
Abstract
Purpose:
To maximize retention of participants in a longitudinal cohort study, we sought to understand young peoples' views about barriers and facilitators to continuing study participation.
Methods:
Ten young people with a previous cancer diagnosis aged 15–24 participated in a 1 day workshop. The workshop used participatory methodology consisting of three exercises as follows: role play/scene setting; force field analysis of research participation in small groups; and focus group discussion. A final prioritization exercise was administered individually after the workshop.
Results:
Twenty-four barriers to maintaining participation were summarized in five themes as follows: life commitments; concerns specific to the study; emotional barriers; practical barriers; and other reasons. The top 3 specific barriers were as follows: not a priority/other things are more important; too time consuming; and forgetting/memory. The top 3 facilitators for participation were as follows: wishing to help other young people; giving back to the cancer community; and honoring an initial commitment to participation. The top 3 suggested solutions to encourage continued participation were as follows: reminder text message or email before each survey to check preferred method of delivery; breaking up the online survey into modules to make completion less overwhelming; and consolidation of study information in one location.
Conclusion:
Involving young people in designing a retention strategy for young people with cancer has informed the BRIGHTLIGHT retention strategy. Patient and public involvement is imperative for successful research but measuring impact is challenging. The success of implementing the changes to optimize retention was shown in the increase in retention in Wave 3 from 30% to final participation of 58%.
Background
T
As such, two key factors are judged to be necessary for successful cohort studies these are: initial recruitment of participants to establish the cohort and then subsequent retention throughout the study period. Many recommendations have been proposed to improve recruitment and retention6,7 and they are often discussed as similar entities, but in practice require different approaches to achieve success. Notably, recruitment is often led predominantly by recruiters such as healthcare professionals in multiple participating institutions, who may act as gatekeepers to potential patients8–10 in contrast to study participant retention where the core research team is likely to have the leading role.
Cancer patients are reported to be highly motivated to join research studies. 11 Although motivation levels may be high at the outset of study participation, motivation may not be maintained, resulting in attrition of study populations.6,7 The loss of subjects may increase research costs, threaten validity of results, and delay or prevent meaningful outcomes. 12
Retention strategies are therefore desirable to maintain participant engagement. Reviews of retention strategies for cohort studies 7 and clinical trials 6 consistently found incentivization to be the most effective retention strategy. Most cohort studies reporting use of incentives are from North America or, if the studies were based in United Kingdom, involve nonhealth populations. 7 Regulatory processes for health research in the United Kingdom do not easily permit incentivization as it is viewed to be potentially coercive. 13 An additional challenge for retaining young people in research is accommodating their unique psychosocial needs and life stage commitments, which create specific challenges to research participation. This must be taken into account in the design and conduct of research with young people.2,11,14
BRIGHTLIGHT (NIHR RP-PG-1209-10013) is a national longitudinal cohort study evaluating specialist cancer care for young people aged 13–24 years.15,16 The study follows young people aged 13–24 at cancer diagnosis for 3 years and data collection occurs over five times points15,16 (www.brightlightstudy.com). Young people have been integral to BRIGHTLIGHT; before funding young people were involved in the feasibility work,17,18 helped implement the protocol,15,16 and advised on study related issues 10 and readers are referred to our publications.10,15,16 BRIGHTLIGHT aimed to recruit 2012 young people over 18 months and while a number of strategies were used to optimize recruitment,10,19 it was below the anticipated target of 2012. A number of barriers existed to recruitment 10 but study uptake was higher than anticipated (80% vs. 60%) and retention at Wave 2 an impressive 69%. However, we noted early on that uptake at Wave 3 was not in parallel to Wave 2 retention figures, and therefore, we decided to review our retention strategy so we could implement prompt changes.
From the outset, our retention strategy was developed based on recommendations derived from the literature and from our experience of working with young people and specifically what young people had told us during feasibility and set up of BRIGHTLIGHT.15,16 Table 1 illustrates the retention strategies we adopted and why we felt they were particularly relevant for our population. Having identified that typical recruitment strategies may be less effective for young people, 10 we recognized the importance of examining their unique needs to maximize retention and felt that young people themselves were best placed to describe these to us.
Ipsos MORI is the commercial research organization who administers the BRIGHTLIGHT survey.
The BRIGHTLIGHT Young Advisory Panel (YAP) is a group of 20 young people convened to work alongside BRIGHTLIGHT researchers to optimize study design and delivery. They will also play a pivotal role in dissemination (www.brightlightstudy.com/event/november-2014-brightlight-update-at-fysot).
