
Abstract
Background:
This study aims to explore the associations of human epidermal growth factor receptor 2 (HER2) and breast cancer susceptibility gene 1 (BRCA1) expression levels with prognosis and radiation sensitivity in patients with breast cancer.
Materials and Methods:
Breast cancer tissues, adjacent normal breast tissues, and benign breast lesions were initially obtained from 256 breast cancer patients as well as an additional 245 patients with breast lesions. Reverse transcriptase–quantitative polymerase chain reaction (RT-qPCR) was conducted to assess the expression of HER2 and BRCA1 in the collected tissues. Immunohistochemistry was performed to examine HER2 and BRCA1-positive expression levels in the tissues. The relationship between HER2 and BRCA1 expression levels and radiation sensitivity as well breast cancer prognosis was assessed by the Spearman correlation analysis and Kaplan–Meier survival analysis.
Results:
Compared with adjacent normal breast tissues and benign breast lesions, the breast cancer tissues exhibited high expression of HER2 mRNA and protein, and low expression of BRCA1 mRNA and protein. Patients with positive HER2 expression had a significantly shorter survival time, and survival time of patients with positive BRCA1 expression was markedly longer, which were consistent with RT-qPCR results. After radiotherapy, the local failure rate of HER2-positive patients was higher than that of the negative ones, while that of BRCA1-positive patients was lower than that of the negative ones.
Conclusions:
This study suggested that breast cancer patients with high HER2 expression and low BRCA1 expression were less sensitive to radiotherapy with poor prognosis in breast cancer.
Introduction
As one of the most commonly occurring malignancies, breast cancer represents a leading cause of death among women worldwide. 1 Breast cancer is a clinically and biologically heterogeneous disease that possesses significant metastatic potential that has been well documented to spread to the bone marrow and regional lymph nodes, as well as the liver and lungs. 2,3 Despite commendable advances in medical technology, particularly in the diagnosis and treatment of breast cancer, the National Cancer Institute reported more than 230,000 cases of breast cancer in females in the year 2014, among which more than 40,000 women succumbed to their disease. 1 Important prognostic factors include age, status of axillary lymph nodes, tumor size, pathological grade, histologic type of the tumor, and hormone receptor status. 4
Both human epidermal growth factor receptor 2 (HER2) and breast cancer susceptibility gene 1 (BRCA1) have been found to be involved in the pathogenesis and prognosis of breast cancer. 5,6 Higher expression levels of HER2 represent a critical predictive marker of the therapeutic effect of targeted therapy as well as overall breast cancer prognosis. 7 HER2 has been shown to be amplified and overexpressed in ∼30% of breast cancer patients in addition to acting as an independent indicator for poor prognosis. 8 As a tumor suppressor protein, BRCA1 possesses the ability to maintain genomic stability through regulating a variety of biological processes, including transcription, cell cycle arrest, and DNA repair. 9 Abnormal BRCA1 function has been reported to result in cell apoptosis, and thus the functional inactivation of BRCA1 is a known contributor to oncogenesis in breast cancer. 10,11
Treatment options generally include surgery, immunotherapy, radiation, and medications, 12 depending on the different characteristics of an individual's breast cancer. The event of secondary resistance such as a gene mutation following endocrine therapy poses a more serious challenge. 13 Therefore, the study aimed to investigate the downregulation of HER2 and upregulation of BRCA1 signaling pathways and their contribution to prognosis and radiotherapy sensitivity in breast cancer.
Materials and Methods
Ethics statement
All participants in the current study signed written informed consent documentation, and the current study was approved by the Ethics Committee of the First Hospital of China Medical University.
Study subjects
The data of 256 patients with breast cancer, who underwent surgery between May 2008 and May 2016 at the Department of Obstetrics and Gynecology in the First Hospital of China Medical University, were collected. Patients with a mean age of 46.9 ± 6.3 years (ranging from 35 to 63 years), who did not receive any previous radiotherapy, chemotherapy, or hormone therapy, and had no form of acute/chronic diseases, Lynch syndrome, or other malignant tumors were recruited for the study. As per the eighth edition of TNM staging by AJCC, 14 there were 66 stage I cases, 102 stage IIa cases, 47 stage IIb cases, and 41 stage III cases.
These patients received modified radical mastectomy and radiotherapy (according to the thickness of the chest wall, conventional or three-dimensional conformal radiotherapy was used; 50 Gy every 5 weeks; the range of radiotherapy was the chest wall field and supraclavicular and infraclavicular fields, and the irradiation scheme was 2.0 Gy/f × 25 f, 5 f/W) and postoperative adjuvant chemotherapy (CAF regimen: doxorubicin 50 mg/m2 was intravenously injected on the first day, cyclophosphamide 500 mg/m2 was intravenously administered on the first day, and 500 mg/m2 fluorouracil was given intravenously on the first and eighth day, 21 d as a cycle). After radiotherapy, psychological nursing was carried out.
