
Abstract
Background:
Epithelial splicing regulatory proteins (ESRPs) can regulate alternative splicing of RNA and play roles in tumorigenesis and development of various malignancies. In this study, bioinformatic analyses and immunohistochemistry (IHC) were used to investigate the function of ESPRs in serous ovarian carcinoma (SOC) oncogenesis and metastasis.
Materials and Methods:
The mRNA levels of ESRPs were analyzed by Oncomine and gene expression profiling interactive analysis (GEPIA). Prognostic values of ESRPs were analyzed by GEPIA and the UALCAN website. Genetic variations of ESRPs were analyzed by cBioPortal. ESRP1 was selected for further research. The relationship between ESRP1 and immunoregulatory molecules was studied by using the TISIDB database. ESRP1 protein expression in OC was investigated via IHC assays.
Results:
ESRP1 and ESRP2 mRNA were significantly upregulated in SOC (p < 0.05). The prognostic value of ESRP1 mRNA in SOC was inconsistent, and ESRP2 mRNA level did not relate to prognosis for OC patients. The IHC results showed higher ESRP1 expression in OC tissues than in normal ovarian tissues (p = 0.002), and ESRP1 expression in metastatic lesions of OC patients was higher than in paired primary OC tissues (p = 0.035). The ESRP1 expression was related to FIGO stage, differentiation, and peritoneal metastasis (p = 0.016; 0.031; 0.038, respectively). The ESRP1 switch (the differential expression of ESRP1 between metastatic and primary tumor of ovarian carcinoma) was significantly associated with E-cadherin expression in metastatic OC tumors (p = 0.012). The ESRP1 expression in both metastasis and ESRP1 switch significantly correlated with poor prognosis of OC patients (p = 0.045; 0.038, respectively), and ESRP1 switch and FIGO stage were independent risk factors for OC patient prognosis (p = 0.033; 0.009, respectively).
Conclusions:
The ESRP1 may promote OC metastasis by promoting OC cell colonization via the mesenchymal–epithelial transition (MET) process. The ESRP1 expression in metastatic lesions of OC patients may be a biomarker for predicting prognosis and a potential therapeutic target in OC.
Introduction
Ovarian cancer (OC) is the third most common gynecological cancer, and it is in the top ten causes of cancer death in females in the world. 1,2 Most OC patients are diagnosed at advanced stages due to the absence of obvious symptoms at early stages. The poor prognosis of OC patients mainly results from severe peritoneal metastasis. 3 When peritoneal spreading occurs, ovarian tumor cells become more invasive by changing their morphology and epigenetic characteristics to implant into pelvic and abdominal organs and form metastatic lesions. 4 Therefore, it is important to study invasion and metastasis mechanisms of OC in depth and to discover new molecular biomarkers and therapeutic targets for OC peritoneal metastasis.
The epithelial splicing regulatory protein (ESRPs) family includes ESRP1 and ESRP2. 5 The ESRP1 is an epithelial-specific RNA-binding protein that serves as an alternative splicing (AS) regulator. It may regulate the AS of a variety of genes involved in cell adhesion, motility, and epithelial–mesenchymal transition (EMT). 6 Since AS plays an important role in multiple biological and pathological processes, increasing evidence has shown that ESRP1 not only participates in the formation of some organs and tissues in mammalian development but also plays important roles in tumorigenesis and progression of some malignancies such as breast, prostate, lung, and colorectal cancers. 7 –12 The ESRP2 is associated with postnatal hepatic alternative pre-mRNA splicing transitions, prostate cancer metastasis, and pituitary adenoma tumorigenesis. 13 –15
A previous study has shown that decreased ESRP1 expression significantly increases OC cell migration and invasion. 16 The ESRP1 knockdown promoted peritoneal metastasis in a human OC nude mouse model, and upregulating ESRP1 and E-cadherin in a nude mouse model with peritoneal grafted tumors indicated that ESRP1 may also participate in the mesenchymal–epithelial transition (MET) during OC peritoneal spreading. 16,17 However, evidence on the function of ESRP1 in peritoneal metastasis of OC patients, especially evidence from human tumor tissues, is still limited, and the underlying mechanism remains unclear.
In the current study, we analyzed the transcript levels of ESRP1 and ESRP2 in OC by using the Gene Expression Profiling Interactive Analysis (GEPIA) and Oncomine databases; investigated the relationship between ESRP1 and ESRP2 expression and prognosis for OC patients by using the GEPIA database and University of Alabama Cancer Database (UALCAN) website; and studied genetic variations of ESRP1 and ESRP2 in OC tumors by using the cBioPortal database. We further explored the expression of ESRP1, E-cadherin, and N-cadherin in OC by immunohistochemistry (IHC). This study aimed at exploring the possible functions and underlying mechanisms of ESRP1 in OC metastasis as a potential biomarker for prognosis prediction and a therapeutic target for OC.
Materials and Methods
Oncomine analysis
The Oncomine database is a gene microarray database that includes data from 18,000 cancer microarrays. 18 It serves as a tool for collecting, standardizing, and analyzing expression levels, signaling pathways, and interaction networks of genes in cancer tissues. In this study, expression levels of ESRPs in different normal tissues and corresponding malignant tumors were validated by using the Oncomine database. The thresholds for this analysis were set as follows: p value: 0.05; fold change: 1.5; gene rank: all.
Gene expression profiling interactive analysis
The GEPIA database contains RNA expression data, including 9736 tumor samples and 8587 normal samples from the TCGA and GTEx databases. 19 The database is available for single-gene, multi-gene, and correlation analysis of specific tumor types. In the present study, the mRNA expression levels of ESRPs in normal tissues and malignant tumors as well as the correlation between ESRP RNA levels and OC patient prognosis were analyzed by using the GEPIA database. P < 0.05 represented statistical significance.
