
Abstract
Purpose:
Adolescent patients with cancer experience unique stressors due to their developmental stage, with increased physical, emotional, and social distress. Palliative care (PC) serves an important role in pediatric cancer care. We examined “palliative opportunities,” or events during a patient's cancer course where subspecialty PC would be warranted and compared opportunities between adolescents and younger patients.
Methods:
Patients from a single center, 0–18 years of age at cancer diagnosis, who died from January 1, 2012, to November 30, 2017, were included. In this secondary analysis, patients were divided into cohorts based on age at diagnosis: 0–12 and 13–18 years. Demographic, disease, and treatment data were collected. Descriptive statistics and modeling were performed. Number, type, and timing of palliative opportunities and PC consultation timing and reason were evaluated across cohorts.
Results:
Of the 296 patients included for analysis, 27.7% were 13–18 years (82/296) at diagnosis. Frequency of palliative opportunities did not differ by age (median 7.0 [interquartile range 4.0 and 10.0] in both cohorts). PC consultation occurred in 36.5% (108/296), with neither rate nor timing differing by age group. PC consultations in adolescents were more often for symptom management (p = 0.0001). Adolescent patients were less likely to have a do-not-resuscitate order placed before death (61.0%, 50/82) compared to younger patients (73.8%, 158/214, p = 0.03).
Conclusion:
Adolescent patients with cancer did not experience more palliative opportunities than younger patients in this cohort, although they often have challenging psychological, family, and social stressors that were not identified. Incorporating additional palliative opportunities could enhance identification of stress and symptoms in adolescents with cancer such that PC could be timed to meet their needs.
Introduction
Adolescents are a distinct population in cancer care as their unique needs straddle the binary (adult vs. pediatric) health care system.1,2 Adolescence, defined here as patients diagnosed from ages 13–18 years, is marked by unique biological, emotional, and psychosocial changes that warrant tailored efforts different from those utilized for children or older adults.1,3 Adolescents face numerous disparities in cancer care, including delays in diagnosis due to poorer access to health care and insurance,3,4 lower enrollment in clinical trials,5,6 and financial burdens. 6 Compared to younger children, adolescents have greater cancer incidence and mortality rates, and differ in common primary cancer diagnoses. 7
Studies support subspecialty pediatric palliative care (PC) integration as a standard of cancer care to improve quality of life and family coping.8–13 Although children with cancer demonstrate high overall survival, children and their families experience physical, psychological, social, and existential distress, which could be mitigated through PC involvement focused on symptom management, emotional and psychosocial support, and if needed, advance care planning (ACP) and end-of-life (EOL) discussions.12–16 PC is especially important for adolescents, given their distinctive role and transition to autonomy in medical decision making, potential for disagreement with parents or legal decision makers, and sense of missed life experiences.
Compared to younger children, teens with cancer have significant mental health needs, 17 experiencing more guilt, fear of death, 18 somatic distress, and mood disturbances. 19 Although adolescents with cancer desire to have early conversations regarding their medical care and EOL decisions,20,21 and value less intensive EOL management such as do-not-resuscitate (DNR) order placement and hospice, 22 prior studies show that adolescents actually experience late goals of care discussions and intensive EOL care.23,24 In addition, providers identify emotional difficulties caring for adolescents with cancer as conversations are intense and teens may resist the idea of PC or their own mortality.25,26
Including PC in cancer care results in improved goals of care discussions, symptom management, psychological support, and EOL decisions. 27 PC teams can help oncology clinicians navigate complicated and emotionally charged conversations between teens and their families. Despite cancer challenging a teen's sense of invincibility and the natural order of life, adolescents demonstrate significant maturity and identify more benefits than burdens from having cancer. 28 Adolescents who receive PC are less likely to die in the intensive care unit (ICU), receive fewer invasive medical procedures near the EOL, and have a DNR order in place for a longer time, 2 and are more likely to enroll in hospice. 29
Given the demonstrated benefits of PC, it is crucial to understand the pattern of events associated with suffering to determine the best timing for PC consultation. A “palliative opportunity” is an event during a patient's disease course at which time subspecialty PC, or care provided by clinicians with subspecialty training in PC, could be provided to diminish suffering and improve the patient's or family's overall experience.30–32 Comparison of palliative opportunities between adolescents and younger patients has not been described. This secondary analysis aims to examine the number and timing of palliative opportunities in adolescents with cancer and compare to younger children, hypothesizing that adolescents experienced the most palliative opportunities. The secondary aim was to assess PC consultation rates by age, hypothesizing that adolescents receive PC earlier and more often than younger patients.