The patients' mental state, skin reaction after radiation, gastrointestinal reactions such as nausea, vomiting, and anorexia, and respiratory symptoms such as cough and shortness of breath were observed and recorded. Additional 245 female patients (with a mean age of 46.0 ± 5.5 years, ranging from 32 to 58 years) served as the control. Although their lesions were suspected to be cancerous, the results of the pathological examinations were determined to be either fibromas or benign breast lesions. No significant difference was detected in regard to age and the general information between patients with breast cancer and benign breast lesions (all p > 0.05).
Specimen processing
After the surgery, a portion of the samples of breast cancer tissues, adjacent normal breast tissues (2 cm away from the lesions of breast cancer), and benign breast lesions was washed with normal saline and promptly preserved in liquid nitrogen in preparation for subsequent RNA extraction. Another portion of samples was fixed in the neutral buffered formalin for 24 h and preserved by paraffin embedding.
Reverse transcriptase–quantitative polymerase chain reaction
Tissues were collected from the liquid nitrogen and ground into powder. The total RNA of cells was extracted using the TRIzol method, with RNA concentration and purity subsequently determined. RNA was then reverse transcribed into cDNA, with the transcribed cDNA thoroughly diluted in 65 μL of diethyl pyrocarbonate water and amplified in a system of 5 μL of Sso Fast EvaGreen Supermix (2 × ), 0.5 μL of forward primer (10 μM), 0.5 μL of reverse primer (10 μM), and 4 μL of cDNA.
The polymerase chain reaction (PCR) amplification conditions were performed as follows: predenaturation at 95°C for 4 min, denaturation at 95°C for 30 s, annealing at 58°C for 5 s, and extension at 72°C for 5 s, completing 30 cycles. The reverse transcriptase–quantitative polymerase chain reaction (RT-qPCR) primers were synthesized by the Beijing Genomics Institute Co., Ltd., (Table 1). HER2 and BRCA1 gene expression levels relative to the internal reference glyceraldehyde phosphate dehydrogenase were calculated and statistically analyzed.
Primer Sequences for Reverse Transcription–Quantitative Polymerase Chain Reaction
BRCA1, breast cancer susceptibility gene 1; HER2, growth factor receptor 2; GAPDH, glyceraldehyde-3-phosphate dehydrogenase.
Immunohistochemistry
The paraffin-embedded samples were sectioned into 4 μm serial sections, incubated at 70°C for ∼15 min, and dehydrated with gradient ethanol. The samples were then incubated with H2O2 to inactivate endogenous enzymes, rinsed three times with phosphate-buffered saline (PBS) buffer (5 min each time), and incubated with normal goat serum for 15 min at room temperature. The samples were subsequently incubated with 20–30 μL of PBS-diluted HER2 (Cell Signaling Technology, Inc.; No. #2165) and BRCA1 (Abcam Plc, Cambridge, United Kingdom; No. ab16780) primary antibodies overnight at 4°C. The primary antibody was then replaced using PBS as the negative control. After incubation, samples were rinsed three times with PBS buffer (5 min each time) and incubated with secondary antibody for 45 min at 37°C. Next, the sections were stained for 5–10 min with diaminobenzidine (Fuzhou Maixin Biotechnology Development Co., Ltd., Fuzhou, China) and thoroughly washed with tap water. The sections were then counterstained with hematoxylin for 5 min, desalinated with dilute hydrochloric acid for 30 s, and washed for 5 min. Sections were then dehydrated, cleared, sealed, and observed under a microscope. Paraffin sections with positive expression of HER2 and BRCA1 proteins were selected as positive controls. Results were diagnosed by two experienced pathologists blindly.
Based on immunohistochemistry results, the membranes of HER2 appear brown and granular, this was considered to be a sign of positive cells. Result estimations were as follows: if the staining area of the tumor cell membranes was <10%, it was marked as “−”; if the staining area of membranes was seen to be ≥10%, staining intensity was mild, and distribution was disjunctive and partly surrounding the membranes, it was marked as “+”; if the staining area of membranes was ≥10%, staining intensity was mild to moderate, and distribution was continuous and completely surrounding the membranes, it was marked as “++”; and if the staining area of membranes was ≥10%, staining intensity was thought to be strong, and distribution continuous and completely surrounding the membranes, it was marked as “+++.”