UALCAN analysis
UALCAN is an interactive website for analyzing malignant tumor data. 20 UALCAN can evaluate gene expression and interplay and DNA promotor methylation with regards to patient prognosis. In this study, UALCAN was used to acquire the relationship between ESRP expression levels and overall survival (OS) of patients with serous ovarian carcinoma (SOC). p < 0.05 represented statistical significance.
cBioPortal analysis
The cBioPortal website provides gene-level data retrieved from multiple platforms. 21 It is often used for analyzing the multidimensional cancer genome data and exploring genetic alternations among diverse samples, genes, and pathways. In the current study, the genetic variation (amplification, deep deletion, and mutation) of ESRPs was demonstrated through cBioPortal analysis.
TISIDB analysis
TISIDB is a database that contains 988 genes related with tumor immune processes and provides a data resource of tumor immune-related genes and the interplay networks of these genes. 22 The database can be used to investigate the effects of genes in tumor immune processes. In this study, the association between the ESRP1 expression and immune regulators was explored by using the TISIDB database.
Patients and samples
Eighteen normal ovary samples and 81 SOC tumors were collected by the Department of Obstetrics and Gynecology at the Shengjing Hospital, China Medical University from April 2008 to August 2014. All samples were histologically diagnosed by pathologists after surgery. All included patients that had not been treated with hormone therapy, radiotherapy, or chemotherapy before surgery.
Primary SOCs (n = 81), paired peritoneal metastatic tumors (n = 64), and normal ovary tissues (n = 18) were obtained for IHC. Each patient had a complete record of clinical pathology data and follow-up data, except five patients who failed to re-visit. Tumor stage was determined according to the 2014 International Federation of Obstetrics and Gynecology (FIGO) classification. 23 All research was approved by the Ethics Committee of Shengjing Hospital, China Medical University (2019PS233K), and written informed consent was obtained from all participants.
IHC assays
The expression of ESRP1, E-Cadherin, and N-Cadherin proteins was verified by IHC. The IHC procedures were conducted according to Chen et al. 24 and positive and negative controls were used in each experiment. A polyclonal antibody against ESRP1 (Abcam, Cambridge, United Kingdom; 1:100), a monoclonal antibody against N-Cadherin (Cell Signaling Technology, MA; 1:200), and a polyclonal antibody against E-Cadherin (Signalway Antibody, MD; 1:600) were used.
The immunostaining score was semi-quantitatively estimated as previously reported. 25 Intensity score: 0 points for no color, 1 point for light yellow, 2 points for brown-yellow, and 3 points for dark brown. Positive distribution score: <5% positive cells were 0 points, 5%–25% were 1 point, 26%–50% were 2 points, 51%–75% were 3 points, and >75% were 4 points. The IHC score of each slice was the average of the product of intensity score and positive distribution score across different vision fields, ranging from 0 to 12 points. Each section score was performed by two experienced pathologists using a double-blind procedure.
