
Abstract
Frequent cases of gastroenteritis, resulting in several fatalities within remote communities in the Yasawa Islands, Fiji, prompted an urgent drinking water quality and supply assessment. This project initially investigated the quality of drinking water from multiple sources in communities on Naviti Island. Escherichia coli was detected in all sampled sources, including wells, springs, and rainwater tanks (above ground). E. coli most probable number counts were higher in well and spring water (typically >100 organisms per 100 mL) than rain tanks (ranging between 13.6 and >100). Assessment of potential water treatment alternatives, incorporating community input, determined that disinfection of rain tanks through chlorination was the most feasible and community acceptable option to address the contamination. A model was then developed to assess: (1) the likelihood that a typical household rainwater tank could adequately supply water throughout the wet and dry seasons and (2) the likely free chlorine residual that would result from a program of periodic dosing with 12.5% sodium hypochlorite. In a pilot trial in Mua-Ira village, chlorination of rainwater tanks proved successful in removing E. coli and community rollout was initiated. Periodic chlorination paired with tank and gutter maintenance were recommended to community and a local partner organization, and a training package was developed to assist this. The project holds potential to minimize pathogenic bacterial contamination in the studied drinking water sources and serve as a model to address water contamination through simple, low-cost, community-accepted solutions in the wider region.
Introduction
Access to safe drinking water is recognized as a fundamental human right (UN, 2010) and was added as an individual right to the national constitution of Fiji in 2013 (WHO, 2015). The United Nations identifies access to improved water, sanitation, and hygiene (WaSH) services as critical for improving the health, wellbeing, and socioeconomic situation in developing countries, such as Fiji; WaSH is the focus of Sustainable Development Goal (SDG) 6 (UN, 2015).
Over the past few decades there have been significant improvements in access to WaSH services in Fiji, spurred by development funding, with access to improved drinking water for the country reported by WHO (2015) as 96%. However, while people and communities may be nationally reported to have access to improved water, the situation on the ground is often different. Certain geographically remote regions, such as the Yasawa Islands, which are only accessible by boat or sea plane, struggle with water source contamination and a high degree of variability in seasonal water availability (van der Lann et al., 2016).
In response to illness and fatalities (predominantly children) resulting from gastroenteritis, a waterborne disease, leaders from remote rural communities of the Yasawa Islands, specifically Mua'ira, Kese, and Soso on Naviti Island and Namara on Wayasema Island (Fig. 1) requested assistance from the research team through a local organization, the Barefoot Collection. The Barefoot Collection operate ecotourism sites on the Yasawa Islands of Drawaqa and Kuata (Fig. 1), providing employment and a share of revenue to these local communities. In line with the call to address the Grand Challenges facing the world (NASEM, 2019), an urgent investigation was launched by our team of environmental engineers into the nature and quality of drinking water sources in these communities, and possible approaches to improving the safety of drinking water resources (if the suspected contamination was confirmed).
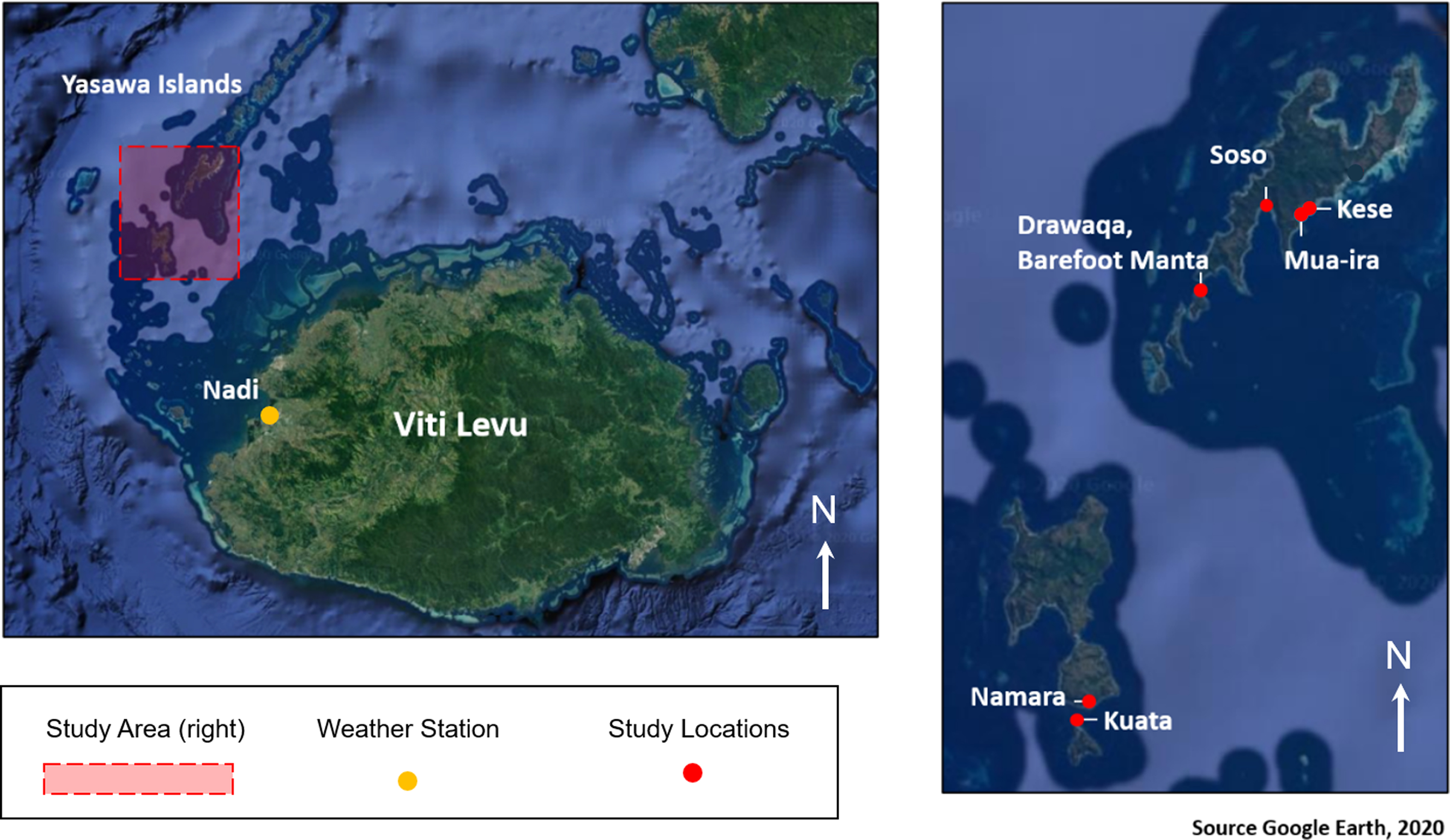
Location of the Yasawa Islands chain and communities participating in this study (Image source: Google Earth, 2020).