Positive signals of BRCA1 were yellow, brown, or brownish yellow granules deposited in the nucleus or cytoplasm. Result estimations were as follows: scored according to the percentage of positive cells: <10% was 0 points, 10%–25% was 1 point, 26%–50% was 2 points, and >50% was 3 points. scored according to staining intensity: unstained was 0 points, yellow was 1 point, brownish yellow was 2 points, and brown was 3 points. The sum of two indexes was the final score: 0–1 point was “−,” 2–3 points was “+,” 4–5 points was “++,” and 6 points was “+++.”
15
Evaluation standard
Three months after radiotherapy, if the tumor or parts of it still existed, or any sort of new lesions appeared in the breast, it was regarded as an uncontrolled case. The local failure control symptoms of breast cancer were diagnosed based on computed tomography and pathological examination. Local failure rate = the number of patients with locally uncontrolled symptoms/total number of patients × 100%.
Follow-up
All clinical and histopathological data, as well as follow-up information of the patients, were collected. Follow-up information was collected through phone calls or through the clinical data collection system, starting from the date of discharge once every 3 months for the first 3 years and once every half a year in 3–5 years. The follow-up ended on the day of death or the final follow-up date. The deadline date of follow-up was May 2019. The recurrence and death of patients were recorded, with the calculated total survival and relapse-free survival rates.
Statistical analysis
All data were analyzed using the two-sided test and the software SPSS 21.0 (IBM Corp., Armonk, NY). Measurement data are expressed as mean ± standard deviation. Comparisons between groups were analyzed by one-way analysis of variance in cases with even variance and by the Wilcoxon rank-sum test in cases of uneven variance (the expression levels of HER2 and BRCA1 mRNA and protein in different breast tissues were detected). Enumeration data are expressed as percentage or rate and analyzed using the χ 2 test (the relationship between the expression of HER2 and BRCA1 and the clinical pathology and radiotherapy effect of breast cancer patients was determined). Correlations were analyzed by Spearman rank correlation analysis (correlation between HER2 and BRCA1 expression in breast cancer). Kaplan–Meier curves were plotted to evaluate the total survival and relapse-free survival rates. The log rank test was applied to compare the survival curves among groups, while the test level was α = 0.05; p < 0.05 was considered to be indicative of statistical significance.
