
Abstract
Background:
Endostar combined with concurrent chemoradiotherapy (CRT) has been used in patients with gastric cancers (GCs). However, there are no reliable markers to predict the treatment response and prognosis of these patients. Apelin and its receptor (APJ) are involved in angiogenesis in tumor tissues. We aimed to study whether Apelin and Apelin receptor (APJ) tumor expression can predict the treatment response of combination therapy of endostar and CRT.
Materials and Methods:
We enrolled patients with locally advanced GC receiving CRT only and CRT+endostar combination therapy. Apelin receptor (APJ) in tumor samples was determined by immunohistological staining and scored by measuring staining area and signal intensity.
Results:
The high APJ expression has significantly higher rates of tumor invasion, local lymph node, and distant metastasis (all p < 0.001). In the CRT only group, the distribution of high and low APJ expression in patients with good and poor treatment response to CRT is not significantly different (p = 0.235). However, in the CRT+endostar group, the chance of having poor response to combined treatment is 3.645-fold higher in those having high APJ expression levels than those who have low APJ expression levels. Our prognostic analysis shows that in the CRT+endostar group, high APJ expression had significantly shorter overall survival (OS) period than those with low APJ expression (p < 0.001). Furthermore, multivariate survival analysis reveals that the APJ expression is an independent predictor for the OS period in GC patients treated with CRT+endostar.
Conclusion:
Tumor APJ can be used to predict the therapy response and prognosis in GC patients receiving CRT+endostar therapy.
Introduction
Gastric cancer (GC) is one of the most common gastrointestinal cancers worldwide. 1 Despite improving surgical and adjuvant treatment approaches, the prognosis of GC patients remains dismal, with 5-year overall survival (OS) less than 25%. 2 –4 Many patients are not eligible for surgical treatment because of late diagnosis. Concurrent chemoradiotherapy (CRT) is the standard treatment for these patients with advanced tumor stage. 5,6 However, the treatment response is low and the prognosis remains poor.
Tumor growth and invasion rely on angiogenesis. Inhibition of tumor angiogenesis has been suggested as a major strategy for cancer therapy. 7 –9 Endostar, a modified recombinant human endostatin, is a novel angiogenesis inhibitor, which inhibits endothelial cell proliferation and angiogenesis. 10 Endostar together with CRT can improve outcome of advanced cervical cancer. 11 As first-line therapy, the combined treatment with endostar and chemotherapy is well tolerated in patients with metastatic colorectal and GCs. 10 Endostar inhibits the vascular endothelial growth factor expression in human GC cell line. 12 So far, there is no reliable marker to predict the treatment response in GC patients receiving endostar treatment.
Apelin is a bioactivated peptide actively involved in the angiogenesis process. 13,14 Being widely expressed in the heart and vasculature, Apelin (APLN) exerts its biological effect through binding to the APLN receptor (APJ). APJ has been taken as a pivotal angiogenic factor in different types of tissues. 15 –18
In this study, we enrolled patients with advanced GC who underwent combined therapy of CRT and endostar. We found that higher APJ expression in cancer tissues is closely associated with the poor treatment response and worse prognosis in these patients, suggesting that tumor APJ expression may be used to predict therapy response of endostar in GC patients receiving CRT.
Materials and Methods
Patient enrollment
We enrolled 122 patients with locally advanced GC between June 2010 and Mar 2015. The diagnosis was histologically established through endoscopic biopsy. None of these patients received surgical treatment. All patients were treated with CRT. The radiation dose was 45 Gy (daily dose 1.8 Gy). The chemotherapy regimen consisted of two or three of the following drug combinations: 5-fluorouracil-based regimens (capecitabine, S-1) leucovorin, platinum (cisplatin, oxaliplatin), taxol (taxotere, docetaxel), and irinotecan. These patients were assigned randomly into two groups: CRT only and CRT+endostar groups. The patients received endostar (rh-endostatin, Shangdong Simcere-Medgenn Bio-Pharmaceutical Co., Ltd., China) at a dose of 15 mg daily from days 1 to 14 every 3 weeks and from days 1 to 7 every 2 weeks when combined with other chemotherapy regimens, respectively. Endostar solved in 500 mL normal saline was administered by intravenous infusion for 4 hours. A written consent was acquired from patients. The Ethical Committee of our hospital approved the protocol according to the ethical guidelines of the 1975 Declaration of Helsinki.
Data collection and treatment response evaluation
The clinicopathological characteristics, such as gender, age, tumor type, number of chemotherapeutic regimens, number of chemotherapeutic cycles, and laboratory markers, were obtained.
