 1 month later.
An MRI scan re-evaluation showed a partial regression of the HCC with persistence of the lesion just in the posterior segments of the liver, where the macrovascular invasion was still evident while the main right branch was nearly completely recanalized (Figs. 1B and 2B).
Therefore, due to the good response after sorafenib treatment, the case was discussed by the multidisciplinary oncologic group and addressed to selective internal radiation therapy with Yttrium-90. A 99mTechnecium macroaggregated albumin SPECT scan was performed to calculate the lung shunt, which resulted to be less than 10%. In addition, an elective capitation of the radioactive tracer in the posterior segments of the right hepatic lobe was registered. The prescribed activity of microspheres to be delivered was calculated using the body surface area (BSA) method, which incorporates BSA, liver lobe volume, and the percent of tumor involvement of the lobe into the dose calculation. 5 Radioembolization of the whole right hepatic lobe was performed without complication with a total activity delivered of 2 GBq. Just mild anorexia and abdominal pain (responsive to nonsteroidal anti-inflammatory drugs therapy) occurred after the procedure, but without clinical or laboratory signs of liver function deterioration.
Ten months after the first sorafenib dose and 1 month after the radioembolization, the alfafetoprotein serum level was completely normalized. MRI control 1 month after the radioembolization showed complete remission of the hepatocarcinoma with compensatory left lobe hypertrophy and partial recanalization of the portal vein. Residual right branch portal thrombosis without signs of arterial hypervascularization was thus treated with low molecular weight heparin (subcutaneous Enoxaparin 4000 UI b.i.d.) and disappeared at color ultrasonography control 2 months later. After 12 months from the radioembolization, the patient is in good clinical conditions, the liver cirrhosis is well compensated, the alfafetoprotein is 2.5, and the MRI has shown the persistence of complete tumor regression with a marked left lobe hypertrophy (Figs. 1C and 2C).
Discussion
The current standard of treatment for advanced unresectable HCC (BCLC stage C) is the antiangiogenic monotherapy with sorafenib. 1,5 Although associated with an improvement of patient survival compared with supportive cares, 7 the prognosis is still poor. 1,5 Complete radiological and biochemical response is possible and histologically verified, but rare. 7,12,16,17 The reported incidence is 0.6%, and the underlying pharmacodynamic mechanism is controversial, considering the extremely wide range of duration and dosage of treatments. 7,8,18 Moreover, drug-related toxicity forces therapy discontinuation in a relevant percentage of cases. 4,13 It occurred in 38% and 15% of patients in the SHARP and in the Asia-Pacific studies, respectively. 19,20 Partial response is obtained in 2%–3.3% of cases and stable disease 54%–71% with median time to progression of 5.5%–2.8% months. To date, it has not been identified as a second-line treatment in case of sorafenib intolerance or tumor progression. 1,5
The 90Y microspheres radioembolization was developed for being targeted specifically to HCC with macrovascular invasion. 3,13,14 Because selective internal radiation therapy is a microembolic procedure causing minimal occlusion of hepatic arteries, it may be safely used in the setting of PVTT, contrary to TACE that shows a greater vaso-occlusive effect, and thus, a high risk of hepatic necrosis. 3,13,21 The technical feasibility of radioembolization with 90Y is not affected by sorafenib therapy. 15 The radiation-induced necrosis produced by 90Y microspheres has been verified by pathologic examination after liver transplantation, 22 and the reported clinical results have shown an overall survival of 10–17 months and disease control rate of 40%–80%, 13 which are comparable or even higher than those of sorafenib treatment. 23,24 Both 90Y and sorafenib have demonstrated a possible downstaging effect. A second step curative intent treatment based on hepatic resection, 16,17,25 TACE plus radiotherapy, 26 or OLTx (after locoregional adjunctive treatment) 27 –30 has been reported, achieving also complete response.
The multicenter phase II study by Chow et al., carried out on 35 cases of inoperable HCC treated with 90Y SIR-sphere (maximum dose 3 GBq) and adjuvant sorafenib therapy (400 mg b.i.d.), with a median follow-up of 34 weeks (10–72 weeks), showed 12% complete regression, 21% partial regression, 47% stable disease, and 21% progressive disease. 31
Rana et al. performed 15 radioembolizations in 10 patients affected by BCLC stage C HCC, who have previously received sorafenib for a median period of therapy of 43 days, reporting a median overall survival and radiographic progression-free survival of 30 and 28 weeks, respectively. 15 With a median follow-up of 16.5 weeks, the disease showed partial regression in 30% of cases, stability in 60%, and progression in 10%. In the same clinical setting, Chaudhury et al. reported a case of complete response, histologically verified after hepatic resection, after a 2-month course of sorafenib plus adjuvant 90Y. 12
In the present case, the initial tumor burden was a contraindication for surgical resection, OLTx, TACE, and radioembolization, but the sorafenib therapy achieved a partial response that allowed 90Y treatment to be safely performed. The discontinuation of antiangiogenic agent was forced by the development of collateral toxic effects, which actually represent a major clinical problem in the management of advanced HCC. The selective internal radiation therapy with its microembolic effect represents a promising therapeutic alternative to sorafenib for HCC with vascular invasion. It is a safe procedure with mild side-effects and promising clinical results. Both treatments worked synergically, achieving the biochemical and radiological complete response of the reported case.
Finally, after the achievement of both a radiological and biochemical complete response to treatment, the question of whether to observe the clinical course or to perform hepatic resection or liver transplantation represents an open controversy to date. From one hand, the histologic examinations of hepatic specimens of lesion completely regressed after either sorafenib or 90Y reported necrosis without viable tumor cells in most cases. From the other hand, the risk of liver failure or worsening of the underlying cirrhosis hampers the hepatic resection. OLTx might be the treatment of choice in those cases, but it might be weighed against the chronic donor's organs shortage and the high-risk of HCC recurrence in case of conservative strategy. In this case, after 12 months of radiologic follow-up negative for recurrence, with normalized alfafetoprotein levels and compensated liver function, the authors decided for a conservative approach.
Conclusion
The chemotherapy with sorafenib and the radioembolization with 90Y may work synergically to achieve even the biochemical and radiological complete response of HCC. In accordance with other studies, it appears feasible, safe, and effective to perform radioembolization even after sorafenib therapy in selected patients, but the correct therapeutic timing of these two therapies needs to be identified to achieve the best tumor response.
Moreover, further studies are needed to standardize the duration and the dosage of the therapy with sorafenib, particularly in case of occurrence of side-effects, and to identify any potential predictive factors of clinical response. Besides, randomized controlled trials (RCTs) investigating the role of 90-Y radioembolization in the management of advanced HCC will clarify its real efficacy in comparison to sorafenib as an alternative or combined treatment. Finally, the question of whether to observe the clinical course or to radicalize the disease (performing a hepatic resection or a liver transplantation), after both the radiological and biochemical complete response, has to be defined by large-scale series and RCTs.
Consent
Written informed consent was obtained from the patient for publication of this Case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Footnotes
Disclosure Statement
No competing financial interests exist.