Statistical analysis
Continuous variables were presented as medians with interquartile ranges, and non-parametric statistics (Mann–Whitney U test) were used to test differences between groups. The correlation between ESRP1 expression and clinical pathology factors and the relationship of ESRP1 switch with E-Cadherin and N-cadherin in metastasis were demonstrated via the Chi-square test. The Spearman test was used to analyze ESRP1 expression between primary OC and metastatic OC. Survival curves were analyzed by the Kaplan–Meier method. The Cox hazard regression model was used to conduct univariate and multivariate analyses of patient OS. SPSS 21.0.0 software (IBM, NY) was used for statistical analysis. All tests in this study were two-sided, and p < 0.05 was considered statistically significant.
Results
Bioinformatic analyses
ESRP expression levels in a variety of cancers
The GEPIA database was used to study the mRNA expression of ESRPs in several different carcinomas and their respective normal tissues (Fig. 1A–D). We found increased ESRP1 expression compared with normal tissues in breast cancer, leukemia, OC, and other cancers, and decreased expression in cervical and kidney cancers, among others. Increased ESRP2 expression was found in bladder, breast, ovarian, and other cancers, and decreased ESRP2 expression was found in kidney cancer, sarcoma, and others. Both ESRP1 and ESRP2 mRNA were significantly upregulated in SOC (p < 0.05).
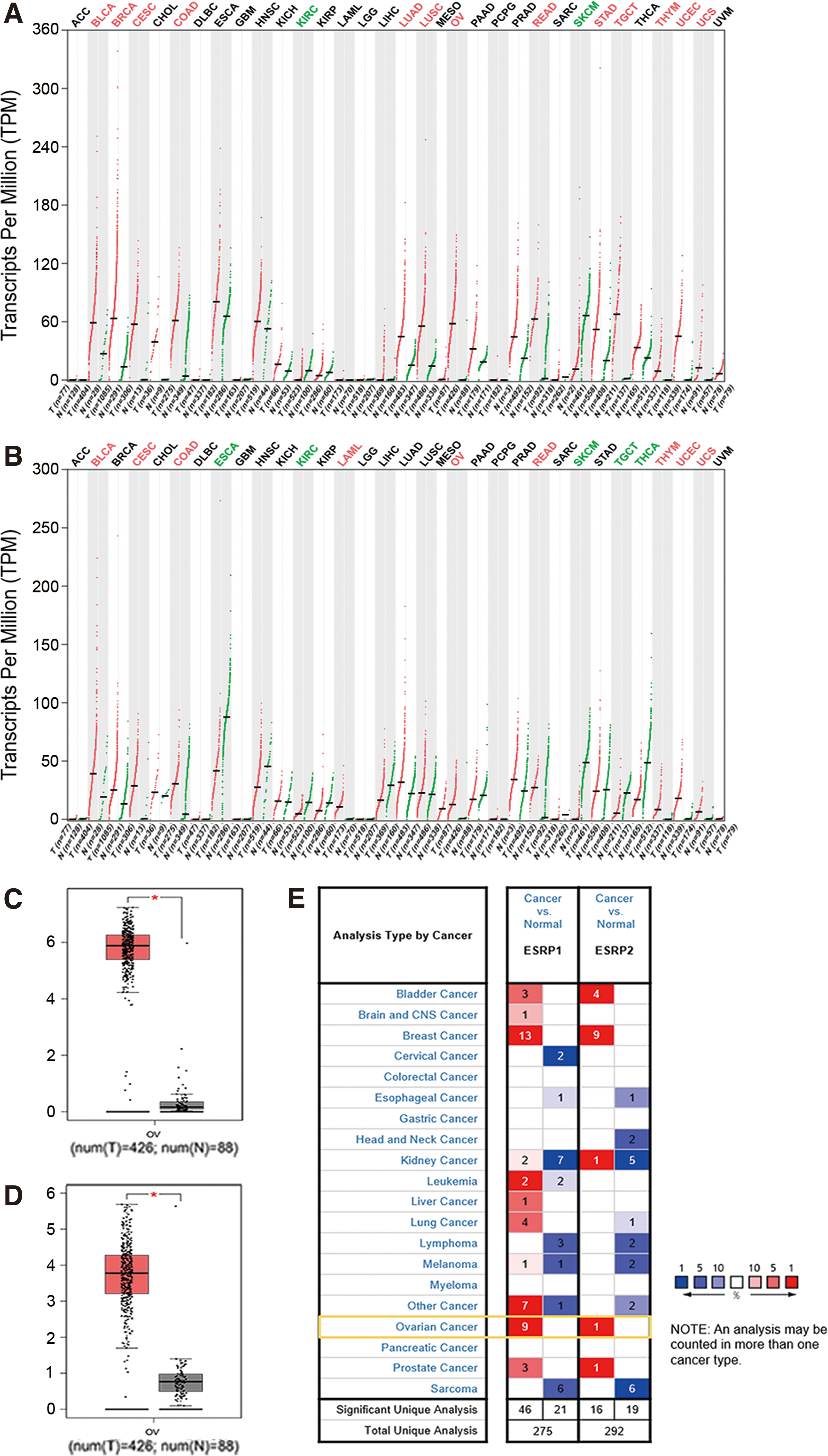
Expression of ESRPs in different types of tumors and normal tissues based on the GEPIA database
The Oncomine database was used to further investigate differential mRNA expression levels of ESRPs in various malignant tumors and normal tissues (Fig. 1E). Compared with normal tissues, ESRP1 expression was significantly upregulated in several malignancies, including bladder urothelial carcinoma, breast carcinoma, and SOC. It was downregulated in skin cutaneous melanoma. In addition, ESRP2 was increased in bladder urothelial carcinoma, breast carcinoma, and SOC. The ESRP2 was decreased in esophageal and kidney renal clear cell carcinomas. All four studies concerning SOC in the Oncomine database showed higher ESRP1 expression in carcinoma tissues than in normal ovary tissue, and two of the four studies showed higher ESRP2 expression in carcinoma tissues (Table 1).
Comparison of Epithelial Splicing Regulatory Proteins in Normal Ovarian and Ovarian Cancer (Oncomine)
Prognostic value of ESRPs in OC
We used the GEPIA and UALCAN databases to analyze the prognostic value of ESRPs in OC. The GEPIA survival analysis showed that neither ESRP1 nor ESRP2 had any relationship with prognosis for OC patients (p = 0.22; 0.41, respectively) (Fig. 2A). However, the ULCAN database showed that ESRP1 overexpression negatively correlated with OS for SOC patients (p = 0.02), whereas ESRP2 expression was not related to OS (p = 0.77) (Fig. 2B).
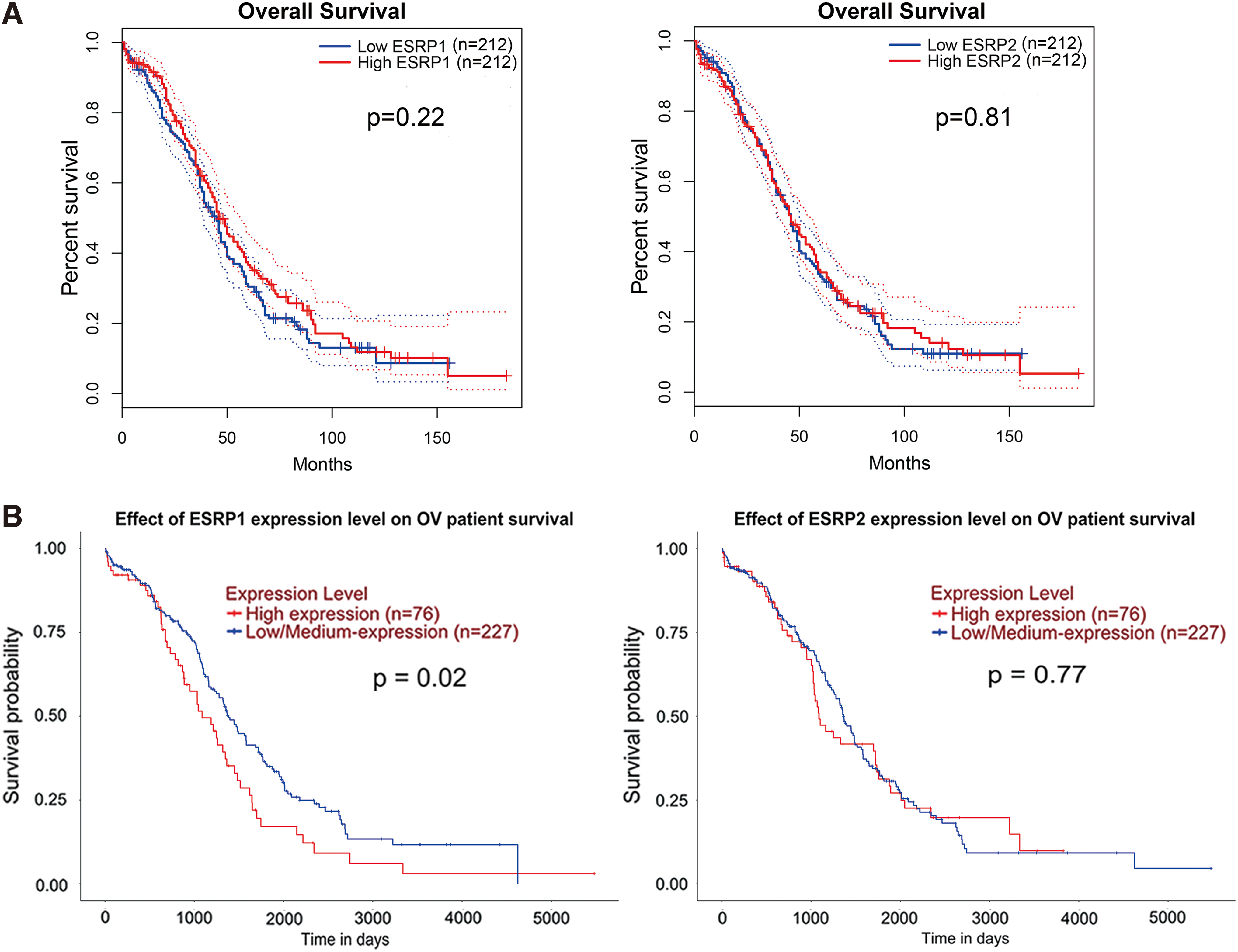
Prognostic value of ESRPs in ovarian cancer in the GEPIA and UALCAN databases. The Kaplan–Meier method was used for univariate survival analysis.