Results
Expression of HER2 and BRCA1 mRNA in adjacent normal breast tissues, benign breast lesions, and breast cancer tissues
The RT-qPCR results revealed that the expression levels of HER2 mRNA were 0.30 ± 0.08, 0.31 ± 0.09, and 0.37 ± 0.09, respectively, among the adjacent normal breast tissues, benign breast lesions, and breast cancer tissues. In addition, there was no significant difference in the HER2 mRNA expression between adjacent normal breast tissues and benign breast lesions (p > 0.05), while the breast cancer tissues exhibited statistically significantly higher expression when compared with the adjacent normal breast tissues and benign breast lesions (p < 0.001) (Fig. 1A). The expression levels of BRCA1 mRNA in adjacent normal breast tissues, benign breast lesions, and breast cancer tissues were 0.28 ± 0.06, 0.27 ± 0.06, and 0.21 ± 0.08, respectively.
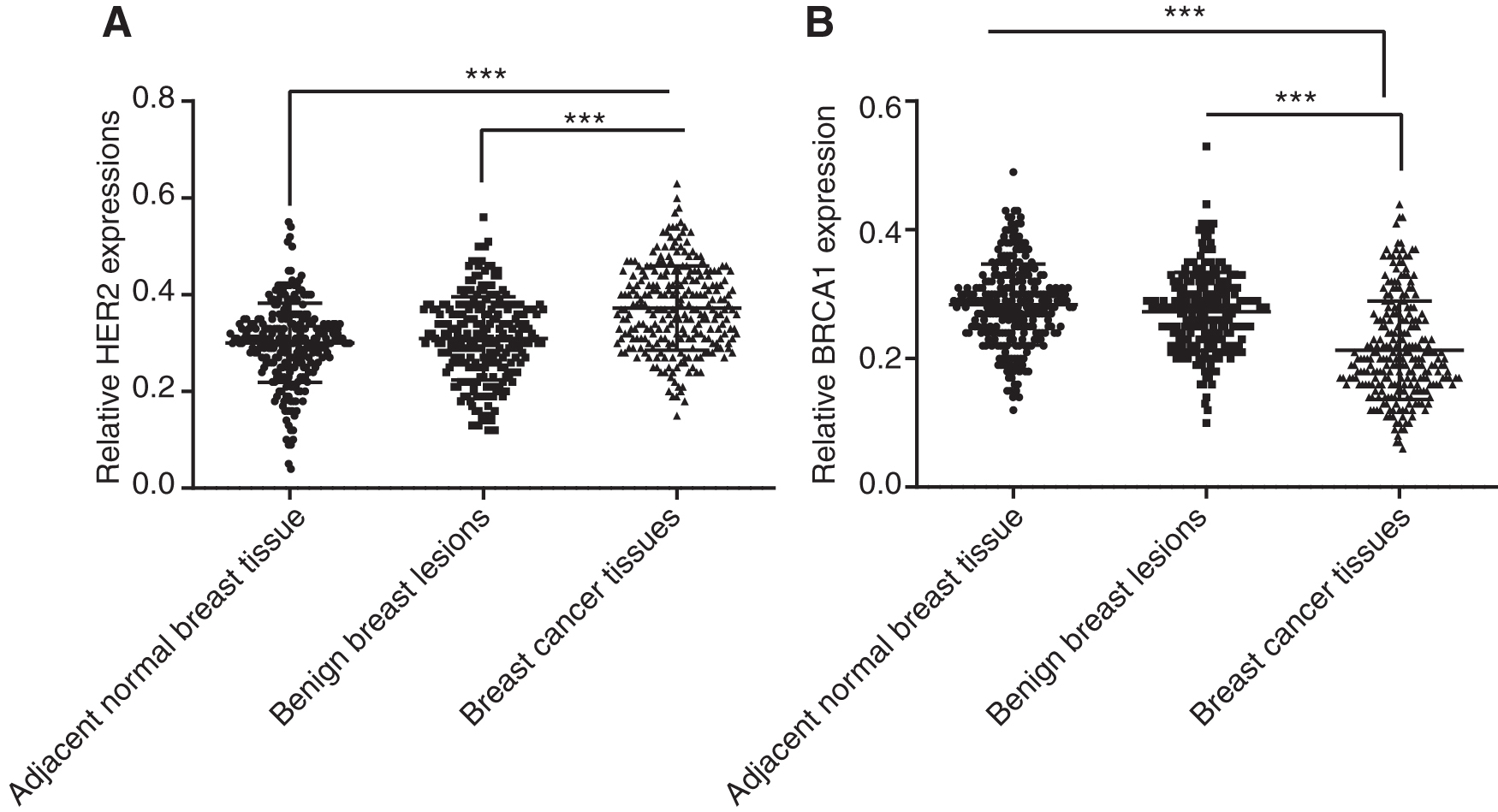
The expression of HER2 and BRCA1 mRNA in breast cancer tissues, benign breast lesions, and adjacent normal breast tissues.
No significant difference was detected in terms of the BRCA1 mRNA expression between the adjacent normal breast tissues and benign breast lesions (p > 0.05), while the breast cancer tissues exhibited considerably lower expression levels when compared with the other two groups (p < 0.001) (Fig. 1B). The aforementioned results provided verification, indicating lower expression of BRCA1 along with higher HER2 expression in breast cancer tissues when compared with the adjacent normal breast tissues and benign breast lesions.
Expression of HER2 and BRCA1 proteins in breast cancer tissues, benign breast lesions, and adjacent normal breast tissues
Immunohistochemistry results revealed that HER2 expression levels in the adjacent normal breast tissues, benign breast lesions, and breast cancer tissues were 12.50%, 17.96%, and 34.77%, respectively, illustrating a positive HER2 expression in breast cancer tissues. The breast cancer tissues displayed a significant difference in terms of higher expression of HER2 when compared with the other two (both p < 0.001) (Fig. 2A). The positive expression levels of BRCA1 in the adjacent normal breast tissues, benign breast lesions, and breast cancer tissues were 62.89%, 54.69%, and 32.03%, respectively, exhibiting a downward tendency. The breast cancer tissues had a significant difference in the higher expression of BRCA1 compared with the other two (p < 0.001) (Fig. 2B). There was no significant difference detected between the adjacent normal breast tissues and benign breast lesions in both positive expression levels of the genes HER2 and BRCA1 (p = 0.062).