Provisional testing by Otley et al. (2018) using the simple Whirl-Pak® presence/absence test found that Escherichia coli—a ubiquitous indicator of fecal matter contamination, was present in the majority (>75%) of drinking water sources sampled in Mua'ira, Kese, Soso, and Namara (Fig. 1). The sources tested included rainwater tanks (both large above-ground communal tanks and above-ground individual household tanks), shallow wells (dug into the surficial sand aquifer) and spring water (fed to the villages through gravity flow from outlets in nearby mountainous areas). During initial community consultations it was noted that the wells were suspected by users to be contaminated and a (primary) cause of gastrointestinal illnesses, and that typically, the alternative water sources (rain and spring water) were unable to provide adequate volumes of drinking water during the dry season (normally May to October), meaning residents had little choice but to periodically utilize contaminated well water. The contamination source(s) impacting drinking water were hypothesized to be primarily linked to fecal contamination associated with unimproved sanitation infrastructure and practices, and a lack of any formal water source protection measures (Otley et al., 2018).
The research presented in this article expands the investigation by Otley et al. (2018), following their recommendations to:
Obtain more detailed information regarding the extent of fecal matter contamination in drinking water sources (e.g., through quantitative methods) and hence better understand contamination severity and pathways, Assess a range of possible interventions, which could result in increased access to improved drinking water, free of pathogens associated with fecal contamination, Engage community leaders and households in this process, thereby building their capacity to participate in ongoing activities required to maintain access to safe drinking water.
Donnelly (2010) evaluated a strength-based approach in such contexts within the Pacific, arguing that common western approaches led by Non-Governmental Organizations (NGOs) often alienate community members, decreasing the potential for lasting impact (e.g., improved health outcomes). The strength-based approach aims to incorporate existing skills, values, and assets within communities to improve WaSH outcomes and add value to the ongoing effectiveness and sustainability of WaSH interventions. The lasting effectiveness of previous projects aimed at enhancing access to safe drinking water within the Pacific region is very low, for example, Clarke et al. (2014) found that just 1 of 27 WaSH improvement projects evaluated in Pacific Island nations could be deemed sustainable and beneficial 3 years following cessation of funding and third-party management. This breakdown was attributed to the communities' lack of access to ongoing expertise, funding, and materials, indicating many well-intentioned projects are destined to fail. Mirti and Davis (2005) also recognized that most Pacific Island nations have limited ability to carry out comprehensive water quality monitoring and management programs. A lack of ability to carry out monitoring and management is often due to insufficient equipment and expertise for ongoing water quality supply system control (e.g., disinfection and other treatment methods), and water quality monitoring and associated data management as well as inadequate skills and capacity. These findings are consistent with wider reviews of the effectiveness of WaSH programs across the sector (e.g., Marshall and Kaminsky, 2016), and the importance of monitoring to underpin successfully addressing global environmental, health, and humanitarian challenges in the 21st Century (NASEM, 2019).
Our approach aimed to overcome these challenges through development of a pilot program, using a “design with” the community approach involving: (1) simple, low-cost methods of assessing drinking water quality and treating contaminated water sources that aligned with community strengths and wishes; (2) development of training and educational materials designed to build capacity and thereby enhance the likelihood of lasting and sustainable improvement in access to safe drinking water in the communities. The objectives of the study were to:
Design, implement, and demonstrate a targeted and low-cost approach to rapidly assess the quality of drinking water sources in the remote communities, overcoming limitations, such as geographic remoteness and lack of access to laboratory facilities,
Based on community consultation and wishes, develop and implement a pilot program of targeted intervention—chlorine disinfection of rain tanks—to address contamination of one of the major drinking water sources (and assess the program's effectiveness in such settings),
Strengthen relationships and build capacity and knowledge within the community (e.g., through simple training guides), aiming to increase participation in the management of community drinking water sources, enhancing the prospects that they will remain free from contamination in the future.
We believe the approach and findings outlined in this study are of wider relevance to many geographically remote communities faced with similar water supply issues and constraints throughout the Pacific Islands and elsewhere.
Methodology
To meet the study objectives, two site visits were completed. As the provisional testing by Otley et al. (2018) had detected the presence of E. coli during both the wet season (November to April) and dry season (May to October) it was deemed appropriate to conduct a single detailed water quality assessment at the earliest opportunity and capture any seasonal variations as part of ongoing monitoring. This first water quality assessment visit, in April/May 2019, to the communities of Mua'ira, Kese, Soso, and Namara (Fig. 1), focused on determining the level of E. coli present in 15 drinking water sources, as well as a community consultation regarding potential WaSH options. A follow-up site visit in September 2019 focused on a chlorine disinfection pilot of seven rainwater tanks in the village of Mau'ira. In between these visits, a team conducting related research visited the site and were able to conduct limited additional testing at our team's request (see Pilot disinfection program implementation, validation, and dissemination).
Drinking water source assessment
Initial testing for the presence/absence of E. coli in the communities' drinking water sources, including a selection of wells, above-ground rainwater tanks (installed adjacent to households and other community buildings) and drums containing gravity-fed spring water, was conducted by Otley et al. (2018) in March, August, and November 2018, using the Nasco Thio-Bag Test Kits (Whirl-Pak). These kits provide a simple indication of the presence or absence of bacterial coliforms and E. coli, through assessment of the fluorescence of a bacterial enzyme, without the need for an incubator, complex laboratory equipment, and/or extensive training.