Methods
Study design
This retrospective chart review was conducted at Children's Healthcare of Atlanta (CHOA). Patients 0–18 years of age at diagnosis, who received cancer care at CHOA and who died between January 1, 2012, and November 30, 2017, were considered eligible. Inpatient pediatric PC consultative services started in 2011. Patients were excluded if adequate records were not available (lost to follow-up and received care outside of CHOA for prolonged periods). The Institutional Review Board granted exempt status.
Palliative opportunities
Palliative opportunities were defined a priori by expert consensus in 2017 before all chart review as previously described and published.30–32 Palliative opportunities are events with an increased risk of morbidity or distress during a patient's cancer course, in which PC could be initiated (Table 1). For data analysis, palliative opportunities were clustered into five categories: disease related, treatment related, symptom related, ICU related, or EOL related. Initial diagnosis was not included. Only symptoms causing hospital admission were included, rather than those arising during a hospital course or outpatient.
Palliative Opportunities in Pediatric Patients with Cancer
CAR-T, chimeric antigen receptor T cell therapy; DNR, do-not-resuscitate; EOL, end of life; HSCT, hematopoietic stem cell transplant; ICU, intensive care unit; IV, intravenous.
Data collection
Demographic information (age at diagnosis and death, sex, race, ethnicity, religion, language, and insurer), disease-related information (primary cancer diagnosis and group, relapse, progression, hospital admissions, hematopoietic stem cell transplant [HSCT], and phase 1 trial enrollment), EOL information (DNR orders, hospice enrollment, and cause of death), and date and reason for PC consultation were obtained through manual electronic health record (EHR) review using a standardized data abstraction guide, including evaluation of hospital and clinic notes, physical examination findings, imaging, and pathology results. Each episode identified as a palliative opportunity was counted and dated as a unique event, unless a patient was admitted for ICU care or multiple symptoms, which were only recorded once.
The reason for PC consultation was abstracted from the initial PC consultation note as the PC consultation note details one of three main reasons for consultation: disease related (progression/relapse or poor prognosis), symptom management (pain, dyspnea, or nausea/vomiting), or EOL related (imminently dying, hospice enrollment, or admission for EOL management). After data collection was complete, the palliative opportunity immediately preceding consultation was also denoted to further clarify the circumstances around the time of consultation. Palliative opportunities continued to be counted following a PC consultation and PC was assumed to follow a patient from consultation to death. A full description of the methods is available in Ebelhar et al. 30
Statistical analysis
The cohort was stratified based on age at diagnosis: 0–12 years (younger) and 13–18 years (adolescent). The cohort was restratified by age at death (0–12 vs. 13+) for select EOL analyses. Descriptive statistics included frequencies (percentages) for categorical variables and means (standard deviation) or medians (interquartile range [IQR]) for continuous variables. Chi-square or Fishers exact test was used to determine differences in demographics, primary diagnosis type, PC consultation, reasons for PC consultation, clinical factors, and EOL outcomes between cohorts. Mann-Whitney U test was used to assess differences in cohorts by the total and per-category number of palliative opportunities as age at diagnosis and total palliative opportunities were non-normally distributed.
Univariate and multivariate linear regression modeling were used to analyze associations between age and other covariates (sex, race, disease, and PC consultation status) on the number of palliative opportunities. p-Values were two sided and considered significant if p < 0.05; nonparametric test p-values are approximations. Analyses were conducted using SAS Enterprise Guide, v.7.1.
Results
A total of 296 deceased patients with cancer were included. More patients were 0–12 years of age (214/296, 72.3%) than 13–18 years of age at diagnosis (82/296, 27.3%) (Table 2). The median age at diagnosis was 7 years (range 0–18) and the median age at death was 10 years (range 0–22). Patients were more often non-Hispanic (86.1%), English speaking (88.8%), Christian (84.5%), and with Medicaid insurance (49.7%). Cancer diagnoses differed between cohorts, with the most common diagnoses being central nervous system (CNS) tumors in younger children (37.4%) and non-CNS solid tumors in adolescents (52,4%, p = 0.002).