Aberrant ESRP genes in OC
The cBioPortal database was used to analyze the genetic variations of ESRPs across three studies. We derived a total of 1680 cases from cBioPortal, with 489 cases from TCGA, Nature 2011, 585 cases from TCGA, PanCancer Atlas, and 606 cases from TCGA, Firehose Legacy (Fig. 3D). Across all 1680 cases, we found that ESRP1 displayed a higher rate (10%) of genetic variations than ESRP2 (2.4%) (Fig. 3A). Among the ESRP1 variations, gene amplification played the most important role, with gene amplification rates of 15.78% (TCGA; Firehose Legacy), 7.71% (TCGA; PanCancer Atlas), and 4.29% (TCGA; Nature 2011) (Fig. 3B). The main genetic variation of ESRP2 was gene deletion, with gene deletion rates of 3.09% (TCGA; Firehose Legacy), 2.23% (TCGA; PanCancer Atlas), and 1.02% (TCGA; Nature 2011) (Fig. 3C).
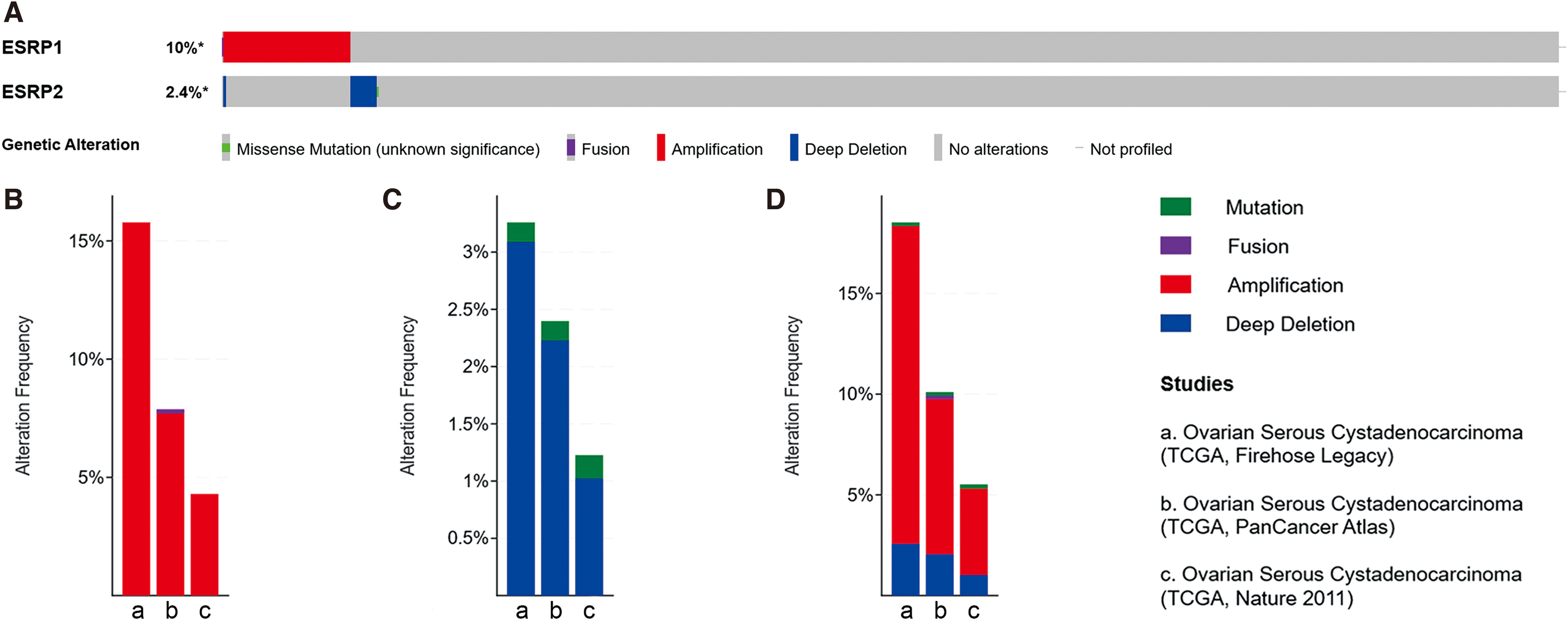
Genetic variation analyses of ESRPs in ovarian cancer via the cBioPortal database.