The rain tanks predominantly collect water off household rooftops, although community also reported that the communal church tank (asset ID RW201) is periodically filled by a government water barge, which delivers emergency water supplies on an ad hoc basis. All homes are rectangular and single storey with corrugated metal roofs at a standard pitch of ∼20 degrees. Plastic guttering on just one edge of the roof diverts rainwater to individual tanks with no first flush system integrated. Spring flow is seasonal and derives from a fractured rock aquifer, whereas the wells are shallow dug wells intersecting the water table in the localized phreatic sand aquifer.
To further understand the extent of E. coli contamination in drinking water sources, the Aquagenx Compartment Bag Test (CBT) was selected as the technique for obtaining a quantitative measure of the severity of fecal contamination in the water sources. This method requires no major laboratory equipment or specialized expertise, has been validated against other established methods of quantifying E. coli (Stauber et al., 2014), and has been shown to be effective in analogous field settings (Wang et al., 2017). The method provides results for the “most probable number” (MPN) of E. coli organisms in a 100 mL water sample according to a five-increment scale, within a 95% confidence interval (Stauber et al., 2014). The scale allows for ready comparison with the Guidelines for Drinking Water Quality (WHO, 2011); the relevant data are reproduced in Table 1. The only major constraint with the method is that samples require incubation for between 24 and 48 h at a temperature above 25°C (Aquagenx, n.d). This was readily achievable at the study site given the normal 24-h temperature range of 23–31°C. While E. coli is not necessarily the most appropriate or sensitive indicator of the health risk from consumption of rainwater-based sources, and more advanced testing methodologies are being developed (e.g., Bae et al., 2019), the need to use cheap and simple test kits, which could readily provide a rapid indication of fecal contamination was deemed to outweigh the benefits of attempting to use more sophisticated methods (e.g., Sorensen et al., 2015).
Health Risk Categories at Different Escherichia coli Concentrations, from WHO (2011)
MPN, most probable number.
To conduct a quantitative assessment, water samples were taken during the site visit in April-May 2019 to the communities of Mua'ira, Kese, Soso, and Namara, (Fig. 1). Sample sites included three above-ground rainwater tanks, seven groundwater wells, and four outlets from a gravity-fed spring water supply (including the highest accessible elevation where the spring water emerges). Each of the 15 water sources were assigned an asset ID with the exact GPS location recorded. At the time of the April-May 2019 site visit, the relationship between the research team and the communities was still developing and access for sampling was provided at the community level rather than individual households. As such, sampling focused on communal water sources for example, RW201, a communal 100,000-L tank connected to the church in Mau'ira, and wells accessible to all community members. The only private water source sampled was a Mau'ira resident who requested that their household rainwater tank be sampled (asset ID RW202). The specific locations for these water sources in Mau'ira and Kese are shown in Fig. 3.
All steps required to prepare the samples for incubation were conducted immediately at the water source in accordance with the product instructions (Aquagenx, n.d.). At the same time, physiochemical parameters (pH, electrical conductivity, and dissolved oxygen) were recorded using a HACH™ 40qd portable field meter. The CBT samples were then incubated in darkness (to prevent UV light impacting bacterial presence) in a secure location, where temperatures remained above 25°C. Results were assessed following 40 to 48 h of incubation. Two samples of Fiji Water™, a common commercial bottled water brand, were used as a control for the CBT testing—neither control sample recorded any detectable E. coli using the method.
Community consultation and assessment of WaSH options
The links between the project team and local communities were established through a long-term partnership between RMIT University and the Barefoot Collection, an ecotourism operator located on Drawaqa and Kuata Islands (Fig. 1). During the April-May 2019 site visit, discussions with community leaders and assessment of current and possible future drinking water supply opportunities were conducted. Several new 5200- and 10,300-L household rainwater tanks and guttering systems were observed to have been recently delivered; residents indicated that these had been donated and installed with the aid of two NGOs—Vinaka Fiji and UN-Habitat. These tanks provided the potential for contained drinking water sources for most households in Mua'ira village for the first time, increasing the prospect that households may be able to source drinking water from rainwater (as opposed to contaminated wells) throughout the year. At the time of the April-May 2019 site visit, several of the household rainwater tanks were not yet installed and were being stored on the beach front. During a traditional Sevusevu ceremony in Mua'ira village following the team's arrival in April 2019, community leaders requested “adding some chemical to the rainwater tanks to make them safe.” This and other discussions highlighted a consensus among the community that rainwater would be a preferred source over well water for drinking water, and that there was an awareness that rainwater tanks were also vulnerable to contamination if not treated and maintained. These opinions likely stemmed in part from the dissemination of results of the work by Otley et al. (2018) during the 12 months before the site visit, as well as ongoing communications between Barefoot Collection staff, the NGOs and locals, throughout the region. The results of water quality testing and community consultation, along with a process-oriented analysis of the potential options available to enhance drinking water safety (Fig. 2), led the team to focus on rainwater tank disinfection and maintenance as the next logical, achievable, and locally accepted means toward achieving more sustainable, safe drinking water in the communities.