To evaluate the treatment response, all patients underwent a radiological and endoscopic examination after CRT. Therapy responsiveness was assessed according to the Response Evaluation Criteria in Solid Tumors criteria. Responses were classified as complete response (CR), partial response (PR), stable disease (SD), and progressive disease (PD). 19,20 All patients were followed after leaving from hospital. OS was defined as the time interval between the date of treatment and death or last follow-up. The last follow-up was done on March 2015, with a range of 3–60 months and median of 25.7 months.
APJ immunohistological staining and scoring
All tumor samples were obtained from biopsy and were formalin fixed and paraffin embedded, placed in a solution of absolute methanol and 0.3% hydrogen peroxide for 30 minutes, and treated with blocking serum for 20 minutes. The slides were incubated overnight with APJ antibody (Abcam) at a 1:200 dilution at 4°. The immune reaction was observed with diaminobenzidine. Sample scoring was performed by semiquantitative microscopic analysis, measuring the staining area and signal intensity. The two mentioned scores were multiplied to categorize APJ expression as low (0–6) and high (>6).
Statistical analysis
The χ2 tests and Fisher's exact tests were performed for comparing the treatment response status between patients with low and high APJ expression. The prognosis was analyzed using the Kaplan–Meier method and compared by using a log-rank test. A p < 0.05 was considered statistically significant. COX hazard model was used to determine prognostic factors. All statistical analyses were performed by using SPSS version 20.0 (IBM Corp., Armonk, NY).
Results
The typical immunohistological staining for APJ is shown in Figure 1. APJ is predominately expressed in the cytoplasm of cancer tissues (Fig. 1a, b). The neighboring noncancerous tissues show low APJ expression (Fig. 1c).
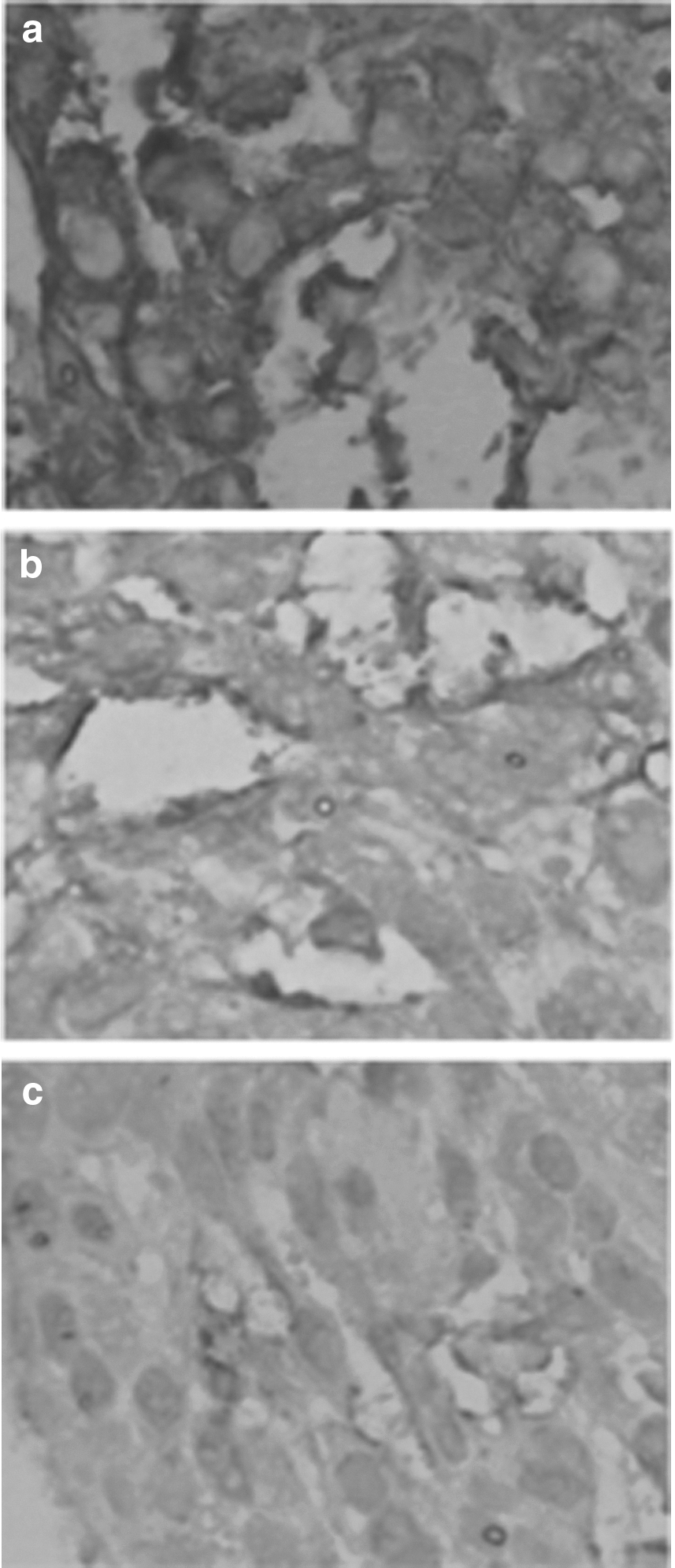
Typical immunohistological staining for APJ.