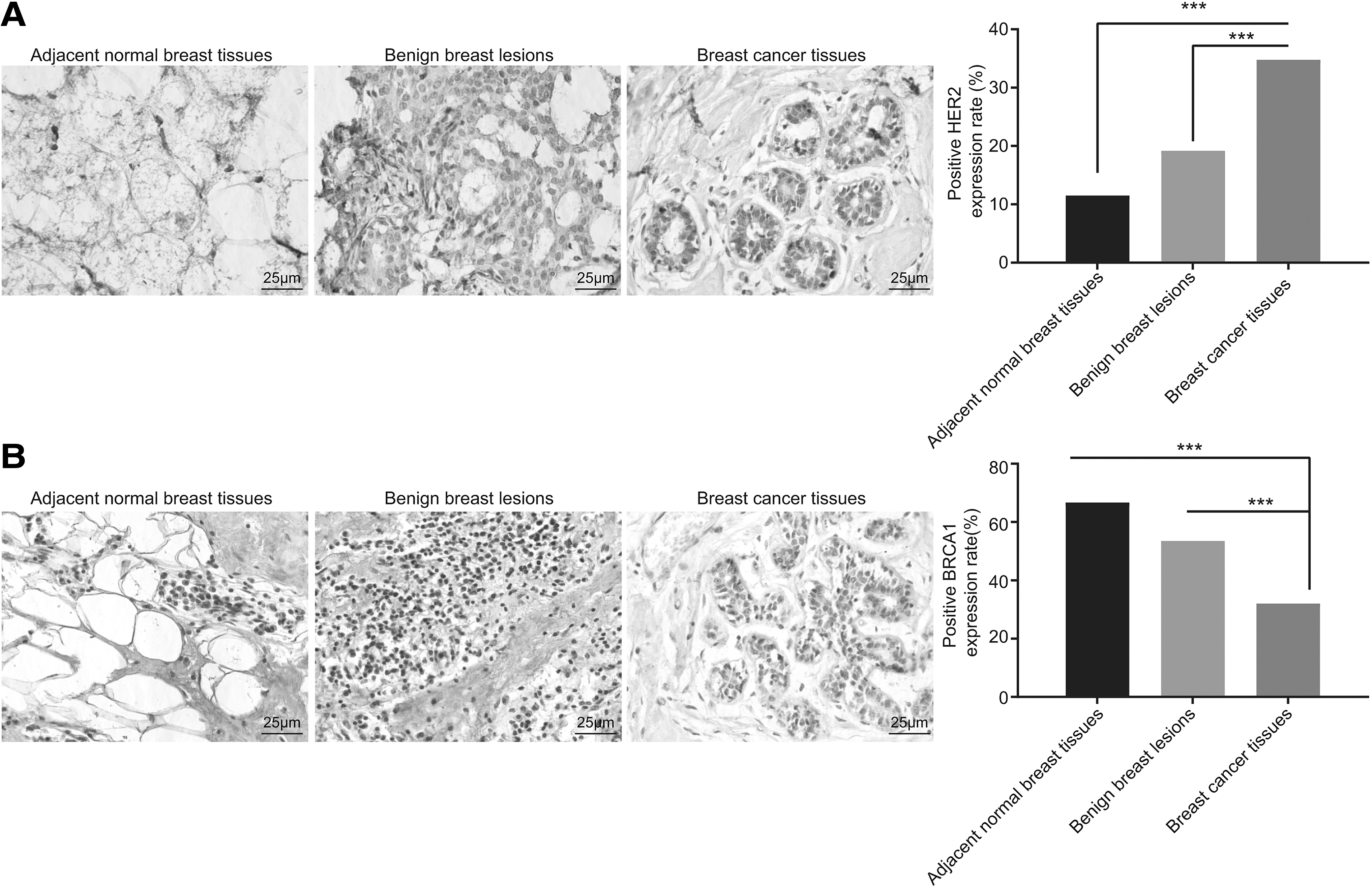
The expression of HER2 and BRCA1 proteins in breast cancer tissues, benign breast lesions, and adjacent normal breast tissues.
Correlation between HER2 and BRCA1 protein expression and clinical data in breast cancer patients
Among the 256 breast cancer patients, a relationship between HER2 expression, histological grade, clinical stage, number of lymph nodes, lymph node metastasis, and androgen receptor (AR) classification was identified (p < 0.05); however, no correlation with age, tumor size and location, pathological type, menopause, estrogen receptor (ER), and progesterone receptor (PR) classification was detected (p > 0.05). BRCA1 expression was found to be associated with clinical stage, lymph node metastasis, and AR and PR classification (p < 0.05), but not correlated with age, histological classification, number of lymph nodes, tumor size and location, pathological type, menopause, and ER classification (p > 0.05), as shown in Table 2.
Clinical Data Analysis of Breast Cancer Patients
AR, androgen receptor; ER, estrogen receptor; PR, progesterone receptor.
Expression of HER2 and BRCA1 in breast cancer and their relationship with the efficacy of radiation sensitivity
Next, the authors set out to evaluate the relationship between positive and negative immunohistochemistry expression of HER2 and BRCA1 and radiation sensitivity. The results revealed that the local failure rate of the 89 HER2-positive patients (31%) was higher than the 167 HER2-negative patients (16%) (p < 0.01) (Fig. 3A), whereas the local failure rate of the 82 BRCA1-positive patients (18%) was significantly lower than the 174 BRCA1-negative patients (39%) (p < 0.001) (Fig. 3B). Results suggest that higher HER2 expression and lower BRCA1 expression are associated with local failure.