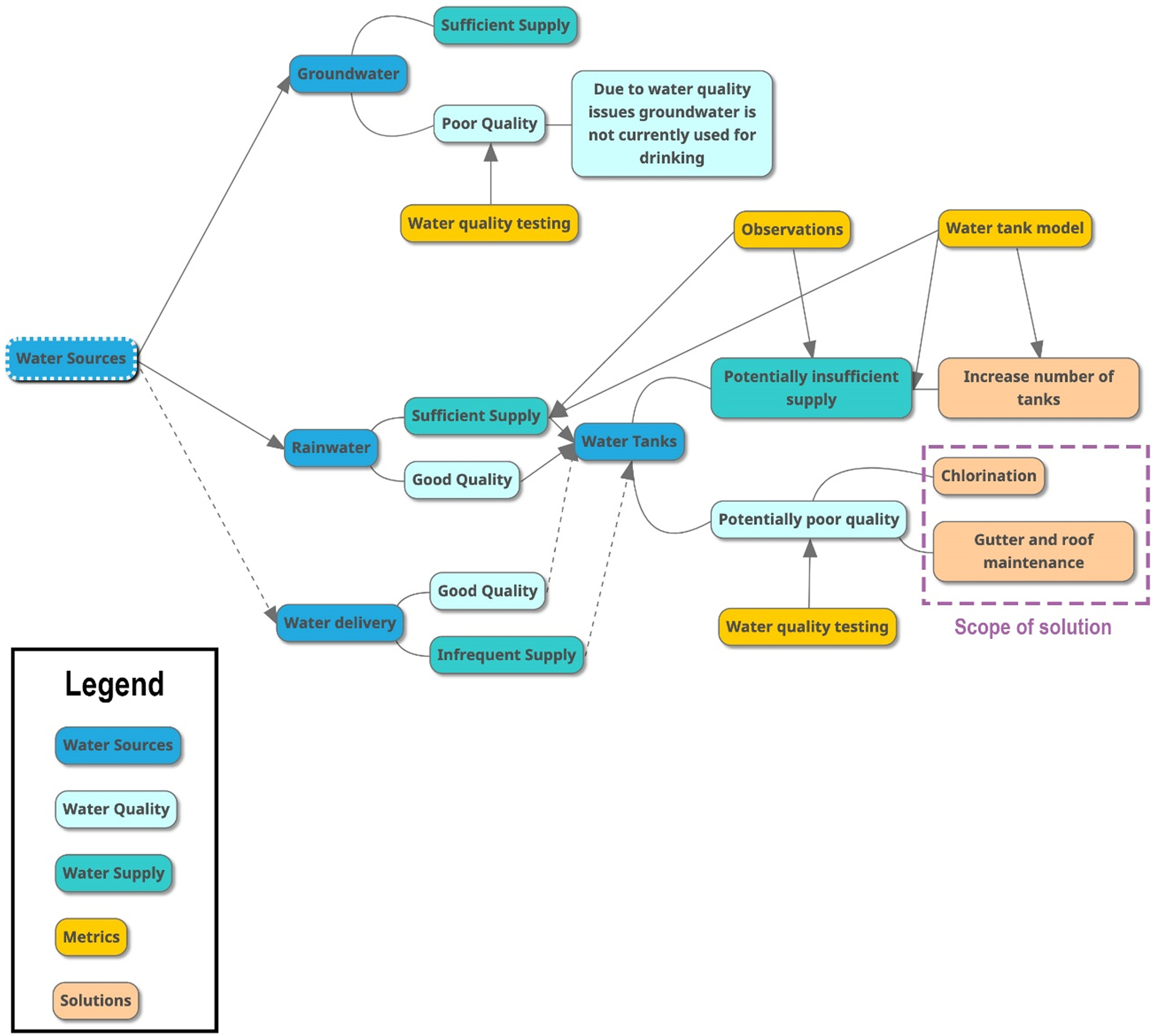
Flow chart used to assess range of possible drinking water source protection.
Development of rainwater tank model
Following the April-May 2019 site visit, a contextualized rainwater tank model was developed to:
Determine the extent to which the installed rainwater tanks could provide sufficient volumes of drinking water to meet ongoing household needs.
Determine the influence of dosing these tanks with sodium hypochlorite at different times of the year on the likely length of disinfection.
The Rainwater model was developed in Microsoft Excel® and included local climatic data sourced from the Fiji Meteorological Service, including daily rainfall from the nearest available weather station, Nadi (Fig. 1) from 1971 to 2016 (with some missing years in the record). The distance between Nadi and the site location (74 km), and likely influence of local factors, such as topography on precipitation amount, are acknowledged to introduce uncertainty into the model results.
The model calculated the anticipated volume of water in a tank throughout the year, based on roof area and tank volume, initially using the following default parameters: tank volume of 5200 L, roof area of 40 m2, and average water usage for cooking and drinking of 20 L per person per day (WHO, 2012). These were later updated, in the September field visit, using on-site data collected from a range of households (e.g., measurements of specific roof areas). The volume calculations used a baseline period (average monthly rainfall over the dataset) and three case study years (2014, 2015, and 2016), to assess the status of rain tanks during a range of climate scenarios, including average, wet, and dry years.
Both future climate—particularly under the influence of global climate change—and changing household demand for water are acknowledged to be sources of uncertainty in the applicability of the model in the coming years. Additionally, the model simulated the likely chlorine residual present in a rainwater tank each day of the year, following dosage at different times, using standard 12.5% sodium hypochlorite solution, which is available at the nearby Barefoot Collection resort (and whose owners agreed to supply for the purposes of the pilot). The model assessed the daily chlorine residual concentration against a target of achieving a value within the recommended range of 0.2 to 5.0 mg/L (WHO, 2003). The model assumed no chemical decay of the added chlorine and complete mixing of water and chlorine throughout the tanks. Chlorine decay testing and detailed chlorine decay modeling could not be conducted (due to difficulties determining and validating key input parameters such as organic matter concentration), which is acknowledged to result in uncertainty in the model results, potentially leading to underestimation of the decay rate.
Design of training/educational material package
The importance of training, education, and capacity building in the success of WaSH programs has been highlighted by many previous studies and organization, including the United Nations Development Program, which is working in ∼170 countries to achieve the SDGs. As such, the team developed a series of support materials, including a Household Information Package, aimed at capacity building, including instructional stickers, a booklet, and a video, which were provided to the community during and following the pilot program, outlined below. Six different poster designs outlining the reasons for, and methods of, periodic tank disinfection and maintenance were created and printed on nylon sticker sheets. The stickers used clear and simple language and imagery to demonstrate what chlorination is designed to achieve, and how it can be conducted effectively. The sticker text was refined using the “Up-goer five” text editor as a tool to ensure clear and recognizable language. The tool restricts users to the 1000 most commonly used words in the English language, aiming to facilitate communication of potentially complicated ideas in as simple language as possible. Habyarimana and Jack (2015), highlighted the effectiveness of stickers of this kind in a road safety campaign in Kenya.
The video (https://www.youtube.com/watch?v=0nzpKWo44B0&feature=youtu.be) was produced using footage filmed during the site visit(s), ensuring all concepts shown and explained could be readily related to the local infrastructure and conditions. The video demonstrated the procedure for determining the appropriate chlorine dosage, including estimation of tank volume, measurement of the required volume of hypochlorite solution, and mixing of the solution in the tank—activities which were conducted with the participation of community members during the pilot. The educational materials were extensively prototyped and modified throughout the project, incorporating community input before and during the pilot, aiming to maximize their clarity, effectiveness, and suitability to the local culture.