Demographic Characteristics of Patients Who Died Stratified by Age at Diagnosis
Hispanic includes Mexican NOS, Mexican Chicano, Puerto Rican, South or Central American (except Brazil), Hispanic, NOS, Spanish, NOS, or Latino, NOS.
Christian denominations include Unitarian and Catholicism.
CNS, central nervous system; IQR, interquartile range.
Younger patients had a median of 2.0 (IQR 1.0, 4.0, range 0–17) progression/relapse events compared to 3.0 (IQR 0.0, 4.0, range 0–10, p = 0.39) in adolescents. Sixty-nine patients (23.3%) died without ever having a relapse/progression event without difference by age (p = 0.44). There was no association between age and phase 1 trial enrollment. Younger patients received HSCT more commonly than adolescents (25.2% vs. 10.9%, p = 0.01).
These 296 patients experienced a total of 2176 palliative opportunities. The number of palliative opportunities did not differ by age at diagnosis, with younger children and adolescents both experiencing 7.0 (IQR 4.0, 10.0) palliative opportunities (p = 0.95, Fig. 1). Palliative opportunity number did not differ by sex, race, ethnicity, primary language, or insurer. Patients reached their first palliative opportunity quickly after diagnosis: median 36.0 days (IQR 0.0, 178.0) in younger children and 24.0 days (IQR 2.0, 102.0) in adolescents (p = 0.54). Adolescents experienced more symptom-related opportunities (1.0, IQR 0.0, 2.0, range 0–6) than younger children (0.0, IQR 0.0, 1.0, range 0–12, p = 0.04).
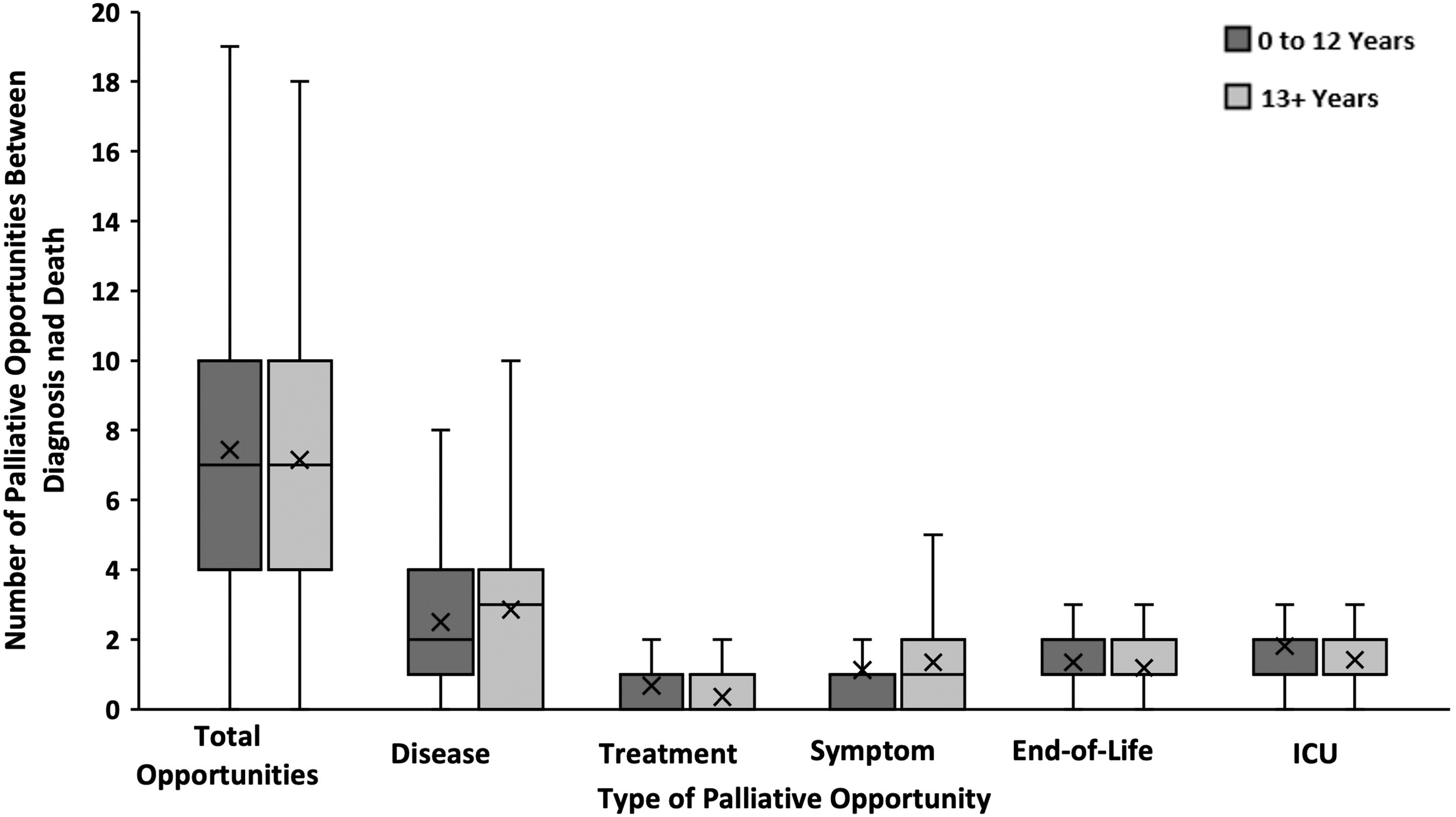
Palliative opportunities by age and type.
When stratified by age and diagnosis (leukemia/lymphoma, solid tumor, and CNS tumor), there was no difference in palliative opportunities within solid and CNS tumor diagnoses (median of 8 and 7 opportunities in both cohorts, respectively). Among those with leukemia/lymphoma, adolescents experienced fewer palliative opportunities (median 3.5) compared to the younger cohort (median 5.0), although this was not significant (p = 0.32).