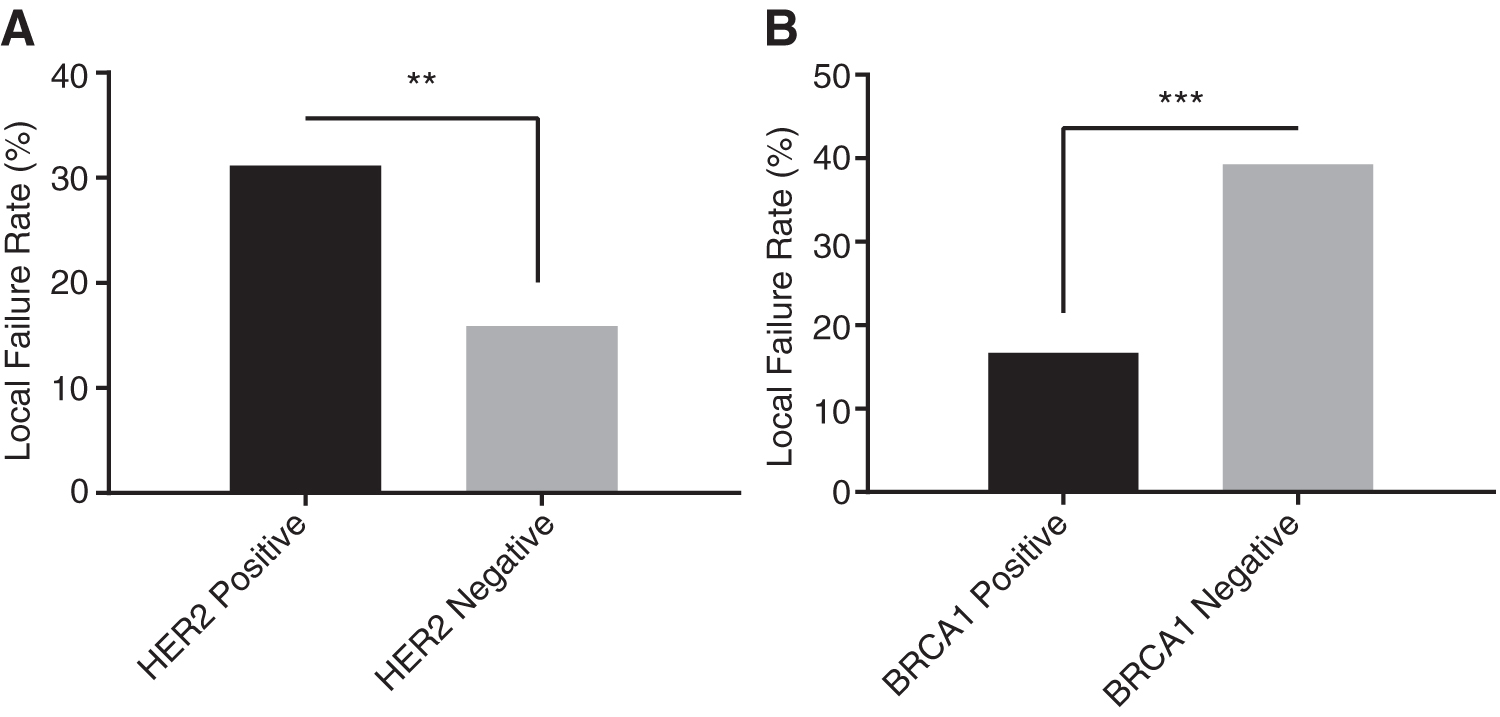
Relationship between HER2 and BRCA1 expression levels in breast tissues with the efficacy of radiation sensitivity.
Prognosis of breast cancer in patients with different expression levels of HER2 and BRCA1
The total survival rate of the 256 patients with breast cancer was 76.2%, with a median value at 32 months, among which the total survival rate and relapse-free survival rate of immunohistochemistry BRCA1-positive patients were 89.0% and 75.6%, higher than that of the immunohistochemistry BRCA1-negative patients with 70.1% and 61.5%, respectively (p = 0.001 and p = 0.038) (Fig. 4A, B). However, the total survival rate and relapse-free survival rate of immunohistochemistry HER2-positive patients were 66.3% and 52.8%, both of which were markedly lower than that of the immunohistochemistry HER2-negative patients with 81.4% and 73.1%, respectively (p = 0.003 and p = 0.020) (Fig. 4C, D).