The clinical data of all patients are listed in Table 1. Based on the APJ expression scores, all patients are subgrouped into high APJ expression (n = 76) and low expression groups (n = 46). The high and low APJ expression groups had similar age and gender distributions. Tumor size is similar between these two groups as well. However, the high APJ expression has significantly higher rates of tumor infiltration, local lymph node (LN), and distant metastasis (all p < 0.001).
NS, no significant difference.
Among all 122 patients, 71 patients had poor treatment response (SD+PD) and 51 (CR+PR) had good treatment response. Based on APJ expression status, all the patients were assigned into high and low APJ expression groups. Globally, the treatment response status was compared using × 2 analyses, as shown in Table 2. These data suggest that, overall, the APJ expression status is unrelated to treatment response in enrolled GC patients (p = 0.276).
Next, we stratified the patients based on the therapy protocol used in this study, namely, CRT group (n = 79) and CRT+endostar group (n = 43). In the CRT only group, the distribution of high and low APJ expression in poor and good treatment groups is not significantly different (p = 0.235, Table 3).
We then analyzed the APJ expression status in the CRT+endostar group (n = 43). In this group, we observed that patients with poor response have a dramatically increased rate of high APJ expression than those with good treatment response. The chance of having poor treatment response is 3.645-fold higher in those having high APJ expressions than those who have low APJ levels (Table 4). To further confirm the association between APJ treatment responses in this group, we performed a multiple variable regression logistic regression analysis, with adjustment of age, gender, tumor location, tumor grade, therapy reagents, endostar, and CRT. Our data reveal that tumor APJ expression level can predict a poor treatment response in this group (adjusted HR = 3.45, 95% CI: 2.13–6.02, p < 0.001).
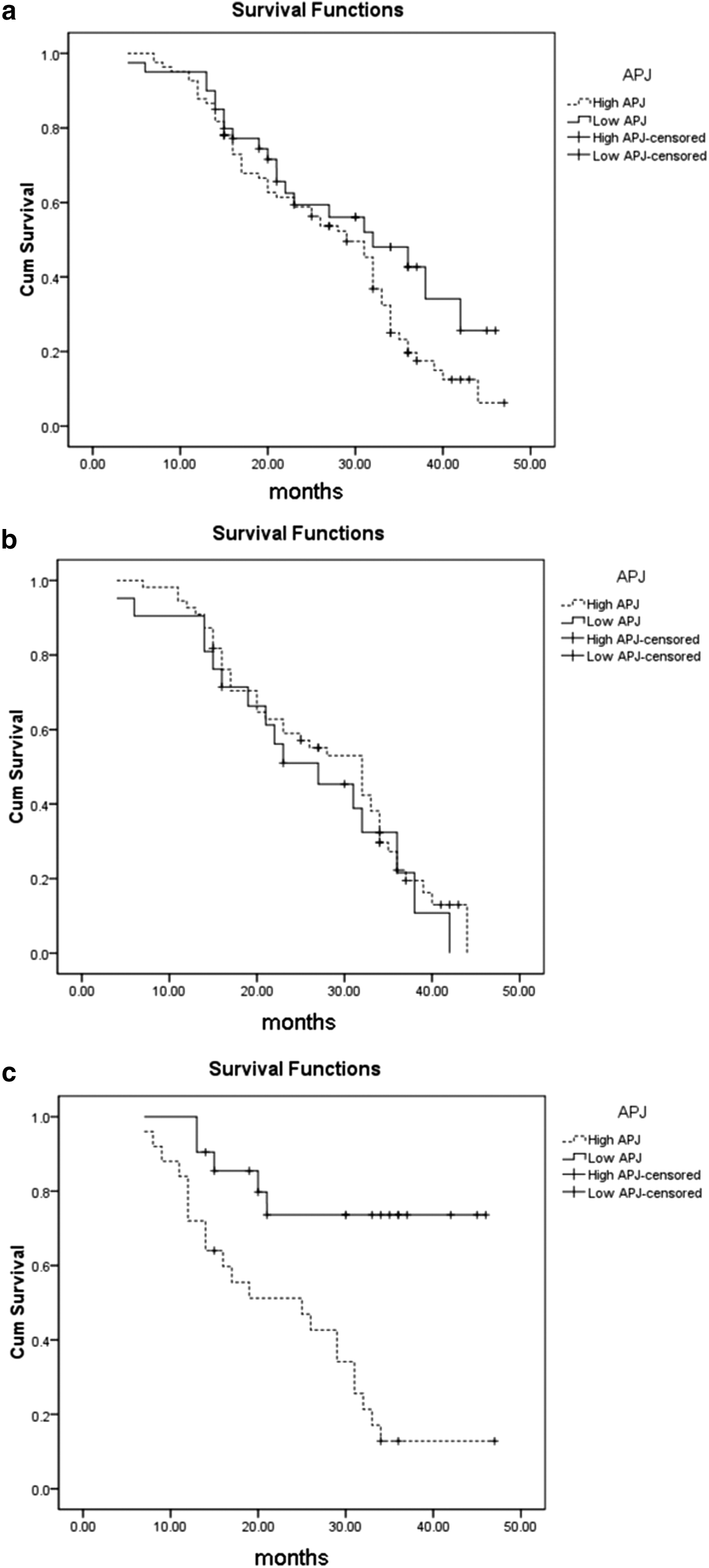
We further analyzed the relation of APJ expression with the OS of GC patients in this study. As shown in Figure 2a, generally, there is no significant difference in the OS period between patients with high and low APJ expression (25.6 ± 3.4 vs. 26.5 ± 4.6, months, p = 0.452). When all patients were subgrouped based on therapy protocol (CRT group and CRT+endostar group), we note that those with high APJ had significantly shorter OS period than those with low APJ expression only in CRT+endostar group (29.2 ± 4.1 vs. 21.5 ± 3.9, months, p < 0.001, Fig. 2c), whereas in the CRT only group, the OS period remains similar between two groups (25.0 ± 4.8 vs. 26.1 ± 6.2, months, p = 0.475, Fig. 2b).
Subsequently, we performed the COX univariate analysis to identify the prognostic significance of tumor APJ expression. In GC patients receiving chemoradiotherapy and Endostar, our data revealed that the OS rates were associated with tumor infiltration (p = 0.023), LN metastasis (p = 0.004), distant metastasis (p = 0.034), and APJ expression (p = 0.002). Thereafter, COX multivariate survival analysis was performed and we found that tumor APJ expression is an independent prognostic factor for the OS rates in patients with GC (p = 0.003, Table 5). However in patients receiving chemoradiotherapy only, none of the clinical characterstics showed prognostic significance in these patients (Table 6).