Aim
To maximize retention of participants in a longitudinal cohort study, we wished to understand young peoples' views about barriers and facilitators to continued study participation.
Methods
Participants, setting, and recruitment
Data were collected from a workshop held in a nonclinical venue attended by members of the YAP.10,15,17 The workshop was advertised on the YAP Facebook page and by newsletter sent to the BRIGHTLIGHT Cohort of ∼950 young people. Having members of the YAP who are and are not in BRIGHTLIGHT has been invaluable for acquiring the opinions of those presented with a hypothetical scenario, as well as those in the study. Being able to seek the advice from young people nationally has the added benefit of ensuring national representation, as well as a range of ages, cancer types, and experiences of care. In line with national guidelines for user involvement in the United Kingdom, the YAP received a £30 voucher. Travel costs and refreshments were also provided.

BRIGHTLIGHT wristband “reward” for participation. Young people were rewarded with BRIGHTLIGHT wristbands following completion of each wave of data collection. (Photo produced with permission from James Shaw.)
Twenty-three young people expressed interest in attending the workshop. Of those, 10 young people attended, median age 21.5 (range 15–25) years, 6 female, and 4 male. Young people were diagnosed median age 20 (range 13–23) years with Hodgkin lymphoma (n = 5), osteosarcoma, acute myeloid leukemia, testicular, brain, and thyroid cancer. Three were still on treatment. Two researchers (L.A.F., R.M.T.) and one Teenage and Young Adult cancer nurse (S.L.) facilitated the workshop.
Ethics
BRIGHTLIGHT is approved by an NHS Research Ethics Committee. Before the workshop, participants were sent information about the day. Written consent was obtained from all attendees after a detailed description of what the day would entail. Young people were made aware they were free to leave the workshop at any time. After the workshop, each young person was contacted by a member of the research team to ensure the workshop had not resulted in any distress.
Workshop format
Using established formats,10,15,17 young people were given an opportunity to get to know each other before commencing activities. The day was structured around three exercises to explore retention of study participants specifically at the fourth and fifth waves of data collection, when young people are 2 and 3 years after diagnosis. The day was interspersed with short breaks and time for individual reflections.
Exercise 1: role play and presentation
The study team reenacted a stakeholder meeting held among the research funder, the chief investigator, and work stream leads. The purpose of this scenario was to convey the discussions and questions asked by the funder on the progress of the study so young people would be aware of the importance of recruitment and retention (Table 2). Simultaneously, it provided an opportunity to update the workshop attendees of the research objectives and how their previous involvement had impacted change.
The stakeholder is the funder of BRIGHTLIGHT: The National Institute for Health Research.
YAP, Young Advisory Panel, the BRIGHTLIGHT patient user group.
A slide presentation was used to present the study structure, photographs, and results of previous workshops involving young people (www.brightlightstudy.com/user-involvement), including actions taken on their previous recommendations.10,17 A short discussion was then held to address any questions from the YAP. This allowed the research team to reinforce the objectives of the workshop and ensure young people were clear what their involvement would entail and how it could contribute to improving the study.
Exercise 2: force field analysis
Young people worked in small groups to consider barriers to survey participation and possible approaches to overcome these. The study team utilized a decision-making tool named “Force Field Analysis,” commonly used in business, to list, discuss, and consider variables for and against implementing change. 20 It is a systematic and transparent model made up of three stages as follows: evaluation function; analysis function; and project planning, useful for identifying “restraining” and “driving forces.” Groups were instructed to consider the restraining forces which would limit young people's participation in the study and the driving forces which would include their motives for continuing. The groups were asked to consider both sets of variables and then suggest interventions or solutions that the study team could adopt.