In total, 36.4% of patients received subspecialty PC consultation, 36% (77/214) of younger children and 37.8% (31/82) of adolescents (p = 0.79). Patients experienced a median of 4.0 (IQR 2.0, 7.0) palliative opportunities before consultation in both cohorts (p = 0.72). The time between first palliative opportunity and PC consultation was 176.5 days (IQR 47.0, 416.0) in younger children and 281.0 days (IQR 31.0, 541.0) in adolescents (p = 0.49). This lag time decreased over time, from 310.0 days (IQR 69.0, 569.5) in 2012–2014 to 171.0 days (IQR 30.0, 398.5) in 2015–2017. Patients in the younger cohort received PC consultation 47.0 days (IQR 10.0, 159.0) before death, compared to 62 days (IQR 12.0, 114.0) before death in the adolescent cohort (p = 0.97).
The most frequent reason for PC consultation was disease-related progression/relapse in children (76.6%) compared to symptom management in adolescents (48.4%, p = 0.0001). Overall, 83.7% (1821/2176) of palliative opportunities occurred before or without PC involvement with no significant difference by age (1340/1590, 84.3% in younger cohort and 481/586, 82.1% in adolescent cohort). There was no significant difference in survival time [younger cohort: 480.5 days (IQR 242.0, 965.0) and adolescents: 460.5 days (IQR 202.0, 799.0, p = 0.30).
In assessing EOL care, 53% of both younger patients and adolescents enrolled in hospice (44/82 and 114/214, respectively, p = 1.0). Overall, 208/296 (70.2%) had a DNR order documented a median of 6 days (range 0–277) before death. Adolescents were slightly less likely to have a DNR order (61.0%, 50/82) compared to younger patients (73.8%, 158/214, p = 0.03). There was no difference in the median time from DNR order to death (younger 6.5 days (IQR 1.0, 23.0) versus adolescent 6.0 days (IQR 1.0, 25.0; p = 0.67).
Few patients (18, 6.1%) were admitted to the hospital specifically for EOL care, with no difference across cohorts (p = 0.42), although small numbers limited analysis. In the last month of life, 39.9% (118/296) of patients had an ICU admission with no difference between cohorts (p = 0.60). Younger children (78%) and adolescents (74.4%) predominately died of disease progression (p = 0.46, Table 3). If EOL outcomes are instead assessed by age at death, having a DNR order trends nonsignificant (158/214, 74.3% in younger cohort vs. 72/113, 63.7% in adolescent group, p = 0.05). All other EOL outcome variables remained nonsignificant.