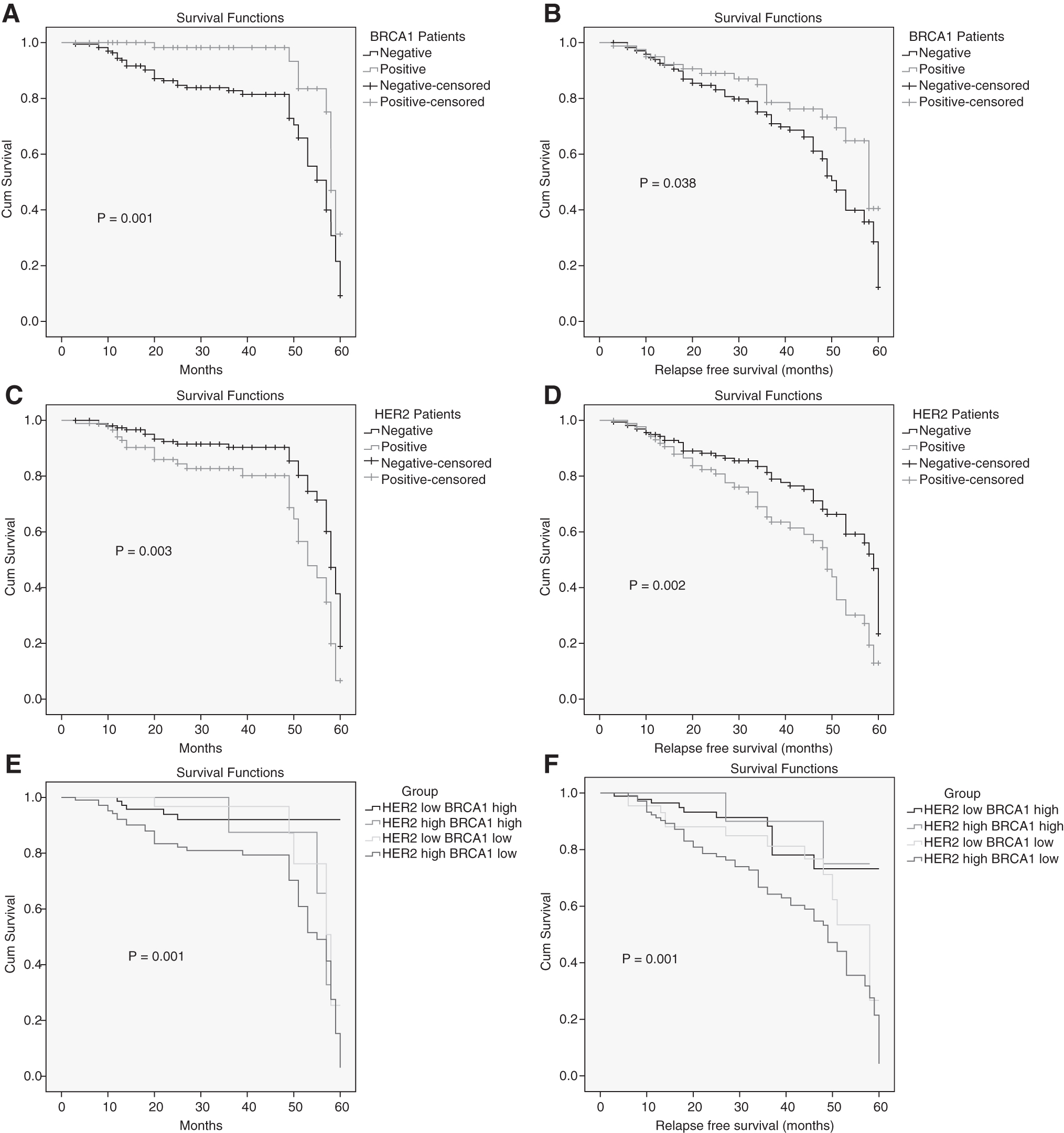
The total survival rate and relapse-free survival rate of patients with different expression levels of HER2 and BRCA1 in breast cancer tissues.
Furthermore, the total survival rate and relapse-free survival rate of patients in the HER2 low BRCA1 High group were higher than that in the HER2 High BRCA1 low group (p = 0.001 and p = 0.001), while there was no significant difference detected in relation to the total survival rate and relapse-free survival rate of patients in the HER2 low BRCA1 low and HER2 High BRCA1 high groups (Fig. 4E, F). Altogether, these results indicated that HER2-positive and BRCA1-negative patients may have poor prognosis.
Correlation between HER2 and BRCA1 expression in breast cancer tissues
To elucidate the relationship between HER2 and BRCA1 expression in breast cancer tissues, the expression of HER2 and BRCA1 was examined in 256 breast cancer samples. Among the 256 breast cancer tissues, 63 patients displayed high HER2 and low BRCA1 expression, while 56 patients exhibited HER2-negative and BRCA1-positive expression; additionally, 26 patients were positive for expression of both, while 111 patients were negative for expression of both. The Spearman correlation analysis indicated that there was no significant difference regarding the expression levels of HER2 and BRCA1 (r = 0.044, p = 0.483) (Table 3).