Pilot disinfection program implementation, validation, and dissemination
The pilot program involved trials of disinfecting rainwater tanks using sodium hypochlorite and routine tank maintenance activities (e.g., gutter cleaning). The pilot also involved validation that the chlorination was effective at removing bacterial contamination, and community prototyping of the training/educational materials. The pilot was limited to the community of Mau'ira, as the research team had established a close relationship with community leaders, and the community requested involvement in a program of this kind.
The pilot was rolled out during further site visits. Initial dosing of one household 5200-L tank (asset ID: RW202) whose owners volunteered, took place in July 2019 by adding 12.5% sodium hypochlorite in the appropriate volume—based on the model and on-site assessment of tank water level—to achieve a chlorine residual within the WHO target range (initially, this could not be verified on site as suitable testing equipment was not operable). Dosing was conducted by a team of engineers visiting Mau'ira after being briefed and trained by the research team before departure. Following this, dosing of the large communal village rainwater tank (asset ID: RW201), and a further five individual household above-ground rainwater tanks (RW206-210) at the request of the owners was conducted in September 2019; the sample locations are shown in Fig. 3. Crocker et al. (2017) found that outcomes in community-led total sanitation interventions were more sustainable in a supportive enabling environment where sufficient follow-up visits were conducted and as such further visits to the communities are planned.
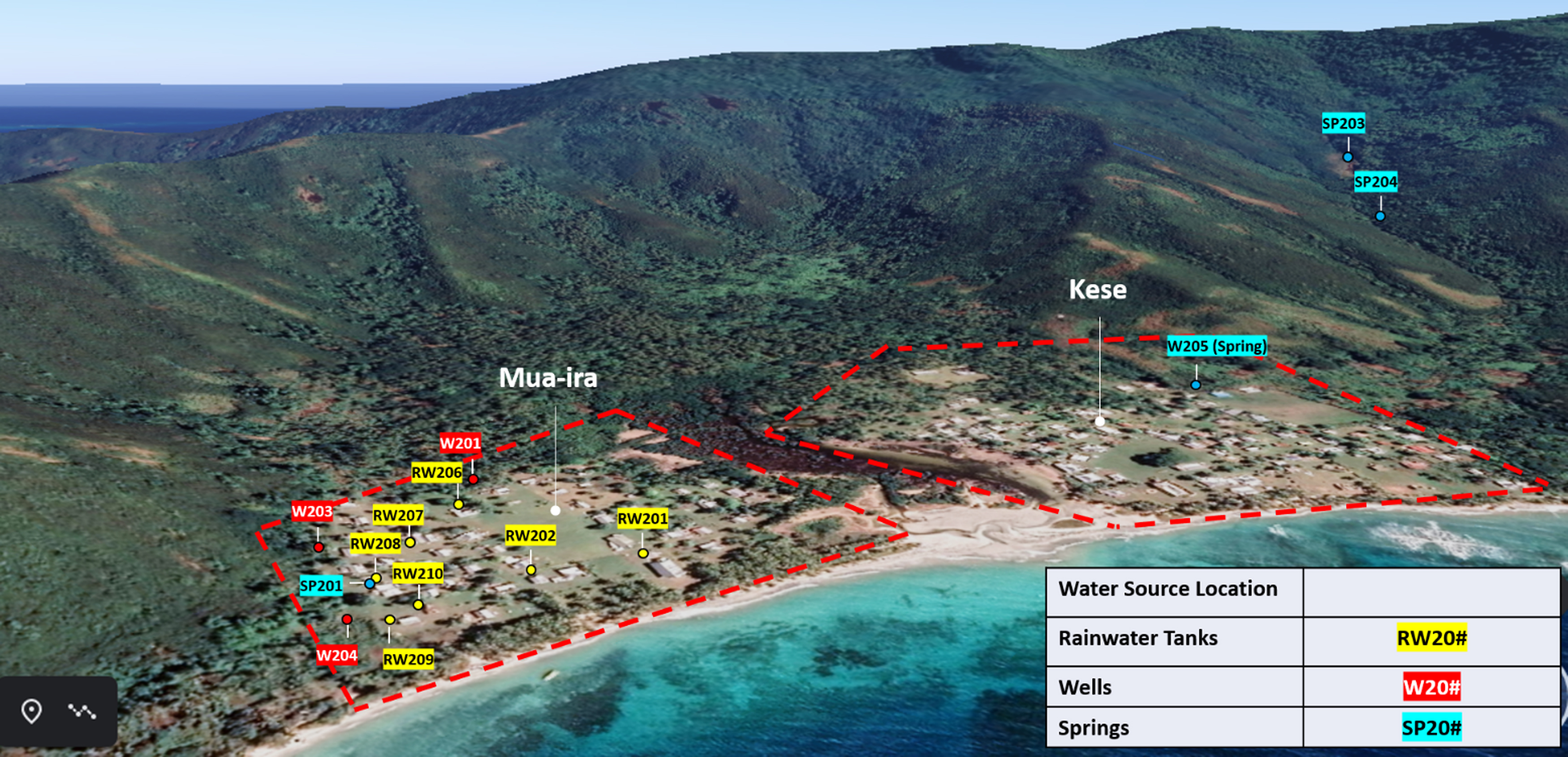
Sample locations in Mua'ira and Kese.
Validation of the effect of the chlorination was achieved by:
Retesting the tank water after periods of time ranging from ∼2 days to 2 months for E. coli, using the CBT Kits (for comparison with the prechlorination E. coli results);
Testing the free and total chlorine concentrations of the tank water, using a portable HACH DR300 pocket colorimeter at different time intervals following chlorination (Table 4).
The ultimate project goal and subsequent processes and actions were developed using a Theory of Change approach (Allen et al., 2017). The framework in Fig. 4 demonstrates how the ultimate project goal of healthier communities will be achieved through the proposed key actions in this study.

Overview of proposed actions working toward overarching goal of the project.