Correlations between immunoregulatory molecules and ESRP1
We next used the TISIDB database to evaluate the correlation between ESRP1 expression and immunomodulators. Figure 4A shows correlations between ESRP1 expression and immune inhibitors. ADORA2A, VTCN1, IDO1, and IL10RB were the top four immune inhibitors related with ESRP1 (Fig. 4B–E). Figure 4F shows a correlation between ESRP1 expression and immune stimulators, with TNFRSF13C, IL6R, CXCR4, and TNFRSF18 as the top four immune stimulators related with ESRP1 (Fig. 4G–J).
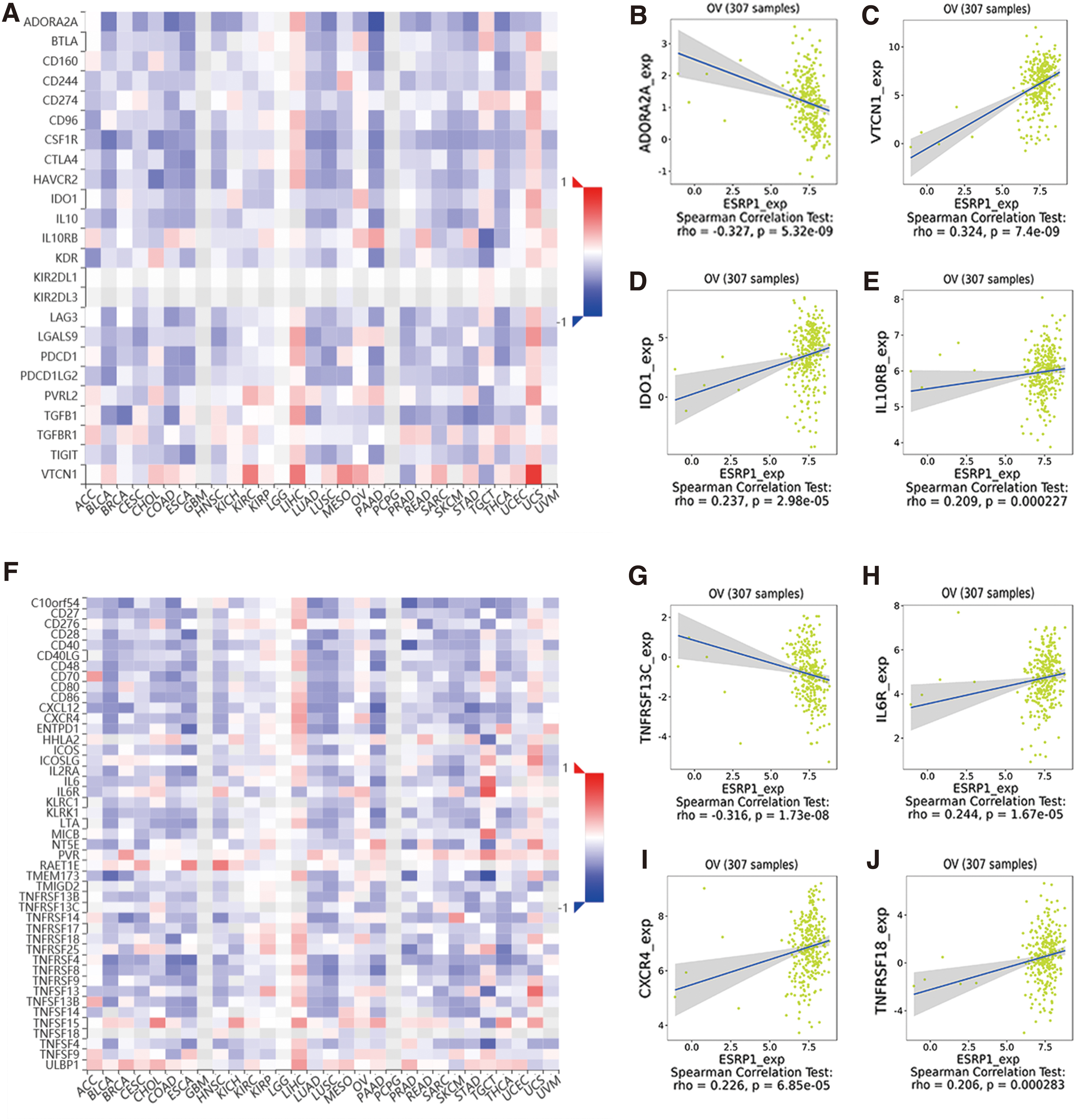
Spearman's correlation of ESRP1 with immunomodulators in the TISIDB database.
ESRP1 expression in OC via IHC assay
ESRP1 expression in normal ovary tissue and SOC
The ESRP1 was mainly detected in the nuclei of normal ovarian cells and SOC cells. The ESRP1 expression in SOC [3.0 (2.0–6.0)] was higher than in normal ovary tissue [1.0 (1.0–2.0)] (p = 0.002) (Fig. 5A–D, S). E-cadherin and N-cadherin were detected in the cell membrane and cytoplasm of normal ovarian cells and SOC cells. The expression of E-cadherin in normal ovary tissues [5.0 (0–8.25)] and primary OC tissues [3.0 (0–6.0)] showed no statistical difference (p = 0.266) (Fig. 5G–J, U). The expression of N-cadherin in SOC tissues [4.0 (3.0–6.0)] was higher than in normal ovary tissues [0 (0–5.0)], (p = 0.002) (Fig. 5M–P, V).