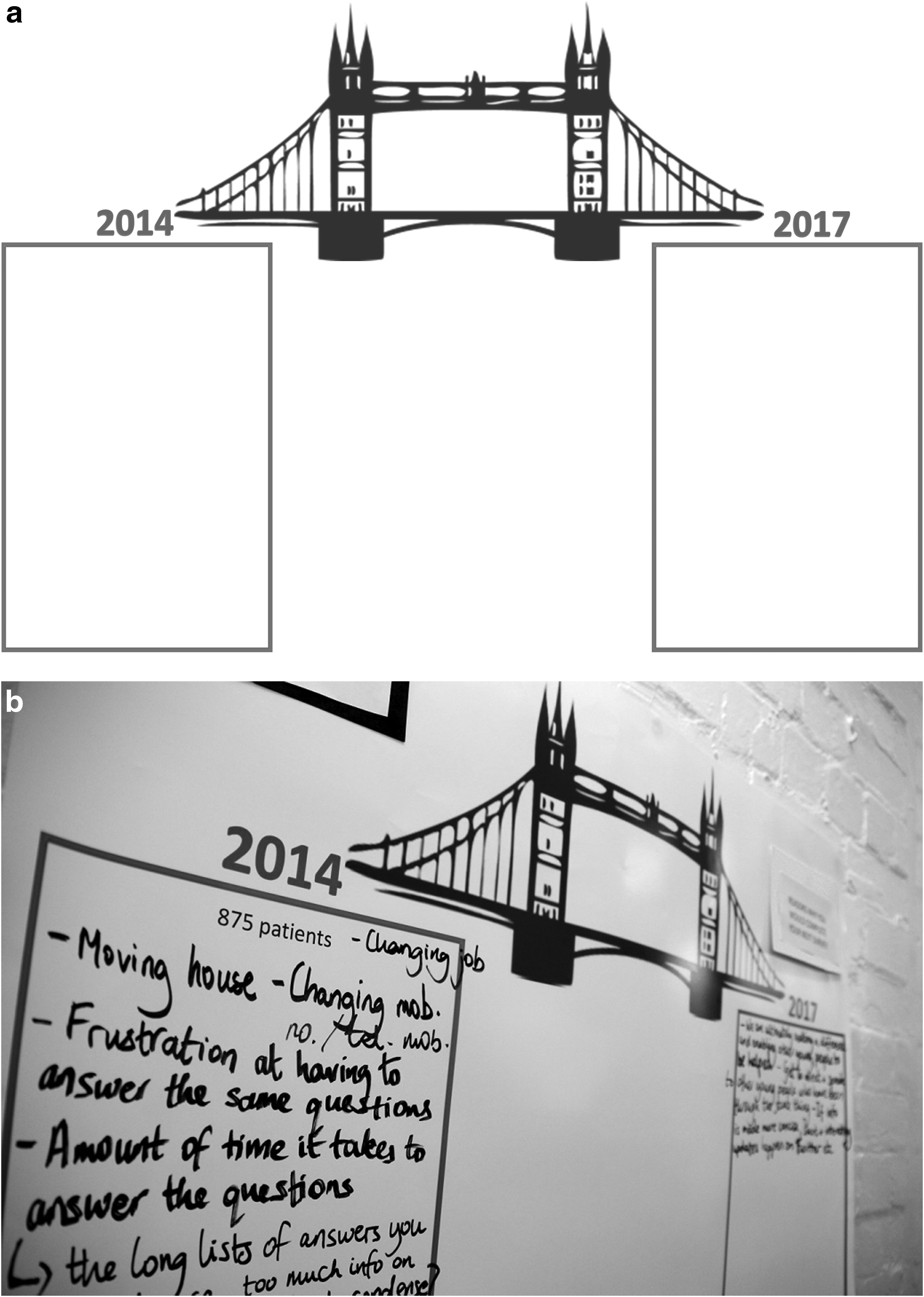
Groups were provided with a large poster of a bridge used to represent two time points of the study, 2014 and 2017. Within the 2014 box, groups were asked to list the restraining forces that may limit their participation in future surveys. Similarly, in the second box representing the end point of data collection in 2017, groups were asked to list reasons which would motivate young people to complete all or most of the surveys (Fig. 2a). Finally, the space in the middle was used to list the interventions that might support the “crossing of the bridge” successfully from 2014 to 2017. The concept of a “bridge crossing” was used in a previous workshop and found to be easily understandable by young people and so was adapted for this study. 15 Following this activity young people reconvened to feedback their results and comment on the results of the other groups.
Exercise 3: BRIGHTLIGHT online presence
We sought feedback from participants on the content and structure of the study website. Our earlier work highlighted the benefit of a website to engage study participants, 10 and the BRIGHTLIGHT website is the primary method of communicating both with young people and other stakeholders. However, concerns had arisen about its appearance and content.
On a large screen a researcher presented the current website. Groups were given laptops and asked to look at websites they often visited. We provided a list of questions to help list appealing features such as branding and navigation (Box 1).