Results
Drinking water source data
Water quality results for E. coli from the April-May 2019 site visit (taken on April 24, 2019), before the chlorination pilot, are summarized for Mau'ira and Kese in Table 2 (additional samples taken from other communities in the region, including Soso and Namara are reported in Appendix A1). Sample locations are shown in Fig. 3. Consistent with the results of Otley et al. (2018) and community opinions on the degree of safety of different water sources, all wells in Mau'ira and Kese were contaminated with the maximum quantifiable level of E. coli (MPN of >100 organisms per 100 mL). Contrary to community expectations, all spring water samples from the gravity-fed supply (including the sample from close to the spring's most elevated outlet) also exhibited MPN values of >100 per 100 mL. Consistent with community expectations, rainwater tanks in Mua'ira showed the lowest degree of contamination, but nonetheless showed evidence of significant bacterial contamination with MPN values ranging from 13.6 to 48.3 per 100 mL.
Mau'ira and Kese E. coli Results—April 2019
Asset ID convention: W = well, SP = spring, RW = rainwater tank, DL = instrument detection limit.
Water quality data pre- and postchlorination pilot program
The chlorine dosing pilot covered seven above-ground rainwater tanks in Mau'ira (one communal RW201, and six household RW202 and RW206-210); tank locations are shown in Fig. 3. All postchlorine dosing E. coli sampling was conducted during the September 2019 site visit (September 11, 2019). Prechlorine dosing sampling was also completed immediately before the chlorine was added, generally 2 days before the postdosing sampling (Table 3) with the exception of RW201 and RW202 (see below). These results are shown in Table 3.
Recorded E. coli Levels Before and After Chlorine Disinfection of Rainwater Tanks in Mua'ira
An administrative error meant that the prechlorine dosing reading for RW210 could not be used as part of the analysis, however, the tank was dosed, and no E. coli were detected in the test conducted 2 days later. In all tanks tested during the September pilot disinfection program, dosing with chlorine resulted in a decrease in the E. coli levels to zero, observed 2 days following the dosing. A tank, which was dosed 4 days earlier than the others (RW201), also recorded a MPN of zero 6 days after dosing. One of the tanks (RW202) was presampled and dosed by the collaborating research team in the July 2019 visit, at the request of the household. The effect of dosing was in this case assessed in the September 2019 visit, following a period of ∼2 months. At this time, the tank recorded an MPN of 48.3 and was found to be close to empty. It was determined from discussions with community representatives that due to this tank being the first to be disinfected, people had preferentially accessed this tank for drinking water, leaving it vulnerable to depletion.
Tank volume and chlorine residual modelling
A contextualized model was developed to first determine the extent to which rainwater tanks could provide sufficient volumes of household water and second to determine the influence of dosing these tanks with sodium hypochlorite at different times of the year on the likely length of disinfection. Based on the developed model, it was estimated that according to 1971 to 2000 and 2014 to 2016, rainfall data from Nadi (from the Fiji Meteorological Service: https://www.met.gov.fj/), it should be possible to supply drinking water through the rainwater tanks throughout the year; however, during years of below-average rainfall (e.g., 2015), the tanks would fail to supply drinking water for between 2 and 27 days, depending on tank dimensions and roof area. Anecdotal evidence from the communities indicates that currently, rainwater tanks become empty for longer periods than is indicated by the modeling during the dry season. This is potentially due to lower rainfall in the Yasawa Islands compared with Nadi, where the nearest detailed rainfall data were available. Furthermore, all villages were anticipated by the model to have extended periods (96 or more days), during which water supply levels drop below 50% of community requirements. This indicates that while there is potential to meet a substantial component of drinking water needs using the rainwater tanks, additional/alternative safe drinking water supplies should also be investigated and secured (a topic for future research and investigation).
The developed model also provided results pertaining to the likely frequency required, and optimum dates for dosing rainwater tanks to achieve a chlorine residual within the WHO recommended level (0.2–5 mg/L). As shown in Fig. 5, multiple dosing events are likely to be required in a typical year to maintain a residual concentration in this range. It is also noted that the rate of decay in the model likely under-estimates the true decay, as chemical decay (influenced by temperature, pH and organic matter) was not incorporated. Notwithstanding the limitations, the model indicated that dosing during the early stages of the wet season (e.g., December) is only effective for a short period of time (less than 2 months), whereas dosing at the end of the wet season (e.g., late April) will likely result in a chlorine residual within the target range for considerably longer periods. As such, targeting this period (which approximately coincides with Easter, one of the major cultural events in the Fijian calendar), was thought to be an effective approach, and this was communicated in the developed training package. A combined approach involving cleaning tanks before the onset of the wet season, and dosing with chlorine before the onset of the dry season (e.g., Easter), was on this basis recommended to community as an effective starting point for maximizing bacteria-free drinking water supply in the tanks (with additional dosing events and maintenance, further increasing the chances of bacteria-free water throughout the year).

Model output showing typical tank storage level and chlorine residual in Mua'ira (using average rainfall data from 1971 to 2016 collected at Nadi), when dosed with chlorine in late April, at the end of the typical wet season. Note that modeling during drier years (such as 2015) resulted in extended periods in which the tank(s) ran out of water.
Validation of chlorine residual data
Free and total chlorine results for the rainwater tanks measured before, immediately after, and ∼48 h after dosing with chlorine are shown in Table 4. In general, while some free chlorine persisted in the tank water 48 h after dosing, this rapidly declined in the first 48 h, and the concentrations at this time were below the minimum recommended chlorine residual of 0.2 mg/L. This indicated greater volumes of sodium hypochlorite than were initially determined using the developed model are likely to be required to achieve and maintain a residual within this range for an extended period. Further community consultation regarding some of the common issues associated with chlorination (e.g., odor and taste of the water) and assessment of potential side effects (e.g., generation of disinfection by-products) are deemed necessary before dosage in higher quantities is implemented on an ongoing basis. These results, and additional data collected as part of ongoing work, will be used to refine the rainwater model until it can be validated for site conditions. The validated model will be used to determine the likely influence of variables on the supply and quality of household water. These variables could include changes to rainfall, changes in household water use and changes to the delivery of barged government water.
Free and Total Chlorine Measurements in Rain Tanks Before and After Pilot Dosing
Discussion
Safety of drinking water supplies and effectiveness of chlorination pilot
When compared against the WHO's guidelines (Table 2), the sampling and analysis program identified that all water sources currently available in the communities were exposing people to a high level of health risk (Table 3). This included the rainwater tanks, although the health risk was generally lower for these than wells and spring water.