Palliative Opportunities, Palliative Care Consultation, and Mechanism of Death Stratified by Age at Diagnosis
Palliative opportunity categories as noted in Table 1.
Reason for PC consultation was categorized as disease related (progression and relapse), symptom management (pain, dyspnea, fatigue, and nausea/vomiting), and EOL related (DNR, hospice enrollment, and EOL management).
Among those that received a PC consultation.
PC, palliative care.
In univariate regression analyses, age at diagnosis was not a significant predictor of total opportunities (beta = −0.28, 95% confidence intervals (CI), −1.48 to 0.9; p = 0.64). There remained no statistically significant association in multivariate linear regression models between age and total palliative opportunities after adjusting for sex, race, diagnosis, and receipt of PC (beta = −0.47, 95% CI, −1.65 to – 0.71; p = 0.43) (Table 4).
Factors Associated with the Total Number of Palliative Opportunities
β estimates represent the increase or decrease in total number of palliative opportunities for every one unit of change in the predictor variables.
Age at death was also evaluated as a predictor of total opportunities to determine if age at death (compared to age at diagnosis) resulted in significant differences. In this adjusted model, age at death was also nonsignificant. No other significant differences existed when compared to using age at diagnosis as the predictor.
β, linear regression coefficient; CI, confidence interval.
Discussion
Adolescents often have higher physical and psychological symptom burden and receive more intensive care at the EOL than younger patients with cancer.17,19 We sought to identify whether age at diagnosis would be a factor in the number and timing of palliative opportunities. Adolescents and younger patients with cancer had a similar number of palliative opportunities and rate of PC consultation, with few associations found between diagnosis age and palliative opportunities. However, differences by primary diagnosis groups (leukemia/lymphoma, solid tumors, and CNS tumors) as well as differences in patterns of palliative opportunities and EOL experiences provide insight into the ways in which children of different ages and their families experience cancer.
These 296 patients experienced 2176 palliative opportunities, or seven palliative opportunities per patient, emphasizing the high potential for suffering during a cancer course, regardless of age. Adolescents experienced more symptom-related palliative opportunities than younger patients, consistent with prior data showing more physical and psychological distress in adolescents.18,19 It is unknown if adolescents suffer from more symptoms or are better able to communicate their experience to their family and care team.
As expected, diagnoses differed by age. Older patients had more solid tumors compared to younger patients who had more CNS tumors. Prior studies30–32 have shown that diagnosis influences the number of palliative opportunities. Therefore, further analysis of palliative opportunities accounting for both age and diagnosis was required to account for confounders between age and palliative opportunities. While patients with solid or CNS tumors experienced the same median number of palliative opportunities regardless of age, adolescents with leukemia/lymphoma experienced fewer palliative opportunities compared to children, although this was not significant.
As older patients with leukemia are classified as high risk, 33 this could be explained by several factors. First, our system of evaluating palliative opportunities did not account for (1) physical symptoms occurring without hospital admission, a common preference among teenagers who prefer their home environment, (2) psychological symptoms, like depression or anxiety, (3) psychosocial stressors with friends or family, and (4) challenges with autonomy or lack of concordance with parental decisions, a challenge that disproportionately affects teenagers. 34 Second, certain opportunities, including HSCT and DNR orders, were more common in the younger cohort. HSCT often leads to additional opportunities such as ICU admissions and symptom-related admissions, and increases the likelihood of PC consultation. 31 Although having a DNR order placed, an often upsetting conversation for patients and families, counted as a palliative opportunity, it is perhaps a “full code” order that causes clinician distress in patients with end-stage cancer. Third, nonadherence and higher rates of being lost to follow-up among teenagers could contribute to missed opportunities.