Discussion
In this study, we enrolled advanced GC patients receiving CRT with or without endostar treatment. We found that tumor APJ expression is not correlated with the treatment response in those who underwent CRT only; however, it is significantly associated with the treatment response in the endostar +CRT-treated patients. This finding suggests that the tissue APJ expression may be used as a biomarker to predict the treatment effect in GC patients receiving CRT and endostar treatment.
Previous studies showed that Apelin/APJ pathway regulates endothelial cell growth, thus playing an important role in angiogenesis process in vitro and in vivo. 21,22 Apelin upregulation was also found in human cancers. 23 –25 Consistent with previous studies, in our study, we found that APJ is associated with tumor distant metastasis. In hepatocellular carcinoma (HCC), more APJ-positive staining arteriole and a higher Apelin expression were observed in poorly differentiated than in well-differentiated HCC.
It should be noted that, in our study, around 50% of patients (23 with low APJ vs. 21 with high APJ) receiving CRT only treatment have a good response, whereas in patients receiving CRT+endostar treatment, only 20% of patients (21 with low APJ vs. 6 with high APJ) have good response. We think that this might be a dose-related effect of endostar in treating patients. It is possible that current endostar dose (or even its formula) works better in patients with relative lower APJ expression, but not potent enough in patients with high APJ expression. As a marker for angiogenesis, higher APJ means higher blood supply to cancer tissue, which may counteract the effect of endostar. However, in those patients with lower tumor blood supply, endostar still works. Another possible reason is sample size. We enrolled only 43 patients in the CRT+endostar group. The sampling bias cannot be excluded. To better address this issue, we are carrying out a clinical trial with larger number of participants to solidify the finding of this study.
Previous animal studies revealed that lymphangiogenesis is associated with LN metastasis. Overexpression of Aplelin confers a growth advantage to tumor grafts, induces intratumoral lymphangiogenesis, and promotes lymphatic metastasis. 26 Apelin increases the number of endothelial cells in vitro and stimulates lymph vessels growth in the Matrigel plug model in vivo. 27,28 In agreement with these previous reports, in our study, we found that patients with high APJ tend to have higher local LN metastasis. However, the role of Apelin/APJ in lymphangiogenesis warrants further study.
Several limitations in this study should be addressed. First, the sample size is relatively small and only Chinese patients were enrolled. Second, the effect of Apelin/APJ pathway on the biological behavior of gastric cell lines was not included in this study, so the molecular mechanism under which APJ affects the clinical outcome of GC progression and prognosis remains unclear.
Footnotes
Disclosure Statement
No competing financial interests exist.