Current unimproved community sanitary practices include the use of unlined drop latrines and basic household “septic tanks” (constructed using old fuel drums), which are likely responsible for the high level of fecal contamination in the sampled wells. This is a common cause of bacterial contamination of shallow domestic wells and springs in many global settings (e.g., Arwenyo et al., 2017; Ngasala et al., 2019). These wells are shallow (no more than 4 m deep) and in proximity—mostly within 30 m, and in some cases within 10 m—to many of the latrines, known to be a high-risk factor for pathogenic contamination of groundwater sources (Sphere, 2018). The wells and latrines are dug within high-permeability sand deposits, hence, there is likely direct connectivity between latrine effluent and the wells through flow in the surficial aquifer from which they draw water. The high E. coli levels suggest minimal or no attenuation of contamination between the latrines or septic tanks and wells. The humid conditions and lack of covering on the wells also likely enhance the growth of bacterial colonies (e.g., Elisante and Muzuka, 2016).
Springs that supply water for the villages of Mua'ira, Kese, and Namara also tested positive for the maximum level of E. coli contamination, somewhat contrary to expectations. The springs were flowing at a high rate (>20 L/s) at the time of testing. It is hypothesized that animal feces, for example, from wild goats and pigs common in the mountainous area surrounding where the springs emerge, are impacting the water quality, due to lack of any source protection measures (e.g., fencing), as has been documented in other settings (e.g., Ministry of Health, 2014; Gwimbi et al., 2019). Anecdotally, the flow rate of the springs is highly seasonal (reverting to minimal or no flow during the dry season), indicating the springs are predominantly fed by recent rainfall and that there is a short water residence time within the springs' source aquifer. This indicates there may be potential to achieve relatively rapid improvement in spring water quality by initiating source protection measures within the surrounding catchment. This is suggested as a topic for future research and community consultation.
The possible pathways of rainwater tank contamination with fecal matter include the incorporation of animal excrement from rooftops, preexisting bacterial colonies present on equipment surfaces (taps, pipes, etc.) and/or crosscontamination, such as during cleaning or filling of the tanks with other water sources (to increase supply during times of water shortage) (Gwenzi et al., 2015; Bae et al., 2019; Senevirathna et al., 2019). Many of the rainwater tanks tested within this study had been installed for less than 1 year, indicating that the contamination is recent and/or ongoing.
Following chlorination of the rainwater tanks, the CBTs showed that E. coli were absent and thus fecal contamination had likely been effectively neutralized (acknowledging that chlorine is ineffective against certain water-borne pathogens)—for example, the tank water fell within the “Safe” health risk category according to WHO (2011) guidelines (Table 1). The results of the pilot thus indicated that simple periodic chlorination is an effective disinfection strategy. It is currently unclear for what duration of time this strategy is effective, and the results of just the tank that was subjected to early chlorination (RW202) indicated that after a period of ∼1 months, fecal matter contamination was once again present. Further investigation is required to understand if the preferential use of RW202—the first chlorinated water source in the community—leading to near depletion, influenced the lower-than-expected disinfection time. Ongoing work is monitoring the E. coli levels in the other five pilot rainwater tanks to give a more comprehensive understanding of expected disinfection time with recommendations for dosing strategy updated accordingly. The field-based free chlorine testing also indicated a relatively rapid decline in chlorine residual even 2 days after treatment. This indicates that:
A relatively regular program of chlorination of this kind will be required to maintain disinfection;
complementary measures such as ongoing tank and roof cleaning and maintenance are required to reduce source contamination and thereby enhance the effectiveness of chlorination;
slower release forms of chlorine may be a more effective alternative than traditional sodium hypochlorite (although such products may be more difficult to source locally).
Ongoing work is aiming to test and implement these strategies and secure a reliable source of chlorine (or alternative/additional disinfectant) for the communities.
Capacity building and education
During community engagement in Mua'ira, individuals from the households where rainwater tanks were tested, were provided with a range of sticker designs, explaining the benefits of chlorine disinfection and methods of dosing and cleaning tanks and associated infrastructure. Figure 6 shows the design of the most favored option, which was selected by most of the participating households to stick on the outside surface of the tanks. These materials were included alongside the Household Information Package and video providing more detailed information and instructions.
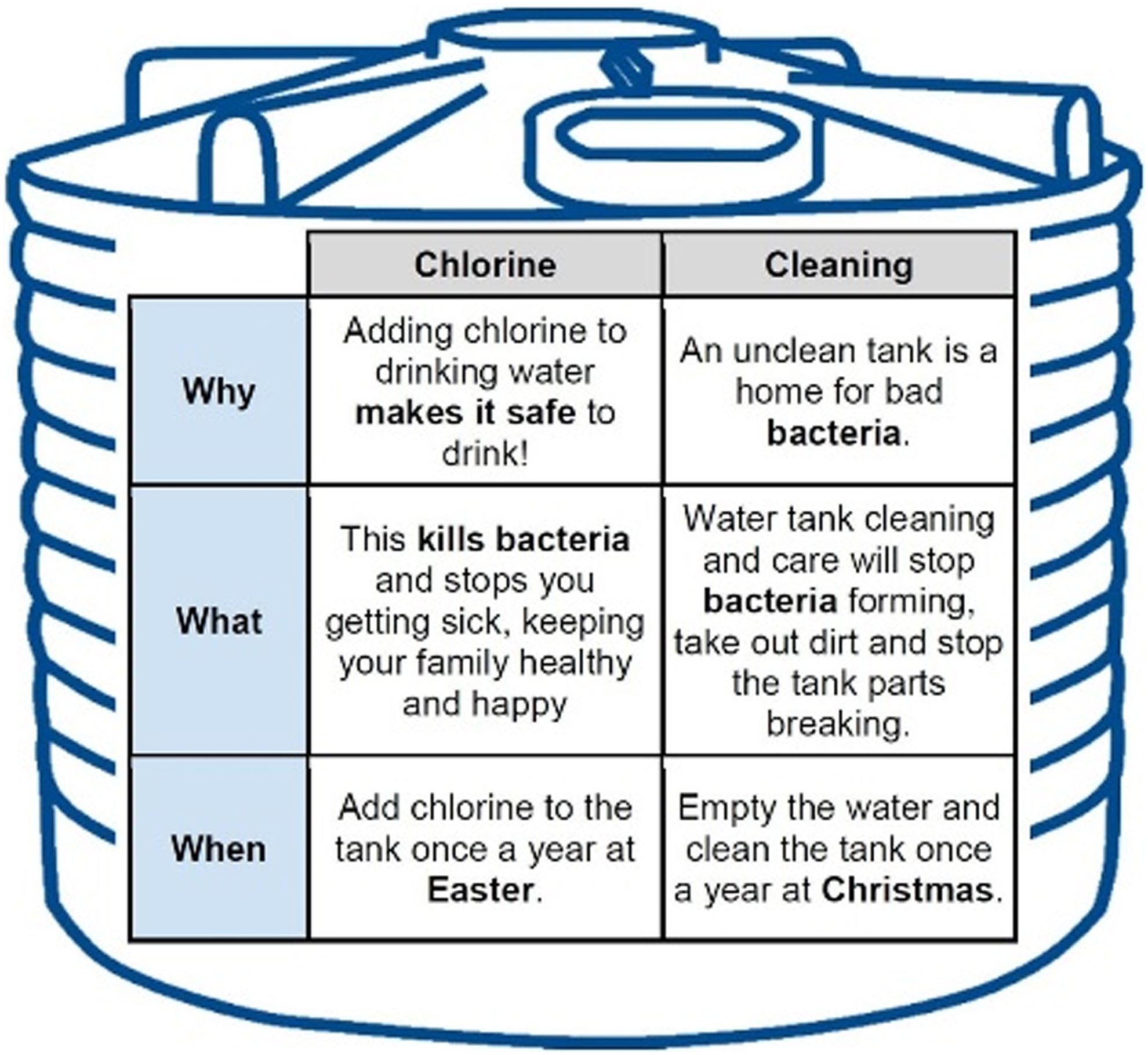
Design of the most favored rain tank sticker, explaining ‘why, what, and when’ tank disinfection and cleaning are important.