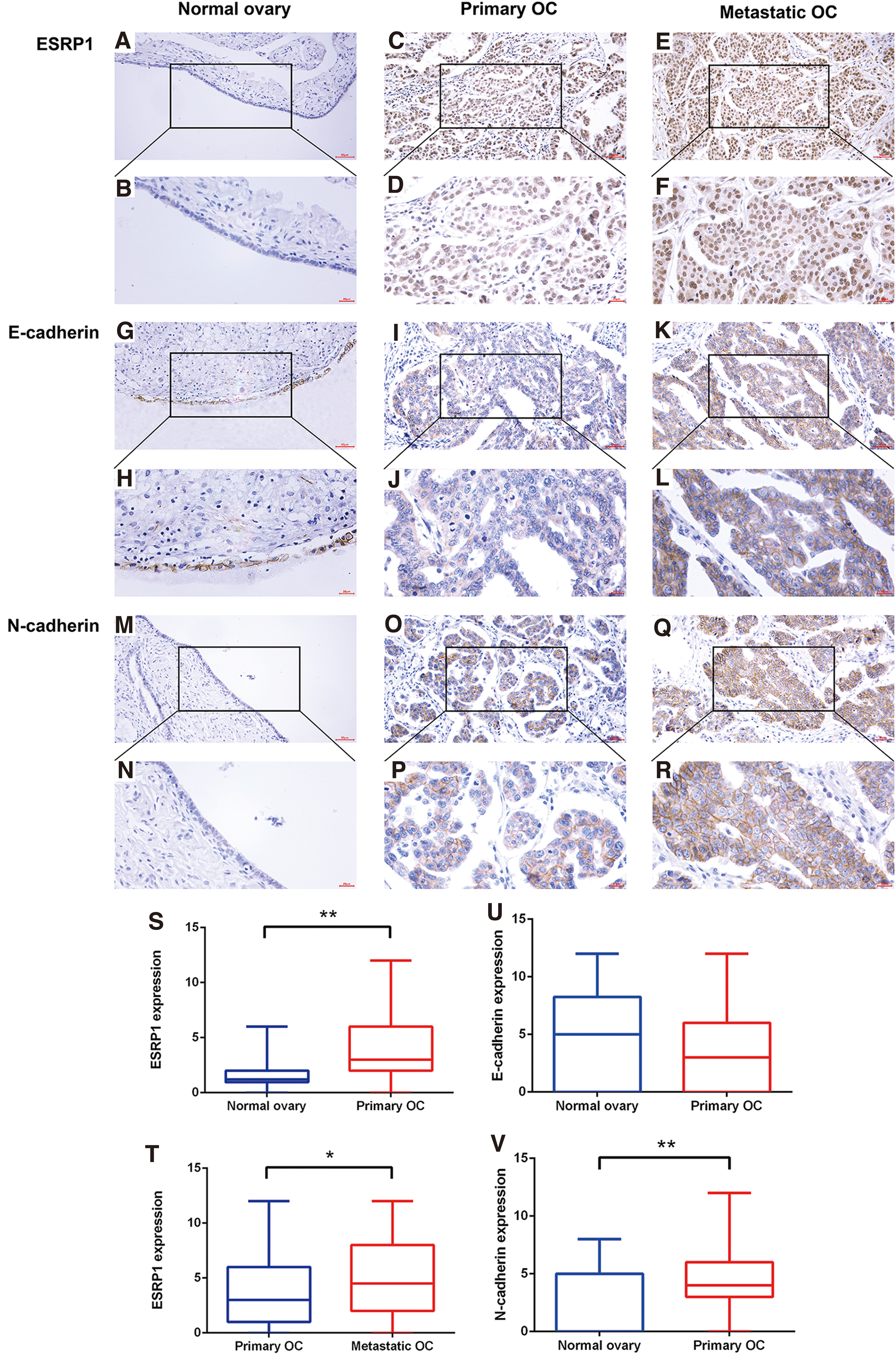
The immunohistochemical detection of ESRP1, E-cadherin, and N-cadherin in tissues.
The relationship between ESRP1 expression and clinical pathological characteristics in SOC
Age, CA125 level, and ascites quantity were each used to divide OC patients into two groups according to the median of variables. The ESRP1 expression significantly correlated with advanced FIGO stage (p = 0.016), differentiation (p = 0.031), and peritoneal metastasis (p = 0.038), but it did not correlate with age, ascites quantity, lymphatic metastasis, or CA125 level in OC patients (p > 0.05) (Table 2).
Correlation Between ESRP1 Expression and Clinicopathologic Factors in Ovarian Serous Cancer Patients
p < 0.05.
ESRP1 expression in primary and metastatic SOC tumors
The ESRP1 expression was significantly increased in metastatic OC tumors [4.5 (2.0–8.0)] compared with paired primary OC tumors [3.0 (1.0–6.0)] (p = 0.035) (Fig. 5C–F, T).
The relationship between ESRP1 switch and E-cadherin and N-cadherin expression in metastatic SOC tumors
Increased ESRP1 expression in metastatic OC tumors compared with paired primary tumors was marked as switch (+), and decreased ESRP1 expression in metastatic OC tumors was marked as switch (−). The ESRP1 switch significantly correlated with E-cadherin expression in metastatic SOC tumors (p = 0.012): ESRP1 switch (+) positively correlated with higher E-cadherin expression, and ESRP1 switch (−) positively correlated with lower E-cadherin expression. However, ESRP1 switch was not related with N-cadherin expression in metastatic SOC tumors (p > 0.05) (Table 3) (Fig. 5K, L, Q, R). In addition, ESRP1 expression in primary tumors had no correlation with expression in metastatic tumors (p = 0.202).
Correlation Between ESRP1 Switch and E-Cadherin Expression as Well as N-Cadherin Expression in Metastasis
p < 0.05; Switch (+) means increased ESRP1 expression in metastatic OC tumors compared with paired primary tumors; Switch (−) means decreased ESRP1 expression in metastatic OC tumors compared with paired primary tumors.
ESRP1 expression and OC patient prognosis
ESRP1 expression in primary OC, metastatic OC, and ESRP1 switch affecting the prognostic value for OC patients
Of the 81 SOC patients included in our study, 76 patients had successful follow-up visits, a rate of 94%. Both high ESRP1 expression in metastatic SOC tumors and ESRP1 switch (+) significantly correlated with unfavorable prognosis (p = 0.045; 0.038, respectively) (Fig. 6B, C), whereas ESRP1 expression in the primary OC tumor had no correlation with patient prognosis (p = 0.419) (Fig. 6A).