Question Prompts for the Young People to Consider When Discussing the BRIGHTLIGHT Website
The participants were asked to select three websites they liked and discuss in their groups how the BRIGHTLIGHT website could be improved. The groups reconvened to feedback their discussions and also offered individual reflections of the current website and which features should be enhanced or new items introduced to improve its value.
Results
Exercise 1: role play and presentation
An interactive discussion followed the role play and after the presentation few questions emerged about the study. It was apparent that most young people had a good understanding of BRIGHTLIGHT, including its objectives and the importance of recruitment and retention.
Exercise 2: force field analysis
Young people discussed and listed potential reasons for attrition during study progression, reasons for continuation, and finally, how the study team could implement strategies to improve retention (Fig. 2b and Table 3).
Barriers to participation
Young people discussed several reasons why those in the study may not continue with subsequent stages of the study. Five themes emerged as follows:
(1) Life commitments, for example, school or work and more important/pressing things to do (2) Study specific barriers, for example, no incentives, repetition, and too time consuming (3) Emotional barriers, for example, unwillingness to revisit cancer experience and not wanting to talk about issues (4) Practical barriers, for example, changing telephone number and moving house (5) Other reasons, for example, memory and physical health
Reasons to continue
Reasons to continue with the study stemmed mainly from the discussions the YAP had about the benefits of BRIGHTLIGHT to the wider young cancer community. They perceived this as one of the most important reasons for the Cohort members to continue with the surveys as participation could help influence Teenage and Young Adult (TYA) cancer care. This notion of helping other young people with cancer was a recurring reason which presented in a number of ways, for example, “prevent others from a bad experience” and “making a difference and enabling others to be helped.”
Another common reason for continuation with the study was for the personal sense of achievement it would bring to those completing BRIGHTLIGHT and the commitment they had shown over the course of the study (Table 3).
Interventions to facilitate continuation
By considering both the list of barriers to participation and reasons to continue, the YAP proposed practical solutions, including using a wider range of engagement and interaction methods with the Cohort, for example, Instagram. Among this list were changes such as shortening the lengthy correspondence, which invites participants to the next survey (Table 3). The Group also suggested sending out retention postcards on emerging results, an example can be seen in Figure 4.

Example of a postcard sent to young people containing emerging results.
Exercise 3: methods to engage study participants
The groups reflected on the current website and how this could be improved to better appeal with the Cohort. The recommendation for a complete website redesign was unanimous. Collectively the group felt that the existing design and “feel” of the website did not attract young users and should adopt a less text-heavy and “fresher” look. As young users they felt most information they wanted should be kept short and easily available through simple navigation instead of being spread across different pages. The video information on the current website was well received and was a preferred method of relaying information in place of text.
Postworkshop consultation
After the workshop, we sought feedback from the user panel by an online survey. This enabled the research team to collect individual reflections of the force field activity and get young people to independently rate their top 3 barriers, facilitators, and interventions the study team should consider adopting to optimize retention.
The top 3 barriers were as follows:
(1) Not a priority/other things are more important (n = 6; 20%) (2) Too time consuming (n = 5; 16.7%) (3) Forget/memory (n = 5; 16.7%)
The full list of options can be seen in Figure 3.