Correlation Between HER2 and BRCA1 Expression Levels in Breast Cancer Tissues
Discussion
The current study aimed to investigate the relationship between prognosis and radiation sensitivity and expression of HER2 and BRCA1. The results of a series of experiments revealed that prognosis and radiation sensitivity in breast cancer change in patients with varying expression of HER2 and BRCA1.
RT-qPCR results initially revealed an increase in the expression of HER2 mRNA in breast cancer tissues when compared with the adjacent normal breast tissues and benign breast lesions. However, the expression of BRCA1 mRNA was decreased in breast cancer tissues. HER2 is a well-documented, negative prognostic indicator for breast cancer, particularly in the absence of HER2-directed therapy. 16,17 A previous study indicated that activation of HER2 from kinase domain mutation or overexpression is oncogenic in vivo and in vitro and that 20%–25% of breast cancers carry the overexpressed HER2 gene. 18 As a pleiotropic DNA damage response protein, BRCA1 is involved in DNA repair, checkpoint activation, and protection of the genome from double-strand DNA damage in the process of DNA replication. 19 Existing literature has suggested that a germline mutation in BRCA1 may elevate susceptibility to ovarian and breast cancers. 20 Furthermore, increased expression and activity of HER2 have been shown to trigger the oncogenic development of breast tumor cells. 21 Moreover, decreased BRCA1 has been identified among breast cancer patients due to the overexpression of ubiquitin-like with PHD and RING finger domains 1 (UHRF1), 22 which leads to methylation of the BRCA1 promoter by recruiting DNMT1. 23 The expression of HER2 was found to be elevated in breast cancer tissues in comparison with the adjacent normal breast tissues and benign breast lesions, while the expression of BRCA1 was reduced. HER2 stimulates tumorigenesis in breasts through multiple intracellular signaling molecules. 24 The overexpression of HER2 has been found to increase rates of motility and proliferation of cancer cells and is also used in existing therapeutic interventions, such as hormone therapy, radiation, and types of chemotherapy. 25 BRCA1 is a crucial factor involved in the process of DNA repair. 26 Therefore, BRCA1 represents a vital biomarker of DNA damage resistance and reduces risk in breast cancer patients. 26,27
Additionally, the local failure rate in patients with high HER2 expression was found to be higher than that in patients with lower HER2 expression, but the result was opposite with BRCA1. It is demonstrated that high HER2 expression is a poor prognostic factor, 28 with patients exhibiting low BRCA1 expression being at a greater risk with lower overall survival rate than those with high BRCA1 expression. 29 The findings clearly indicate that the total survival of patients with high HER2 expression was lower than that with low HER2 expression, while the total survival of patients with high BRCA1 expression was higher than that with low BRCA1 expression.
Among the 256 breast cancer patients, the expression of HER2 was found to be associated with histological grade, clinical stage, number of lymph nodes, lymph node metastasis, and AR classification, and expression of BRCA1 was found to be correlated with clinical stage, lymph node metastasis, and AR and PR classification. ER, PR, and HER2 statuses represent a crucial tool in guiding treatment decisions for breast cancer patients. In a recent study, Cox regression was employed to evaluate total invasive breast cancer risk by measuring ER, PR, and HER2 statuses, with the results obtained indicating that patients with a lower risk of invasive breast cancer exhibited stronger associations with ER as well as ER-/PR- and ER-/PR-/HER2 subtypes. 30 However, of all three receptors, the PR status is most frequently assayed, on both biopsy and tumor resection material, and is also the most frequently discordant, while the probability of a discordant test result is generally low, but may be affected by several patient and tumor characteristics. 31
Conclusions
In conclusion, the results provide evidence indicating that regulation of HER2 and BRCA1 might be a possible strategy to improve the prognosis of breast cancer and offer a novel therapeutic method for breast cancer treatment. However, extended studies with larger sample sizes are required to confirm the authors' findings. Furthermore, this study only focused on the effects of HER2 and BRCA1 on radiotherapy of breast cancer; whether there are any other additional confounders affecting radiotherapy of breast cancer needs to be further investigated in the future.
Footnotes
Acknowledgments
The authors acknowledge and appreciate their colleagues for their valuable suggestions and technical assistance for this study.
Authors' Contributions
L.Z. designed the study. Y.S. collated the data, carried out data analyses, and produced the initial draft of the manuscript. Y.H. contributed to drafting the manuscript. All authors have read and approved the final submitted manuscript.
Disclosure Statement
There are no existing financial conflicts.
Funding Information
No funding was received for this article.