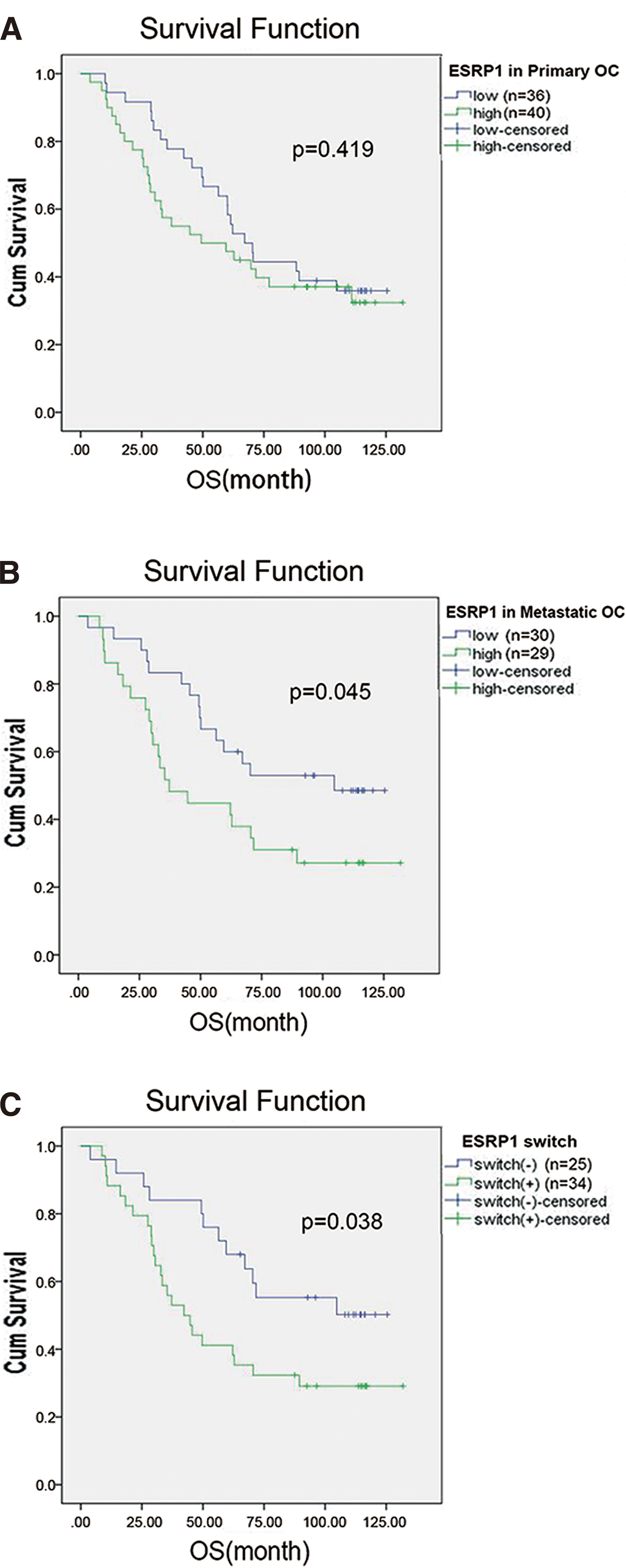
Correlation of ESRP1 expression and OS of OC patients was analyzed by Kaplan–Meier plot.
Independent risk factors affecting prognosis of OC patients
The Cox regression model was used to analyze the relationship between OS and ESRP1 expression in primary and metastatic SOC tumors, ESRP1 switch, age, FIGO stage, CA125 level, lymph node metastasis, and ascites quantity of SOC patients. Univariate analysis showed that ESRP1 expression in metastatic SOC tumors, ESRP1 switch, FIGO stage, and ascites quantity were all risk factors for prognosis of OC patients (p = 0.049; 0.042; 0.005; and 0.007, respectively). Multivariate analysis indicated that ESRP1 switch and FIGO stage were independent risk factors for prognosis in SOC patients (p = 0.033; 0.009, respectively) (Table 4).
Univariate and Multivariate Analyses for Ovarian Cancer Patients on Overall Survival
p < 0.05; Switch (+) means increased ESRP1 expression in metastatic OC tumors compared with paired primary tumors; Switch (−) means decreased ESRP1 expression in metastatic OC tumors compared with paired primary tumors.
CI, confidence interval; HR, hazard ratio; OC, ovarian cancer.
Discussion
The SOC accounts for about 70% of OC. Eighty-five percent of SOC patients with poor prognosis are diagnosed at an advanced stage. 29 Therefore, it is highly significant to investigate the molecular mechanism of SOC tumorigenesis and progression.
The ESRPs are RNA-binding proteins that can regulate alternative RNA splicing. 5,30 Studies show that ESRPs participate in embryonic development in some vertebrates and that they associate with development defects of some vertebrates. 30 Recent studies show that ESRPs are involved in regulating cell adhesion, polarity, and migration 5 and that they relate with tumorigenesis and progression of malignancies, including colorectal, pancreatic, and pulmonary cancers. 31 –34
In the current study, we used a variety of bioinformatic analyses to show that ESRP1 and ESRP2 are highly expressed in OC compared with normal ovary tissue and that there is a higher gene mutation rate in ESRP1 than ESRP2. We also found that ESRP1 is related with prognosis of OC patients according to the UALCAN database.
According to the Oncomine database, ESRP2 expression was higher in OC than in normal ovary tissues. However, according to cBioPortal analysis, the genetic alteration of ESRP2 in OC is mainly deep deletion. It is confusing that ESRP2 transcripts are higher in OC whereas the main genetic alteration of ESRP2 is deep deletion, but the total deletion rate of ESRP2 is less than 2.4%, much lower than the nearly 10% of amplification rate of ESRP1. Besides the genetic alterations, epigenetic alterations such as histone modification, DNA methylation, and non-coding RNAs may also play important roles in transcription. It is possible that these epigenetic alterations may promote ESRP2 transcription to overcome the deep deletion mutations.