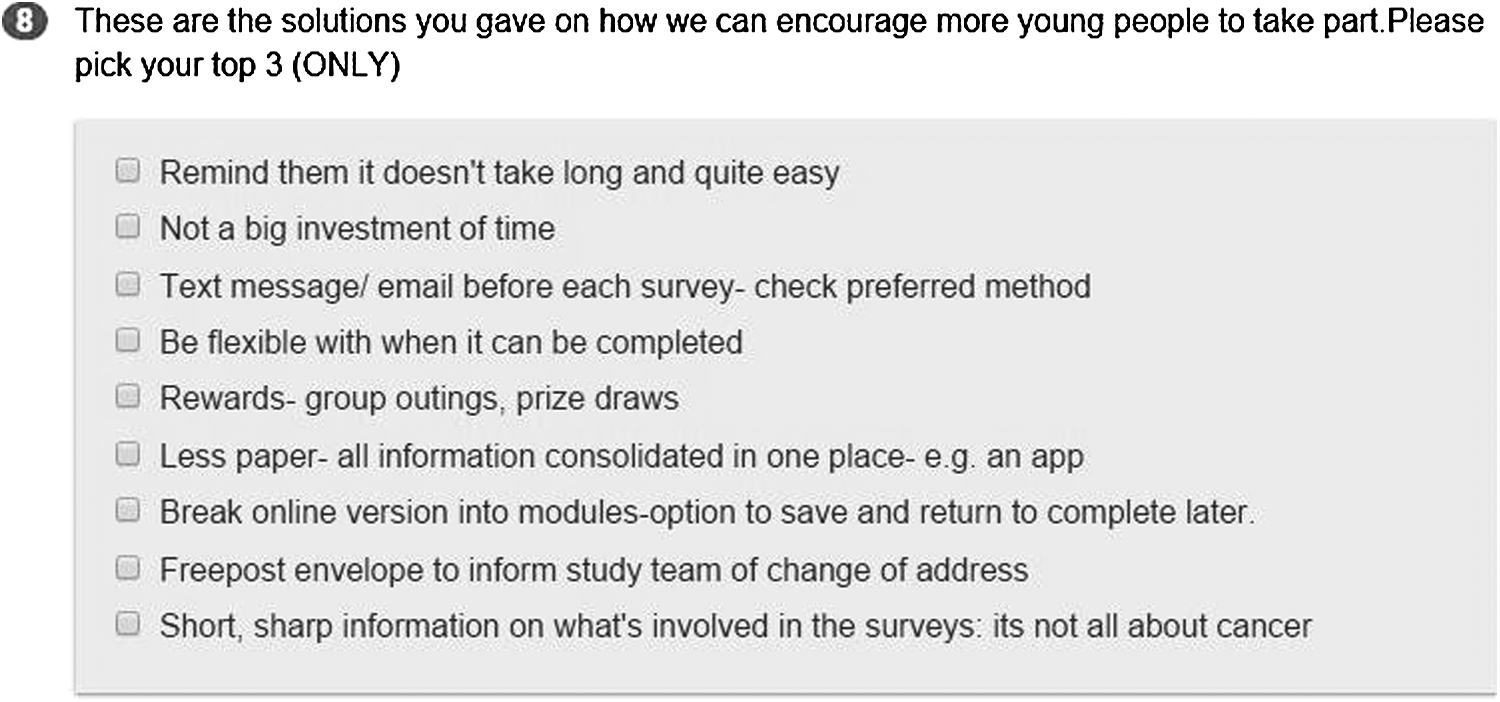
Question from the online survey to gather independent reflections of the three most suitable solutions to retention.
From this task it emerged that the three most frequently ranked reasons to take part were helping others (n = 6; 26.7%), giving back to the cancer community (n = 5; 16.7%), and commitment (n = 4; 13.3%). The three most highly ranked solutions to increase retention composed of a reminder text or email before each survey to check preferred method of delivery (n = 7; 23.3%), followed by breaking up the online version of the BRIGHTLIGHT survey (main method of data collection) into modules to make completion less overwhelming (n = 7; 23.3%), and for all information to be consolidated in one place online, for example, in an app (n = 6; 20%). Feedback indicated that the activities enjoyed most by the group included the bridge activity, followed by the opportunity to provide input into the website, and finally, meeting other young people.
Discussion
To our knowledge this is the first time young people with cancer have been actively consulted to assist in the development of a longitudinal study retention strategy. While the majority of the results supported existing recommendations6,7,14,21–25 and had already been implemented in BRIGHTLIGHT, confirming acceptability and preferences of young people is important to identify where resources should be targeted to optimize retention. Based on the workshop a number of changes were made to our existing strategy (Box 2).
Summary of Changes Made to Optimize Retention
The most common solution to improve retention was text message/email before each survey. As shown in Table 1, contact before each wave of data collection was already used. This is a combination of postal notification and email depending on young people's preference. As the study progressed and young people are 2–3 years postdiagnosis, we identified the challenge of keeping track of young people as they moved on from their cancer treatment back to work, college, and university. Even with prompts, young people rarely updated us with their change of address and we were dependent on their secondary care providers to keep us informed of change of address. However, within 2–3 years following diagnosis many young people often had minimal contact with their cancer inpatient team leaving us to rely on their primary care providers. Young people represent the most mobile populations in the United Kingdom 26 so often they had moved and/or changed their primary care provider. We were therefore unable to check if young people were still alive and send them notification of the next survey by post; we did not want to send mail to young people who had passed away or confidential mail to addresses where young people no longer lived. Young people were still invited to participate through email (on the assumption the email address would be inaccessible to others) but this was not an optimal retention strategy.