PC consultation rates were low, and timing was often late, yet did not differ by age. Despite reports of earlier PC involvement for adolescents with cancer, 27 this was not seen in our cohort, which may be due to institutional differences (different PC services and presence or lack of outpatient services). Interpersonal stress between patients, families, and care teams, secondary to emerging independence and complex roles in decision making, could lead to desire for PC consultation. 35
Numerous studies reveal the difficulties in caring for adolescents with cancer from the provider viewpoint.25,36,37 However, families of children of all ages are open to receiving early PC support and express a desire to engage in discussion about their care and goals.21,28,35 Providers' emotional connections to adolescents who are often more aware of their prognosis, coupled with hope for cure, may delay goals of care conversations, contributing to the difference in reason for consultation. This study cannot assess the presence, timing, or quality of goals of care conversations with the primary oncology team or implicit age bias from the provider team.38,39
Patients age 13–18 years at diagnosis had slightly lower rates of DNR order placement than younger patients. Intensive EOL care is not uncommon in adolescents with cancer, and many were not engaged in EOL discussions until close to death, despite studies showing that adolescents want to be included in ACP early in the disease course.20,23,24,40 Many adolescents are also willing to accept invasive procedures in an attempt to continue to “fight,” get back to their prior baseline, prolong life as long as possible,23,24,41 appease family members, or avoid death.18,42 In addition, growing autonomy among adolescents can make ACP more complex, as family and patient wishes may not always align.34,43,44 Adolescent and younger patients had similar rates of hospice utilization, presumably due to a prevailing wish to spend time at home. 45
Several limitations exist. Results were gathered from a large, tertiary care, single institution with an inpatient PC team and therefore may not be generalizable to all pediatric oncology centers. All patients were deceased, so the number of met and unmet palliative opportunities in surviving patients is unknown. Young adult patients (19+ years at diagnosis), frequently treated in pediatric centers, were excluded, but are also known to have high symptom burden, ACP needs, and distress. Patients were divided into cohorts by age at diagnosis, although developmental differences are incredibly diverse within each cohort, and 31 patients diagnosed in the younger cohort died as adolescents (median 14 years), necessitating some analyses by both age at diagnosis and death, although minimal differences existed. We recommend clinicians focus on age at diagnosis when caring for patients. Finally, although minimized through multiple mechanisms, missed opportunities could occur when a patient developed additional symptoms during long hospitalizations, spent months at home before the EOL, died at home, or their home DNR order was not scanned into the EHR, furthering the likelihood that median number of palliative opportunities is a conservative minimum.
Future directions for research include identification of psychosocial and mental health-related palliative opportunities and their significance in cancer care. Defining psychosocial and mental health needs of this population could include consultation with adolescent medicine, psychology, and psychiatry specialists who often manage mental health in teens. Consideration should be given to electronic symptom monitoring and capture of patient-reported outcomes relevant to health-related quality of life. Qualitative analysis of EOL discussions with adolescents, including how their goals are balanced with family and care team goals, as well as their integration into decision making, may inform providers on how best to support their preferred style of information receipt, medical decision making, and timely PC intervention to preserve QOL. 46 Finally, comparison of palliative opportunities across the entire adolescent/young adult age spectrum (15–39) could identify places for improvement in pediatric and adult cancer care.
Conclusion
Patients with cancer have unique experiences based on their varying developmental status, emerging independence, and psychosocial needs. Perhaps due to the focused list of palliative opportunities, there was no difference in the number or timing of palliative opportunities between younger children and adolescents with cancer. Across all ages, patients endured numerous events that could lead to patient suffering and family distress. Despite data showing positive outcomes for PC within adult and pediatric oncology care, patients endured over 80% of these episodes without subspecialty PC support.
Further refining and expanding the list of palliative opportunities to include mental health diagnoses, patient-reported outcomes, and provider or interdisciplinary team assessments of family coping should be considered. While PC consults in adolescents are often symptom focused, opportunities to engage around coping, goals of care, and planning for EOL may present themselves. Understanding differences in palliative opportunities between adolescents and younger patients could help target PC interventions to the right patients at the right time.
Footnotes
Authors' Contributions
E.J.L.: data curation, investigation, visualization, writing-original draft, and writing-review and editing. N.P.D.: data curation, formal analysis, methodology, project administration, visualization, and writing-review and editing. J.E.: conceptualization, data curation, methodology, supervision, validation, and writing-review and editing. A. M.M.: investigation, data curation, and writing-review and editing. K.E.A.: data curation, formal analysis, and writing-review and editing. S.M.C. and K.W.-M.: supervision and writing-review and editing. K.E.B.: conceptualization, data curation, investigation, methodology, project administration, resources, supervision, validation, visualization, and writing-review and editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
K.E.B. is supported by the Rally Foundation for Childhood Cancer. The funding agency was not involved in the design or conduct of this study. Award ID 19YIC42.