In addition, community members were encouraged to become involved in the pilot, initially through observation and later participation in the key tasks, such as determination of appropriate chlorine doses, adding chlorine to the tanks and mixing it throughout the tank (Fig. 7) as well as gutter and pipe cleaning activities. We consider these valuable experiences which have the potential to enhance the communities' sense of ownership and participation in the program, and ultimately hope this can lead to ongoing development of skills and actions within the community to improve the safety of drinking water supplies. The focus on capacity building aims to mitigate some of the problems associated with many western sponsored WaSH interventions highlighted by (for example) Donnelly (2010) and Marshall and Kaminsky (2016). In collaboration with community, educational materials will be updated based on user feedback and changed dosing recommendations as part of ongoing work.

A resident of Mua'ira mixing chlorine throughout their household's tank; note the instructional sticker at eye level above the outlet (Image source: Nick Lowe, 2019).
Future research and follow-up
There are currently several uncertainties regarding the likely effectiveness of the pilot program and other activities conducted by the team, in achieving the ultimate goal of improving community health outcomes through enhanced access to safe drinking water (Fig. 4). These include:
It is currently unknown whether and to what extent a program of rainwater disinfection and tank maintenance such as our pilot will lead to improved health outcomes (e.g., reduced exposure to pathogens and fewer cases of gastroenteritis). There are plans to investigate this question through ongoing liaison with the staff at a local health clinic in Kese (who have been periodically recording or estimating the number of cases of gastrointestinal illness in the communities Mua'ira and Kese). A water quality database, recording the results of any testing for E. coli and related parameters has also been developed with the intention of monitoring change in the quality of drinking water sources over time (e.g., allowing assessment of the effect of the pilot and subsequent follow-up activities on water quality);
It is unclear to what extent the educational and capacity building activities conducted by the team have led (or will lead) to improved understanding of the steps that can be taken to enhance drinking water safety, or whether they will increase levels of ongoing participation in such activities independently of the research team and other partners (e.g., NGOs) involved with the communities. It is intended this will be gauged through follow-up visits being planned;
The degree to which the relatively newly installed rain tanks can meet drinking water needs on an ongoing basis (including accounting for climate change and variability) is uncertain. While our model, and anecdotal accounts provide some indication, future monitoring and research into the number of days in which community members have no choice but to access alternative, less safe water sources is required. Currently, emergency water is delivered to Yasawa Island communities through a Fiji Government-owned boat on an ad hoc basis (e.g., in response to reports of extreme water stress from communities to the government). While this is vitally important to address critical water shortages in the short term, the continued sustainability of this approach must be considered carefully, in consultation with the communities.
Conclusions
The results obtained from this study support a hypothesis from Otley et al. (2018) that the water supply is contributing to fecal/oral disease transmission and impacting the health of people in Yasawa Island communities. Detection of E. coli contamination indicated that drinking water sources in Mua-Ira, Soso, Kese, and Namara communities were above the WHO (2011) drinking water guidelines, prompting chlorine-driven disinfection. Following a rainwater tank disinfection trial in Mua-Ira village, chlorination proved to be successful and community rollout was initiated. Point source addition of chlorine in household rainwater tanks, paired with tank and gutter maintenance, has been recommended to community and other key stakeholders to minimize pathogenic bacterial contamination in drinking water sources. Continuation of chlorine disinfection will require appropriate management methods and follow-up actions. This will be encouraged by capacity building and education, utilizing the provided materials and methods demonstrated to the community and the strong relationship between communities and local partner Barefoot Resorts.
As an important long-term project for the improvement of public health through securing and maintaining a safe drinking water supply, ongoing monitoring and evaluation of the implemented solutions will be vital. This may then provide data and insights which can be used to assist in the design and implementation of other drinking water safety interventions throughout the Yasawa Islands and other Pacific Island Nations.
Footnotes
Acknowledgments
The authors would like to thank Tai Semisi, Sami-soni, Q'oro, Rusiate, Ronnie, Tiu, Taro, Sobby, and the community leaders for welcoming them into the Mua'ira community. The families of Mua'ira who took part in the tank chlorination trial and codeveloped material to ensure effective project development. They also acknowledge Peter Farrell, Gareth Van Eyssen, Rob Macfarlane, and the entire Barefoot Collection staff for making this project possible and making their stay very welcoming. Additional thanks to the RMIT students who helped them with this project through testing, data collection, and fieldwork assistance.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.