Having accurate contact information is reported as key to retention into longitudinal studies.14,21,24,27,28 The United Kingdom has centralized healthcare informatics (http://digital.nhs.uk) so it is possible to trace any patient with an NHS identifier number to obtain up-to-date address and details of whether they are still alive. We obtained additional regulatory approvals for this method and the first linkage made on the whole Cohort identified that 113 out of 1126 young people had died, compared to the 62 we were previously aware of and that addresses of 305 young people had changed.
The second most popular solution was to break up the online survey into modules. This was already in place, but may have reflected the traditional computer-assisted-web-interviewing (CAWI) format being used and not the “app” style applications young people are more familiar with. This is also related to the third suggestion: less paper–all information consolidated in one place. All documents have always been available through the website (www.brightlightstudy.com), which was codeveloped with young people. 10 However, from the point of study funding in 2011 until now, internet technology has advanced at an unprecedented rate and the website was now perceived as outdated by young people. As healthcare professionals working in a heavily-regulated environment it is often a challenge to keep up with technology and ensure that methods of communication are in line with those currently being used by young people. Our experience has demonstrated a yearly shift in social media preferences. From August 2012 permission to host a BRIGHTLIGHT Facebook page to be accessed on NHS computers within our host Trust took 8 months to approve and was then only granted as a closed group with young people we had physically met and who had filled out a number of consent and code of conduct forms. When we tried to reengage the Group who had suggested the Facebook page a number of them had moved on and the opportunity for continual engagement had been lost. We launched our Twitter campaign in 2014, as a public facing communication tool and as a recruitment and retention intervention. In 2015, we revised the website in response to requests from the YAP and in 2016 we launched an Instagram account at the recommendation of young people. Digital media requires an informed communications contact, which research teams may not have.
Finally, although not mentioned in young people's top 3, a topic discussed in the workshop (Table 3) and fed back by our telephone survey interviewers is that young people do not always want to revisit their cancer story. We initially had some awareness of this, and the survey is designed to only ask questions relevant to the young person's current life situation. 16 Therefore, when preparing our postcards/newsletters to feedback results to young people at 2/3 years after diagnosis we ensure they are related to noncancer issues, for example, sex and relationships. Based on the YAP's advice we will provide “short sharp information” to reinforce this fact.
This study had a number of limitations, which include a single focus group of self-selected research-aware young people and may not represent the opinions of other young people. In addition, the focus of the workshop was on cohort studies, and therefore, the recommendations may not be applicable to clinical trials. Despite this, young people have identified the retention strategies that are most acceptable to them and can act as a guide to direct resources in future research to maximize retention.
Consulting young people on measures to improve retention has been invaluable for not only affirming what we are currently doing but also ensuring this is refined to reflect young people's preferences. Similar to our previous work exploring reasons why young people would want to participate in BRIGHTLIGHT, 15 altruism, and “giving back” was a feature of conversations within the workshop. However, when facing the transition from cancer patient into living after cancer while simultaneously transitioning from a teenager into early adulthood, participation in longitudinal research is challenging. Based on the results of this workshop our recommendations for retaining young people in a cohort study are outlined in Box 3. The success of implementing the changes to optimize retention was shown in the increase in retention in Wave 3 from 30% to final participation of 58%.
Recommendations for Retaining Young People in a Cohort Study
Footnotes
Acknowledgments
The authors thank the members of the Young Advisory Panel who attended the workshop (Natasha Tollett, Nicola Johnson, Sarah Louise Metcalf, Mariia Onasanya, Stephanie Still, Jonathon Wheeler, Andrew Davies, Matthew Burgess, Zeena Beale, and Joshua Lerner); and Anita Solanki, former BRIGHTLIGHT Patient and Public Involvement Manager for maintaining the Cohort.
This article presents independent research funded by the National Institute for Health Research (NIHR) under its Program Grants for Applied Research Program (Grant Reference No. RP-PG-1209-10013). The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR, or the Department of Health. The BRIGHTLIGHT Team acknowledges the support of the NIHR, through the Cancer Research Network. L.A.F. is funded by Teenage Cancer Trust who had no input into study design, analysis, or write up.
This article is dedicated to the memory of Matthew Cook, valued member of the National Cancer Research Institutes Teenage and Young Adult Clinical Studies Group and BRIGHTLIGHT YAP.
Author Disclosure Statement
The authors R.M.T., S.L., J.S.W., and N.A. have no conflicts of interest to declare. L.A.F. is funded by Teenage Cancer Trust.