It should be mentioned that the prognosis results of ESRP1 from the GEPIA database are not consistent with the UALCAN database. This may be due to several reasons. First, the patients from the GEPIA database could only be restricted to OC, whereas the patients from UALCAN could be restricted to SOC. This difference in patient source between the two databases may lead to different results. Second, the two databases also use different patient grouping methods. The patients from the GEPIA database were divided equally into two groups according to the median level of ESRP1, whereas the patients from the UALCAN database were divided into high expression and low and middle expression groups, each with different numbers of patients, which may cause statistical contradictions. A larger sample size may be needed to verify these results. Since the results from the databases were inconsistent, we decided to investigate ESRP1 expression in OC in depth.
We used IHC to investigate ESRP1 expression in SOC and found higher ESRP1 protein expression in SOC than in normal ovary tissue, indicating that ESRP1 may promote OC cell proliferation, consistent with a previous report. 17 The cBioPortal analysis showed a significantly higher gene mutation rate for ESRP1 than ESRP2, and the gene mutation type of ESRP1 was mainly gene amplification. Gene amplification can alter copy number variants of genes, leading to abnormal expression of corresponding genes and playing a significant role in the development of malignant tumors such as prostate cancer. 35,36 Both bioinformatic analysis and IHC assays indicated high ESRP1 expression in SOC, suggesting that dysregulated ESRP1 expression, possibly caused by gene amplification, may relate to SOC tumorigenesis.
Our finding that ESRP1 relates to the FIGO stage of SOC suggests that ESRP1 might relate to SOC metastasis. Further research confirmed that ESRP1 expression was higher in peritoneal metastasis than in primary SOC tumors, indicating that ESRP1 expression increases during the process of SOC cell metastasis from the primary tumor. Previous studies show that metastasis activates drastic changes in morphology and genetic and epigenetic performance of tumor cells and that these differences may correlate with progression of tumor metastasis and chemotherapy resistance. 37,38 Therefore, the differential expression of ESRP1 between primary and metastatic SOC indicates that ESRP1 is closely associated with SOC metastasis and that it likely participates in the metastasis process.
Tumor metastasis can be conceptually divided into two stages: tumor spreading and tumor colonization. 39 Previous studies have indicated that EMT and MET occur in the two stages of OC metastasis, respectively, with tumor cells acquiring enhanced motor ability and invasiveness through EMT 40 –44 in the primary tumor and then enhanced adhesion and colonization ability through MET in the metastatic lesion. Tumor cells separate from the primary lesion through EMT, then seed into another place, and grow through MET. Cell function experiments also indicate that ESRP1 may associate with MET in OC. 16,17
To further clarify the correlation between high ESRP1 expression in SOC metastasis and MET at the tissue level, the expression of ESRP1 and the classic EMT markers E-cadherin and N-cadherin was studied through IHC. The results indicate that ESRP1 switch (+) relates with high E-cadherin expression in metastasis, whereas switch (−) relates with low E-cadherin expression in metastasis, but ESRP1 switch showed no relationship with N-cadherin expression. These findings suggest that ESRP1 may associate with the MET process in SOC cell adhesion and colonization at the metastasis site to promote disease progression.
We further analyzed the relationship among ESRP1 expression in primary OC, metastatic SOC, ESRP1 switch, and OS for SOC patients. We found that higher ESRP1 expression in both SOC metastasis and ESRP1 switch (+) was associated with poor prognosis of SOC, whereas the expression of ESRP1 in the primary tumor did not relate to patient prognosis. This illustrates that ESRP1 expression in metastasis is a more effective candidate biomarker for predicting SOC prognosis.
The TISIDB database showed that ESRP1 had a positive and negative association with several immunoregulators, including immune inhibitors and immune stimulators. Currently, the relationships between most of these immunoregulators and OC remain unclear. Among these immunoregulators, ESRP1 was positively associated with immune inhibitors, VTCN1 and IDO1. VTCN1 can promote OC progression and metastasis as an immunoinhibitory factor, 45,46 and IDO1, a tumor-associated antigen, is also related to progression and poor prognosis in OC. 47,48 Thus, ESRP1 may also work as an immunosuppressor to promote the progression of OC, leading to poor prognosis for OC patients.
Conclusion
Our combined bioinformatic and IHC results show that ESRP1 associates with SOC tumorigenesis and progression, and it may promote peritoneal spreading of SOC by participating in the MET process in metastatic tumors. The ESRP1 expression in both metastatic SOC tumors and ESRP1 switch is associated with SOC patient prognosis, indicating that ESRP1 expression in metastatic tumors is a better biomarker, compared with its expression in primary tumors, for predicting prognosis of SOC. The ESRP1 may also be a potential target for treatments to block metastasis in SOC. In the future, we may improve therapeutic effect and survival of SOC patients by reducing ESRP1 expression or blocking other related pathways.
Footnotes
Acknowledgment
The authors are grateful to the Biobank of Shengjing Hospital of China Medical University for their kind support during tissue collection.
Authors' Contributions
X.L.: Data Collection; R.L.: Statistical Analysis; X.W.: Literature Research; Q.G.: Statistical Analysis; L.W.: Literature Research; X.Z.: Study Design. All coauthors have reviewed and approved of the article before submission.
Disclosure Statement
The authors report that no competing financial interests exist.
Funding Information
This work was supported by the National Key Research and Development Program of China (MOST-2019YFC1316104, X.Z.), the National Nature Science Foundation Project of China (82072885, X.Z.), Key Research and Development Program of Liaoning Province (2020JH2/10300124, X.Z.), the Science and Technology Project of Shenyang city (19-112-4-104, X.Z.), and the 345 Talent Project of Shengjing Hospital of China Medical University (X.Z.).